Atrophic vs Hypertrophic | Stability | Biology
- Nonunion: Fracture that will not heal without intervention (9 months + no progress for 3 months)
- Hypertrophic = mechanical failure (unstable) → improve stability
- Atrophic = biological failure (avascular) → improve biology
- Infection must be excluded in all nonunions
- Diamond concept: Cells + scaffolds + growth factors + stability
- “Elephant foot = most callus, easiest to treat (just stabilize)
- “Horse hoof = less callus but still biological activity
- “Atrophic = avascular ends need resection, grafting
- “Smokers have 2x higher nonunion risk
Abundant callus (elephant foot, horse hoof). Bone is biologically active but unstable. Treatment: Increase stability (compression plating, exchange nailing). May not need bone graft.
No callus, bone ends avascular. Biological failure. Treatment: Resect avascular ends, bone graft, improve stability. May need Masquelet technique for bone loss.
All nonunions should have infection excluded. Bloods (CRP, ESR), aspirate/biopsy for culture. Treat as infected nonunion if positive (needs debridement + antibiotics).
Cells (osteogenic cells, MSCs) + Scaffolds (bone graft, BMP) + Growth factors (BMP, PRP) + Mechanical stability. Optimize all elements.
Overview
Nonunion is defined as a fracture that will not heal without intervention. Often defined as no radiographic progress for 3 consecutive months and at least 9 months from injury.
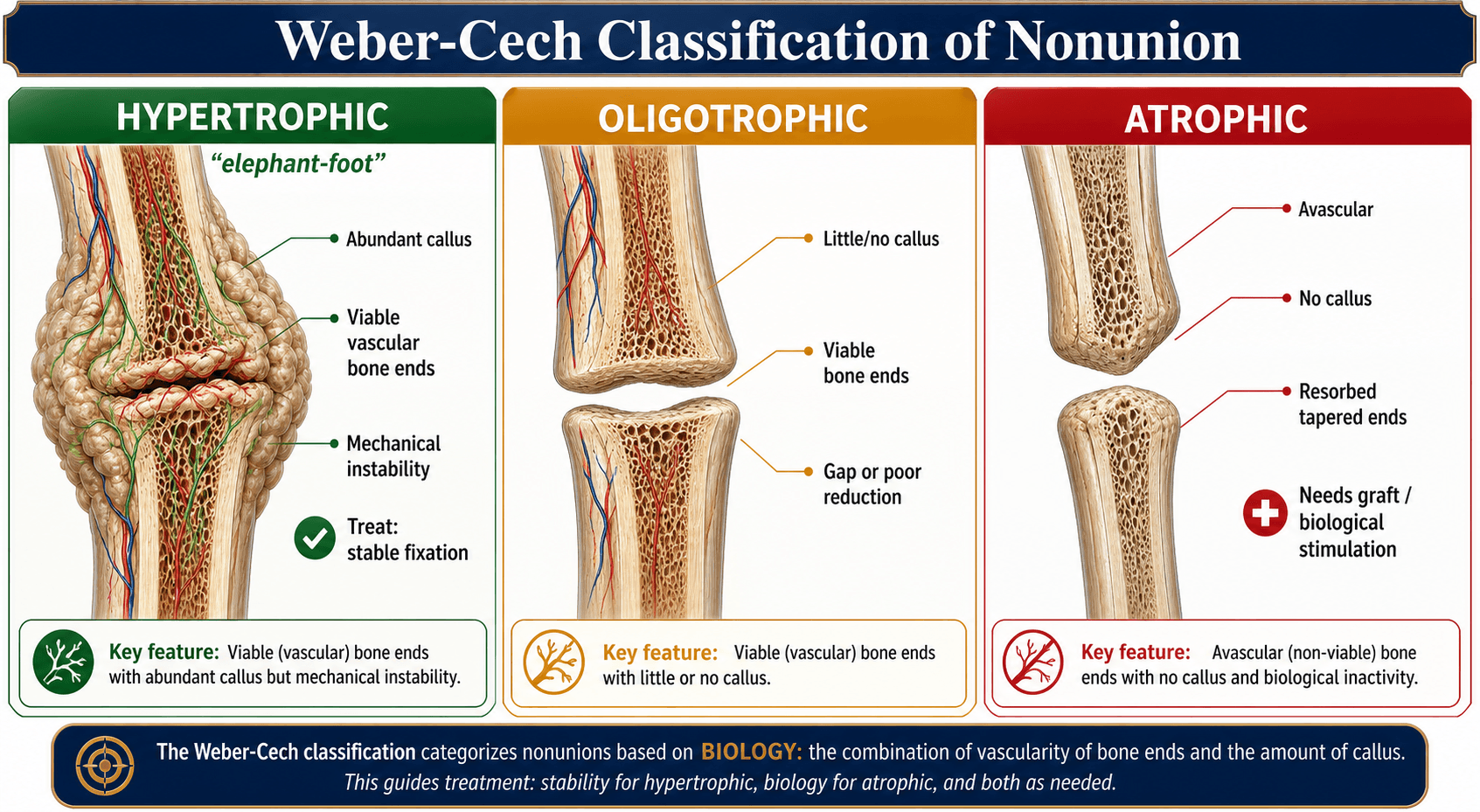
Weber-Cech Classification
Viable (Vascular) Nonunion:
- Hypertrophic (Elephant foot): Abundant callus, very vascular. Mechanical failure.
- Slightly Hypertrophic (Horse hoof): Less callus but some biological activity.
Non-viable (Avascular) Nonunion:
- Oligotrophic: Minimal callus, bone ends present but inactive.
- Atrophic: No callus, avascular ends. May be comminuted or with bone loss.
Pathophysiology
Normal Fracture Healing Process
Normal fracture healing proceeds through overlapping phases:
- Inflammation (Days 1-7): Hematoma formation, inflammatory cells, cytokines (IL-1, IL-6, TNF-α)
- Soft callus (Weeks 1-4): Chondrogenesis, fibrous callus formation
- Hard callus (Weeks 4-12): Woven bone replaces cartilage (endochondral ossification)
- Remodeling (Months to years): Woven bone replaced by lamellar bone, cortical restoration
Why Nonunion Develops
Nonunion occurs when the normal healing cascade is disrupted by mechanical or biological factors:
Mechanical Factors (Hypertrophic Nonunion):
- Excessive motion at fracture site prevents bridging
- Inadequate fixation (undersized nail, loose screws, plate failure)
- Distraction (gap greater than 2mm impairs bridging)
- Biology is intact (abundant callus visible), but instability prevents consolidation
Biological Factors (Atrophic Nonunion):
- Vascular disruption: Severe soft tissue injury (Gustilo IIIB/C), stripping of periosteum during surgery
- Avascular bone: Scaphoid waist, femoral neck (intracapsular), talus body
- Infection: Low-grade biofilm infection suppresses osteoblast function
- Metabolic: Diabetes, smoking (nicotine vasoconstriction), malnutrition, Vitamin D deficiency
- Medications: NSAIDs (inhibit COX-2 needed for bone healing), corticosteroids (impair osteoblast function)
The Diamond Concept
Giannoudis et al (2007) proposed the "Diamond Concept" - healing requires optimization of all four elements:
- Osteogenic cells (MSCs, osteoprogenitor cells from periosteum, bone marrow, circulation)
- Osteoconductive scaffold (bone graft matrix, collagen, HA/TCP ceramics)
- Osteoinductive signals (BMPs, PDGF, TGF-β, VEGF)
- Mechanical stability (absolute or relative depending on healing mechanism)
Fifth element (added later): Vascularity - adequate blood supply for oxygen, nutrients, cell delivery
Atrophic nonunion fails on biology (elements 1-3, 5). Hypertrophic nonunion fails on mechanics (element 4).
Infection and Nonunion
Biofilm formation:
- Bacteria (especially Staphylococcus epidermidis, Propionibacterium acnes) form biofilm on implants/bone
- Biofilm protects bacteria from antibiotics and immune system
- Bacterial toxins and inflammatory cytokines inhibit osteoblast function
- Result: Infected nonunion - will not heal without infection eradication
Clinical clue: Any nonunion with persistent pain, elevated CRP/ESR, or sinus drainage should be cultured.
Clinical Presentation
History
Patient presents months to years after initial fracture with:
Pain:
- Persistent pain at fracture site despite "adequate" healing time
- Pain with weight-bearing or activity (mechanical pain suggests instability)
- Constant pain or night pain (suggests infection or severe instability)
Functional Impairment:
- Unable to return to work or activities of daily living
- Ongoing use of walking aids (crutches, walker)
- Reduced range of motion of adjacent joints
Timeline:
- Typically greater than 9 months from injury
- No radiographic progression over 3 consecutive months (FDA definition)
- History of previous failed treatments (may have had bone grafting, revision fixation already)
Risk Factors to Elicit:
- Smoking (2-3x higher nonunion risk - dose dependent)
- NSAIDs (particularly high-dose, prolonged use post-fracture)
- Diabetes mellitus (especially if poorly controlled, HbA1c greater than 8%)
- Malnutrition (low albumin, low Vitamin D)
- Osteoporosis or metabolic bone disease
- Corticosteroid use (chronic, greater than 7.5mg prednisolone daily)
- Severe soft tissue injury at time of original fracture (Gustilo III open fracture)
Examination
Inspection:
- Muscle atrophy of limb (chronic disuse)
- Scars from previous surgeries
- Sinus tract (pathognomonic for infection if present)
- Swelling, erythema (infection)
- Malalignment (varus/valgus deformity, rotational)
Palpation:
- Tenderness at nonunion site
- Palpable gap or instability (if implants failed)
- Warmth (infection)
Movement:
- Abnormal motion at fracture site (should be stable if healed)
- Pain with stress (axial loading, bending, rotation)
- Adjacent joint stiffness (compensatory, prolonged immobilization)
Neurovascular Exam:
- Check for nerve injury from previous surgery or chronic hardware irritation
- Assess vascular status (chronic injury may have vascular compromise)
Red Flags for Infection
- Draining sinus
- Persistent pain despite apparently stable fixation
- Multiple failed surgeries without union
- Elevated inflammatory markers (CRP, ESR) at presentation
- Previous open fracture (Gustilo II/III)
Investigations
Imaging
Plain Radiographs:
- Orthogonal views (AP and lateral minimum)
- Look for:
- Callus formation (hypertrophic vs atrophic vs oligotrophic)
- Fracture line visibility (persistent gap, sclerosis of bone ends)
- Hardware position (loose screws - lucency around threads, broken plate/screws, nail backing out)
- Alignment (varus/valgus, angulation, rotation, shortening)
- Bone stock (comminution, bone loss, osteopenia)
CT Scan:
- Best for assessing bone healing (more sensitive than X-ray for cortical bridging)
- 3D reconstruction helps surgical planning (visualize deformity, bone stock, implant position)
- Identify sequestrum or bone loss in infected cases
MRI:
- Assess for infection (bone marrow edema, fluid collections, sinus tracts, soft tissue abscess)
- Evaluate vascularity of bone ends (signal characteristics)
- Less useful for bony detail than CT
Nuclear Medicine:
- Bone scan (Tc-99m MDP): High sensitivity but low specificity (increased uptake at nonunion regardless of infection)
- White cell scan (In-111 WBC) or FDG-PET: More specific for infection
- Not routinely needed - reserve for difficult cases where infection suspected but cultures negative
Laboratory Investigations
Exclude Infection (Essential):
- CRP (C-reactive protein): Elevated suggests infection (though may be mildly elevated in chronic nonunion without infection)
- ESR (erythrocyte sedimentation rate): Less specific, but persistently elevated concerning
- WBC count: Usually normal in chronic low-grade infection
- Tissue culture: Gold standard
- CT-guided biopsy or aspiration of nonunion site
- Minimum 5 tissue specimens (not swabs!)
- Prolonged culture (14 days) to catch slow-growing organisms (Propionibacterium, Cutibacterium)
Assess Metabolic/Nutritional Status:
- Vitamin D (25-OH Vitamin D): Target greater than 75 nmol/L for optimal bone healing
- Calcium, phosphate, alkaline phosphatase, PTH: Screen for metabolic bone disease
- Albumin, pre-albumin: Markers of nutritional status (low albumin = poor healing)
- HbA1c: If diabetic, target less than 7% for healing
- Thyroid function (TSH, free T4): Hyperthyroidism impairs healing
Specialized Tests (If Indicated):
- DEXA scan: Assess bone mineral density (osteoporosis)
- Bone turnover markers: CTX (resorption), P1NP (formation) - research use
- Genetic testing: Rare cases (osteogenesis imperfecta, hypophosphatasia)

Workup
Exclude Infection
Essential in all nonunions.
- Bloods: CRP, ESR, WCC
- Aspiration/biopsy: Culture (prolonged incubation for low-grade organisms)
- Imaging: MRI may show sequestrum, fluid collections
If infected nonunion: Treatment is different (debridement, antibiotic course, then reconstruction).
Address Modifiable Factors
- Smoking cessation (roughly doubles nonunion risk; cease at least 4 weeks pre-op)
- Optimize nutrition (protein, vitamins)
- Control diabetes (HbA1c)
- Avoid NSAIDs (may impair healing)
Differential Diagnosis of the Painful, Non-progressing Fracture
The pattern on imaging and inflammatory markers points to the diagnosis and dictates very different treatment.
- Callus / Radiograph
- Abundant callus (elephant foot / horse hoof), persistent line
- Biology vs Mechanics
- Mechanical failure, biology intact
- Infection markers
- Usually normal
- Key action
- Increase stability (exchange nail, compression plate)
- Callus / Radiograph
- Minimal callus, viable but quiet bone ends
- Biology vs Mechanics
- Mixed - often inadequate reduction/gap
- Infection markers
- Usually normal
- Key action
- Optimise reduction/stability +/- graft
- Callus / Radiograph
- No callus, tapered avascular sclerotic ends, possible gap
- Biology vs Mechanics
- Biological failure
- Infection markers
- Usually normal
- Key action
- Resect ends to bleeding bone + autograft + stable fixation
- Callus / Radiograph
- Lucency around implants, sequestrum, periosteal reaction
- Biology vs Mechanics
- Biology suppressed by biofilm
- Infection markers
- CRP/ESR often raised; may be normal
- Key action
- Deep tissue culture, staged debridement + antibiotics
- Callus / Radiograph
- Progressive callus, healing slower than expected
- Biology vs Mechanics
- Healing trajectory intact
- Infection markers
- Normal
- Key action
- Protect, optimise biology, observe
- Callus / Radiograph
- Lytic or blastic lesion, cortical destruction, soft-tissue mass
- Biology vs Mechanics
- Underlying lesion prevents healing
- Infection markers
- Variable
- Key action
- Staging, biopsy before any fixation
Measuring Union Objectively: the RUST and RUSH Scores
The Controversies section notes that "RUST/RUSH radiographic scores are increasingly used to quantify progression", and the entire definition of nonunion rests on "no radiographic progression" - but the topic never explains these scores or the positive criteria for union.
- The problem they solve. "Union" and "no progression" are subjective and poorly reproducible between observers. These scores make radiographic healing objective and reproducible, giving the otherwise arbitrary "9 months / 3 months without progression" definition a measurable anchor.
- RUST (Radiographic Union Score for Tibial fractures). Each of the four cortices seen on two orthogonal radiographs (anterior and posterior on the lateral view; medial and lateral on the AP view) is scored: 1 = fracture line visible with no callus; 2 = callus present but the fracture line is still visible; 3 = bridging callus with the fracture line gone. The four cortices sum to a total of 4 (no healing) to 12 (complete union). A modified RUST adds a fourth grade (remodelled / absent line) for finer discrimination.
- RUSH (Radiographic Union Score for Hip) is the analogous cortical-and-trabecular score validated for femoral neck fractures.
- How they are used. A rising score across serial films indicates progression; a low or plateauing score (for example a RUST that stops climbing well below 10 over three months) supports the diagnosis of nonunion and the need for intervention. They are also used as trial endpoints (for example the TRUST trial of LIPUS).
- The positive criteria for union combine this radiographic bridging (typically 3 of 4 cortices bridged, or a high RUST) with clinical union - no pain on weight-bearing or on stressing the fracture, and the ability to bear weight.
Q: How do you assess union objectively rather than by "eyeballing" the film? A: Use the RUST score - grade each of the four cortices on AP and lateral views (1 = no callus, 2 = callus but visible line, 3 = bridged, line gone), summing 4-12; a rising score means progression, a plateau well below 12 supports nonunion. RUSH is the femoral-neck equivalent. Combine radiographic bridging (roughly 3 of 4 cortices) with clinical union - painless weight-bearing and painless stressing of the fracture.
Management

Problem: Instability. Biology is good.
Solution: Improve stability.
Options:
- Compression plating (DCP with compression mode)
- Exchange nailing (larger, stiffer nail)
- Additional fixation (add locking plate, cerclage)
May not need bone graft - biology is sufficient.
The Reamer-Irrigator-Aspirator (RIA) Autograft
"RIA graft" is named in the atrophic-treatment options, the management algorithm and a viva (and its 500-800 mL blood loss is listed as a complication), but the topic never explains what it is - despite it being the answer to "where do I get enough autograft for a large atrophic or segmental defect?"
- What it is. The Reamer-Irrigator-Aspirator is a single-pass intramedullary reaming system that reams the femoral (or tibial) canal while simultaneously irrigating and aspirating, collecting the reamings in an in-line filter. It harvests a large volume of autologous cancellous bone and marrow from inside the long bone.
- Why it matters in nonunion. Iliac crest bone graft yields a limited volume and carries significant donor-site pain; a large atrophic or segmental defect - or the graft needed to fill a Masquelet membrane - may require more graft than one iliac crest can provide. RIA delivers a large volume (often 40-90 mL) of biologically rich graft containing osteogenic cells, an osteoconductive matrix and osteoinductive growth factors (three arms of the diamond concept), with generally less chronic donor-site pain than iliac crest harvest.
- The trade-offs (which this topic already flags). RIA carries a real blood-loss burden (roughly 500-800 mL) and a risk of iatrogenic fracture, cortical perforation or eccentric over-reaming of the donor bone; it needs an intact, adequately-sized donor canal. The contralateral femur is the usual donor for a femoral or tibial recipient.
- Where it sits. RIA is a harvest technique, not a different graft - the product is autograft, so it complements rather than replaces the diamond-concept biology. (General graft-type selection is covered in the bone-grafts topic; for the large-volume autograft needed in atrophic or segmental nonunion, RIA is the workhorse.)
Q: How do you obtain enough autograft for a large atrophic or segmental nonunion? A: Use the Reamer-Irrigator-Aspirator (RIA) - a single-pass intramedullary reamer that irrigates and aspirates the canal (usually the contralateral femur), harvesting a large volume (about 40-90 mL) of biologically rich autograft (cells, matrix, growth factors) with less chronic donor-site pain than iliac crest. Weigh this against its 500-800 mL blood loss and the risk of iatrogenic fracture/over-reaming; it needs an intact donor canal. It is a harvest technique - the graft is still autograft.
Complications
Complications of Nonunion Itself
Functional Impairment:
- Chronic pain (mechanical or neuropathic)
- Loss of limb function (inability to work, ADL dependence)
- Adjacent joint arthritis (abnormal loading, stiffness from prolonged immobilization)
- Muscle atrophy and weakness
- Psychological impact: Depression, anxiety, reduced quality of life
Deformity:
- Malalignment: Varus/valgus angulation, rotational deformity, shortening
- Limb length discrepancy (up to several centimeters in atrophic nonunion with bone resorption)
- Secondary degenerative changes in adjacent joints
Infection:
- Up to 10% of nonunions are infected (occult low-grade infection)
- Biofilm formation on implants
- Chronic draining sinus
- Osteomyelitis
Complications of Nonunion Surgery
Intraoperative:
- Bleeding: Particularly with takedown of hypertrophic callus, RIA grafting (500-800mL blood loss)
- Nerve injury: Iatrogenic (radial nerve during plating, peroneal nerve during tibial work)
- Vascular injury: Dissection through scarred tissue planes
- Fracture: Intraoperative fracture during hardware removal or reaming
Early Post-operative:
- Infection: Surgical site infection (2-5%), deep infection requiring implant removal (1-2%)
- Wound dehiscence: Poor soft tissue envelope, tension on closure
- Compartment syndrome: Particularly lower limb after extensive surgery
- DVT/PE: Prolonged surgery, re-operation risk factor
Late Complications:
- Re-nonunion: Failure of bone graft to incorporate (5-15% even with appropriate treatment)
- Donor site morbidity: Iliac crest pain (chronic in 5-10%), hematoma, infection, nerve injury (lateral femoral cutaneous nerve numbness in 10%)
- Hardware failure: Plate breakage, screw loosening (more likely if biology inadequate)
- Malunion: Despite union, alignment may be suboptimal
- Reflex sympathetic dystrophy (CRPS): Chronic pain, stiffness, vasomotor changes (1-2%)
Complications Specific to Treatment Methods
Exchange Nailing:
- Femoral or tibial fracture during reaming or nail insertion (1-2%)
- Nail malposition
- Cortical perforation with reaming
Bone Grafting:
- Graft resorption without incorporation (particularly large structural grafts)
- Fracture through graft site if loaded prematurely
Bone Transport (Ilizarov):
- Pin tract infection (almost universal, 20-30% require antibiotics)
- Nerve damage (peroneal nerve palsy 5-10% in tibial transport)
- Joint stiffness (knee, ankle contractures from prolonged external fixation)
- Refracture after frame removal (5-10%)
- Prolonged treatment time (12-24 months), significant patient burden
- Equinus deformity in tibial transport if frame malpositioned
Vascularized Fibula Graft:
- Flap failure (arterial/venous thrombosis 5-10%)
- Donor site morbidity: Ankle instability, numbness (sural nerve), gait disturbance
- Stress fracture of fibula graft before consolidation
- Requires microsurgery expertise - not widely available
BMP (Bone Morphogenetic Protein):
- Heterotopic ossification (ectopic bone in soft tissues - up to 30% in some series)
- Swelling (inflammatory response to rhBMP-2)
- Cost (very expensive, often not covered)
- Off-label use in long bones (only FDA-approved for tibial shaft, ALIF spine fusion)
- Potential carcinogenicity (theoretical concern with supraphysiologic doses - not proven)
Worst-Case Scenario: Amputation
Indications for Amputation:
- Multiple failed reconstructions (persistent nonunion after 2-3 surgeries)
- Chronic infection not controllable with limb salvage
- Severe soft tissue loss (inadequate coverage)
- Neuropathic limb (insensate foot, severe nerve injury)
- Patient preference (after informed consent - some patients choose amputation over prolonged unsuccessful limb salvage)
Amputation may provide:
- Pain relief (better than chronic pain from unstable nonunion)
- Faster return to function (modern prosthetics enable good mobility)
- End to repeated surgeries
Guidelines, Registries & Global Practice
Global Epidemiology
- Tibial shaft fractures carry the highest long-bone nonunion rate; pooled prevalence is approximately 7% (Tian et al, 2020), rising sharply with open, high-energy and Gustilo IIIB/IIIC injuries.
- Smoking roughly doubles nonunion risk worldwide (OR ~2.5); diabetes, NSAID use, BMI over 40, age over 60 and infection are consistent global risk factors.
- In limited-resource settings, delayed presentation, open injuries from road traffic trauma, and constrained access to implants and microsurgery shift the burden toward established and infected nonunion.
Guidelines & Society Positions, Side by Side
- Emphasis
- Diamond concept - analyse stability and biology together
- Practical recommendation
- Match construct to fracture personality; reamed exchange nailing for diaphyseal aseptic nonunion; staged management for infection
- Emphasis
- Open fracture and bone-infection pathways
- Practical recommendation
- Combined orthoplastic care, early specialist transfer, multidisciplinary management of infected nonunion
- Emphasis
- Adjuncts and biologics evidence appraisal
- Practical recommendation
- Biophysical stimulation (LIPUS/PEMF) not supported as a substitute for surgical correction of stability/biology
- Emphasis
- Defect reconstruction strategy
- Practical recommendation
- Induced membrane (Masquelet) and distraction osteogenesis as complementary options selected by defect size, infection and host
Where guidance genuinely converges: exclude infection in every nonunion, correct the dominant deficit (mechanics vs biology), optimise modifiable host factors, and refer complex segmental or infected cases to units with limb-reconstruction and orthoplastic capability.
Registry & Outcome Evidence
- Arthroplasty-style national registries (NJR, AJRR, AOANJRR, Swedish/Norwegian) do not track diaphyseal nonunion directly, but trauma and fracture-outcome datasets consistently identify open tibial fractures, infection and smoking as the dominant drivers of revision for nonunion.
- Reported union rates: reamed exchange nailing ~90% in selected aseptic tibial nonunion; induced membrane technique ~84-90% across long bones and tibia-specific series.
Practice Variation by Resource Setting
- High-resource: routine deep-tissue culture with prolonged incubation, RIA autograft, antibiotic-loaded cement spacers, rhBMP-2 as off-label salvage, microvascular free fibula, and circular frames available.
- Limited-resource: reliance on iliac crest autograft, conventional external fixation and bone transport over costly biologics; emphasis on infection control, soft-tissue coverage and modifiable-factor optimisation. Antibiotic cement spacers (gentamicin/vancomycin-loaded PMMA) remain a low-cost, widely applicable standard for staged infected-nonunion care.
- Antibiotic principles (global): empiric cover then de-escalation guided by deep-tissue culture and sensitivities, typically around 6 weeks of targeted therapy before definitive reconstruction in infected nonunion, in conjunction with infectious-diseases input.
Controversies & Areas of Uncertainty
Nonunion management carries several genuinely unresolved debates that examiners use to separate safe from outstanding candidates.
- Definition and timing. The "9 months plus 3 months without progression" FDA wording is a regulatory construct, not a biological truth. Many surgeons now diagnose nonunion functionally when union is not expected to occur without intervention regardless of an arbitrary calendar threshold, and tools such as the RUST/RUSH radiographic scores are increasingly used to quantify progression.
- Reamed versus unreamed exchange nailing. Reaming delivers local autograft and a larger, stiffer nail, but the thermal and vascular cost in a compromised diaphysis is debated; the benefit is clearest in hypertrophic patterns and least convincing in atrophic biology.
- rhBMP-2: efficacy versus harm and cost. Despite the BESTT data, routine use in long-bone nonunion is off-label, expensive and associated with heterotopic ossification and inflammatory swelling. Enthusiasm has cooled, and many units reserve it for salvage or graft-volume problems rather than first-line use.
- Masquelet versus distraction osteogenesis (bone transport). For segmental loss there is no high-quality head-to-head trial. Masquelet offers a shorter, more predictable timeline; bone transport avoids large graft harvest and corrects length/deformity but carries prolonged frame time and a high pin-site burden. Choice remains surgeon- and patient-specific.
- Biophysical adjuncts. Low-intensity pulsed ultrasound (LIPUS) and pulsed electromagnetic fields are widely marketed, but large pragmatic trials (e.g. the TRUST trial of LIPUS in tibial fractures) showed no clinically important benefit, so they are not a substitute for addressing stability and biology.
- When to stop limb salvage. The threshold for converting to amputation after repeated failed reconstructions is value-laden; modern prosthetics and shared decision-making mean amputation is a legitimate, sometimes superior, functional choice rather than a failure.
Essential Mnemonics
SCGMSDiamond Concept (Enhanced)
Hook:SCGMS = Diamond Concept for healing (Stability, Cells, Growth, Matrix, Supply)!
HABTreatment Selection
Hook:HAB = Hypertrophic fix, Atrophic graft, Big defect reconstruct!
MCQ Practice Points
Q: What distinguishes hypertrophic from atrophic nonunion?
A: Hypertrophic nonunion: Abundant callus ("elephant foot" or "horse hoof"), adequate blood supply, lacks mechanical stability. Treatment: improved fixation alone. Atrophic nonunion: No callus, avascular bone ends, requires biological stimulation. Treatment: bone graft + stable fixation. Radiographic appearance guides treatment strategy.
Q: What are the four components of the Diamond Concept for nonunion treatment?
A: The Diamond Concept requires: 1) Osteogenic cells (mesenchymal stem cells), 2) Osteoconductive scaffold (bone graft matrix), 3) Osteoinductive factors (BMPs, growth factors), 4) Mechanical stability (adequate fixation). All four elements must be optimized for successful union. Fifth element added: vascularity.
Q: What is the definition of delayed union versus nonunion?
A: Delayed union: Fracture not healed by expected time but showing progressive healing signs (typically 3-6 months depending on location). Nonunion: Fracture that will not heal without intervention - typically defined as no radiographic progression over 3 consecutive months or failure to unite by 9 months. FDA definition: 9 months without healing.
Q: What investigation is essential before treating an apparent nonunion?
A: Infection must be excluded before treating any nonunion. Investigations: ESR, CRP, WBC count, and tissue cultures (not swabs). Consider CT-guided biopsy for deep infections. Infected nonunion requires debridement, antibiotics, and staged reconstruction. Up to 10% of nonunions are occultly infected.
Q: What is the role of exchange nailing in tibial shaft nonunion?
A: Exchange nailing (reaming + larger diameter nail) achieves 70-90% union rates in hypertrophic tibial nonunions. Mechanism: Reaming provides local bone graft, improves nail-cortex contact, and increases stability. Best for hypertrophic nonunions. May add dynamization or bone graft augmentation for atrophic patterns.
At a Glance
Nonunion is defined as a fracture that will not heal without intervention (typically no radiographic progress for 3 months and greater than 9 months from injury). The Weber-Cech classification distinguishes hypertrophic (elephant foot/horse hoof with abundant callus - mechanical failure requiring stability) from atrophic (no callus, avascular ends - biological failure requiring bone graft and stability). All nonunions must have infection excluded (CRP, ESR, aspirate/biopsy for culture). The Diamond Concept guides treatment: optimise cells (osteogenic cells), scaffolds (bone graft), growth factors (BMP), and mechanical stability. Key: hypertrophic just needs compression plating; atrophic needs resection of avascular ends plus biological augmentation.
VITAMIN DCauses of Nonunion
Hook:VITAMIN D = causes of nonunion (Vascular, Infection, Tissue, Age, Motion, Inadequate, Drugs)!
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A patient has a tibial shaft fracture that was treated with IM nailing 12 months ago. X-rays show no healing and abundant callus (hypertrophic). How do you manage?”
“A 45-year-old man sustained an open femoral shaft fracture in a motor vehicle accident 15 months ago. He was initially treated with debridement and intramedullary nailing. X-rays at 15 months show no healing with a 6cm bone defect and atrophic bone ends with no callus formation. The nail appears loose with some backing out proximally. He has persistent thigh pain and cannot weight-bear. CRP is 8 (normal), ESR 15 (normal). How do you assess this patient and what are your treatment options for this challenging nonunion?”
“A 52-year-old diabetic woman presents with persistent tibial nonunion 18 months after initial plating and bone grafting for a closed tibial fracture. She has already undergone one revision surgery 6 months ago where the plate was changed to a longer plate with additional bone graft, but there is still no healing. She complains of ongoing pain and occasional serous discharge from one of the old screw holes. X-rays show atrophic nonunion with lucency around several screws. CRP is 25, ESR 45. The referring surgeon is planning another attempt at plating with BMP augmentation and asks for your opinion. What is your assessment and how would you proceed?”
Classification
- Hypertrophic: Abundant callus, unstable
- Atrophic: No callus, avascular
- Exclude infection in all cases
Hypertrophic Treatment
- Problem: Instability
- Solution: Increase stability
- Exchange nail, compression plate
Atrophic Treatment
- Problem: Biology (avascular)
- Solution: Resect ends + bone graft
- Autograft, BMP, stable fixation
Modifiable Factors
- Smoking cessation
- Optimize nutrition
- Avoid NSAIDs, control diabetes
Evidence Base
Diamond Concept of Fracture Healing - Foundational Framework
- Proposed expanding the classic tissue-engineering triangle (cells, scaffold, growth factors) into a four-element 'diamond' by adding mechanical stability
- Argues the mechanical environment is consistently underestimated and must be given equal weight to biology
- Conceptual basis for the modern strategy of analysing every nonunion as a cell, scaffold, signal and stability problem
- Vascularity later incorporated as a fifth contributing element
Exchange Nailing for Aseptic Tibial Shaft Nonunion
- Prospective series of 25 consecutive tibial shaft aseptic nonunions previously nailed, treated by reamed exchange nailing
- 24 of 25 (96%) united at a mean of 4 months (range 3-6 months)
- The single failure united after a subsequent cancellous bone graft
- No wound infection or malunion; selection required under 1 cm shortening and no segmental defect
rhBMP-2 for Open Tibial Fractures - BESTT RCT
- Prospective, randomised, controlled, single-blind multicentre trial of 450 acute open tibial shaft fractures treated with IM nailing
- 1.50 mg/mL rhBMP-2 reduced the risk of secondary intervention for delayed/nonunion by 44% versus standard care (RR 0.56, 95% CI 0.40-0.78, p=0.0005)
- Fewer invasive secondary procedures (bone grafting, nail exchange), faster fracture and wound healing
- Fewer infections in Gustilo type III injuries with the higher dose
Masquelet (Induced Membrane) Technique - Systematic Review
- Systematic review of 17 studies (427 patients) of the induced membrane technique in long bones, defect length 0.6-26 cm
- Bone union achieved in 89.7% and infection eradicated in 91.1% of cases
- Persistent infection or nonunion requiring further surgery in 18%; deep surgical site infection 4.4%
- Need for reintervention correlated with poorer union; infected indications carried higher complication risk
Masquelet Technique for Tibial Segmental Defects - Meta-analysis
- Random-effects meta-analysis of 30 studies, 643 tibiae with segmental bone loss
- Pooled union rate 84% (95% CI 79-88%)
- No statistically significant association between defect size and union rate (p=0.11) - large defects can still unite
- Confirms effectiveness of the induced membrane technique even for large tibial defects
Smoking and Bone Healing - Systematic Review and Meta-analysis
- Systematic review of 122 studies (417,767 patients); meta-analysis of 71 studies (39,920 patients) of non-pathological fractures
- Nonunion significantly more common in smokers: OR 2.50 (95% CI 1.73-3.61)
- Alcohol consumption showed no significant association with nonunion (OR 0.97)
- Smoking cessation at least 4 weeks before surgery reduced postoperative wound infection (OR 0.37)
Prevalence and Risk Factors for Tibial Nonunion - Meta-analysis
- Meta-analysis of 111 studies, 41,429 patients with tibial fractures
- Pooled nonunion prevalence 6.8% - the tibia is the long bone most prone to nonunion
- 15 significant risk factors including age over 60, male sex, smoking, BMI over 40, diabetes, NSAID use, open fracture, Gustilo IIIB/IIIC and infection
- Closed reduction and MIPPO associated with lower nonunion risk