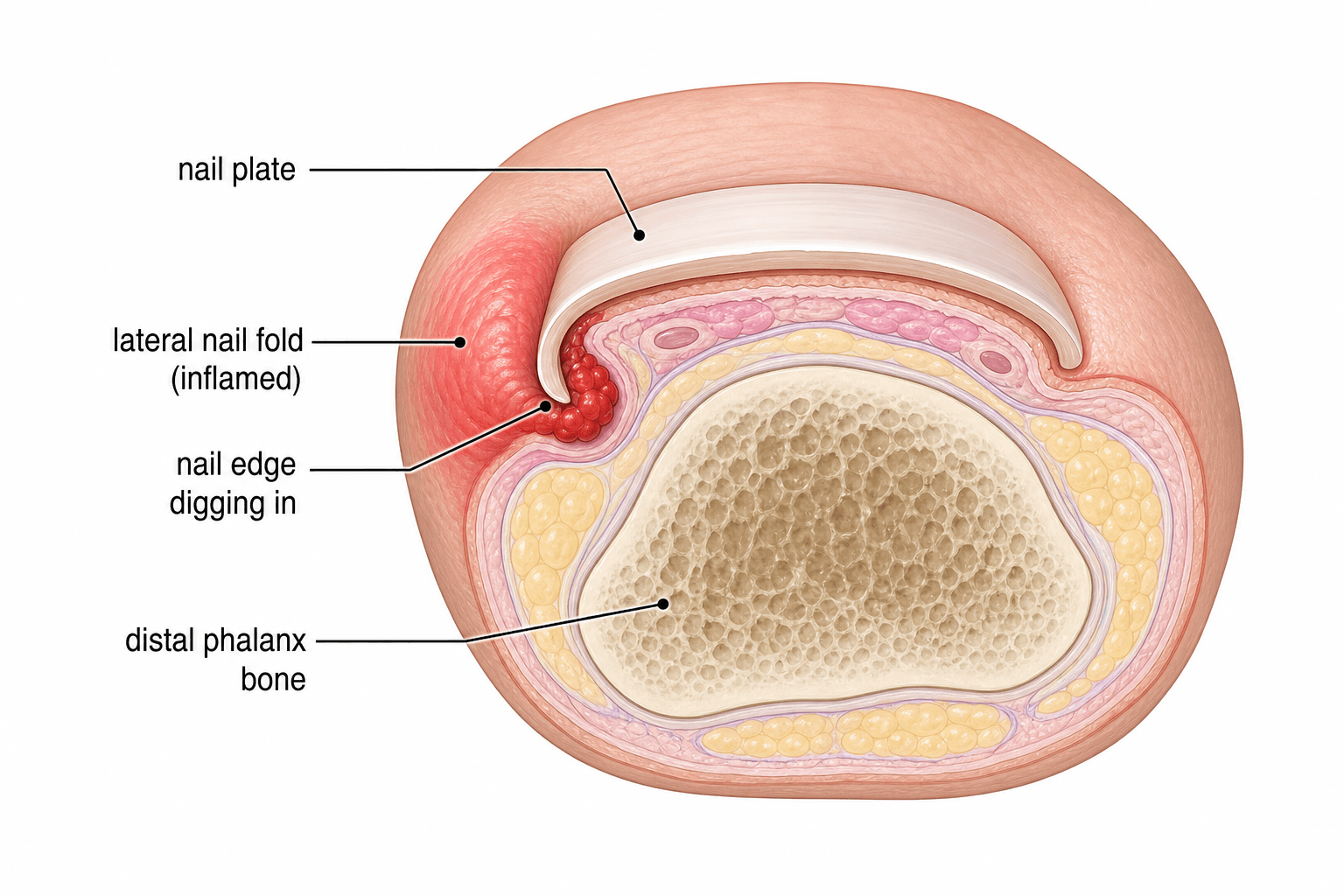
When the Nail Edge Invades the Nail Fold
- Onychocryptosis (ingrown toenail) is penetration of the LATERAL NAIL FOLD by the edge or a spicule of the nail plate, which acts as a foreign body and provokes inflammation, secondary infection and exuberant GRANULATION tissue; it most often affects the GREAT TOE (hallux).
- Contributing factors are improper nail cutting (cutting the nail too short or curved rather than straight across, leaving a spicule), TIGHT/constrictive footwear, trauma, HYPERHIDROSIS, abnormal nail shape (involuted/pincer nail), obesity and a genetic predisposition.
- Severity is graded by the HEIFETZ (and extended MOZENA) staging: stage I inflammatory (erythema/swelling/pain), stage II infected with discharge, stage III chronic granulation tissue and lateral wall hypertrophy (Mozena adds a stage IV with gross bilateral hypertrophy) - the stage guides treatment.
- EARLY (stage I) disease is managed CONSERVATIVELY: warm soaks, correct STRAIGHT-ACROSS nail trimming, lifting the nail edge off the fold with a cotton wisp/dental-floss or a gutter splint, taping techniques, roomy footwear, and treating any infection.
- When conservative measures fail, or for stage II-III disease, the definitive treatment is PARTIAL NAIL AVULSION combined with MATRICECTOMY of the corresponding nail-matrix horn - removing the offending nail edge AND ablating the matrix that produces it; matricectomy markedly reduces recurrence compared with simple avulsion alone.
- CHEMICAL matricectomy with PHENOL is the preferred modality for grade II-III onychocryptosis: meta-analysis shows phenol gives LOWER RECURRENCE and less pain than other methods. In the ONE randomised comparison of the SAME operation with and without phenol, recurrence was 14% versus 41% - the figure to quote, because a large single-centre series reporting about 1.1% with a 4-minute application is an uncontrolled best case rather than an expected rate. Alternatives are sodium hydroxide/TCA chemical matricectomy and surgical (Winograd) wedge excision of the matrix.
- “Ingrown toenail = nail edge/spicule penetrates the LATERAL nail fold (usually hallux); Heifetz/Mozena stages I-III(-IV).
- “Stage I: conservative (straight trimming, soaks, cotton wisp/gutter splint, footwear). Stage II-III: partial avulsion + matricectomy.
- “Phenol chemical matricectomy = lowest recurrence and less pain (meta-analysis); matricectomy beats avulsion alone. Quote 14% vs 41% (the only equal-arms RCT) rather than the ~1.1% single-centre series figure.
Removing the offending nail edge without treating the matrix leaves the matrix to grow the same nail shape back - high recurrence. Acceptable only as a temporary measure.
Partial avulsion + matricectomy (chemical/phenol or surgical/Winograd) ablates the matrix horn that produces the offending edge. In the one randomised comparison of the same operation with and without phenol, recurrence was 14% versus 41%. Preferred definitive treatment.
Nail-Unit Anatomy: Why the Matrix Horn Is the Target
The treatment of onychocryptosis only makes sense once the nail unit is understood, because the whole operation is aimed at one specific part of it - the matrix horn.
- Nail matrix (the growth plate of the nail). It has two functional zones: the germinal (proximal) matrix, lying under the proximal nail fold, which produces the bulk of the nail plate; and the sterile matrix / nail bed (ventral), which adds a thin ventral layer and keeps the plate adherent. The germinal matrix is what must be destroyed to stop a nail edge regrowing.
- The matrix "horns". The germinal matrix extends most proximally and laterally as two crescentic projections - the lateral matrix horns - which sit beneath the lateral nail folds. The horn on the affected side is precisely the tissue that produces the offending lateral nail edge, and is the target of matricectomy.
- Nail folds and cuticle. The proximal nail fold (its keratin layer is the eponychium / cuticle) and the paired lateral nail folds frame the plate; the lateral fold is the soft tissue the ingrowing edge penetrates. The hyponychium seals the nail bed under the free distal edge.
- Nail bed and bony floor. The nail bed lies directly on the dorsal periosteum of the distal phalanx, with only a thin soft-tissue layer between - which is why nail surgery and chemical ablation sit close to bone (relevant to the periostitis risk of over-application).
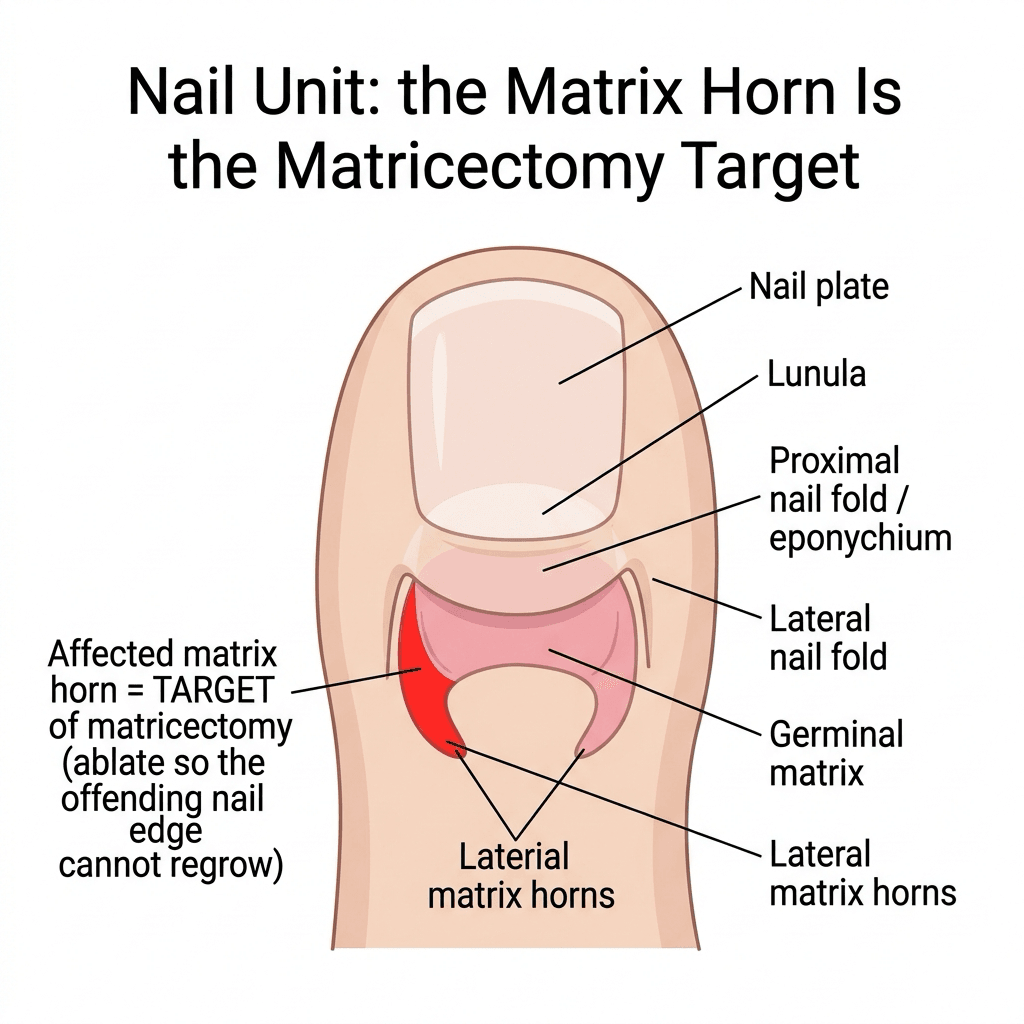
"Matricectomy" means ablating the germinal matrix horn on the involved side, not just pulling the nail. Simple avulsion leaves the horn intact, so the matrix grows the same edge back - which is exactly why avulsion-plus-matricectomy is the recurrence-lowering step. The lateral horn extends proximally under the proximal fold, so an ablation that stops short proximally leaves a viable horn and a recurrent spicule. (Nail-bed and germinal-matrix injury is developed in Seymour Fracture and Nail Bed Injuries.)
Pathogenesis & Presentation
The nail plate edge or a retained spicule penetrates the soft tissue of the lateral nail fold. The embedded keratin behaves as a foreign body, driving an inflammatory response with pain, erythema and swelling; the breached skin is then prone to secondary infection, and chronic irritation produces granulation tissue and hypertrophy of the nail wall. Patients present with a painful, red, swollen nail fold of the great toe, often with discharge, and pain on footwear pressure. Recognising the stage (Heifetz/Mozena) directs whether conservative or surgical treatment is appropriate.

Management
- Stage I (conservative): warm soaks, correct straight-across nail trimming (never cut down the corners), elevating the nail edge with a cotton wisp / dental-floss or a gutter splint, taping the fold away from the nail, roomy footwear, foot hygiene, and treating infection. Many early cases settle.
- Stage II-III / failed conservative care (definitive surgery): partial nail avulsion of the offending
border plus matricectomy of the corresponding matrix horn. Matricectomy options:
- Chemical matricectomy - PHENOL (preferred for grade II-III): apply phenol to the exposed matrix (commonly a 4-minute application) after avulsion - lowest recurrence and less pain.
- Chemical - sodium hydroxide / TCA: alternatives with comparable efficacy; some reports show less postoperative discharge.
- Surgical (Winograd) wedge excision of the lateral nail, matrix and inflamed fold; or Zadik/terminal Syme procedures for total matrix ablation in severe recurrent disease.
- Treat active infection, ensure tetanus cover where relevant, and counsel diabetic/vascular patients carefully (impaired healing).
Not every painful or deformed toenail is onychocryptosis - keep in mind: onychomycosis (fungal nail - thickened, discoloured, crumbly), onychogryphosis ('ram's horn' grossly thickened curved nail), subungual exostosis / osteochondroma (a bony outgrowth of the distal phalanx lifting the nail - radiograph if suspected), subungual melanoma (a pigmented streak/Hutchinson's sign - do not miss), pincer/involuted nail (transverse over-curvature), and paronychia (nail-fold infection). See also Subungual Exostosis.
How Phenol Matricectomy Is Performed - and Its Complications
Phenol matricectomy is a structured sequence, and being able to describe it step by step is what separates knowing the answer from being able to do the operation:
- Anaesthesia and a bloodless field. A digital ring block with local anaesthetic and a digital tourniquet - phenol is inactivated by blood, so a dry field is essential for the chemical to reach the matrix. On the perennial question of adrenaline in a digit: the traditional prohibition arose from historical case reports of digital necrosis involving early anaesthetic preparations rather than from adrenaline itself, and subsequent evidence has not supported a ban in the normally perfused digit - many now use a lidocaine-with-adrenaline block, which has the specific advantage here of helping produce the dry field phenol requires. Two qualifications matter: it is not the moment to abandon the tourniquet, and the argument for adrenaline does not extend to a digit whose perfusion is already compromised, which is exactly the foot that needs its perfusion measured first. Follow local policy, but be able to explain why the old rule existed and why it has been challenged.
- Partial nail avulsion. The offending lateral strip of nail plate is freed from the nail bed and proximal fold with a periosteal elevator and removed with a longitudinal split, exposing the lateral matrix horn; the rest of the nail is left in place.
- Chemical ablation of the horn. The exposed matrix (including the proximal lateral horn) is dried, then liquefied phenol (around 88 percent) is applied on a tightly rolled applicator, classically for an uninterrupted period (the Montesi series used a 4-minute application). The surrounding skin is protected and the matrix curetted/cleared first so the phenol contacts viable matrix.
- Neutralisation and dressing. Phenol is neutralised/flushed (alcohol or copious saline), the tourniquet released, and a non-adherent bulky dressing applied; aftercare is warm soaks, elevation and dressing changes.
- Surgical alternative. Where chemical ablation is unsuitable, the Winograd procedure excises the lateral nail, matrix horn and inflamed fold sharply, and Zadik / terminal Syme procedures ablate the whole matrix for severe recurrent disease.
- Prolonged drainage and slow healing. Phenol produces a controlled chemical burn, so a phenolised toe characteristically weeps for two to several weeks and heals more slowly than a clean surgical wound - patients must be warned. This is the trade-off for the low recurrence.
- Recurrence / residual spicule from incomplete ablation of the lateral horn (too short an application, a blood-contaminated field, or a missed proximal horn) - the commonest reason phenol "fails".
- Postoperative infection of the healing wound; treat as for any nail-fold infection.
- Periostitis / over-ablation because the matrix lies just off the distal phalangeal periosteum - excess phenol or contact time can injure adjacent tissue.
- Caution in the diabetic / ischaemic foot. Impaired healing and the open weeping wound make patient selection and vascular assessment important before offering chemical matricectomy - assessed by measuring the ankle-brachial index, toe pressure and transcutaneous oxygen rather than by impression.
A phenol matricectomy deliberately creates an open chemical burn that weeps for weeks. In a well-perfused foot that is a nuisance. In an ischaemic or neuropathic one it is an ulcer with a portal to the distal phalanx, and the distance from nail bed to bone is only a few millimetres - which is how a trivial procedure becomes osteomyelitis and then an amputation.
Perfusion is measured, not estimated. Palpating the dorsalis pedis and posterior tibial pulses is the start and not the answer, because pulses can be present in a foot that will not heal:
- Ankle-brachial index - 0.9 to 1.3 is normal; below 0.9 indicates peripheral arterial disease. Above 1.3 means incompressible, calcified vessels, which is common in diabetes and makes the index falsely reassuring - in that situation the ABI is uninterpretable and a toe pressure must be used instead.
- Toe pressure - below 30 mmHg indicates critical ischaemia and the need for revascularisation, not a nail operation.
- Transcutaneous oxygen - below 30 mmHg indicates poor healing potential.
These are the same thresholds used throughout the diabetic foot, set out in The Diabetic Foot.
Then adjust the operation to the foot. Where perfusion is adequate, favour the approach that leaves the smallest wound and avoid a chemical burn where a clean surgical wound would heal more predictably; keep the nail plate where possible; involve the diabetic foot service; and arrange review in days rather than weeks. In neuropathy the patient will not feel the complication developing, so follow-up must be scheduled rather than symptom-triggered. Where perfusion is inadequate, the nail problem is not the priority - refer for vascular assessment first. (See also Diabetic Foot Infections and Diabetic Neuropathy.)
The two things that make phenol work are a bloodless field (phenol is deactivated by blood) and reaching the proximal lateral matrix horn; the two things to counsel about are prolonged drainage (a chemical burn weeps for weeks) and that the main failure mode is a residual spicule from incomplete ablation.
What Recurrence Rate Should You Actually Quote?
Two very different recurrence figures circulate for phenol matricectomy, both correct, and quoting the wrong one to a patient or an examiner is a trap worth understanding.
- Where it comes from
- A single-centre series of 622 consecutive procedures with a 4-minute application - uncontrolled, one team, one technique
- What it can and cannot support
- Shows what an experienced unit achieves with a long, standardised application. It is a best-case, single-arm figure and not a general expectation
- Where it comes from
- The one randomised comparison in which BOTH arms had the same operation - partial nail avulsion with matrix excision - differing only by the addition of phenol (117 participants, RR 0.34, 95% CI 0.17 to 0.69)
- What it can and cannot support
- This is the figure that actually demonstrates what phenol ADDS, because it is the only clean comparison. It supports the recommendation to add chemical ablation
- Where it comes from
- 4 of 12 comparisons in the Cochrane review found a significant reduction
- What it can and cannot support
- Weaker than it looks: in most of those studies the surgical procedures in the two arms were NOT the same, so the benefit cannot be attributed to the phenol alone
How to use this. The defensible statement is that adding phenol to a matricectomy roughly halves recurrence in the only like-for-like randomised comparison, and that experienced units using a long application report rates around 1%. When consenting a patient, quoting 1% as the expected recurrence overstates what the evidence supports for a first operation by an occasional operator. The honest counselling position is that recurrence is uncommon but real, that it rises if the ablation is incomplete, and that a second procedure is possible if a spicule regrows.
Surgery beats conservative treatment for recurrence - that much is consistent across the Cochrane review, comparing surgical intervention against gutter treatment and against orthonyxia (brace) treatment. Conservative measures remain correct first-line for stage I disease because most early cases settle and the toe is spared an operation, not because they match surgery at preventing recurrence.
Antibiotics: the Answer Is Usually No
Because stage II disease is defined by infection and discharge, the instinct is to prescribe. The evidence does not support it as a routine.
Around the operation, antibiotics add nothing measurable. The Cochrane review examined post-operative interventions - antibiotics among them, alongside manuka honey, povidone-iodine with paraffin, hydrogel with paraffin and paraffin gauze - and none showed any significant difference in infection rate, pain or healing time. The reason is mechanical rather than microbiological: the pathology is a foreign body in the soft tissue, and removing the offending nail edge removes the cause, drains the infected fold and lets it heal. Antibiotics without removing the nail edge treat the consequence and leave the cause in place.
Where antibiotics still belong is the ordinary indication - spreading cellulitis beyond the nail fold, systemic upset, or a host who cannot contain infection (poorly controlled diabetes, immunosuppression, peripheral arterial disease). Localised erythema and discharge confined to the nail fold is not that.
The practical consequence is that an infected stage II ingrown toenail does not need a course of antibiotics before it can be operated on. Waiting for the infection to "settle" on antibiotics before doing the definitive procedure delays the only treatment that addresses the cause, and the same argument applies to draining a paronychia associated with an ingrown nail - treatment is directed at the causal toenail. (See Paronychia.)
Mnemonics & Memory Aids
STRAIGHT
Hook:Cut STRAIGHT across - and for the matrix, ablate it (phenol) to stop recurrence.
PHENOL
Hook:PHENOL matricectomy = partial avulsion + ablate the matrix horn = low recurrence.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“How would you assess and manage a patient with a painful ingrown great toenail, and what determines whether you operate?”
“A nail looks abnormal but is lifting up with a firm swelling under the nail edge, and the toe is not simply inflamed at the fold. What else must you consider besides an ingrown toenail?”
Definition & cause
- Nail edge/spicule penetrates the lateral nail fold (usually hallux)
- Causes: cutting too short/curved, tight shoes, trauma, hyperhidrosis, pincer nail
- Foreign-body inflammation -> infection -> granulation/hypertrophy
Staging (Heifetz/Mozena)
- I: inflammatory (erythema/swelling/pain)
- II: infected with discharge
- III: granulation + lateral wall hypertrophy (Mozena IV: gross bilateral)
Treatment
- Stage I: soaks, straight trimming, cotton wisp/gutter splint, footwear
- Stage II-III/failed: partial avulsion + MATRICECTOMY (avulsion alone recurs)
- Phenol chemical matricectomy preferred (14% vs 41% recurrence in the equal-arms RCT, less pain); Winograd = surgical option
- Antibiotics change nothing post-operatively - reserve for spreading cellulitis or a compromised host
- Diabetic/vascular foot: measure ABI (0.9-1.3; over 1.3 = calcified, use toe pressure), toe pressure and TcPO2 (both under 30 mmHg = poor healing) BEFORE operating
Differential (abnormal nail)
- Subungual exostosis (radiograph), subungual melanoma (Hutchinson's - biopsy)
- Onychomycosis, onychogryphosis, pincer/involuted nail, paronychia
- Care in diabetic/vascular feet (healing)
Evidence & Key Studies
Efficacy and safety of phenol-based partial matricectomy in onychocryptosis: a systematic review and meta-analysis
- Across 18 controlled studies (1655 patients), phenol matricectomy was associated with significantly FEWER recurrences than other modalities (about 49 fewer per 1000).
- Phenol also produced less postoperative pain; however TCA- and NaOH-based matricectomies had less postoperative discharge/haemorrhage.
- Phenol matricectomy combines a low recurrence rate with a favourable adverse-effect profile and is the preferred modality for grade II-III onychocryptosis.
Recurrence of onychocryptosis treated with phenolization: does phenol application time matter? A follow-up of 622 procedures
- In 622 consecutive procedures using a 4-minute phenol chemical matricectomy, overall recurrence was only 1.1%.
- Recurrence was higher in patients with cardiovascular disease (5.1%) and in younger patients.
- An uninterrupted 4-minute phenol application appears to be an appropriate time to achieve matrix ablation with a low recurrence rate.
Interventions for ingrowing toenails (Cochrane systematic review)
- 24 randomised studies, 2,826 participants: surgical interventions prevented recurrence better than non-surgical gutter treatment, and probably better than orthonyxia (brace) treatment.
- In the ONE study comparing identical operations differing only by phenol - partial nail avulsion with matrix excision, 117 participants - recurrence was 14% with phenol versus 41% without (RR 0.34, 95% CI 0.17 to 0.69).
- In 4 of 12 other chemical-versus-no-chemical comparisons a significant reduction was found, but the surgical procedures in the two arms were NOT equivalent, so the benefit cannot be attributed to the chemical alone.
- Post-operative interventions - including ANTIBIOTICS, manuka honey, povidone-iodine with paraffin, hydrogel with paraffin and paraffin gauze - showed NO significant difference in infection rate, pain or healing time.
The superiority of phenol matricectomy for recurrence/pain comes from the cited Vinay meta-analysis, and the ~1.1% recurrence with a 4-minute application (higher with cardiovascular disease and youth) from the cited Montesi series - an uncontrolled single-centre cohort, which is why it is presented as a best-case figure rather than an expected rate. The 14%-versus-41% comparison, the caveat that most chemical-versus-no-chemical studies did not compare equal operations, and the finding that post-operative antibiotics do not change infection, pain or healing come from the cited Cochrane review. The perfusion thresholds (ABI 0.9 and 1.3, toe pressure and TcPO2 below 30 mmHg) follow The Diabetic Foot. The Heifetz/Mozena staging and conservative measures are standard clinical teaching. (See also Paronychia, Subungual Exostosis and Subungual Melanoma.)