High-Risk Tarsal Stress Injury | Central Third Watershed | Athlete Foot Pain
- Navicular stress fracture is a high-risk stress fracture with delayed/nonunion potential
- Central third is a vascular watershed - medial and lateral blood supplies meet but do not anastomose robustly
- X-ray is frequently normal; MRI is the most sensitive first test, CT confirms and grades
- Tenderness on the 'N-spot' (dorsal proximal navicular) is the key clinical sign
- Treatment hinges on NWB immobilisation for incomplete fractures, headless compression screw for complete/displaced
- “Most common tarsal stress fracture; most common cause of midfoot pain in athletes with normal X-ray
- “Vague, insidious midfoot pain is the rule - high index of suspicion needed
- “Single-leg hop reproduces pain in nearly all cases
- “Screw trajectory: lateral-to-medial across the fracture in the proximal-distal plane
- “Nonunion risk driven by watershed biology, not by athlete compliance
- Diagnosis
- MRI oedema, CT confirms dorsal-cortex fracture
- Treatment
- NWB cast 6-8 weeks for Type I incomplete
- Key Pearl
- X-ray often normal - do not be falsely reassured
- Diagnosis
- CT shows fracture extending into body (Type II)
- Treatment
- Headless compression screw, percutaneous
- Key Pearl
- Screw from lateral to medial, central in both planes
- Diagnosis
- CT or MRI shows fracture into opposite cortex (Type III)
- Treatment
- ORIF with screw and bone graft, NWB post-op
- Key Pearl
- Address cavovarus or limb-length risk factors
RISKYWhy Navicular Stress Fracture Is High-Risk
Hook:RISKY - navicular stress fracture sits in the high-risk tier because of the watershed biology and easy X-ray miss.
SPOT HOPThe N-Spot and Hop Test
Hook:SPOT the HOP - locate the N-spot and use the single-leg hop to provoke the pain before imaging.
LATERALScrew Fixation Principles
Hook:LATERAL - start laterally, aim medially, headless compression screw through the central third.
Overview and Epidemiology
The navicular is the most common tarsal bone to sustain a stress fracture and one of the four classic high-risk stress fractures. Because the central third is a vascular watershed and the initial X-ray is normal in the majority of cases, the diagnosis is missed in up to 80 percent of patients at first presentation. Vague, activity-related midfoot pain in a running, jumping, or cutting athlete must prompt an N-spot examination, a hop test, and MRI even when the X-ray looks normal.
- Sprinters, hurdlers, middle-distance runners: highest incidence in track and field
- Jumpers: basketball, netball, ballet, gymnastics
- Cutting sport athletes: football, soccer, rugby
- Military recruits: high volume of repetitive impact loading during basic training
- Return-to-sport time: 4-6 months even with optimal care
- Re-fracture rate: up to 10 percent after apparent union
- Career impact: documented in elite athletes; may end professional careers if mismanaged
- Diagnostic delay: typical delay 4-7 months from symptom onset - most common cause of poor outcome
Navicular stress fracture represents approximately 15-35 percent of all stress fractures in athletes and is the most common tarsal stress fracture. In a large military cohort, navicular stress fractures accounted for the longest average time to return to duty of any lower-extremity stress fracture.
Pathophysiology
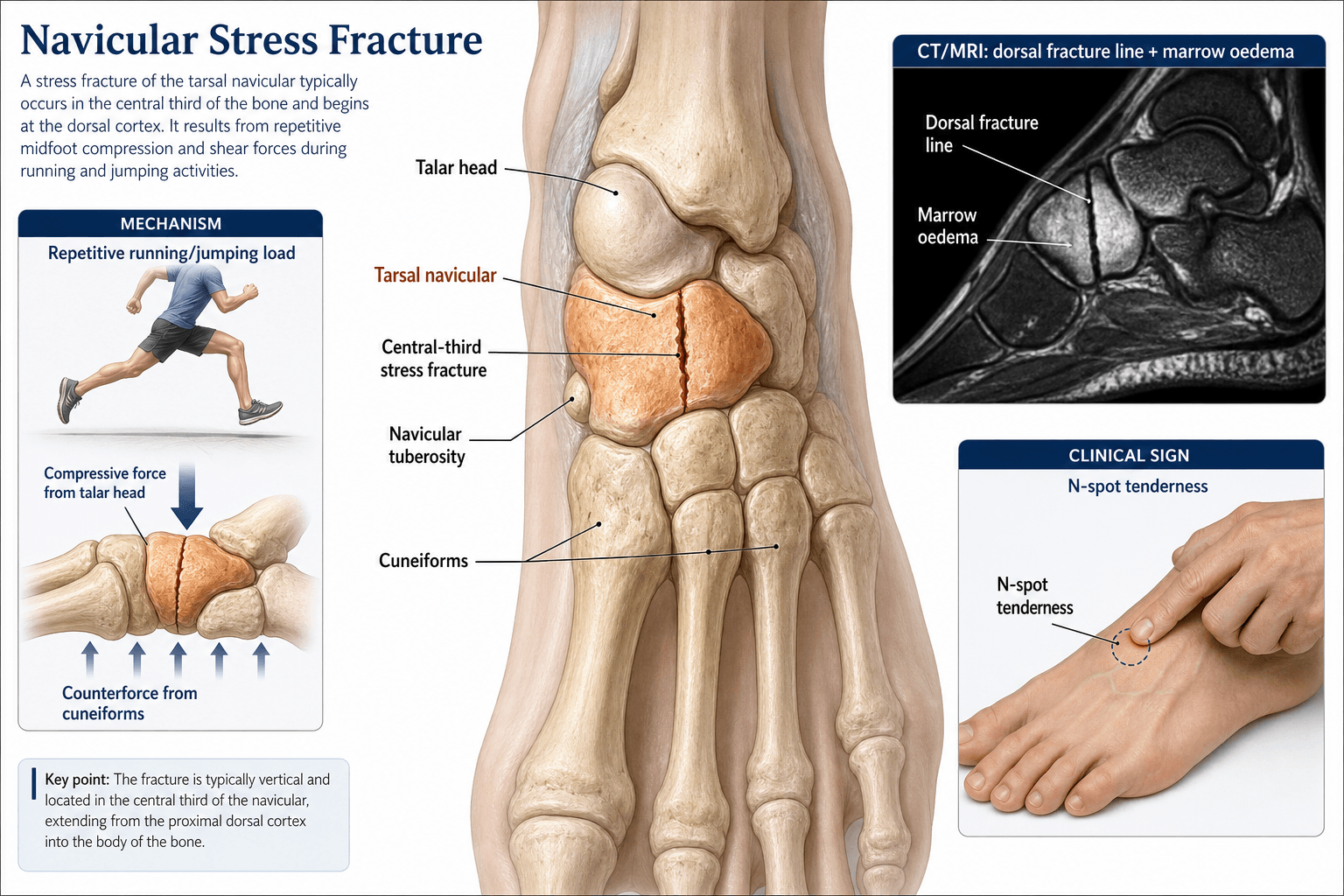
The central third of the navicular is a vascular watershed. The medial half is perfused by branches of the posterior tibial artery, and the lateral half is perfused by branches of the dorsalis pedis artery. These two systems converge at the central third but do not form a rich anastomotic network. Repetitive impaction of this hypovascular zone outstrips repair. Microdamage accumulates, a sagittal-plane fatigue fracture begins on the dorsal cortex (the compression side of the bending moment), and propagates proximally to distally. Because the biology of repair is limited, even a recognised fracture heals slowly, and unrecognised fractures progress to complete or displaced patterns.
- Blood supply
- Posterior tibial artery branches
- Mechanical role
- Articulates with medial cuneiform, tibialis anterior insertion
- Pathologic consequence
- Robust healing potential
- Blood supply
- Watershed - limited collateral supply
- Mechanical role
- Bears compressive load at apex of medial longitudinal arch
- Pathologic consequence
- Stress fracture, delayed/nonunion
- Blood supply
- Dorsalis pedis artery branches
- Mechanical role
- Articulates with lateral cuneiform, cuboid stability
- Pathologic consequence
- Robust healing potential
Repetitive loading: cumulative impact cycles in running, jumping, and cutting
Arch mechanics: navicular is the keystone of the medial longitudinal arch; the central third is the apex of bending
Ground reaction force: 2-3 times body weight during running, higher in jumping
Cavovarus foot: lateral column overload concentrates stress at the navicular
Watershed zone: central third has the lowest vascular density
Cortical geometry: dorsal cortex thinner than plantar in many specimens
Intramedullary pressure: relatively low, limiting endosteal healing
Reparative response: limited periosteal callus in cortical bone
The fracture characteristically begins on the dorsal cortex and runs in the sagittal plane (proximal-distal direction) across the central third. The dorsal start point reflects the compression side of the bending moment; the sagittal direction reflects the orientation of the watershed zone. A short, dorsal, partial fracture is the hallmark of an early stress injury.
Classification and Types

Saxena CT Classification (Most Widely Used)
- Fracture pattern
- Dorsal cortex fracture only, incomplete
- Treatment
- NWB cast 6-8 weeks
- Healing prognosis
- High union rate with offloading
- Fracture pattern
- Fracture extends into navicular body
- Treatment
- Operative fixation recommended
- Healing prognosis
- Good union with surgery
- Fracture pattern
- Fracture into opposite (plantar) cortex, displaced or comminuted
- Treatment
- ORIF, possible bone graft
- Healing prognosis
- Variable, depends on displacement and graft use
Saxena classification is based on CT appearance and is the most useful treatment-stratification tool. Both knees and ankles of the patient are usually scanned, and the contralateral side is often used to plan screw length.
Clinical Assessment
- Sport and training load: sprinting, jumping, cutting, sudden mileage increase
- Symptom onset: insidious, gradual, often weeks to months before presentation
- Pain character: vague midfoot or dorsal midfoot ache, worse with push-off
- Relief: pain settles with rest but recurs when training resumes
- Prior treatment: many have already had physiotherapy, orthotics, or imaging
- N-spot tenderness: dorsal proximal navicular, between tibialis anterior and extensor hallucis longus - positive in almost all cases
- Single-leg hop test: hop on the affected foot reproduces pain - highly sensitive
- Pain on tiptoe: standing on tiptoe or hopping on the affected foot reproduces pain
- Gait: antalgic or shortened push-off in established cases
- Foot posture: assess for cavovarus, planovalgus, limb-length discrepancy
The N-spot is the dorsal aspect of the proximal navicular, palpated with the thumb between the tibialis anterior and extensor hallucis longus tendons. Firm thumb pressure reproduces the patient's pain in the majority of cases. Tenderness is occasionally bilateral; compare to the contralateral side. The single-leg hop test (hop on the affected foot in place) reproduces pain in nearly every symptomatic athlete and is the most useful provocative bedside test.
- Pain location
- Dorsal proximal midfoot, 'N-spot'
- Discriminating finding
- Hop test positive, N-spot tender
- Best confirmatory test
- MRI (oedema), CT (fracture line)
- Pain location
- Medial ankle and arch
- Discriminating finding
- Pain on resisted inversion, arch collapse
- Best confirmatory test
- Ultrasound, MRI of tendon
- Pain location
- Medial midfoot, between navicular and sustentaculum
- Discriminating finding
- Medial arch collapse, valgus heel
- Best confirmatory test
- MRI with attention to ligament
- Pain location
- Medial navicular tuberosity
- Discriminating finding
- Bony prominence, tender over accessory ossicle
- Best confirmatory test
- Plain X-ray, MRI for oedema
- Pain location
- Dorsal midfoot, multiple joints
- Discriminating finding
- Stiffness, crepitus, prior injury
- Best confirmatory test
- Weight-bearing X-ray, CT
- Pain location
- Tarsometatarsal region
- Discriminating finding
- Pain on stress testing, swelling, inability to hop
- Best confirmatory test
- Weight-bearing X-ray, MRI
- Pain location
- Rigid flatfoot, peroneal spasm
- Discriminating finding
- Restricted subtalar motion, pes planus
- Best confirmatory test
- CT or MRI of hindfoot
A subtle Lisfranc injury can mimic a navicular stress fracture. Both cause midfoot pain, both can present after a low-energy twisting episode, and both can produce pain on single-leg hop. Weight-bearing X-rays (or a weight-bearing CT) and a careful examination of the tarsometatarsal joints are essential to avoid a missed Lisfranc.
Investigations
Imaging Protocol
Views: AP, lateral, and oblique of the foot
Look for: Sclerotic line in the central third, cortical break on the dorsal aspect, cyst formation, dorsal exostosis in chronic cases
Clinical correlation: Normal in 70-80 percent of acute navicular stress fractures; never rely on a normal X-ray to exclude the diagnosis
Indication: First imaging study of choice in a symptomatic athlete with normal X-rays
Protocol: Fat-suppressed T2 or STIR sequences detect marrow oedema; T1 detects the fracture line
Findings: Marrow oedema in the central third, sagittal-plane fracture line on T1
Sensitivity: approaches 100 percent for stress fracture
Indication: Required to grade by Saxena and plan treatment
Protocol: Fine-cut (1 mm) CT in the plane of the navicular body, coronal and sagittal reformats
Findings: Dorsal-cortex break, fracture extent, displacement, sclerosis at the margins (nonunion), cyst formation
Use: Drives decision between non-operative and operative management
Indication: Recurrent stress fractures, female athlete triad features, low BMI
Tests: DEXA scan, vitamin D, calcium, parathyroid hormone, oestradiol, menstrual history
Rationale: Identify and address the systemic component of stress injury
The standard sequence in a high-performance athlete with vague midfoot pain is X-ray, then MRI if X-ray is normal, then CT if MRI is positive. Skipping the CT leads to an inability to grade the fracture and uncertainty about whether surgical fixation is required. Skipping the MRI in a high-risk scenario (high-performance sprinter, persistent pain despite NWB) risks missing the diagnosis entirely.
- Strength
- Cheap, available, detects established fracture
- Weakness
- Misses most early fractures
- Role
- First-line, not sufficient alone
- Strength
- Most sensitive, detects bone stress reaction
- Weakness
- Cannot always grade fracture
- Role
- First test after normal X-ray
- Strength
- Best for fracture morphology and union
- Weakness
- Cannot show oedema; radiation dose
- Role
- After positive MRI - drives management
- Strength
- Peritendinous oedema, tibialis posterior
- Weakness
- Limited value for navicular itself
- Role
- Adjunct, not primary
- Strength
- Highly sensitive
- Weakness
- Poor specificity, no anatomic detail
- Role
- Largely replaced by MRI
Differential Diagnosis
Activity-related midfoot/medial arch pain in an athlete has a broad differential. The navicular stress fracture is the diagnosis not to miss.
- Key features
- Insidious midfoot pain, positive 'N spot', often normal early X-ray
- Distinguishing point
- Sagittal central-body line on MRI/CT; high-risk for nonunion
- Key features
- Medial pain/swelling along tendon, weak single-heel-rise, progressive flatfoot
- Distinguishing point
- Tenderness along the tendon, not focal over the navicular
- Key features
- Medial prominence, pain at tuberosity, often bilateral
- Distinguishing point
- Ossicle at medial tuberosity on imaging; chronic, not a sagittal body line
- Key features
- Dorsal midfoot pain, stiffness, older or post-injury
- Distinguishing point
- Joint-space narrowing/osteophytes on weight-bearing X-ray
- Key features
- Child with limp and medial midfoot pain
- Distinguishing point
- Sclerotic, flattened navicular in a child; self-limiting osteochondrosis
- Key features
- Activity-related forefoot/midfoot pain
- Distinguishing point
- Localising tenderness and MRI/CT site differ
Management Algorithm
Non-Operative Management (Type I Incomplete Dorsal-Cortex Fracture)
Goal: Offload the watershed zone, allow biological union, prevent progression to complete fracture
Treatment Protocol
Cast or boot: Below-knee walking cast in neutral or NWB cast; many surgeons use a removable boot for hygiene
Crutches: Strict NWB for a minimum of 2 weeks in cast
Analgesia: Paracetamol; avoid NSAIDs in early healing (theoretical effect on bone healing)
Education: Explain the watershed biology, the high-risk status, and the 6-8 week offloading requirement
NWB cast: Continue for a total of 6-8 weeks
Re-imaging: CT at 6 weeks to assess union before allowing weight-bearing
Nutrition: Calcium, vitamin D, adequate protein; investigate relative energy deficiency in sport (RED-S) in thin athletes
Address risk factors: cavovarus assessment, training error review, footwear review
Repeat CT: Look for bridging callus across the fracture
If union: gradual return to weight-bearing in boot, then to activity
If no union: consider bone stimulator, prolonged casting, or conversion to operative fixation
Phase 1 (weeks 8-12): protected weight-bearing, low-impact cross-training, swimming, cycling
Phase 2 (weeks 12-16): walk-jog progression on flat ground, intrinsic foot strengthening
Phase 3 (weeks 16-24): graduated return to running, sport-specific drills
Return to full sport: when pain-free hop, no N-spot tenderness, and CT-confirmed union
Weight-bearing through an incomplete dorsal-cortex fracture propagates the fracture line. The most common reason for nonunion is a partially compliant athlete who bears weight in the boot. Treat Type I fractures with the same respect as Type II: NWB cast for 6-8 weeks and confirm union with CT before any return to running.
The aggressive treatment of the navicular only makes sense within the high-risk vs low-risk stress-fracture framework examiners love:
- High-risk stress fractures occur on the tension side or in a watershed/poorly-vascularised zone, so they tend to progress, displace, go to nonunion or AVN, and need aggressive treatment (strict non-weight-bearing and/or internal fixation, with imaging-confirmed union before return). The classic list: tarsal navicular, femoral neck (tension/superior side), anterior tibial cortex ("dreaded black line"), medial malleolus, proximal fifth metatarsal (Jones, zone 2), great-toe (hallux) sesamoid, and talar neck/body.
- Low-risk stress fractures (compression-side, well-vascularised: femoral-neck compression side, posteromedial tibial shaft, metatarsal shafts 2-4, calcaneus, distal fibula) usually heal with relative rest and activity modification.
The navicular sits squarely in the high-risk group because of its central-third watershed and dorsal-tension geometry - which is exactly why a "minor" incomplete dorsal-cortex fracture is treated like a true fracture.
Exam point: classify any stress fracture as high-risk (tension/watershed -> NWB +/- fixation, confirm union) or low-risk (compression/well-vascularised -> activity modification); the navicular, femoral-neck-tension, anterior-tibial, medial-malleolar, Jones, sesamoid and talar fractures are the high-risk ones to name.
A navicular stress fracture is a biomechanical and metabolic warning sign, and fixing the bone without finding the cause invites recurrence (and a fracture on the other foot). Work it up on two axes:
- Mechanical / structural: examine for a cavovarus foot, hindfoot varus, a plantarflexed first ray, equinus, and limited subtalar/midfoot motion that overload the medial column and navicular; assess footwear and prescribe orthotics to offload, and consider deformity correction for a true cavovarus foot. A cavovarus foot should also prompt a peripheral-neuropathy screen (Charcot-Marie-Tooth).
- Metabolic / load: screen for relative energy deficiency in sport (RED-S) / the athlete triad (low energy availability, menstrual dysfunction, low BMD), check vitamin D and calcium, and review training-load error (rapid increase, hard surfaces) - these drive both the index fracture and the recurrence.
- Bilateral and recurrence: these fractures are frequently bilateral and recurrent, so have a low threshold to image the contralateral foot and to counsel the athlete that return must be graded and cause-corrected.
Exam point: a navicular stress fracture mandates a secondary-cause workup - correct the cavovarus/foot-overload mechanics (and screen for CMT), optimise bone health/RED-S and training load, and consider imaging the other foot - or it will recur.
Surgical Technique
Percutaneous Screw Fixation (Preferred)
Indications:
- Failed conservative treatment
- Displaced fracture
- Complete fracture with sclerosis
Technique:
- Exposure: Medial stab incision near the navicular tuberosity
- Guidewire: Place from medial to lateral, perpendicular to the fracture, under fluoroscopy
- Verification: Confirm position on AP, lateral and oblique views
- Screw: Cannulated lag screw (commonly 4.0-4.5mm); single or double screws (double increasingly used for rotational control)
- Compression: Lag technique / partially threaded screw across the fracture
- Verification: Confirm reduction and hardware position fluoroscopically; avoid joint penetration
Note: For complete fractures without nonunion, percutaneous fixation is reasonable; established nonunion or sclerosis usually requires open debridement and grafting.
Complications
- Incidence
- 10-30 percent with non-operative care, lower with surgery
- Risk Factors
- Watershed biology, weight-bearing during healing, delayed diagnosis
- Management
- Compression screw with bone graft for atrophic nonunion
- Incidence
- 5-10 percent in high-level athletes
- Risk Factors
- Early return to sport, unaddressed biomechanics, RED-S
- Management
- Repeat NWB cast or surgery; correct risk factors
- Incidence
- 5-10 percent with screw fixation
- Risk Factors
- Lateral screw head prominence, low-profile not used
- Management
- Hardware removal after union confirmed
- Incidence
- Rare, more in neglected complete fractures
- Risk Factors
- Disruption of central-third watershed supply
- Management
- Arthrodesis for advanced collapse
- Incidence
- Variable, long-term
- Risk Factors
- Intra-articular fracture, prolonged immobilisation, residual deformity
- Management
- Orthotic support, arthrodesis if symptomatic
- Incidence
- 5-15 percent
- Risk Factors
- Cavovarus foot, RED-S, coexisting midfoot pathology
- Management
- Address foot posture, nutrition, training load
Up to 80 percent of navicular stress fractures are missed on first presentation, and the median diagnostic delay is 4-7 months. Every vague midfoot pain in a high-demand athlete needs an N-spot test, a hop test, and MRI if X-ray is normal. The single biggest predictor of outcome is the interval from symptom onset to definitive management.
Before any return-to-sport plan, screen every navicular stress fracture for the systemic and biomechanical drivers that may have caused the injury. The high-performance sprinter with a normal training load and a normal foot still has the diagnosis - but if the load is excessive, the foot is cavus, the oestradiol is low, or the vitamin D is depleted, the next fracture is already on its way. Address the cause, not just the bone.
Postoperative Care
Immediate Postoperative
- Immobilisation: Short leg cast or boot
- Weight bearing: Non-weight bearing (6-8 weeks)
- ROM: Ankle ROM after cast removal
- PT: Midfoot ROM and strengthening
Rehabilitation Protocol
Weeks 0-6: Short leg cast, non-weight bearing; elevation; ankle ROM exercises (if stable)
Weeks 6-8: CT to confirm healing; cast removal if healing; transition to walking boot; progressive weight bearing
Weeks 8-12: Full weight bearing; progressive activity; return to sport (3-4 months)
Outcomes and Prognosis
- Setting
- Type I incomplete dorsal fracture
- Union rate
- 85-100 percent
- Return to sport
- 4-6 months from injury
- Setting
- Complete fracture without displacement
- Union rate
- 90-100 percent
- Return to sport
- 4-6 months post-op
- Setting
- Displaced or chronic nonunion
- Union rate
- 80-95 percent
- Return to sport
- 6-9 months post-op
- Setting
- Late presentation, partial weight-bearing
- Union rate
- 30-60 percent
- Return to sport
- Often converts to surgery
- Better outcome
- Under 3 months from symptom onset
- Worse outcome
- Over 6 months - established nonunion
- Better outcome
- Type I (incomplete dorsal)
- Worse outcome
- Type III (displaced into opposite cortex)
- Better outcome
- Strict NWB for 6-8 weeks
- Worse outcome
- Partial weight-bearing during healing
- Better outcome
- None, normal foot posture, balanced nutrition
- Worse outcome
- Cavovarus, RED-S, training error, vitamin D deficiency
The single most powerful predictor of union is the time from symptom onset to definitive management. Athletes managed within 3 months of symptom onset have a high union rate with appropriate care, while those presenting after 6 months face a substantial nonunion rate regardless of the technique used. Treat the clock as well as the bone.
Guidelines, Registries & Global Practice
- Navicular stress fracture is the most common tarsal stress fracture and accounts for 15-35 percent of all stress fractures in athletic cohorts
- Highest incidence in elite sprinters, hurdlers, middle-distance runners, jumpers, and dancers; also well documented in military recruits undergoing basic training
- Mean age of presentation is in the second and third decades, with no consistent sex predominance once exposure is controlled
- Bilateral stress reaction is present in up to 25 percent of cases, often subclinical, and warrants bilateral imaging in a high-risk athlete
- High-resource centres: MRI within 24-48 hours, CT for grading, headless compression screw sets, dedicated foot and ankle surgery, athlete-specific rehabilitation
- Limited-resource settings: X-ray plus clinical examination may be the only available tools; treat on clinical suspicion with NWB cast and refer if nonunion develops
- Universal principle: outcome depends on time to diagnosis and strict NWB compliance, not on the cost of the implant
- Telemedicine and image-sharing now allow rural or overseas athletes to share MRI and CT with specialist centres for triage
- Diagnostic emphasis
- High index of suspicion in athletes; N-spot and hop test as bedside tests
- Treatment emphasis
- Stratify by CT (Saxena); NWB cast for Type I, surgery for Type II and III
- Return-to-sport gate
- CT-confirmed union, full pain-free hop, graduated running
- Diagnostic emphasis
- MRI as the imaging test of choice after normal X-ray
- Treatment emphasis
- Surgical fixation recommended for complete fractures in athletes
- Return-to-sport gate
- Symptom-free plus CT or MRI union
- Diagnostic emphasis
- MRI for early diagnosis; CT for surgical planning
- Treatment emphasis
- Operative fixation with headless compression screw and bone graft as needed
- Return-to-sport gate
- Pain-free function plus imaging-confirmed union
- Diagnostic emphasis
- Mandatory evaluation of vague midfoot pain in elite and military athletes
- Treatment emphasis
- Surgical fixation increasingly favoured for complete fractures in high-demand athletes
- Return-to-sport gate
- Graduated return with bone-strain monitoring where available
There is no dedicated registry for navicular stress fracture in the way there is for arthroplasty (NJR, AJRR, AOANJRR). The evidence base is built on retrospective series, the Saxena classification cohort, systematic reviews, and a small number of prospective diagnostic-accuracy studies. Registries of stress injuries in elite athletes and military populations (such as the Australian Defence Force and US Army bone-health programmes) increasingly inform return-to-duty decisions.
Record in every suspected navicular stress fracture:
- Mechanism (sport, training load, recent change) and time from symptom onset
- N-spot and single-leg hop test findings
- Imaging performed: X-ray, MRI (oedema, fracture line), CT (Saxena type)
- Treatment chosen: NWB cast versus surgery, with rationale linked to Saxena type
- Plan for return to sport gated on CT-confirmed union and pain-free function
- Screening for systemic drivers (vitamin D, RED-S, training error, foot posture)
A missed navicular stress fracture that progresses to nonunion is a recurring source of complaints and claims in elite and recreational sport worldwide. Document the index of suspicion, the imaging pathway, and the shared return-to-sport decision.
Controversies & Areas of Uncertainty
Some centres still attempt NWB cast immobilisation for selected Type II fractures, particularly in low-demand or skeletally immature patients. High-demand athletes increasingly receive surgical fixation because union rates are higher and return to sport is faster. The decision remains patient-centred and surgeon-dependent.
Autograft remains the standard for atrophic nonunion. The role of bone morphogenetic protein, platelet-rich plasma, and pulsed electromagnetic bone stimulators in navicular stress fracture is not defined by high-quality trials. Their use is a surgeon-and-patient decision and not the standard of care.
Most guidelines now require CT-confirmed union in addition to pain-free function before return. Some clinicians rely on symptoms and MRI alone. The imaging-confirmed union standard is more conservative and probably safer, but it is not validated by a single randomised trial.
Routine hardware removal is not required, but lateral prominence, irritation of the tibialis anterior tendon, and symptomatic hardware are indications. The threshold varies between surgeons and patients. There is no consensus on prophylactic removal in elite athletes.
MCQ Practice Points
Q: Why is the central third of the navicular prone to stress fracture? A: The central third is a vascular watershed. The medial half is perfused by the posterior tibial artery and the lateral half by the dorsalis pedis artery. These two systems converge at the central third without forming a rich collateral network, so the zone has limited biological reserve to repair repetitive microdamage.
Q: A 24-year-old sprinter has 6 weeks of vague midfoot pain and a normal X-ray. What is the next investigation? A: MRI. Plain X-ray is normal in 70-80 percent of acute navicular stress fractures, and MRI is the most sensitive test. Once MRI confirms the injury, CT is required to grade by Saxena and plan management.
Q: How does the Saxena classification influence management? A: Type I (incomplete dorsal-cortex fracture) is managed with a non-weight-bearing cast for 6-8 weeks. Type II (fracture extending into the body) and Type III (fracture into the opposite cortex or displaced) are managed with operative fixation, typically a headless compression screw placed from lateral to medial, often with bone graft in chronic cases.
Q: Describe the screw trajectory and implant choice for navicular stress fracture fixation. A: A 3.0 to 4.5 mm headless compression screw placed from lateral to medial, through the central third of the navicular, perpendicular to the fracture line. The headless design allows burial beneath the lateral cartilage and avoids impingement on the talar head.
Q: What is the strongest predictor of outcome in navicular stress fracture? A: Time from symptom onset to definitive management. Athletes treated within 3 months of symptom onset have a high union rate, while those presenting after 6 months face a substantial nonunion rate regardless of technique. Diagnostic delay is the single biggest modifiable cause of poor outcome.
Q: When is return to full sport safe after a navicular stress fracture? A: When the patient is pain-free, has no N-spot tenderness, has a negative single-leg hop test, and has CT-confirmed bridging callus across the fracture. The average return to full sport is 4-6 months from injury, longer in established nonunion or with re-fracture.
Clinical Imaging
Imaging is captured in the dedicated Investigations section below. Because this topic is generated for text-first validation, image components are intentionally omitted and will be added by the image-embedding pipeline after content freeze.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 22-year-old elite 400 m sprinter presents with 8 weeks of vague dorsal midfoot pain. Pain comes on with training and eases with rest, but has not settled. He has been running through the pain for the national championships. X-rays taken by his team doctor 6 weeks ago were reported as normal. On examination, the foot looks normal, but firm thumb pressure over the dorsal proximal navicular reproduces his pain. Single-leg hop on the affected side reproduces the pain; contralateral side is comfortable. How do you proceed?”
“A 35-year-old recreational runner presents with 9 months of dorsal midfoot pain. He was treated with an elastic bandage and activity modification by his primary care physician. Pain has progressed and he now has pain at rest and a mild limp. CT shows a complete sagittal fracture of the central third with sclerotic margins and a small cyst at the proximal fragment. What is your diagnosis and how do you manage this?”
Evidence Base and Key Trials
Intraosseous and extraosseous arterial anatomy of the adult navicular
- Cadaveric injection study mapped the extraosseous and intraosseous blood supply of the navicular
- Central third receives contributions from medial (posterior tibial) and lateral (dorsalis pedis) sources that converge but do not anastomose freely
- Dorsal-central region identified as the most consistent watershed zone
- Findings explain the sagittal orientation of the typical fracture and the propensity to nonunion
The non-surgical and surgical treatment of tarsal navicular stress fractures
- Comprehensive review of non-operative and operative strategies for navicular stress fractures
- Non-weight-bearing cast immobilisation remains first-line for incomplete dorsal-cortex fractures
- Surgical fixation with compression screw recommended for complete fractures in athletes
- Return to sport timelines and nonunion risk stratified by fracture completeness
Results of treatment of 22 navicular stress fractures and a new proposed radiographic classification system
- Three-type radiographic classification proposed that underpins the modern Saxena CT system
- Type I (dorsal cortex) treated successfully with non-weight-bearing cast
- Type II and III fractures showed improved outcomes with operative fixation
- Established the principle that fracture extent on imaging drives treatment choice
Overuse injuries in sport: the foot
- Early description of navicular stress fracture patterns in athletes by the group that defined the entity
- Highlighted the central-third location and diagnostic difficulty on plain films
- Advocated non-weight-bearing for incomplete injuries and surgical consideration for complete ones
- Established the clinical framework still referenced in modern high-risk stress fracture protocols