Obturator Nerve Anatomy
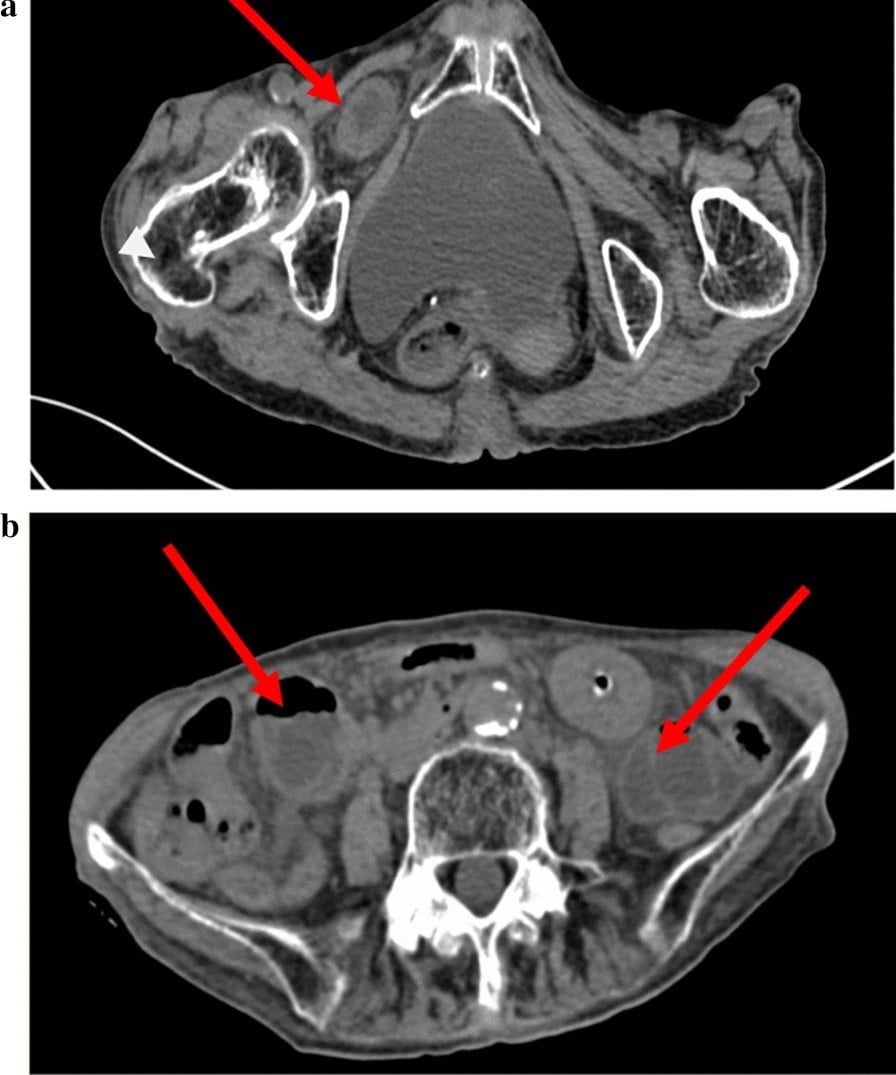
Medial thigh/knee pain and paraesthesia provoked by hip extension, adduction or internal rotation, relieved by hip flexion. It reflects obturator nerve compression - classically by an obturator hernia (typically a thin, elderly woman with bowel obstruction).
It is an easily-missed cause of bowel obstruction and groin/medial-knee pain. Recognising the sign points to the obturator canal and prompts the right imaging - a high-yield exam association.
OAFPObturator vs Femoral Nerve
Hook:Obturator = Anterior divisions/Adductors; Femoral = Posterior divisions/quadriceps.
Overview
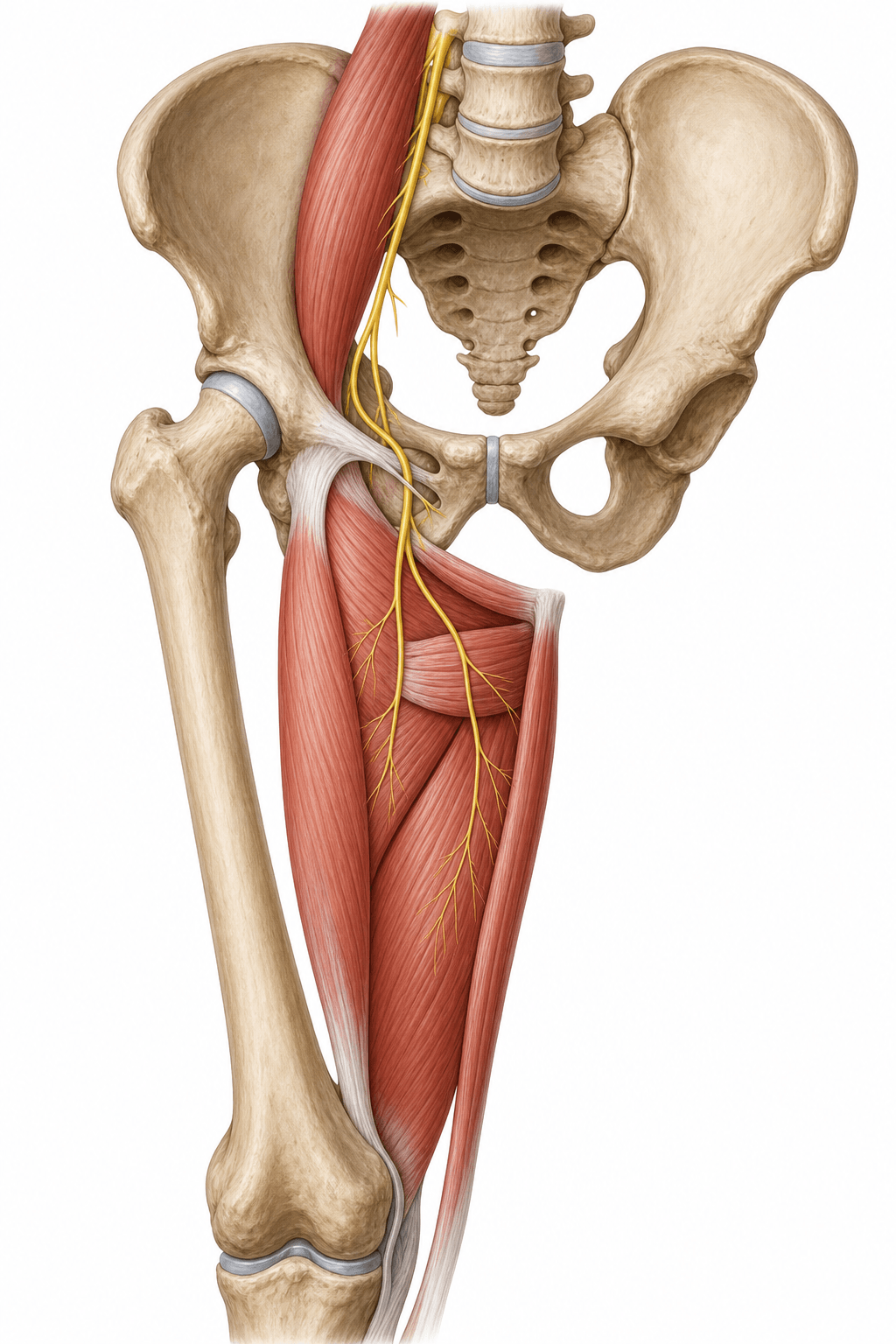
The obturator nerve is the principal nerve of the medial (adductor) compartment of the thigh. It is one of the two major nerves of the lumbar plexus that share the L2–L4 roots — and the recurring exam theme is the mirror-image contrast with the femoral nerve: same roots, but the obturator takes the anterior divisions and exits the medial border of psoas, while the femoral takes the posterior divisions and exits the lateral border. Functionally it does one main job — thigh adduction — but it punches above its weight in exams because of three clinical hooks: it refers pain from the hip to the medial knee (articular branches to both joints), it is the nerve of the Howship-Romberg sign in obturator hernia, and its proximal segment and neighbouring corona mortis vessels are surgical hazards in the pelvis.
Origin & Course
Origin
- The obturator nerve arises from the anterior divisions of the anterior rami of L2, L3 and L4.
- This contrasts with the femoral nerve (same roots, but posterior divisions).
- It forms within psoas major and emerges from its medial border (the femoral nerve emerges from the lateral border - a classic comparison).
Innervation: Motor, Sensory & Articular Supply
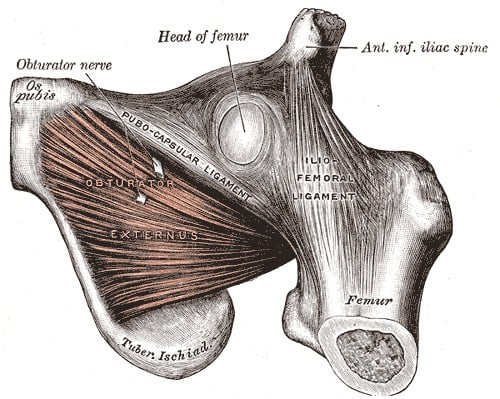
The obturator nerve is the motor nerve of the thigh adductor compartment: adductor longus, adductor brevis, gracilis, obturator externus, and the adductor part of adductor magnus (the hamstring part of adductor magnus is supplied by the sciatic/tibial division).
- Action: adduction of the thigh (and gracilis assists knee flexion/medial rotation).
- Sensory: a variable patch of medial thigh skin via the cutaneous branch of the anterior division (the accessory obturator nerve, when present, is a minor variant).
- Articular: branches to both the hip and the knee, explaining why hip pathology can refer to the medial knee.
Adductors + 2 (gracilis, obturator externus)Muscles supplied by the obturator nerve
Hook:All the adductors (longus, brevis, magnus-adductor-part) plus gracilis and obturator externus. Adductor magnus has DUAL supply (obturator + sciatic); pectineus is the variant via the accessory obturator nerve.
Surgical Anatomy: Corona Mortis, Variants and the Block
The obturator region carries three pieces of surgical anatomy that examiners reliably probe beyond the basic course.
Corona mortis — the "crown of death"
The corona mortis is a vascular anastomosis between the obturator system and the external iliac / inferior epigastric system, running across the superior pubic ramus behind the pubis. It may be venous, arterial, or both, and is present in a large proportion of pelvises (commonly quoted as up to around 80 percent when venous connections are included). It earned its name because it is encountered — and can be torn with torrential, hard-to-control bleeding — during the anterior intrapelvic (modified Stoppa) approach, during plating of the quadrilateral plate and superior pubic ramus, and in pubic ramus fractures. It typically lies roughly 4 to 9 cm lateral to the pubic symphysis, so the surgeon must identify, ligate or avoid it when working along the superior pubic ramus.
When working on the superior pubic ramus or quadrilateral plate (Stoppa or ilioinguinal approach), deliberately look for the corona mortis behind the pubis a few centimetres lateral to the symphysis and ligate it under direct vision. An uncontrolled avulsion retracts into the pelvis and bleeds catastrophically — the "crown of death".
Accessory obturator nerve
In roughly 10 to 30 percent of people an accessory obturator nerve (usually from L3–L4 anterior divisions) is present. Instead of passing through the obturator canal it crosses over the superior pubic ramus (rather than through the foramen), supplies pectineus, and contributes to the hip joint. It is clinically relevant because it can be spared during an obturator nerve block, leaving residual adductor function or an incomplete block.
Obturator nerve block
The block is used for adductor spasticity (e.g. cerebral palsy), as an analgesic adjunct for knee surgery, and crucially to abolish the adductor "jerk" during transurethral resection of a lateral bladder wall tumour (where stimulation of the nerve by the resectoscope causes a violent adduction that can perforate the bladder). The classic landmark approach is at the pubic tubercle / obturator canal; an interfascial (adductor canal–level) approach between adductor longus/brevis and brevis/magnus targets the divisions more selectively. Remember the accessory obturator nerve as a cause of an incomplete block.
A classic regional-anaesthesia trap: the inguinal femoral "3-in-1" block (a single femoral injection intended to spread to the femoral, lateral femoral cutaneous AND obturator nerves) — and likewise the fascia iliaca block — do NOT reliably anaesthetise the obturator nerve, because the obturator has already diverged medially within the pelvis and lies in a separate fascial plane by the time of the groin injection. So when obturator block is genuinely required — for medial-knee / adductor analgesia in knee surgery, for adductor spasticity, or to abolish the adductor jerk during lateral-wall TURBT — a dedicated, separately-targeted obturator block must be performed (and an accessory obturator nerve can still leave even that incomplete). The exam point: never assume a femoral / 3-in-1 or fascia iliaca block has covered the obturator territory.
Do not confuse the Howship-Romberg sign (obturator-nerve compression by an obturator hernia → medial thigh/knee pain on hip extension/adduction/internal rotation) with the obturator test/sign of appendicitis or a pelvic abscess (pain on passive internal rotation of the FLEXED hip, from irritation of obturator internus by an inflamed pelvic structure). Same muscle/nerve region, completely different clinical context.
Clinical Correlations
Causes
- Pelvic surgery: pelvic lymph node dissection (e.g. during radical prostatectomy), gynaecological surgery, and acetabular/quadrilateral-plate fracture fixation - the proximal nerve is the highest-risk segment.
- Obturator hernia: compression in the obturator canal producing the Howship-Romberg sign.
- Hip surgery / arthroscopy and pelvic masses.
- Adductor spasticity is treated with obturator nerve blocks/neurectomy in cerebral palsy.
Chronic obturator neuropathy is a recognised cause of exercise-induced groin pain in athletes. Distinct from the acute compressions above (hernia, pelvic surgery), it is a fascial entrapment of the ANTERIOR branch where it pierces the fascia over adductor brevis (the Bradshaw lesion), seen in kicking and skating sports (footballers, Australian-rules players, ice-hockey players). The picture is exercise-induced medial-thigh / adductor-region pain with adductor weakness or fatigue that comes on with activity and eases with rest — easily mislabelled "adductor strain" or "sportsman's groin." Diagnosis is clinical, supported by EMG showing denervation of the adductors, after excluding the other causes of chronic groin pain (adductor tendinopathy, inguinal/sports hernia, osteitis pubis, hip impingement). Treatment is surgical neurolysis / release of the entrapping fascia over adductor brevis, which reliably relieves symptoms in confirmed cases. The exam point: obturator trouble is not only the elderly hernia — think fascial entrapment in the young athlete with activity-related adductor pain.
Guidelines, Registries & Global Practice
Global Practice Picture
Obturator nerve anatomy is foundational for pelvic and acetabular surgery and for regional anaesthesia. Internationally consistent teaching points are: protect the proximal nerve during pelvic lymph node dissection and quadrilateral-plate fixation; recognise the Howship-Romberg sign of obturator hernia; and use the obturator block for adductor spasticity and to prevent the adductor jerk in bladder surgery.
Side-by-Side Synthesis
- Obturator nerve
- L2-L4 anterior divisions
- Femoral nerve (for contrast)
- L2-L4 posterior divisions
- Obturator nerve
- Medial border
- Femoral nerve (for contrast)
- Lateral border
- Obturator nerve
- Obturator canal
- Femoral nerve (for contrast)
- Under inguinal ligament
- Obturator nerve
- Thigh adductors
- Femoral nerve (for contrast)
- Quadriceps
- Obturator nerve
- Medial thigh
- Femoral nerve (for contrast)
- Anterior thigh + saphenous
- Obturator nerve
- Obturator hernia (Howship-Romberg), PLND
- Femoral nerve (for contrast)
- Anterior THA retractor, iliacus haematoma
Evidence Base
Anatomy topics rest on cadaveric and clinical-series evidence rather than trials. The two studies below were checked against their PubMed records: the Heilbronn series quantifies the clinical danger zone (the proximal obturator nerve accounts for the large majority of pelvic-dissection injuries, though absolute injury rates are very low), and the Goubier cadaveric study underpins the obturator-to-femoral nerve transfer — useful mainly as proof of the close functional relationship between the two L2–L4 nerves. Neither is high-level outcome evidence; for an anatomy viva the reproducible cadaveric relations and the named clinical signs (Howship-Romberg, corona mortis) matter more than any single paper.
Is It Possible to Draw a Risk Map for Obturator Nerve Injury During Pelvic Lymph Node Dissection? The Heilbronn Experience and a Review of the Literature
- Series of 3558 laparoscopic/robotic radical prostatectomies; obturator nerve injury in 0.1% during pelvic lymph node dissection
- Across the literature the PROXIMAL part of the obturator nerve accounts for ~77.8% of reported injuries
- Recognising injury intra-operatively allowed successful simultaneous repair (clip removal or microsuture)
- No long-term adductor or neurologic deficit after timely repair
Transfer of two motor branches of the anterior obturator nerve to the motor portion of the femoral nerve: an anatomical feasibility study
- Cadaveric feasibility study transferring obturator motor branches (to gracilis/adductor longus) to the motor portion of the femoral nerve
- Tension-free direct neurorrhaphy was possible in all specimens (mean overlap 26 mm; matched nerve diameters)
- Access in the thigh was straightforward compared with pelvic transfer
- Proposed as a reproducible reconstruction for proximal femoral nerve injury