Medial Column Keystone | AVN Risk | Sangeorzan Classification | Athletes at Risk
- Precarious blood supply - central third is watershed zone (AVN risk)
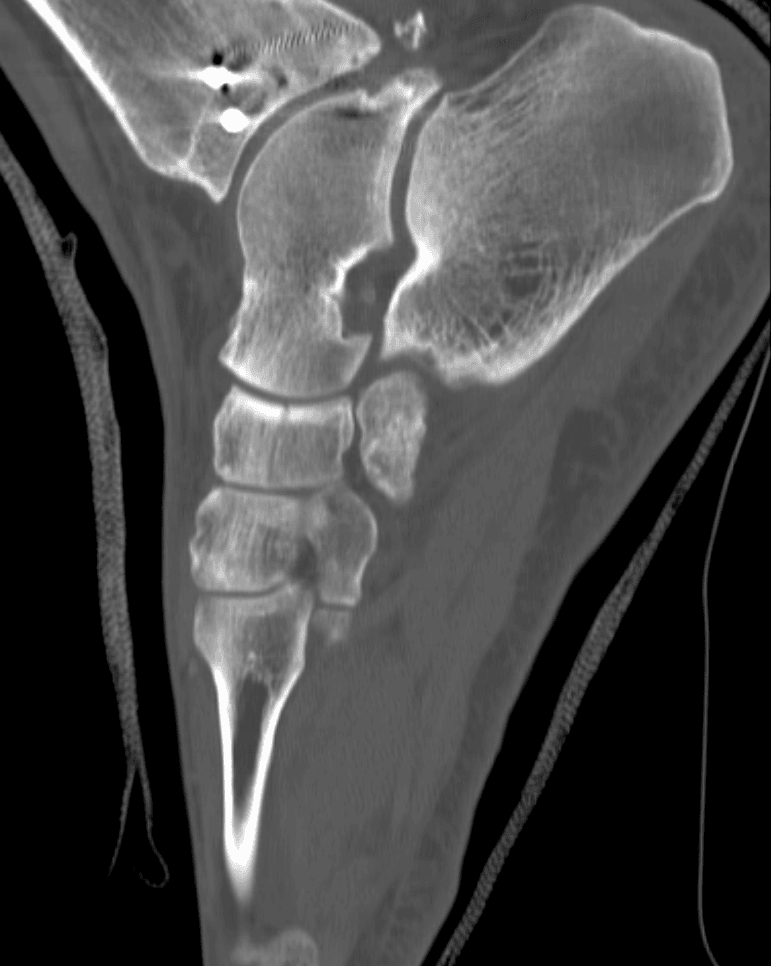
- CT scan essential for body fractures - assess articular displacement
- Stress fractures - often missed initially, high index of suspicion in athletes
- Medial column length must be restored - avoid shortening
- 6-8 weeks non-weight-bearing minimum for stress fractures
- “Blood supply: dorsal and plantar arteries, central zone relatively avascular
- “Sangeorzan Type 2 most common body fracture pattern
- “Stress fractures: central third, sagittal orientation, bone scan/MRI to diagnose
- “Associated injuries: cuboid, cuneiforms, tarsometatarsal joint
- “Malunion leads to planovalgus deformity and midfoot arthritis
- High-energy midfoot trauma - systematic assessment of Chopart/Lisfranc complex
- Athlete with vague midfoot pain - navicular stress fracture until proven otherwise
- Displaced navicular body fracture - surgical approach and fixation options
- Post-operative AVN - recognition and salvage options
- Malunion with planovalgus - reconstructive options
- "X-rays are sufficient for surgical planning"
- "Weight-bear as tolerated for stress fractures"
- "Accept any displacement of navicular body fractures"
- "The navicular has good blood supply like other tarsal bones"
Overview
Tarsal Navicular Fractures
The tarsal navicular is a key bone of the midfoot, serving as the keystone of the medial longitudinal arch. Fractures range from minor avulsions to complex body fractures with significant displacement and associated injuries.
The navicular's tenuous blood supply makes it susceptible to avascular necrosis (AVN), similar to the scaphoid in the wrist. The central third is a watershed zone with limited vascularity, explaining the high nonunion rate in navicular stress fractures.
- Avulsion fractures - Most common (47%)
- Body fractures - Significant injuries, high complication rate
- Stress fractures - Important in athletes
- Tuberosity fractures - Posterior tibial tendon insertion
- Rare injuries - navicular fractures comprise 3-5% of all foot fractures
- Body fractures often associated with high-energy trauma
- Stress fractures common in athletes (track and field, basketball, football)
- Male predominance in body fractures
- Peak age: 20-40 years
Anatomy and Blood Supply
- Location: Keystone of medial longitudinal arch
- Articulations: Talus (proximally), three cuneiforms (distally), cuboid (laterally)
- Insertions: Posterior tibial tendon on tuberosity (major dynamic arch support)
- Shape: Boat-shaped (Latin: navicula = little boat)
- Part of Chopart (transverse tarsal) joint with talus
- Forms talonavicular joint - critical for hindfoot motion
- Spring ligament supports plantar surface
Blood Supply - Critical Exam Topic
The navicular's blood supply is tenuous and similar to the scaphoid:
- Dorsalis pedis artery - dorsal branches
- Medial plantar artery - plantar branches
- These vessels enter from the periphery (medial and lateral)
- The central third of the navicular body is relatively avascular
- Blood supply enters peripherally and does not reach central zone reliably
- This explains high AVN rate in body fractures (25%) and stress fractures
- Central stress fractures have high nonunion rate
- Displaced body fractures disrupt peripheral blood supply
- Open reduction should preserve soft tissue attachments
Functional Anatomy
- Navicular is the "cornerstone" of the medial column
- Medial column: talus → navicular → medial cuneiform → first metatarsal
- Maintains longitudinal arch height
- Shortening leads to planovalgus deformity
- Provides 80% of hindfoot inversion/eversion
- Essential for gait adaptation to uneven surfaces
- Loss of motion significantly affects function
Fracture Types by Location
- Percentage
- 47%
- Mechanism
- Talonavicular capsule pull
- Key Features
- Low energy, good prognosis
- Percentage
- 24%
- Mechanism
- PTT avulsion or direct trauma
- Key Features
- May need fixation if large
- Percentage
- 26%
- Mechanism
- High-energy axial load
- Key Features
- High complication rate
- Percentage
- 3%
- Mechanism
- Repetitive loading
- Key Features
- Athletes, central location
Classification Systems
Sangeorzan Classification for Body Fractures
The Sangeorzan classification (1989) categorizes navicular body fractures based on fracture pattern and degree of displacement.
Coronal plane fracture
- Transverse fracture line
- Dorsal fragment
- No forefoot angulation
- Talonavicular joint intact
- Treatment: ORIF if displaced
- Prognosis: Good if reduced
Dorsomedial to plantar-lateral
- Main fracture oblique
- Forefoot displaced dorsally
- Medial column shortened
- Most common pattern
- Treatment: ORIF essential
- Prognosis: Moderate - AVN risk
Comminuted
- Central/lateral comminution
- Severe articular damage
- Often high-energy
- Associated injuries common
- Treatment: ORIF + bone graft
- Prognosis: Poor - high AVN/arthritis
Clinical Application:
- Higher type = worse prognosis
- Type 2 most common in clinical practice
- All require CT for surgical planning
These fracture patterns guide treatment decisions and prognosis estimation.
Clinical Assessment
History
- High-energy mechanism (MVA, fall from height)
- Axial loading through foot
- Immediate inability to weight-bear
- Associated injuries common (25%)
- Insidious onset of midfoot pain
- Worse with activity, improves with rest
- Often delay in presentation (weeks to months)
- Athletes: recent increase in training intensity
- May recall specific incident when "stress" became "complete"
Examination
- Swelling over dorsum of midfoot
- Ecchymosis (body fractures)
- May appear grossly normal (stress fractures)
- Assess overall foot alignment
- N spot - focal tenderness over navicular body (dorsal, medial, plantar)
- Tuberosity tenderness (posterior tibial tendon insertion)
- Assess adjacent joints (talonavicular, cuneonavicular)
- Single-leg hop test (stress fractures) - reproduces pain
- Navicular compression test
- Assess posterior tibial tendon function
- Assess hindfoot alignment
Navicular Stress Fracture Sign: The "N spot" is focal tenderness over the proximal dorsal navicular at the junction of the proximal and middle thirds - this is the site of stress fractures in the watershed zone.
Sensitivity: 81% Specificity: 100%
If N spot tenderness present in an athlete with activity-related midfoot pain, pursue advanced imaging even with negative X-rays.
Differential Diagnosis
- Distinguishing Features
- N-spot tenderness, insidious onset, athlete with high running load
- Key Investigation
- MRI (oedema) then CT (sagittal central line)
- Distinguishing Features
- Pain without a fracture line; bone-marrow oedema only
- Key Investigation
- MRI - oedema, no cortical break
- Distinguishing Features
- Pain/tenderness along tendon and tuberosity, weak inversion, planovalgus
- Key Investigation
- Ultrasound or MRI of tendon
- Distinguishing Features
- Medial bony prominence, tenderness at accessory ossicle, often bilateral
- Key Investigation
- X-ray (oblique), MRI for synchondrosis oedema
- Distinguishing Features
- Plantar ecchymosis, pain on midfoot stress, weight-bearing films abnormal
- Key Investigation
- Weight-bearing X-ray, CT
- Distinguishing Features
- Older patient, chronic stiffness, dorsal osteophyte, reduced hindfoot motion
- Key Investigation
- Weight-bearing X-ray
- Distinguishing Features
- Child 4-7y, sclerotic/fragmented navicular, self-limiting
- Key Investigation
- X-ray; clinical age context
- Distinguishing Features
- Superficial dorsal pain, no bony tenderness on N-spot
- Key Investigation
- Ultrasound
Associated Injuries
Body fractures often occur with:
- Cuboid fractures (nutcracker injury)
- Cuneiform fractures
- Lisfranc injuries
- Talus fractures
- Chopart joint injuries
Assessment:
- Examine entire foot systematically
- Compare to contralateral side
- Document neurovascular status
- Check for compartment syndrome (rare)
The accessory navicular is the commonest accessory ossicle of the foot and a classic exam mimic of medial midfoot pain - know the Geist classification and its management:
- Type I (os tibiale externum): a small (2-3 mm) separate ossicle within the posterior tibialis tendon, proximal to the navicular - essentially a sesamoid; usually asymptomatic.
- Type II: a larger triangular ossicle joined to the navicular tuberosity by a fibrocartilaginous synchondrosis - the symptomatic type, where repetitive traction or a twist irritates the synchondrosis, causing medial midfoot pain over a bony prominence; it can also contribute to flexible flatfoot via altered PTT mechanics.
- Type III (cornuate navicular): the ossicle has fused to the navicular leaving a prominent horn; symptoms are usually from shoe pressure.
Management of the symptomatic (usually Type II): first-line activity modification, medial arch orthoses, NSAIDs and immobilisation of an acute synchondrosis injury; if refractory, surgery - the Kidner procedure (excision of the ossicle with advancement/re-routing of the posterior tibialis tendon onto the navicular), or simple excision. Distinguish it from a tuberosity fracture (the ossicle is corticated, often bilateral, at the typical accessory-ossicle site).
In a child of about 4-7 years (typically a boy) with a limp and medial midfoot pain, the diagnosis is Kohler disease - an osteochondrosis (idiopathic avascular change) of the tarsal navicular, not a fracture:
- It reflects the navicular being the last tarsal bone to ossify, leaving it vulnerable to compressive ischaemia at the watershed central zone during this period.
- Radiographs show a sclerotic, flattened, fragmented ("disc-like") navicular; comparison with the other foot and the clinical age context make the diagnosis.
- It is self-limiting with an excellent prognosis - the navicular reconstitutes to a normal shape with growth and does NOT cause long-term deformity or arthritis.
- Management is reassurance and symptomatic: activity modification and, for significant pain, a short period (a few weeks) in a walking cast or boot to shorten the symptomatic course; surgery is never indicated.
Contrast with Mueller-Weiss disease (spontaneous AVN of the navicular in middle-aged adults), which is progressive, causes deformity and arthritis, and is a different, non-self-limiting entity.
Investigations
Imaging Protocol
- AP, lateral, oblique views
- Body fractures usually visible
- Stress fractures often negative initially (up to 70%)
- Look for subtle cortical break or sclerosis
- Essential for body fractures - surgical planning
- Assess articular displacement
- Identify comminution pattern
- Evaluate adjacent injuries
- Sangeorzan classification confirmed
- Gold standard for stress fractures
- T2 bone marrow edema before cortical break
- 97% sensitivity for stress fractures
- Also evaluates soft tissue injury
- Alternative to MRI for stress fractures
- Highly sensitive (early uptake)
- Less specific than MRI
- "Hot" navicular in stress fracture/reaction
Imaging Findings
- Fracture pattern (Sangeorzan type)
- Articular step-off measurement
- Comminution assessment
- Medial column length
- T1: Low signal linear fracture line
- T2/STIR: High signal bone marrow edema
- Location: Central third, sagittal orientation
- Assess for complete vs partial fracture
Choose based on fracture type:
- Body fractures: CT for surgical planning
- Stress fractures: MRI for diagnosis and staging
- Both: May be needed for complete evaluation
CT shows bone detail; MRI shows stress reaction before cortical break.
Management Algorithm

Body Fracture Management
- Non-displaced fractures (less than 1mm articular step-off)
- No medial column shortening
- Stable fracture pattern
- Patient able to comply with restrictions
- Short leg cast, non-weight-bearing for 6-8 weeks
- X-rays at 2, 4, 6 weeks to assess alignment
- CT at 6 weeks to confirm union
- Transition to weight-bearing boot at 8-10 weeks
- Progressive rehabilitation
- Displacement greater than 1mm articular step-off
- Medial column shortening
- Unstable fracture pattern (Sangeorzan 2 and 3)
- Open fracture
- Associated midfoot injuries requiring surgery
- High-demand patient
- Inability to comply with non-weight-bearing
Fixation Options:
- Screws: 3.5mm or 4.0mm cortical lag screws
- K-wires: Temporary or definitive for small fragments
- Mini-fragment plates: 2.0-2.4mm for comminuted fractures
- Bridge plating: Talonavicular to cuneiforms for severe comminution
- External fixation: Severely comminuted with soft tissue compromise
Choice depends on fracture pattern and comminution degree.
FIXATION
Surgical Principles for Navicular Fractures
Hook:FIXATION principles guide surgical treatment of navicular body fractures
Surgical Technique
Preoperative Planning
Essential Steps:
- Review CT scan for fracture pattern and comminution
- Assess soft tissue envelope - may need staged surgery
- Plan approach based on fracture location
- Prepare for bone grafting if comminution present
Patient Positioning
- Supine with bump under ipsilateral hip
- Thigh tourniquet
- Image intensifier positioned for AP and lateral views
Thorough planning ensures optimal surgical execution.
Complications
Common Complications
- Wound dehiscence
- Infection
- Hardware prominence
- Neurovascular injury
- Compartment syndrome (rare)
- Avascular necrosis (25%)
- Nonunion (especially stress fractures)
- Malunion and planovalgus
- Post-traumatic arthritis
- Chronic pain
Avascular Necrosis
- Sangeorzan Type 2 and 3 fractures
- Delayed treatment
- Open reduction with extensive soft tissue stripping
- Associated injuries disrupting blood supply
- Persistent pain despite apparent healing
- Progressive collapse on imaging
- Sclerosis followed by fragmentation
- Early: Protected weight-bearing, may revascularize
- Established AVN with collapse:
- Bone grafting (vascularized or non-vascularized)
- Talonavicular fusion
- Triple arthrodesis (severe cases)
Nonunion
- Central stress fractures (watershed zone)
- Inadequate immobilization
- Smoking
- Delayed diagnosis
- Poor blood supply
- Bone stimulator (electrical/ultrasound)
- Surgical fixation with bone grafting
- Consider vascularized bone graft for resistant cases
Malunion
- Medial column shortening → planovalgus deformity
- Talonavicular arthritis
- Altered gait mechanics
- Chronic midfoot pain
- Osteotomy and bone grafting (rarely successful)
- Typically requires talonavicular fusion
- May need triple arthrodesis for severe deformity
Postoperative Care
Immediate Postoperative Period (0-2 weeks)
- Posterior splint, strict elevation above heart
- Non-weight-bearing with crutches
- Ice and analgesia
- Neurovascular checks
- DVT prophylaxis if high risk
- Maintain non-weight-bearing status
- Keep splint dry and clean
- Elevation as much as possible
- Watch for excessive pain, swelling, numbness
Early Phase (2-6 weeks)
- Wound check, suture removal
- Convert to short leg cast or CAM boot
- Continue strict non-weight-bearing
- Begin ankle pumps and toe exercises
- X-rays to assess alignment
- Continue non-weight-bearing
- If stable, may begin gentle ankle ROM in boot
- X-rays to assess early healing
- CT if healing questionable
- Continue non-weight-bearing until bridging callus seen
Mid Phase (6-12 weeks)
- If healing progressing, begin progressive weight-bearing
- Weight-bearing as tolerated in boot
- Physical therapy: ROM, proprioception
- Pool therapy if available
- Transition to supportive shoe
- Continue progressive weight-bearing
- Advance strengthening exercises
- Address gait abnormalities
Late Phase (3-6 months)
- Full weight-bearing in supportive footwear
- Sport-specific rehabilitation begins
- Impact activities avoided
- Gradual return to running (if athlete)
- Sport-specific drills
- Full return to sport if pain-free and full ROM
- Hardware removal if prominent (rarely needed)
Red Flags During Recovery
- Persistent pain despite adequate healing time - consider AVN
- Loss of reduction on serial X-rays - may need revision
- No progression of healing at 12 weeks - nonunion risk
- Wound complications - infection risk
- Progressive collapse on imaging - AVN developing
Return to Sport Criteria
- Pain-free weight-bearing and walking
- Full or near-full ROM compared to contralateral
- Radiographic union (bridging callus on CT)
- Successful completion of sport-specific drills
- Single-leg hop test equal to contralateral
- Psychological readiness
- Office workers: 8-12 weeks
- Manual laborers: 12-16 weeks
- Athletes (non-impact): 4-6 months
- Athletes (impact/running): 6-9 months
Outcomes and Prognosis
Overall Outcomes by Fracture Type
Good-Excellent Outcomes: 70-85%
- Type 1 (coronal): 85-90% good outcomes
- Type 2 (oblique): 70-80% good outcomes
- Type 3 (comminuted): 50-60% good outcomes
- AVN rate: 16-25%
- Arthritis rate: 20-30% at 5 years
Union Rate: 86-95% with early treatment
- Partial fractures: 95% union
- Complete non-displaced: 85-90% union
- Central location: Higher nonunion rate
- Return to sport: 80-90% of athletes
- Recurrence rate: 10-15%
Prognostic Factors
- Early diagnosis and treatment (within 2 weeks)
- Anatomic reduction achieved
- Non-displaced or minimally displaced fractures
- Peripheral location (stress fractures)
- Younger age
- Non-smoker
- Good compliance with rehabilitation
- Delayed treatment (beyond 3 weeks)
- Sangeorzan Type 3 (comminuted)
- Severe articular damage
- Associated injuries (cuboid, cuneiforms)
- Central stress fracture location
- Smoking
- Poor soft tissue envelope
Functional Outcomes
- Sedentary work: 8-12 weeks
- Light manual work: 12-16 weeks
- Heavy manual work: 16-24 weeks
- Low-impact activities: 3-4 months
- Running/jumping sports: 6-9 months
- Elite athletes: May require 9-12 months
- 10-20% of athletes unable to return to pre-injury level
Long-Term Complications
- Post-traumatic arthritis: 20-40% (body fractures)
- Chronic pain: 15-25%
- Reduced activity level: 20-30%
- Need for fusion surgery: 5-10%
- Develops within first 2 years post-injury
- May revascularize in 30% of cases
- Progressive collapse in 50-70% if severe
- Often requires salvage fusion procedures
Quality of Life
Key messages for patients:
-
Body fractures: "Most patients do well with surgery, but there is a 1 in 4 chance of blood supply problems (AVN) and a 1 in 5 chance of arthritis developing over time."
-
Stress fractures: "With strict rest for 6-8 weeks, 9 out of 10 athletes heal and return to sport. The bone heals slowly because of limited blood supply."
-
Time off sport: "Expect 6-9 months before full return to impact sports. Rushing increases risk of re-fracture or failure to heal."
Guidelines, Registries & Global Practice
Global Epidemiology
Navicular fractures are uncommon. Across published series the navicular accounts for only a small fraction of foot fractures, with body fractures usually following high-energy axial loading and stress fractures clustering in running and jumping athletes. There is no dedicated international registry for navicular fractures (unlike arthroplasty), so the evidence base is built from case series and a single meta-analysis rather than registry data.
- Figure
- 86% vs 26% for weight-bearing
- Source (PubMed)
- Khan 1992 (PMID 1456359)
- Figure
- 96% vs 82% (NS; WB inferior)
- Source (PubMed)
- Torg 2010 (PMID 20197494)
- Figure
- 67% / 19% / 14%
- Source (PubMed)
- Sangeorzan 1989 (PMID 2592390)
- Figure
- 100% union, 4% avascular collapse
- Source (PubMed)
- Evans 2011 (PMID 21733456)
- Figure
- Type I/II ~3.7 mo, Type III ~6.8 mo
- Source (PubMed)
- Saxena 2000/2006 (PMID 10789100, 17144953)
Guideline & Society Positions
No single national body publishes a stand-alone navicular-fracture guideline; recommendations are drawn from foot-and-ankle society consensus, AO principles and the sports-medicine literature. The table below summarises the practical position of the major bodies.
- Position
- Restore medial column length and articular congruity; lag screws for simple patterns, bridge/minifragment plating for comminution
- Evidence level
- Expert consensus / Level IV-V
- Position
- CT for surgical planning of body fractures; ORIF for displacement greater than 1-2mm or medial column shortening
- Evidence level
- Expert opinion
- Position
- Open midfoot injuries follow BOAST open-fracture and dislocated/deformed-limb standards (early reduction, prompt senior review)
- Evidence level
- Standard of care
- Position
- CT mandatory for body fractures; medial-column preservation is the key prognostic target
- Evidence level
- Expert consensus
- Position
- Non-weight-bearing immobilisation is standard of care for stress fractures; surgery for Type III / failed conservative
- Evidence level
- Level III meta-analysis (Torg 2010)
Registry & Practice Variation
- No arthroplasty-style registry captures navicular fractures, so practice variation is large and outcome data come from single-centre series.
- Stress-fracture management has converged internationally on strict non-weight-bearing immobilisation following Khan 1992 and the Torg 2010 meta-analysis; however, real-world audits (e.g. Burne 2005, PMID 16157855) show many patients still do not receive guideline non-weight-bearing treatment, and only about half of those return to their previous sporting level.
- Body-fracture fixation varies between independent lag screws and minifragment/bridge plating depending on comminution and surgeon preference; both achieve high union when medial column length is restored.
- Return-to-running and bone health are integral to stress-fracture care worldwide: once imaging confirms union, athletes progress through structured, graded load-progression (return-to-running) protocols, and recurrent stress fractures prompt systematic bone-health screening (energy availability, vitamin D and menstrual function) to correct underlying risk factors before return to full loading.
Viva Scenarios
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 25-year-old track athlete presents with 6 weeks of worsening midfoot pain during running. The pain localizes to the dorsum of the foot over the navicular. X-rays appear normal.”
“A 35-year-old man is brought to ED after a motorcycle accident. He has a swollen, deformed midfoot. X-rays show a displaced navicular body fracture with associated cuboid fracture. CT shows a Sangeorzan Type 2 pattern with 5mm of medial column shortening.”
“A 30-year-old athlete is 4 months post-operatively from navicular body fracture ORIF. She has persistent midfoot pain. X-rays show sclerosis and partial collapse of the navicular. What is your diagnosis and management?”
MCQ Practice Points
High-Yield Facts for MCQs
Q: A young athlete has vague midfoot pain but normal X-rays. What is the next step? A: MRI - X-rays are negative in 70% of early stress fractures. MRI is the gold standard (97% sensitive) showing bone marrow edema before a cortical break appears.
Q: What is the 'N-Spot' and what does it signify? A: Dorsal Navicular Tenderness - Located at the junction of the proximal and middle thirds. It is 81% sensitive and 100% specific for navicular stress fractures.
Q: Why do central navicular fractures have a high nonunion rate? A: Poor Vascularity - The central third is a watershed zone between the dorsalis pedis and medial plantar arterial supplies. This tenuous blood supply impairs healing.
Q: Which Sangeorzan type is the most common? A: Type 2 - The fracture line runs from dorsomedial to plantar-lateral. It results in forefoot medialization and dorsal displacement, requiring ORIF to restore length.
Q: What is the critical management principle for navicular stress fractures? A: Variables: Strict NWB vs Surgery - Conservative management requires 6-8 weeks of strict non-weight-bearing in a cast. Weight-bearing leads to nonunion or recurrence.
Q: When is surgery indicated for a navicular body fracture? A: Greater than 1mm Displacement - Any articular step-off greater than 1mm or loss of medial column length warrants ORIF to prevent post-traumatic arthritis and deformity.
At a Glance Table
- Avulsion
- 47% (most common)
- Body
- 26%
- Stress
- 3%
- Tuberosity
- 24%
- Avulsion
- Capsule avulsion
- Body
- High-energy axial load
- Stress
- Repetitive loading
- Tuberosity
- PTT avulsion/direct trauma
- Avulsion
- Any age, low energy
- Body
- 20-40 years, trauma
- Stress
- Athletes (track/basketball)
- Tuberosity
- Older patients or trauma
- Avulsion
- X-rays sufficient
- Body
- CT essential for planning
- Stress
- MRI gold standard
- Tuberosity
- X-rays, CT if large
- Avulsion
- Conservative if small
- Body
- ORIF if displaced over 1mm
- Stress
- NWB 6-8 weeks
- Tuberosity
- ORIF if large/displaced
- Avulsion
- Very low
- Body
- 25% (high)
- Stress
- Variable (central worse)
- Tuberosity
- Low
- Avulsion
- Rare
- Body
- Moderate
- Stress
- High (central location)
- Tuberosity
- Low
- Avulsion
- 6-8 weeks
- Body
- 4-6 months
- Stress
- 4-6 months
- Tuberosity
- 8-12 weeks
- Avulsion
- Excellent
- Body
- Good-Fair (type dependent)
- Stress
- Good if early treatment
- Tuberosity
- Good
NAVICULAR
Key Features of Navicular Fractures
Hook:The NAVICULAR is critical for arch support but has fragile blood supply
SANGEORZAN
Body Fracture Classification
Hook:Types 1-2-3: Coronal-Oblique-Comminuted (increasing severity)
STRESS
Navicular Stress Fracture Features
Hook:STRESS fractures need REST - 6-8 weeks non-weight-bearing
Evidence Base
Sangeorzan Classification of Navicular Body Fractures (1989)
- 21 displaced body fractures treated with ORIF over 1980-1987, classified into 3 types by fracture-line direction and forefoot displacement (Type 1 coronal, no forefoot angulation; Type 2 dorsal-lateral to plantar-medial with medial forefoot displacement; Type 3 sagittal comminution with lateral forefoot displacement). Satisfactory reduction achieved in 100% of Type 1, 67% of Type 2 and 50% of Type 3. Good result in 67%, fair in 19%, poor in 14%. Fracture type and accuracy of reduction both correlated directly with outcome.
Conservative vs Surgical Management of Navicular Stress Fractures (Khan, 1992)
- 82 athletes with 86 CT-confirmed navicular stress fractures. 19 of 22 (86%) treated with at least 6 weeks of non-weight-bearing cast immobilisation returned to sport, versus only 9 of 34 (26%) who continued weight-bearing with activity restriction (p less than 0.001). CT appearance of healing did not reliably mirror clinical union.
NWB vs Surgery for Navicular Stress Fracture - Meta-analysis (Torg, 2010)
- Systematic review and mixed-model meta-analysis comparing three strategies. Non-weight-bearing conservative treatment gave 96% successful outcomes versus 82% for surgery, with no statistically significant difference (p=0.64) but a trend favouring NWB. Weight-bearing conservative treatment was significantly inferior to both NWB (p=0.0001) and surgery (p less than 0.0003).
CT-Based Classification of Navicular Stress Fractures (Saxena, 2000)
- 22 navicular stress fractures with a proposed frontal-plane CT classification: Type I dorsal cortical break, Type II propagation into the body, Type III propagation through a second cortex. Type III took significantly longer to return to activity (mean 6.8 months) than Type I (3.0) or Type II (3.6). Operative cases returned faster than conservative (3.1 vs 4.3 months, p=0.02). Sclerotic margins were associated with persistent symptoms.
Prospective Study of Navicular Stress Fractures (Saxena, 2006)
- Prospective series of 19 athletes (compared with 22 historical controls). Mean return to activity was 4.0 months across all CT types, with no major difference between Type I (3.8), Type II (3.7) and Type III (4.2) when treated per protocol (non-op for Type I, ORIF for Type II/III). 15 of 16 competitive athletes returned to full competition, including all who had ORIF.
Bridge Plating of the Medial Column in Midfoot Injuries (Schildhauer, 2003)
- Describes temporary internal bridge plating of the medial column with an 8-10 hole 2.7mm reconstruction plate spanning the talar neck to the first metatarsal for severe comminuted midfoot (cuneiform/navicular) crush injuries, maintaining medial column length and alignment until union, as an alternative to spanning external fixation.
Minifragment Plate Fixation of High-Energy Navicular Body Fractures (Evans, 2011)
- 24 navicular body fractures treated with minifragment plate ORIF at a Level I trauma centre. All fractures united with no loss of reduction and no deep infection. Only 1 patient (4%) developed radiographic avascular collapse; 4 (17%) developed talonavicular arthrosis and 4 (17%) required removal of prominent hardware.
Tarsal Navicular Stress Fractures - Original Series (Torg, 1982)
- Foundational retrospective review of 21 tarsal navicular stress fractures in athletes. Established that the diagnosis is frequently delayed because routine radiographs are often normal, that the fracture characteristically lies in the central third in a sagittal plane, and that immobilisation with non-weight-bearing was more reliable than continued activity.