Open Neural Tube Defect | Multidisciplinary Lifelong Care
- Definition: Failure of neural tube closure (3-4 weeks gestation). Exposed spinal cord and meninges.
- Latex Allergy: Assume ALL MMC patients are allergic. 50% will develop clinical allergy. Do NOT use latex gloves or catheters.
- Chiari II Malformation: Present in nearly all MMC patients. Cerebellar tonsils herniate into foramen magnum. Causes hydrocephalus.
- Tethered Cord: Progressive neurological deterioration due to scar tethering. Look for new scoliosis, pain, or changing bladder function.
- Folic Acid: Reduces incidence by 70%. Standard public health measure.
- “The FUNCTIONAL level is often 1-2 segments WORSE than the anatomical level.
- “Sensation is often better preserved than motor (Sacral sparing).
- “Assume shunt malfunction until proven otherwise in any unwell MMC patient.
- “Never use latex! (Tubing, gloves, Foley).
Life Threatening. Anaphylaxis risk. Use non-latex gloves, catheters, IV tubing. Mark charts CLEARLY.
Silent Killer. Any headache, vomiting, irritability, or drowsiness = Shunt series + CT Head STAT.
Surgical Emergency. New neuro deterioration, scoliosis, or bladder changes = MRI Spine URGENT for tethering.
Silent Destroyer. Insensate skin. Brace/Cast breakdown. Ischium/Sacrum ulcers. Prevent with vigilance.
| Defect | Neural Elements | Prognosis |
|---|---|---|
| Spina Bifida Occulta | None exposed (Covered) | Excellent (Often incidental) |
| Meningocele | Meninges only (CSF sac) | Good (Neurologically normal) |
| Myelomeningocele | Cord + Roots exposed | Variable (Level dependent) |
| Myeloschisis | Open placode (No sac) | Poor (High lesion common) |
I LOVE Q-TIPSLevel by Muscle
Hook:Myotome Map for MMC.
BEAKSChiari II Features
Hook:MRI findings of Arnold-Chiari Type II.
SPASMTethered Cord Signs
Hook:Signs of secondary tethering.
Overview and Epidemiology
Definition: Myelomeningocele (MMC) is the most severe form of spina bifida cystica. It is an open neural tube defect (NTD) where the spinal cord and nerve roots are exposed through a defect in the vertebral arches and skin. The neural tissue (placode) lies on the surface of the back, surrounded by meninges and CSF.
Epidemiology:
- Incidence: Approximately 1 in 1000 live births (variable by geography and folic acid fortification).
- Prevention: Periconceptional folic acid supplementation (0.4mg daily) reduces risk by 50-70%.
- Prenatal Diagnosis: Elevated maternal serum AFP (MSAFP), detailed ultrasound (Lemon sign, Banana sign).
- Trends: Incidence decreasing due to folic acid fortification and prenatal diagnosis/termination.
Genetics and Recurrence:
- Recurrence Risk: If one child is affected, the recurrence risk is 2-4%. If two children are affected, risk increases to 10%.
- Folic Acid (Recurrence): High-dose folic acid (4mg daily) is recommended for subsequent pregnancies if there is a history of NTD.
- Genetic Syndromes: MMC is usually sporadic, but can be associated with trisomy 18 or Meckel-Gruber syndrome.
Pathophysiology and Anatomy
Embryology: The neural tube closes between days 21-28 of gestation. Failure of posterior neuropore closure results in MMC. This results in:
- Exposure of Placode: Direct damage and ongoing leakage of CSF.
- Loss of Innervation: Motor and sensory loss below the level.
- Skeletal Deformity: Muscle imbalance drives deformity (hip dislocation, clubfoot, scoliosis).
- Associated CNS Malformations: Chiari II, hydrocephalus.
Chiari Type II Malformation: Present in almost all patients with MMC. The hindbrain (cerebellum, brainstem) herniates through the foramen magnum. This causes:
- Hydrocephalus: 80-90% require shunting.
- Brainstem Dysfunction: Stridor (vocal cord paralysis), apnea, swallowing difficulty.
- Syringomyelia: Cavity formation within the cord.
Tethered Cord: After initial MMC closure, scar formation tethers the neural placode to the dural repair. During growth, differential traction on the cord causes secondary neurological deterioration. This is often insidious.
Classification
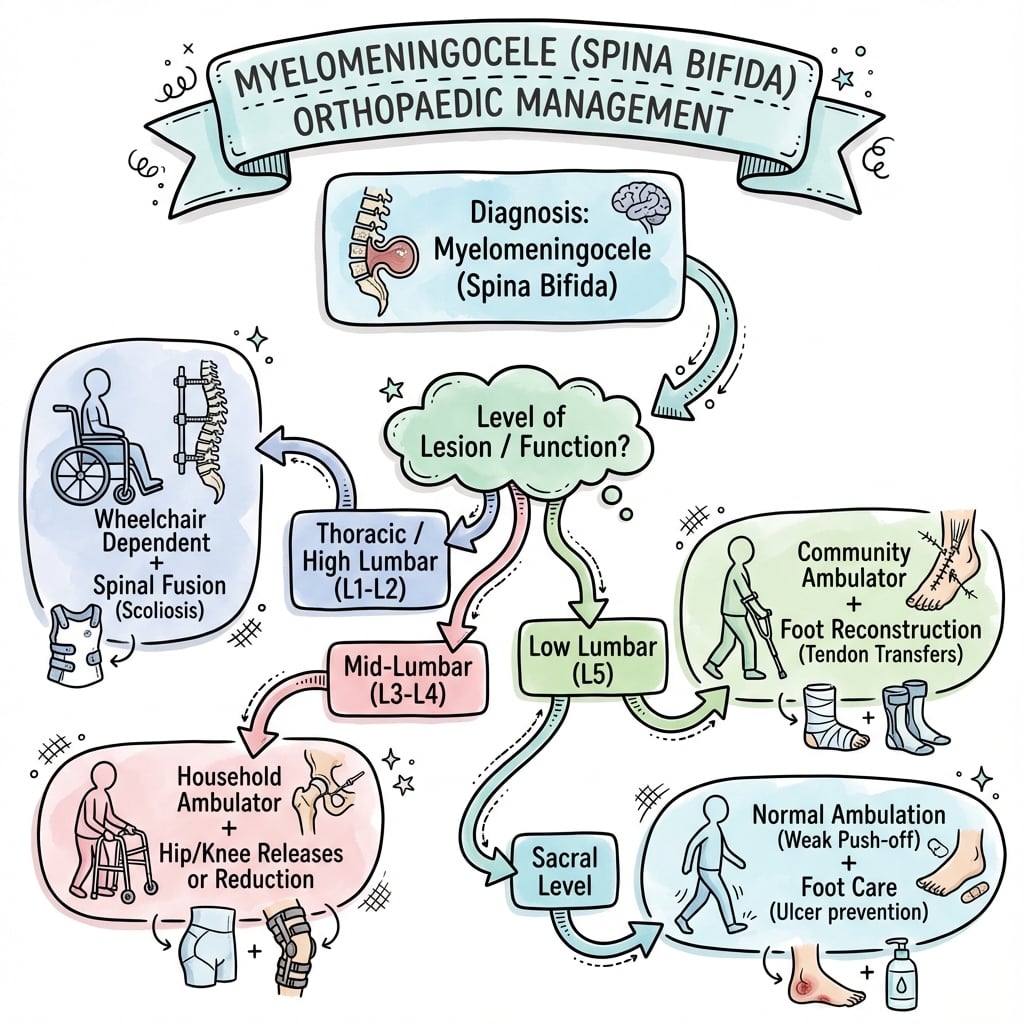
Functional Neurological Level
The key to prognosis and treatment planning. Determined by the LOWEST functional myotome.
- Key Muscle
- None
- Ambulation Potential
- Wheelchair dependent
- Key Muscle
- Iliopsoas (Hip flexion)
- Ambulation Potential
- Therapeutic walking only (HKAFO)
- Key Muscle
- Quadriceps (Knee extension)
- Ambulation Potential
- Household ambulation (KAFO)
- Key Muscle
- Tibialis Anterior (Dorsiflexion)
- Ambulation Potential
- Community ambulation (AFO, Crutches)
- Key Muscle
- Gluteus Medius (Hip abduction)
- Ambulation Potential
- Community ambulation (AFO, minimal aids)
- Key Muscle
- Gastrocnemius (Plantarflexion)
- Ambulation Potential
- Independent ambulation (AFO optional)
The functional level is often 1-2 segments worse than the anatomical (vertebral) level.
Differential Diagnosis
The visible back lesion and the pattern of neurological deficit must be distinguished from other dysraphic and neuromuscular conditions, because management and prognosis differ sharply.
| Condition | Key Features | Discriminator |
|---|---|---|
| Myelomeningocele (open) | Exposed placode, CSF leak, deficit + Chiari II | Open neural tissue at birth; near-universal Chiari II / hydrocephalus |
| Meningocele | Skin-covered CSF sac, cord normal | Neurologically intact; no Chiari II |
| Lipomyelomeningocele | Skin-covered fatty mass tethering cord | Closed lesion presenting later with tethering, not a neonatal emergency |
| Spina bifida occulta / occult dysraphism | Dimple, hairy patch, lipoma; arch defect only | Cutaneous stigmata, usually asymptomatic; MRI to exclude tethering |
| Sacral agenesis (caudal regression) | Flattened buttocks, fixed flexion, often maternal diabetes | Absent sacral segments on X-ray; abrupt cord termination |
| Arthrogryposis | Symmetric rigid contractures, intact sensation | Sensation preserved; no dysraphism or Chiari II |
Clinical Assessment
Neonatal Assessment:
- Urgent Coverage: The open placode must be surgically covered within 24-48 hours to prevent meningitis.
- Neurological Exam: Document motor level (lowest functioning myotome). Check reflexes. Observe spontaneous movement.
- Head Circumference: Monitor for hydrocephalus (increasing HC, bulging fontanelle, sunsetting eyes).
Orthopedic Assessment:
- Spine: Kyphosis (Gibbus)? Scoliosis?
- Hips: Dislocated (common in L3-L4)? Contractures?
- Feet: Clubfoot? Vertical Talus? Calcaneovalgus?
- Overall Posture: Spinal alignment. Pelvic obliquity.
Neurological Monitoring (Lifelong):
- Tethered Cord Surveillance: Annual neuro exam and urodynamics. MRI if any new symptoms (SPASM).
- Shunt Function: Low threshold for shunt series/CT if any change in cognition, headaches, nausea.
Investigations
Clinical Imaging Atlas





Initial Imaging:
- MRI Brain: Evaluate Chiari II, hydrocephalus, corpus callosum.
- MRI Spine: Assess conus level, syrinx, tethering (if suspected later).
- Hip X-rays: AP Pelvis. Assess hip dysplasia/dislocation.
- Spine X-rays: Evaluate kyphosis, scoliosis, congenital vertebral anomalies.
Urological Workup:
- Urodynamics: Baseline and annual. Assess detrusor function (hyperreflexic vs areflexic), sphincter function.
- Renal Ultrasound: Annual. Monitor for hydronephrosis/reflux.
- VCUG: As indicated.
Functional Assessment:
- Gait Analysis: For ambulatory patients, to plan orthotic needs.
- FIM (Functional Independence Measure): Overall function.
Management Algorithm
Neonatal Management (First 48 Hours)
- Prone Positioning: Protect the sac from rupture or contamination.
- MMC Closure: Urgent surgery within 24-48 hours (Neurosurgery). Goal: Watertight dural closure, skin coverage.
- VP Shunt: Often placed at the same time or shortly after MMC closure (if hydrocephalus develops).
- Latex Precautions: Implement from birth.
- Multidisciplinary Team: Neurosurgery, Orthopaedics, Urology, Physical Therapy, Social Work.
The MOMS trial showed fetal MMC repair (prenatal closure) reduces shunt requirement and improves motor function.
Surgical Technique
Hip in MMC
Dislocation is COMMON (especially L3-L4): Strong hip flexors (Psoas), absent glutei (Gluteus Med/Max).
Management Philosophy:
- Thoracic/High Lumbar (No ambulation potential): Leave the hip dislocated. Reduction surgery does NOT improve function and has high complication rate.
- L3-L4 (Ambulatory potential): Controversial. Some advocate for reduction, others leave alone.
- L5-S1 (Good ambulatory potential): Treat similar to DDH. Reduction may improve gait efficiency.
Procedures (if performed):
- Soft tissue releases (Adductor, Psoas).
- Open Reduction +/- Femoral/Pelvic Osteotomy (for older kids).
- Iliopsoas Transfer (Mustard/Sharrard): Transfer Psoas to Greater Trochanter to create abductor. Very high failure rate and rarely done now.
The key question: Will reducing this hip improve this child's function or quality of life?
Complications
| Complication | Cause | Management |
|---|---|---|
| Shunt Malfunction | Blockage / Infection | Shunt series, CT Head, Urgent Neurosurgery |
| Tethered Cord | Scar tissue from repair | MRI Spine, Urodynamics, Surgical Untethering |
| Pressure Sores | Insensate skin, Brace/Cast | Prevention, Wound Care, Plastic Surgery |
| Latex Anaphylaxis | Protein allergy (sensitization) | Strict latex avoidance, Epi-Pen |
| Pathologic Fracture | Osteopenia, Insensate limb | Often minimally symptomatic. Cast/Splint. |
| Renal Failure | Neurogenic bladder, Reflux | CIC, Anticholinergics, Vesicostomy |
Latex Allergy:
- Affects 30-70% of MMC patients (depending on definition).
- Sensitization occurs from repeated mucosal exposures (surgeries, catheterizations).
- Prevention: Latex-free environment from birth.
- Signs: Urticaria, Angioedema, Bronchospasm, Anaphylaxis.
Postoperative Care
- Wound Care: Paramount due to insensate skin. Padding. Frequent skin checks.
- Latex Free: Non-latex catheters, gloves, IV tubing.
- Positioning: Avoid pressure on surgical sites and insensate areas.
- Rehabilitation: Intensive physio for gait training post lower limb surgery.
Outcomes
- Survival: Greater than 80% survive to adulthood with modern care.
- Ambulation: Sacral levels walk independently. Thoracic levels are wheelchair-dependent.
- Cognition: Approximately 80% have normal IQ, though learning disabilities are common.
- Quality of Life: Can be excellent with multidisciplinary support.
- Mortality: Primarily from renal failure and shunt complications.
Controversies & Areas of Uncertainty
- Timing and selection for fetal repair: MOMS/MOMS2 established benefit, but eligibility is narrow and maternal/obstetric risk (preterm birth, uterine dehiscence) is real. Fetoscopic techniques aim to reduce maternal morbidity, but comparative long-term neurological data versus open repair remain immature.
- Prophylactic vs symptomatic untethering: Almost all repaired cords are radiologically "tethered". There is no consensus to operate on a radiologically low conus in the absence of clinical or urodynamic deterioration - surveillance, not the MRI appearance alone, drives surgery.
- The dislocated hip: Whether to reduce a unilateral or bilateral dislocation in a mid-lumbar (L3-L4) ambulator is genuinely contested; many units now prioritise a level pelvis and balanced sitting over radiographic reduction.
- Kyphectomy: Effective for severe rigid gibbus interfering with sitting and skin integrity, but carries high rates of wound breakdown, implant failure and blood loss; indications and fixation strategy vary between centres.
- Folic-acid dosing for prevention vs recurrence: 0.4 mg/day for general prevention vs 4-5 mg/day for women with a prior affected pregnancy; the optimal dose and the role of universal fortification in voluntary-supplementation countries remain debated.
Evidence Base
MOMS Trial - Prenatal vs Postnatal Repair
- Multicentre RCT (183 of planned 200 enrolled; trial stopped early for efficacy); analysis on 158 children at 12 months.
- Prenatal repair (before 26 weeks) reduced actual VP-shunt placement by 12 months to 40% vs 82% postnatal (RR 0.48, 97.7% CI 0.36-0.64).
- Improved composite mental development and motor score at 30 months (P=0.007) and reduced hindbrain herniation.
- Cost: increased preterm delivery and uterine dehiscence.
MOMS2 - Durability of Prenatal Repair at School Age
- Prespecified physical-function follow-up of MOMS at ages 5-10 years (154 children examined by blinded assessors).
- Community ambulation in 51.3% of the prenatal group vs 23.1% postnatal (adjusted RR 1.70, 95% CI 1.23-2.34).
- Prenatal group had better self-care, faster 10-m walk, higher-level mobility skills.
- Less likely to have motor level worse than anatomical level (aRR 0.44, 95% CI 0.25-0.77).
MRC Vitamin Study - Folic Acid Prevention
- Randomised, double-blind factorial trial; 1817 high-risk women (prior affected pregnancy) across 33 centres in 7 countries.
- Folic acid produced a 72% reduction in NTD recurrence (RR 0.28, 95% CI 0.12-0.71).
- The other-vitamins arm showed no significant protective effect.
- Directly underpinned global folic-acid fortification and supplementation policy.
Tethered Cord Release - Long-Term Outcomes
- Single-institution cohort: symptomatic tethering developed in 114 of 502 children with MMC (23%); mean follow-up 12 years.
- Shunt malfunction is the most common cause of decline; tethering is second.
- After untethering, pain improved in 100%, lower-limb strength improved in 70%, and bladder function improved in 64%.
- Scoliosis still progressed after untethering in 52%, with 28% needing fusion.
Latex Sensitisation in Spina Bifida
- 47% (39/83) of children with MMC had latex-specific IgE, vs 15.7% of chronically ill controls and under 4% of medical/well controls.
- Risk of a positive test rose with the number of prior operations.
- MMC children were sensitised more than chronically ill controls with similar surgical histories, implicating MMC-specific exposure.
Surgical Management of the Neurogenic Hip in MMC
- Long-term review of 131 hips in 85 MMC patients (follow-up to 38 years), stratified by modified Sharrard-Parsch groups.
- Operating on minimally involved hips (Groups I-II) was associated with a high recurrence rate.
- In selected ambulatory hips (Group III) comprehensive reconstruction gave good stability; 65% became ambulant.
Viva Scenarios
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“Outline your initial management.”
“Discuss your approach to this hip.”
“What is your differential and workup?”
MCQ Practice Points
Q: What is the key difference between Chiari I and Chiari II malformation? A: Chiari I is tonsillar herniation only (often acquired). Chiari II is seen with MMC and includes brainstem herniation, tectal beaking, and hydrocephalus.
Q: What is the single most important measure to prevent latex allergy in MMC? A: Latex-free environment from birth. Avoid all latex exposure (gloves, catheters, balloons).
Q: What is the main determinant of ambulatory potential in MMC? A: The Functional Neurological Level. Patients with L5 or lower levels have the best ambulatory potential. Thoracic levels are wheelchair dependent.
Q: By how much does folic acid supplementation reduce the risk of neural tube defects? A: Approximately 50-70% reduction.
Q: In a child with thoracic-level MMC and bilateral hip dislocation, should you reduce the hips? A: No. Hip reduction in non-ambulatory patients has high failure rates and does not improve function. Leave them alone unless painful.
Guidelines, Registries & Global Practice
Global Epidemiology:
- NTD birth prevalence varies widely with diet, fortification policy and prenatal screening: roughly 0.5-1 per 1000 in fortified, high-income settings, but markedly higher in regions without fortification (parts of South Asia, the Middle East and sub-Saharan Africa report several per 1000).
- Mandatory folic-acid fortification of staple flour (adopted by the USA, Canada, Australia, much of Latin America and a growing number of African and Asian countries) has reduced NTD prevalence by an estimated 30-50% at population level. Many European countries still rely on voluntary supplementation alone, where uptake is incomplete.
Side-by-Side Guidance (where recommendations differ):
| Body / Source | Folic Acid | Fetal Surgery |
|---|---|---|
| WHO / CDC (US) | 0.4 mg/day all women planning pregnancy; food fortification advocated | Recognised option at experienced fetal centres |
| RCOG / NICE (UK) | 0.4 mg/day; 5 mg/day if prior NTD, diabetes, high BMI or on antiepileptics | Referral to specialist fetal-medicine units |
| High-risk (prior NTD) | 4-5 mg/day periconceptionally (per MRC trial) | Counsel re: MOMS eligibility criteria |
Registry & Network Data:
- National spina bifida registries and care networks (e.g. the US National Spina Bifida Patient Registry and European reference networks) track ambulation, renal function, shunt revisions and pressure-sore burden, and have driven standardisation of multidisciplinary follow-up.
- Outcome data consistently show that renal preservation (clean intermittent catheterisation, anticholinergics, surveillance) and shunt vigilance are the principal determinants of long-term survival.
High- vs Limited-Resource Practice Variation:
- High-resource: prenatal diagnosis, option of fetal repair, lifelong multidisciplinary clinics, urodynamics-guided bladder management.
- Limited-resource: later presentation (sometimes with neglected, infected or ruptured sacs), limited shunt access, reliance on clinical rather than urodynamic bladder monitoring, and greater dependence on bracing/positioning over reconstructive surgery. Prevention through fortification has the largest public-health impact in these settings.
Levels
- L1-L2: Hip Flexion Only
- L3: Quads (Knee Ext)
- L4: Tib Ant (Dorsiflex)
- L5: Glut Med (Abduct)
- S1: Gastroc (Plantar)
Chiari II
- Brainstem Herniation
- Tectal Beaking
- Hydrocephalus (80%)
- Syringomyelia
- Universal in MMC
Tethered Cord
- S: Scoliosis (New)
- P: Pain
- A: Asymmetry
- S: Sphincter (Bladder)
- M: Motor Loss
Latex Rules
- Assume ALL MMC allergic
- Latex-Free from Birth
- No latex gloves/catheters
- Mark charts CLEARLY