Surgical Emergency | Pain Out of Proportion | Early Debridement Saves Lives
NECROTIZING FASCIITIS TYPES
Critical Must-Knows
- Pain out of proportion to clinical findings is the classic early sign - do not dismiss this
- Hard signs: Crepitus, skin necrosis, bullae, 'dishwater' pus - immediate surgery
- Soft signs: Disproportionate pain, rapidly spreading erythema, systemic toxicity - high suspicion
- LRINEC score ≥6: Intermediate risk; ≥8 strongly predictive - do not rely on score alone
- Finger test: Incision, lack of bleeding, 'dishwater' pus, fascial necrosis confirms diagnosis
- Time is tissue: Delay to debridement is the key modifiable driver of mortality (non-survivors waited ~90h vs ~25h for survivors)
Clinical Pearls
- "Pain out of proportion + systemic toxicity = necrotizing fasciitis until proven otherwise
- "Type I (polymicrobial): Diabetics, post-op, perineum (Fournier's) - mixed organisms
- "Type II (monomicrobial): GAS in healthy adults - TOXIC SHOCK SYNDROME
- "Clindamycin is essential - inhibits toxin production (Eagle effect)
- "Surgery is diagnosis AND treatment - CT/MRI delays cost lives
Clinical Imaging
Imaging Gallery





Critical Necrotizing Fasciitis Exam Points
Pain Out of Proportion
The earliest and most important sign. Patient reports severe pain but examination findings are minimal. Pain often extends beyond visible erythema. Do NOT dismiss this symptom - it reflects deep tissue ischemia from fascial necrosis and vessel thrombosis.
Hard vs Soft Signs
Hard signs (100% sensitivity): Crepitus, skin necrosis, bullae (hemorrhagic or serous), 'dishwater' gray discharge, visible fascial necrosis. Soft signs: Disproportionate pain, rapidly spreading cellulitis, systemic toxicity, failure to respond to antibiotics.
LRINEC Score
Laboratory Risk Indicator for NECrotizing fasciitis. Score ≥6 = intermediate risk; ≥8 = high risk. Components: CRP, WCC, Hb, Na, Creatinine, Glucose. CRITICAL: A low LRINEC does NOT exclude NF - clinical suspicion trumps scoring systems.
Time is Tissue
Delay to debridement is the strongest modifiable predictor of death - in McHenry's series non-survivors waited a mean 90 hours versus 25 hours for survivors. Delay beyond 12 hours markedly increases the number of debridements, septic shock and renal failure (Kobayashi). Do NOT delay surgery for CT/MRI - the operating theatre is both diagnostic and therapeutic.
Type I vs Type II Necrotizing Fasciitis
| Feature | Type I (Polymicrobial) | Type II (Monomicrobial) |
|---|---|---|
| Organisms | Mixed aerobic + anaerobic (Streptococcus, Enterococcus, E. coli, Bacteroides, Peptostreptococcus) | Single organism: GAS (Strep pyogenes), S. aureus (MRSA), less commonly Clostridium |
| Patient population | Elderly, diabetics, immunocompromised, post-surgical, perineal (Fournier's) | Previously healthy adults, children, minor trauma or NSAID use |
| Precipitant | Surgery, perianal abscess, decubitus ulcer, diabetic foot | Minor skin break, insect bite, blunt trauma, varicella (children) |
| Gas in tissues | Common (anaerobic organisms) | Less common (unless clostridial superinfection) |
| Toxic shock | Less common | Very common with GAS - high mortality |
| Antibiotic regimen | Broad-spectrum: Piperacillin-tazobactam + Clindamycin ± Vancomycin | Penicillin + Clindamycin (GAS); Vancomycin + Clindamycin (MRSA) |
| Mortality | 15-30% | 30-50% (higher with TSS) |
CWHSCGLRINEC Score Components
| C | CRP Greater than 150: +4 points |
| W | WCC 15-25: +1; Greater than 25: +2 points |
| H | Haemoglobin 110-135: +1; Less than 110: +2 points |
| S | Sodium Less than 135: +2 points |
| C | Creatinine Greater than 141: +2 points |
| G | Glucose Greater than 10: +1 point |
| C | CRP Greater than 150: +4 points | H | Haemoglobin 110-135: +1; Less than 110: +2 points | C | Creatinine Greater than 141: +2 points |
| W | WCC 15-25: +1; Greater than 25: +2 points | S | Sodium Less than 135: +2 points | G | Glucose Greater than 10: +1 point |
Hook:CRP-WCC-Haemoglobin-Sodium-Creatinine-Glucose. Score 6+ = intermediate risk, 8+ = high risk. But clinical judgement trumps score!
CNBDHard Signs of Necrotizing Fasciitis
| C | Crepitus Gas in tissues - palpable crackling |
| N | Necrosis Skin necrosis - dusky, non-blanching |
| B | Bullae Hemorrhagic or serous blisters |
| D | Dishwater discharge Gray, foul-smelling 'dishwater' pus |
| C | Crepitus Gas in tissues - palpable crackling | B | Bullae Hemorrhagic or serous blisters |
| N | Necrosis Skin necrosis - dusky, non-blanching | D | Dishwater discharge Gray, foul-smelling 'dishwater' pus |
Hook:CNBD: Crepitus, Necrosis, Bullae, Dishwater pus = IMMEDIATE surgery. Any hard sign = theatre NOW!
DIABETICCauses/Risk Factors
| D | Diabetes mellitus Major risk factor - impaired immunity, vascular disease |
| I | Immunocompromised HIV, chemotherapy, steroids, transplant |
| A | Alcohol excess Liver disease, malnutrition, poor wound care |
| B | Breaks in skin Surgical wounds, injection sites, trauma |
| E | Extremes of age Very young or elderly |
| T | Tissue ischemia PVD, vasculitis, pressure sores |
| I | IV drug use Contaminated needles, injection site infections |
| C | Chronic illness Renal failure, malignancy, malnutrition |
| D | Diabetes mellitus Major risk factor - impaired immunity, vascular disease | B | Breaks in skin Surgical wounds, injection sites, trauma | I | IV drug use Contaminated needles, injection site infections |
| I | Immunocompromised HIV, chemotherapy, steroids, transplant | E | Extremes of age Very young or elderly | C | Chronic illness Renal failure, malignancy, malnutrition |
| A | Alcohol excess Liver disease, malnutrition, poor wound care | T | Tissue ischemia PVD, vasculitis, pressure sores |
Hook:DIABETIC: Most NF occurs in diabetics and immunocompromised. But Type II GAS can occur in healthy adults!
Overview and Epidemiology
Necrotizing fasciitis (NF) is a rapidly progressive, life-threatening soft tissue infection characterized by necrosis of fascia and subcutaneous tissue with relative sparing of overlying skin (initially) and underlying muscle. It represents a surgical emergency where early recognition and aggressive debridement are the only interventions that improve survival. [1]
Definition: Necrotizing fasciitis is a necrotizing soft tissue infection (NSTI) involving the fascial planes, spreading along the relatively avascular fascia with thrombosis of perforating vessels leading to secondary skin necrosis. Unlike cellulitis, the infection travels in the deep fascial planes, making surface examination misleadingly benign. [2]
Epidemiology:
- Incidence: 0.4-0.9 per 100,000 population per year [3]
- Increasing incidence: 2-4 fold increase over past 20 years
- Mortality: 20-40% overall; up to 70-80% with delayed treatment or toxic shock syndrome
- Male:Female ratio: 2-3:1
- Age: Bimodal - peaks in neonates and adults over 50 years
- Fournier's gangrene (perineal NF): 40% mortality
Historical Context:
- First described by Confederate surgeon Joseph Jones in 1871 during American Civil War
- Term "necrotizing fasciitis" coined by Wilson in 1952
- Previously known as "hospital gangrene," "streptococcal gangrene"
- Remains associated with military trauma, natural disasters, and IV drug use epidemics
The Examination Favourite
Necrotizing fasciitis is an FRCS/FRACS examination favourite because it tests:
- Recognition of a surgical emergency from clinical signs
- Understanding of soft tissue anatomy and fascial planes
- Knowledge of microbiology and antibiotic selection
- Surgical decision-making (when to operate, when to return)
- Ethical aspects of life-threatening disease and limb sacrifice
The examiner wants to hear: "Pain out of proportion = NF until proven otherwise. When in doubt, cut it out."
Pathophysiology
Mechanism of Tissue Destruction:
Necrotizing fasciitis spreads along fascial planes because:
- Fascia is relatively avascular - fewer immune cells reach infection
- Bacteria produce enzymes (hyaluronidase, lipases, collagenases) that digest connective tissue
- Thrombosis of perforating vessels leads to skin ischemia (explains pain out of proportion)
- Toxin production causes systemic toxicity and shock
Type I (Polymicrobial) Pathophysiology:
- Synergistic infection with aerobic and anaerobic organisms
- Aerobes consume oxygen, creating hypoxic environment
- Anaerobes thrive in hypoxia, produce gas (crepitus)
- Typically occurs in compromised tissue (diabetes, PVD, post-surgical)
- Enzymes from multiple organisms accelerate tissue destruction
Type II (Monomicrobial - GAS) Pathophysiology:
- Group A Streptococcus produces multiple virulence factors:
- Streptolysin O and S: Pore-forming toxins causing cell lysis
- Streptococcal pyrogenic exotoxins (SPE-A, B, C): Superantigens causing massive cytokine release
- M-protein: Antiphagocytic, promotes adherence
- Streptokinase: Activates plasminogen, promotes spread
- Streptococcal Toxic Shock Syndrome (STSS): Superantigen activates 20-30% of T-cells (vs 0.01% in normal antigen response) causing cytokine storm
- The Eagle Effect: At high bacterial loads, GAS enters stationary phase and stops dividing. Beta-lactams (which work on dividing bacteria) become less effective. Clindamycin works by inhibiting protein synthesis (including toxin production) regardless of growth phase.
Type III (Gas Gangrene/Clostridial) Pathophysiology:
- Clostridium perfringens produces alpha-toxin (lecithinase)
- Alpha-toxin lyses cell membranes, causing massive tissue necrosis
- Rapid gas production (CO2, H2) causes crepitus
- Extremely rapid progression - can be fatal within hours
Vibrio vulnificus:
- Gram-negative rod found in warm seawater
- Enters through minor wounds during seafood handling or swimming
- Produces cytolysins and proteases
- Particularly severe in patients with liver disease or haemochromatosis (iron overload feeds bacterial growth)
- Mortality 50-60% if septicemic
Why Speed Matters
Necrosis can advance rapidly along fascial planes, so a deceptively small area of involvement at presentation may become extensive within hours if not debrided. Delay to operative debridement is the strongest modifiable determinant of death: in McHenry's series the mean time from admission to surgery was 90 hours in non-survivors versus 25 hours in survivors. The infection cannot be controlled with antibiotics alone.
Clinical Presentation
The Clinical Challenge: Early necrotizing fasciitis mimics cellulitis. The key is recognizing the discordance between patient symptoms (severe) and examination findings (relatively minor).
History
Classic Presenting Symptoms:
-
Pain out of proportion - THE cardinal feature
- Severe pain that seems excessive for appearance
- Pain extending beyond area of visible erythema
- Inadequate response to analgesia
- May paradoxically improve as nerves undergo necrosis (ominous sign)
-
Rapid progression
- "It wasn't like this 4 hours ago"
- Erythema spreading despite antibiotics
- Blisters appearing over hours
-
Systemic symptoms
- Fever, rigors, sweating
- Nausea, vomiting, diarrhea
- Confusion, altered consciousness
- "Feeling like I'm going to die"
Precipitating Events:
- Minor trauma (scratch, insect bite, abrasion)
- Recent surgery (abdominal, perineal, orthopaedic)
- Injection (IVDU, intramuscular injection)
- Perianal abscess, pilonidal disease
- Childbirth, episiotomy
- Varicella infection (children)
- NSAID use (may mask early symptoms, promotes bacterial invasion)
Physical Examination

Hard Signs (100% Specific - Immediate Surgery)
Any ONE of these mandates immediate surgery:
-
Crepitus
- Gas in tissues (palpable crackling)
- Best felt at periphery of infection
- May not be present in Type II (GAS)
-
Skin Necrosis
- Dusky, purplish discoloration
- Non-blanching erythema
- Loss of sensation (cutaneous nerve necrosis)
-
Bullae
- Hemorrhagic (blood-filled): More ominous
- Serous (clear fluid): Still concerning
- Indicate dermal-epidermal separation from vascular thrombosis
-
Dishwater Discharge
- Gray, thin, foul-smelling discharge
- "Dishwater" or "washing-up water" appearance
- May see on spontaneous skin breakdown or aspiration
-
Fascial Necrosis Visible
- Frank tissue necrosis visible through skin breaks
- Gray, non-viable fascia
The Viva Question
Examiner: "A patient with diabetes presents with leg pain and redness. How do you differentiate necrotizing fasciitis from cellulitis?"
Answer: "I would be concerned about necrotizing fasciitis if there is:
- Pain out of proportion to examination findings
- Systemic toxicity - fever, tachycardia, hypotension, confusion
- Failure to respond to 24-48 hours of IV antibiotics
- Hard signs - crepitus, bullae, skin necrosis, woody induration
If I have clinical concern, I would perform the finger test - bedside incision under local anaesthetic. Lack of bleeding, 'dishwater' pus, and fascial necrosis that separates easily confirms the diagnosis and mandates immediate extensive debridement."
Differential Diagnosis
Distinguishing Necrotizing Fasciitis from Mimics
| Condition | Distinguishing features | Key discriminator from NF |
|---|---|---|
| Cellulitis / erysipelas | Erythema, warmth, well/ill-defined margin; systemically less unwell; responds to antibiotics | Pain proportionate to signs; no crepitus, bullae or dishwater pus; improves on antibiotics |
| Abscess | Localised fluctuant collection; point tenderness | Drains pus, not dishwater fluid; no spreading fascial necrosis |
| Clostridial myonecrosis (gas gangrene) | Severe pain, crepitus, bronze skin, marked toxaemia | Primarily muscle (not fascia) necrosis - overlaps with Type III NF; same emergency management |
| Pyomyositis | Deep muscle abscess, often tropical; fever, localised muscle pain | Muscle-centred on imaging; lacks fascial 'dishwater' separation |
| Acute compartment syndrome | Pain on passive stretch, tense compartment, post-injury/ischaemia | No systemic sepsis or skin necrosis; normal inflammatory markers |
| Deep vein thrombosis | Unilateral swelling, calf tenderness; afebrile | No toxaemia, crepitus or skin necrosis; confirmed on Doppler |
| Acute gout / pseudogout | Hot swollen joint, monoarticular, raised urate/crystals | Joint-centred; no fascial necrosis; rapid response to anti-inflammatories |
Investigations
Key Principle: Investigations should NOT delay surgery if clinical suspicion is high. The operating theatre is both diagnostic and therapeutic.
Laboratory Investigations
LRINEC Score (Laboratory Risk Indicator for NECrotizing fasciitis):
LRINEC Score Components
| Parameter | Range | Points |
|---|---|---|
| CRP (mg/L) | Less than 150 | 0 |
| CRP (mg/L) | ≥150 | +4 |
| WCC (×10⁹/L) | Less than 15 | 0 |
| WCC (×10⁹/L) | 15-25 | +1 |
| WCC (×10⁹/L) | Greater than 25 | +2 |
| Haemoglobin (g/L) | Greater than 135 | 0 |
| Haemoglobin (g/L) | 110-135 | +1 |
| Haemoglobin (g/L) | Less than 110 | +2 |
| Sodium (mmol/L) | ≥135 | 0 |
| Sodium (mmol/L) | Less than 135 | +2 |
| Creatinine (μmol/L) | ≤141 | 0 |
| Creatinine (μmol/L) | Greater than 141 | +2 |
| Glucose (mmol/L) | ≤10 | 0 |
| Glucose (mmol/L) | Greater than 10 | +1 |
LRINEC Score Interpretation:
- Score less than 6: Low risk (PPV less than 50%)
- Score 6-7: Intermediate risk - high clinical vigilance
- Score ≥8: High risk (PPV 75%+) - strongly consider surgery
CRITICAL LIMITATION: LRINEC was developed retrospectively. A normal LRINEC does NOT exclude NF. Sensitivity is only 60-80%. Clinical judgement remains paramount. [4]
Other Laboratory Tests:
- Blood cultures: Positive in 20-50%, identifies causative organism
- Lactate: Elevated lactate indicates tissue hypoperfusion and worse prognosis
- Creatine kinase (CK): Elevated if myonecrosis (worse prognosis)
- Procalcitonin: May help differentiate bacterial infection from other causes
- Coagulation: PT/INR, APTT, fibrinogen, D-dimer (DIC is common)
- Arterial blood gas: Metabolic acidosis indicates severe sepsis
Imaging
Plain Radiograph (X-ray)
Role: Quick screening, may show gas in soft tissues
Findings:
- Gas tracking along fascial planes (pathognomonic but only present in 25-50%)
- More common in Type I (polymicrobial) and Type III (clostridial)
- May be absent in Type II (GAS)
Limitation: Low sensitivity; absence of gas does NOT exclude NF

The Finger Test (Bedside Diagnosis)
Indications: High clinical suspicion for NF but diagnosis uncertain
Technique:
- Perform under local anaesthesia at bedside or in theatre
- Make 2cm incision through skin and subcutaneous tissue down to fascia
- Observe for:
- Lack of bleeding (vessel thrombosis)
- "Dishwater" gray pus (pathognomonic)
- Necrotic fascia - gray, stringy, easily separates with finger dissection
- "Finger test" positive - can easily pass finger along fascial plane with no resistance
If positive: Proceed immediately to extensive debridement
Imaging Pitfalls
DO NOT let imaging delay surgery. A patient with hard signs of NF should go directly to theatre. CT or MRI may be normal early in disease. The operating theatre is the definitive diagnostic tool - if fascia is necrotic and separates easily, the diagnosis is confirmed.
Management Principles
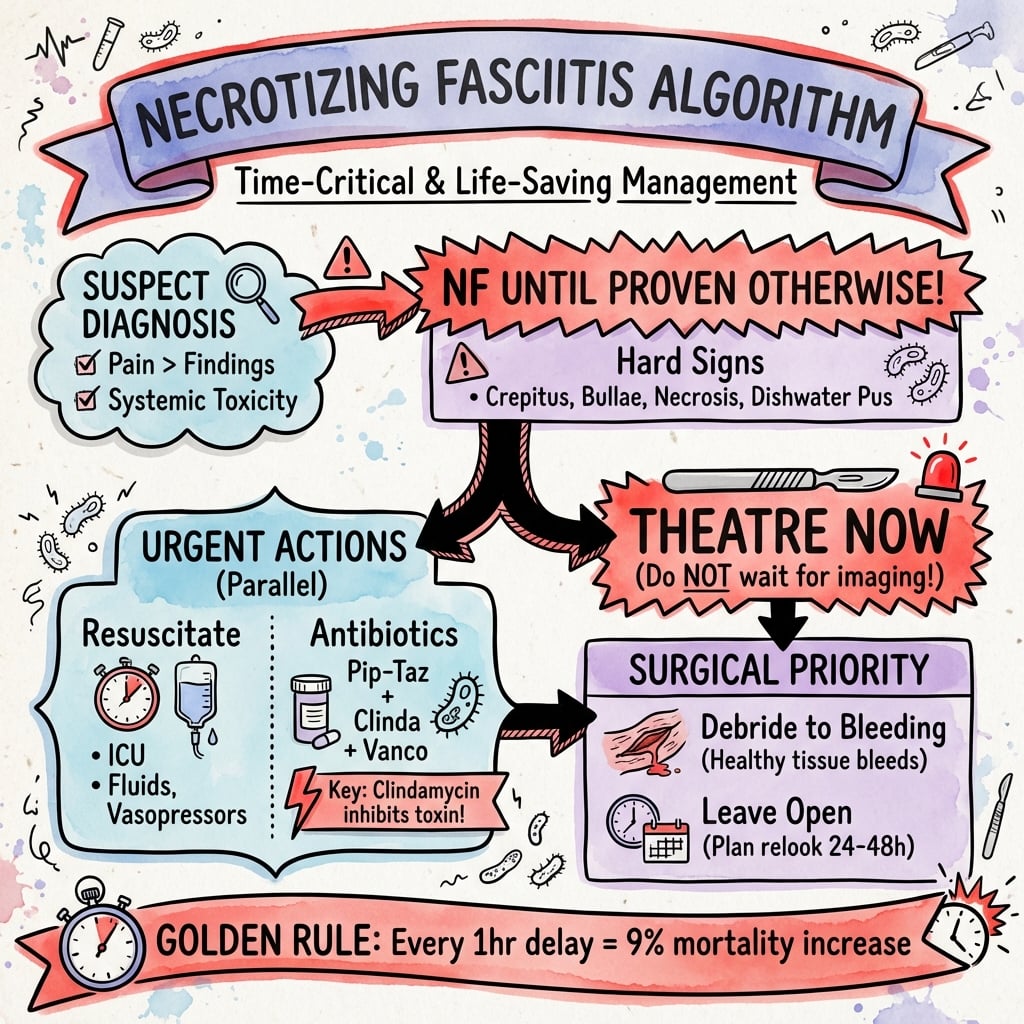
The Three Pillars of NF Management:
- Resuscitation - Aggressive fluid, vasopressor support, ICU admission
- Debridement - Early, extensive, repeated
- Antibiotics - Empiric broad-spectrum, include clindamycin for toxin inhibition
Initial Resuscitation
Recognize Sepsis/Septic Shock:
- Apply qSOFA/SOFA criteria
- Most NF patients meet sepsis criteria
- Many have septic shock requiring vasopressors
Fluid Resuscitation:
- Large bore IV access (ideally 2x large bore)
- Crystalloid bolus 30 mL/kg in first 3 hours
- Titrate to MAP greater than 65 mmHg, UO greater than 0.5 mL/kg/hr
- Central venous access for monitoring and vasopressors
Vasopressor Support:
- Noradrenaline first-line if hypotensive despite fluids
- Target MAP greater than 65 mmHg
- May need multiple agents
ICU Admission:
- All NF patients require ICU/HDU admission
- For ongoing resuscitation, monitoring, and repeated surgeries
- May need renal replacement therapy, mechanical ventilation
Correct Coagulopathy:
- DIC is common with GAS (Type II)
- Transfuse blood products as needed
- FFP, platelets, cryoprecipitate for active bleeding
Surgical Debridement
The Definitive Treatment: Surgery is both diagnostic and therapeutic. No amount of antibiotics can substitute for adequate debridement of necrotic tissue.
Surgical Debridement Technique
Timing:
- Operate as soon as the patient is resuscitated enough for anaesthesia (within hours, not days)
- Delay to debridement is the strongest modifiable predictor of death (90h vs 25h, McHenry); delay beyond 12h markedly increases debridements, septic shock and AKI (Kobayashi)
- Do not delay for imaging if clinical diagnosis clear
Principles:
- Aggressive, extensive debridement
- All necrotic tissue must be removed
- Healthy tissue bleeds - debride until you see bleeding edges
- Fasciotomies if compartment syndrome suspected
Step-by-Step Approach:
-
Incision
- Longitudinal incision over area of maximal involvement
- Extend beyond visible erythema to healthy tissue
-
Assess Fascia (Finger Test)
- Necrotic fascia is gray, stringy
- Easily separates from underlying muscle with finger dissection
- Healthy fascia is glistening white and adherent

-
Debride Fascia
- Excise all necrotic fascia with no resistance
- Continue until fascia bleeds and is adherent
- May need to extend incisions to follow necrosis
-
Assess Muscle
- Healthy muscle: Pink, contracts to stimulation, bleeds when cut
- Necrotic muscle: Dull, non-contractile, does not bleed
- Debride non-viable muscle (myonecrosis = worse prognosis)
-
Assess Skin
- Initially viable skin may become necrotic over 24-48 hours
- Preserve skin if viable (can excise at relook)
- Excise overtly necrotic skin
-
Wound Management
- Leave wounds open
- Apply saline-soaked dressings or NPWT
- Plan for return to theatre
Surgical Pearls
Key Points for Viva:
- "When in doubt, cut it out" - if clinical suspicion, explore surgically
- Debride until it bleeds - necrotic tissue does not bleed
- Healthy fascia is adherent - necrotic fascia separates easily
- Plan for re-look - most patients need 2-4 debridements
- Life over limb - do not delay amputation if indicated
Complications and Prognosis
Complications
Immediate/Early:
- Septic shock - multi-organ failure, DIC, death
- ARDS - acute respiratory distress syndrome
- Acute kidney injury - from sepsis, rhabdomyolysis
- Limb loss - amputation required in 15-20%
- Exsanguinating hemorrhage - from eroded vessels
- Toxic shock syndrome - especially Type II (GAS)
Late:
- Chronic wounds - prolonged healing, skin grafts
- Scarring and contractures - may limit function
- Chronic pain - phantom limb pain if amputated
- Psychological morbidity - PTSD, depression, body image issues
- Functional impairment - particularly after limb amputation
Prognostic Factors
Factors Associated with Increased Mortality:
Prognostic Factors in Necrotizing Fasciitis
| Factor | Relative Risk | Comments |
|---|---|---|
| Delay to first debridement | Strongest modifiable risk | Non-survivors waited ~90h vs ~25h (McHenry); delay beyond 12h increases debridements/shock/AKI (Kobayashi) |
| Admission to non-surgical service | 2x mortality | Recognition and surgical referral delays |
| Age greater than 60 years | 2-3x mortality | Reduced physiological reserve |
| Diabetes mellitus | 1.5-2x mortality | Immunocompromise, vascular disease |
| Streptococcal toxic shock | 30-70% mortality | Cytokine storm, DIC |
| Trunk involvement | Higher mortality | Harder to debride, vital structures |
| WCC greater than 30 or less than 4 | Poor prognosis | Extremes of immune response |
| Renal failure | 2x mortality | Marker of severe sepsis |
| Inadequate initial debridement | 2x mortality | Must debride to healthy tissue |
Survival Outcomes
Overall Mortality:
- Historical: 70-80% (pre-antibiotic era)
- Current: 20-40% with modern treatment
- Early recognition and aggressive surgery: 10-25%
- Delayed treatment: 50-70%
Factors Improving Survival:
- Recognition within 24 hours of symptom onset
- Surgery within 6-8 hours of presentation
- Adequate debridement (multiple re-looks)
- ICU care with multi-organ support
- Clindamycin in antibiotic regimen
- IVIG in streptococcal toxic shock
Evidence Base
LRINEC Score Development
- Retrospective derivation/validation (145 NF vs 309 severe cellulitis/abscess)
- Six routine variables: CRP, WCC, Hb, sodium, creatinine, glucose
- Cut-off of 6 gave PPV 92.0% and NPV 96.0% in this cohort
- AUC 0.98 (developmental) and 0.976 (validation)
LRINEC, Exam & Imaging Accuracy (Meta-analysis)
- Systematic review/meta-analysis: 23 studies, n=5982
- LRINEC ≥6 pooled sensitivity only 68.2%, specificity 84.8%
- LRINEC ≥8 sensitivity 40.8%, specificity 94.9%
- CT sensitivity 88.5%/specificity 93.3%; plain film sensitivity 48.9%
A LRINEC of Zero Does Not Exclude NF
- Case report of a 37-year-old man with surgically confirmed NF
- LRINEC score was 0 despite established disease
- Illustrates the danger of using LRINEC to rule out NF
- Reinforces that NF remains a clinical diagnosis
Time to Surgery and Outcome
- 65 patients with necrotising soft-tissue infection
- Mean time admission-to-operation 90 h in non-survivors vs 25 h in survivors (p=0.0002)
- Average 3.3 debridements per patient; overall mortality 29%
- Early debridement was the key modifiable determinant of survival
Delay Increases Debridements & Morbidity
- Retrospective cohort of 47 NSTI patients (overall mortality 17%)
- Surgery delayed beyond 12 h required far more debridements (7.4 vs 2.3, p<0.001)
- Delay beyond 12 h associated with more septic shock and acute kidney injury
- Effect persisted after adjustment for confounders
Clindamycin Suppresses Streptococcal Toxins
- In vitro study of 14 fully susceptible S. pyogenes isolates
- Clindamycin superior to penicillin at reducing SPE-A and SPE-B production
- Effect independent of bacterial growth phase (rationale for the Eagle effect)
- Supports adding clindamycin even to penicillin-susceptible GAS
IVIG in Streptococcal Toxic Shock (RCT)
- European randomised, double-blind, placebo-controlled trial in STSS
- Terminated early for slow recruitment (21 patients enrolled)
- 28-day mortality 3.6-fold higher in placebo group (not statistically significant)
- Significant improvement in SOFA score and superantigen neutralisation with IVIG
Key Evidence Points
For the exam, remember:
- LRINEC score has only 68% sensitivity - clinical judgement essential
- Delay to debridement is the key modifiable mortality driver (90h vs 25h, McHenry)
- Clindamycin inhibits toxin production - always include
- IVIG in STSS has one underpowered RCT (Darenberg) - supportive but not definitive
- Hyperbaric oxygen evidence is weak - should not delay surgery
Viva Practice Scenarios
Use these scenarios to practise clinical reasoning and management decisions
"A 55-year-old diabetic man presents with a painful, swollen right leg. He had a minor cut 3 days ago. He appears unwell with HR 120, BP 90/60, T 39.2°C. There is erythema from mid-calf to mid-thigh with woody induration. He has severe pain despite IV morphine. How would you manage this patient?"
"You are in theatre and have made an incision over the affected area. Describe what findings would confirm necrotizing fasciitis and your operative approach."
"A previously healthy 35-year-old woman presents with rapidly progressive leg pain and redness 2 days after a minor skin abrasion. Her LRINEC score is 4. What are your concerns and how would you proceed?"
Guidelines, Registries & Global Practice
Global Epidemiology
Necrotising fasciitis is uncommon but its incidence appears to be rising worldwide. Reported population incidence is approximately 0.4-1.0 per 100,000 per year in high-income countries, with overall mortality of 20-40% even in modern series. According to PubMed, the McHenry single-centre series reported 29% mortality and identified delay to debridement as the dominant determinant of death PMID 7748037, while the Stevens & Bryant NEJM review summarises the global microbiology and management of necrotising soft-tissue infections PMID 29211672.
Regional Microbiology & Risk Pattern Variation
| Setting | Predominant pattern | Notable organisms / risks |
|---|---|---|
| High-income (UK, Europe, North America, Australia) | Type I polymicrobial in diabetics/elderly; Type II GAS in healthy adults | Rising invasive GAS; MRSA in some regions |
| Coastal / tropical (N. Australia, SE Asia, US Gulf Coast) | Marine-acquired NSTI | Vibrio vulnificus (warm seawater, liver disease); Aeromonas (freshwater) |
| South & East Asia | Type I polymicrobial; high diabetes prevalence | Klebsiella, Vibrio, marine exposure |
| Resource-limited settings | Late presentation, higher mortality | Delayed access to theatre/ICU is the key driver |
Guideline Comparison
There is broad international consensus on the core principles - early surgical debridement, broad-spectrum antibiotics with clindamycin for toxin suppression, and aggressive resuscitation - although no high-quality randomised data exist for the surgical strategy itself.
Major Guidance on Necrotising Soft-Tissue Infection
| Body / Source | Position on diagnosis & timing | Antibiotic & adjunct guidance |
|---|---|---|
| WSES/SIS-E 2018 (Sartelli, global consensus) | Surgery is diagnostic and therapeutic; do not delay debridement for imaging; LRINEC supportive not exclusionary | Broad-spectrum empirical cover + clindamycin; IVIG may be considered in STSS |
| IDSA (USA) SSTI guideline | Urgent surgical exploration when NSTI suspected; tissue Gram stain/culture | Empirical broad-spectrum + clindamycin for GAS; narrow on culture |
| NICE / BOA-UK practice | Recognise sepsis early, immediate senior surgical referral, no delay for imaging | Local microbiology-guided broad-spectrum + clindamycin; sepsis-six resuscitation |
| Australian Therapeutic Guidelines (eTG) | High clinical suspicion mandates exploration; LRINEC adjunctive only | Piperacillin-tazobactam or meropenem + clindamycin ± vancomycin; benzylpenicillin + clindamycin for confirmed GAS |
Evidence Level of the Guidance
Almost all guideline recommendations on the surgical management of NSTI are based on observational data and expert consensus (low-grade evidence) - there are no RCTs of debridement timing or strategy. The strongest comparative evidence in this field is the Fernando 2019 meta-analysis on diagnostic accuracy PMID 29672405 and the Darenberg 2003 RCT of IVIG in STSS PMID 12884156. No dedicated NF registry exists; epidemiology is drawn from national infection surveillance (e.g. invasive GAS programmes) and single-centre cohorts.
Australian & Local Practice Notes
In Australia, NF is managed within the public hospital system with emergency surgical services at major metropolitan and regional centres; patients presenting to smaller rural hospitals may require urgent retrieval to facilities with ICU and surgical capability. The Therapeutic Guidelines (eTG) recommend piperacillin-tazobactam or meropenem combined with clindamycin and vancomycin empirically, with benzylpenicillin plus clindamycin first-line for confirmed GAS. Vibrio vulnificus is a recognised concern in tropical northern Australia during the warm months (October-April), and Aeromonas hydrophila in freshwater exposures, particularly northern Queensland.
Aboriginal and Torres Strait Islander Australians have higher rates of diabetes, chronic kidney disease and skin infection, increasing NF risk; renal dosing adjustments are frequently required, and family involvement and culturally safe wound care should inform management. For survivors requiring wound healing, referral to Quitline (13 7848) and nicotine replacement therapy supports cessation, which is critical for graft and wound success.
Necrotizing Fasciitis - Exam Rapid Review
Clinical summary
Classification
- •Type I: Polymicrobial (aerobic + anaerobic), diabetics, post-surgical, Fournier's
- •Type II: Monomicrobial (GAS, S. aureus), healthy adults, minor trauma
- •Type III: Clostridial (gas gangrene), Vibrio vulnificus (seawater)
Clinical Features
- •PAIN OUT OF PROPORTION - cardinal early sign
- •Hard signs: Crepitus, necrosis, bullae, dishwater pus - immediate surgery
- •Soft signs: Disproportionate pain, rapid spread, systemic toxicity, antibiotic failure
- •Woody induration - tense swelling beyond erythema
LRINEC Score
- •CRP greater than 150 (+4), WCC greater than 25 (+2), Hb less than 110 (+2)
- •Na less than 135 (+2), Creatinine greater than 141 (+2), Glucose greater than 10 (+1)
- •Score ≥6 intermediate risk, ≥8 high risk
- •CRITICAL: Sensitivity only 60-80% - clinical judgement trumps score
Finger Test
- •Bedside incision to fascia under local anaesthetic
- •Lack of bleeding indicates vessel thrombosis
- •Dishwater gray pus is pathognomonic
- •Necrotic fascia separates easily with finger dissection
- •If positive - proceed to extensive debridement
Antibiotics
- •Empiric: Piperacillin-tazobactam + Clindamycin + Vancomycin
- •GAS: Benzylpenicillin 2.4g IV q4h + Clindamycin 900mg IV q8h
- •ALWAYS include clindamycin - inhibits toxin production (Eagle effect)
- •Vibrio: Doxycycline + Ceftriaxone
Surgical Principles
- •Time is tissue - delay to debridement drives mortality (90h vs 25h, McHenry)
- •Debride until it bleeds - necrotic tissue does not bleed
- •Healthy fascia is adherent - necrotic fascia separates easily
- •Plan re-look at 24-48 hours - most need 2-4 debridements
- •Life over limb - amputate if refractory sepsis
Prognosis
- •Overall mortality 20-40%, up to 70% if delayed
- •Delay to debridement is the strongest modifiable mortality driver
- •GAS toxic shock - 30-70% mortality
- •Amputation required in 15-20%
Key Exam Phrases
- •Pain out of proportion = NF until proven otherwise
- •When in doubt, cut it out
- •The operating theatre is both diagnostic and therapeutic
- •Surgery should not be delayed for imaging
- •Clindamycin inhibits toxin production regardless of bacterial growth phase
References
-
Sartelli M, Guirao X, Hardcastle TC, et al. 2018 WSES/SIS-E consensus conference: recommendations for the management of skin and soft-tissue infections. World J Emerg Surg. 2018;13:58. doi:10.1186/s13017-018-0219-9
-
Stevens DL, Bryant AE. Necrotizing Soft-Tissue Infections. N Engl J Med. 2017;377(23):2253-2265. doi:10.1056/NEJMra1600673
-
Arif N, Yousfi S, Vinnard C. Deaths from necrotizing fasciitis in the United States, 2003-2013. Epidemiol Infect. 2016;144(6):1338-1344. doi:10.1017/S0950268815002745
-
Wong CH, Khin LW, Heng KS, Tan KC, Low CO. The LRINEC (Laboratory Risk Indicator for Necrotizing Fasciitis) score: a tool for distinguishing necrotizing fasciitis from other soft tissue infections. Crit Care Med. 2004;32(7):1535-1541. doi:10.1097/01.ccm.0000129486.35458.7d
-
Fernando SM, Tran A, Cheng W, et al. Necrotizing Soft Tissue Infection: Diagnostic Accuracy of Physical Examination, Imaging, and LRINEC Score: A Systematic Review and Meta-Analysis. Ann Surg. 2019;269(1):58-65. doi:10.1097/SLA.0000000000002774
-
Wilson MP, Schneir AB. A case of necrotizing fasciitis with a LRINEC score of zero: clinical suspicion should trump scoring systems. J Emerg Med. 2013;44(5):928-931. doi:10.1016/j.jemermed.2012.09.039
-
McHenry CR, Piotrowski JJ, Petrinic D, Malangoni MA. Determinants of mortality for necrotizing soft-tissue infections. Ann Surg. 1995;221(5):558-565. doi:10.1097/00000658-199505000-00013
-
Kobayashi L, Konstantinidis A, Shackelford S, et al. Necrotizing soft tissue infections: delayed surgical treatment is associated with increased number of surgical debridements and morbidity. J Trauma. 2011;71(5):1400-1405. doi:10.1097/TA.0b013e31820db8fd
-
Mascini EM, Jansze M, Schouls LM, Verhoef J, Van Dijk H. Penicillin and clindamycin differentially inhibit the production of pyrogenic exotoxins A and B by group A streptococci. Int J Antimicrob Agents. 2001;18(4):395-398. doi:10.1016/s0924-8579(01)00413-7
-
Darenberg J, Ihendyane N, Sjölin J, et al. Intravenous immunoglobulin G therapy in streptococcal toxic shock syndrome: a European randomized, double-blind, placebo-controlled trial. Clin Infect Dis. 2003;37(3):333-340. doi:10.1086/376630
-
Therapeutic Guidelines Limited. Therapeutic Guidelines: Antibiotic. Melbourne: Therapeutic Guidelines Limited.