Craniocervical Junction Instability
- NEVER apply traction to a distraction-type atlanto-occipital dissociation - it further distracts the disrupted junction and can kill or cause devastating cord injury. This is the single most important safety point. Rigid immobilisation instead.
- AOD is a measurement/ligamentous diagnosis - the bones often look aligned. Actively measure the C1-condyle interval (CCI, the MOST sensitive sign) on CT; do not be reassured by a "normal-looking" lateral.
- The CCI is far more sensitive than the older criteria - Harris BDI/BAI, Powers and Wholey ratios miss a large fraction of AOD (Harris ~27% sensitive, Powers ~55%). Know CCI as the lead measurement.
- Children are predisposed (horizontal condyles, large head) - have a low threshold in the paediatric high-energy trauma.
- Screen the atraumatic at-risk groups - rheumatoid arthritis (pannus, cranial settling), Down syndrome (laxity, os odontoideum) - especially before intubation/anaesthesia.
- Match the fusion to the level - C1-C2 fusion for isolated atlanto-axial instability, but INCLUDE the occiput (C0-C2) when the occipito-atlantal junction is disrupted.
Overview & Epidemiology
Craniocervical junction (CCJ) instability spans two very different clinical worlds: a catastrophic high-energy traumatic injury (atlanto-occipital dissociation, AOD) and an insidious atraumatic instability in predisposed patients. Both matter because the upper cervical cord and brainstem are at stake.
- Traumatic AOD - a rare, highly unstable distraction injury from motor-vehicle and pedestrian trauma; historically often fatal at the scene, though better pre-hospital care has improved survival and detection. Children and young adults are over-represented (more horizontal occipital condyles, a relatively large head).
- Atraumatic instability - rheumatoid arthritis (the classic), Down syndrome, and congenital os odontoideum / skeletal dysplasias produce slowly progressive atlanto-axial or occipito-atlantal instability, sometimes with myelopathy.
- Why it is examinable: AOD is lethal and easily missed, the no-traction rule is a hard safety point, and the at-risk-group screening (RA, Down) is a recurring clinical-governance theme.
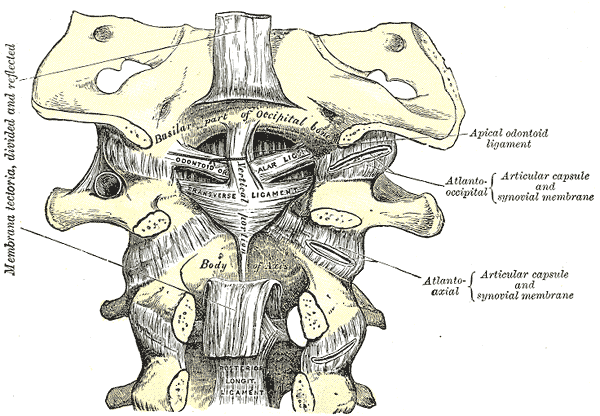
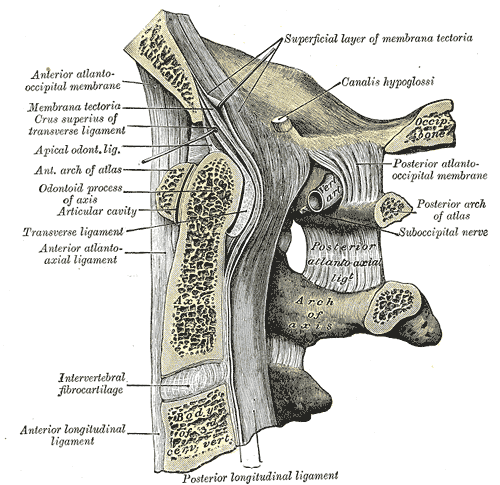
Anatomy — a ligament-dependent junction
The craniocervical junction (CCJ) — the occiput, atlas (C1) and axis (C2) — provides nearly half of cervical flexion-extension and rotation, yet its bony articulations are shallow and incongruent, so stability depends on ligaments:
- the transverse ligament (part of the cruciate ligament) holds the odontoid (dens) against the anterior arch of the atlas — the key restraint to anterior atlanto-axial translation;
- the alar ligaments run from the dens to the occipital condyles, restraining rotation and distraction;
- the tectorial membrane (the cephalad continuation of the posterior longitudinal ligament) and the apical and atlanto-occipital membranes/ligaments span the dens/atlas to the occiput.
Disruption of these — by trauma or disease — produces craniocervical instability.
Pathophysiology & causes
Instability arises whenever the ligamentous restraints fail faster than the shallow bony joints can compensate - acutely, by high-energy distraction (trauma), or chronically, by inflammatory/erosive or congenitally lax tissue. The result is pathological motion at occiput-C1 (occipito-atlantal) and/or C1-C2 (atlanto-axial), threatening the cervicomedullary cord.
Atlanto-occipital dissociation is a rare, highly unstable ligamentous injury of the occiput–C1 junction from high-energy hyperextension/distraction — typically motor-vehicle and pedestrian trauma. It carries very high morbidity and mortality (often fatal at the scene from brainstem/upper cord injury), and children and young adults are disproportionately affected because of their relatively horizontal occipital condyles and large head. Survivors may present with cranial-nerve palsies, brainstem/cord signs or, with milder unilateral injuries, neck pain — CCJ ligamentous injury is best thought of as a spectrum, a subset of which can be managed non-operatively.
Clinical Presentation
- High-energy mechanism (MVC, pedestrian); often multi-trauma and reduced consciousness
- May be fatal at the scene (brainstem/upper-cord injury); survivors range from lower cranial-nerve palsies and brainstem/cord signs to neck pain alone
- A subtle deficit or isolated neck pain in a high-energy injury is the warning - have a low threshold
- Examine cranial nerves, long tracts and respiratory function; assess the whole cervical spine
- Insidious neck pain, occipital headache, and progressive myelopathy (gait/hand dysfunction, hyperreflexia)
- In rheumatoid arthritis: long-standing erosive disease; watch for cranial settling/basilar invagination
- In Down syndrome / congenital disease: often asymptomatic, detected on screening; symptoms may emerge with minor trauma
- Pre-anaesthetic concern: instability risks cord injury at intubation/positioning
Investigations
AOD is frequently missed, so look for it actively on the craniocervical CT using objective measurements:
- C1-condyle interval (CCI) — the gap between the occipital condyle and the C1 lateral mass; an increased CCI is the most sensitive sign of AOD (in adults and children).
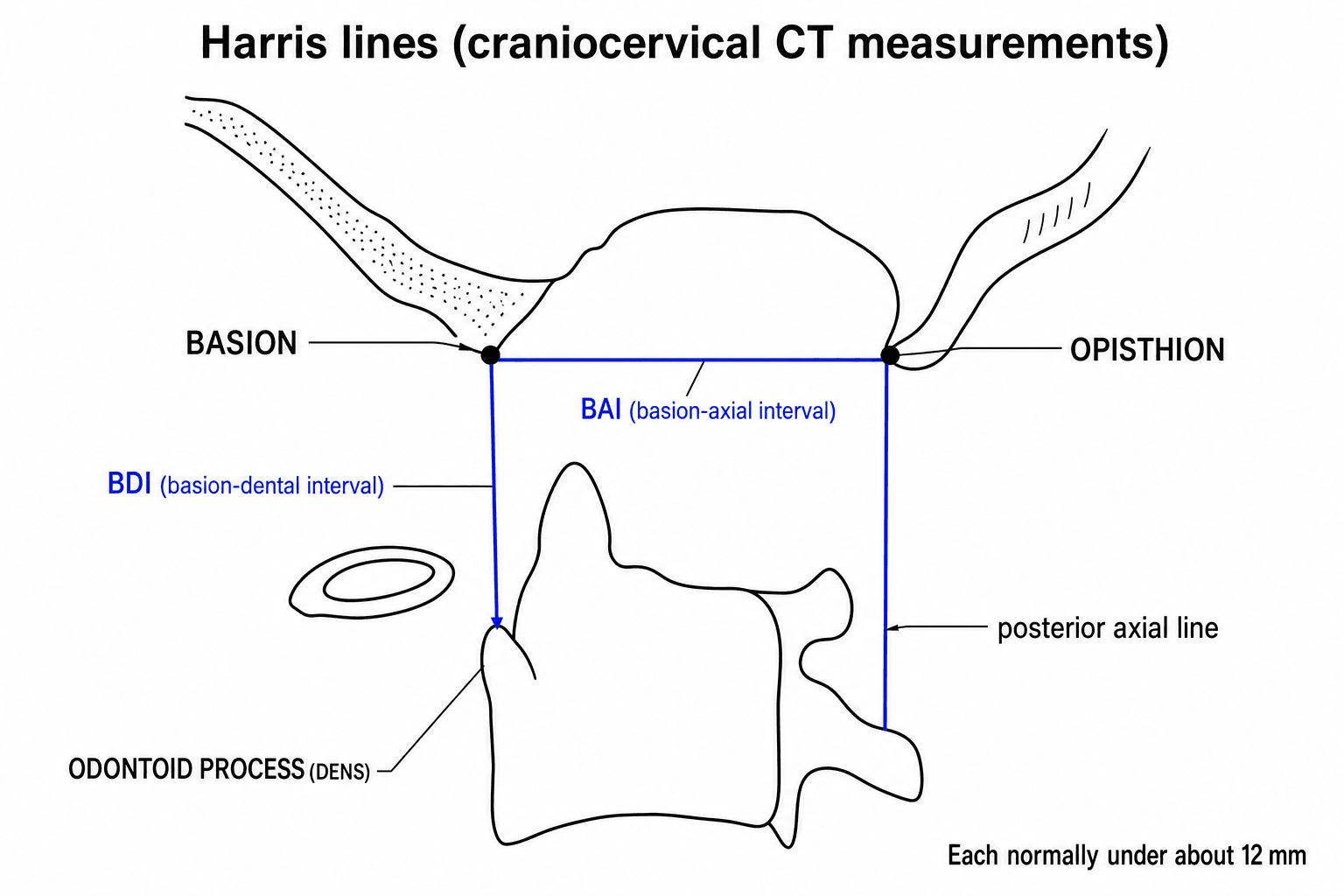
- Harris lines — the basion-dental interval (BDI) (basion to the tip of the dens) and the basion-axial interval (BAI) (basion to the posterior axial line); each should normally be under about 12 mm.
- Powers ratio (basion–posterior arch / opisthion–anterior arch) — over ~1 suggests anterior dislocation (less reliable for distraction/posterior injuries).
MRI assesses the ligaments, cord signal, oedema and epidural haematoma. Always evaluate the whole cervical spine and the neurology.

- What it assesses
- Occipital condyle to C1 lateral mass gap
- Note
- Most sensitive for AOD (adults & children)
- What it assesses
- Basion to tip of dens (Harris)
- Note
- Normally under ~12 mm
- What it assesses
- Basion to posterior axial line (Harris)
- Note
- Normally under ~12 mm
- What it assesses
- Basion–posterior arch / opisthion–anterior arch
- Note
- Over ~1 = anterior AOD (misses distraction/posterior)
Traumatic atlanto-occipital dissociation is classified by the direction of occipital displacement on the atlas:
- Type I - anterior displacement (occiput translated forward on the atlas) - the commonest pattern in many series.
- Type II - longitudinal / vertical distraction (the occiput separated upward from the atlas) - the most unstable, pathognomonic pattern, and the one in which traction is most dangerous.
- Type III - posterior displacement.
The classification aids communication and flags the unstable distraction pattern, but note it did not predict mortality in the pooled data - associated traumatic brain injury was the dominant prognostic factor.
The CCI and Harris lines diagnose the occipito-atlantal (AOD) injury; the atlanto-axial axis and rheumatoid cranial settling have their own measurements:
- Anterior atlanto-dental interval (AADI) - the gap between the anterior arch of the atlas and the dens; abnormal above ~3 mm in adults (above ~5 mm in children), indicating transverse-ligament incompetence / atlanto-axial instability.
- Posterior atlanto-dental interval (PADI) - the space available for the cord behind the dens; a PADI below ~14 mm predicts neurological compromise and is the better operative indicator in rheumatoid disease (Boden) once erosion has occurred.
- Basilar invagination / cranial-settling lines - McRae (foramen magnum), Chamberlain (hard palate-opisthion) and McGregor (hard palate-occiput) lines for the dens tip, plus the Ranawat and Redlund-Johnell criteria for vertical settling.
So measure the AADI/PADI for atlanto-axial instability and the settling lines for the rheumatoid dens, alongside the CCI/Harris for AOD.
Management
In a distraction-type atlanto-occipital dissociation, cervical traction is contraindicated — it can further distract the already-disrupted junction and worsen neurological injury or cause death. Immobilise the head and neck rigidly (collar/sandbags; halo with great caution), avoid traction, and proceed to definitive stabilisation. This is a classic exam safety point.
- 1Suspect and measureIn any high-energy injury (especially a child/young adult) with neck pain or a subtle deficit, scrutinise the CT for an increased C1-condyle interval and Harris BDI/BAI; MRI for the ligaments and cord. AOD is easily missed when the bones look aligned.
- 2Immobilise rigidly — NO tractionRigid collar/sandbags; traction is contraindicated in a distraction injury. Resuscitate and protect the airway/cord.
- 3Fuse the unstable junctionPosterior occipitocervical stabilisation and fusion, commonly occiput–C2, with an occipital plate and C1/C2 screw-rod construct + graft. Tailor levels: C1–C2 fusion (Goel-Harms/Magerl) for isolated atlanto-axial instability; include the occiput for occipito-atlantal disruption.
- 4Individualise the milder spectrumMilder, stable unilateral ligamentous injuries may be treated non-operatively with immobilisation and follow-up. Screen rheumatoid and Down-syndrome patients (e.g. before anaesthesia) for instability/myelopathy.
Acute distraction AOD: rigid external immobilisation (collar/sandbags; halo with great caution) and resuscitation. Traction is contraindicated in a distraction injury. This is a temporising bridge to definitive fixation, not a definitive treatment for an unstable injury.
Unstable craniocervical injury/instability is treated with posterior occipitocervical stabilisation and fusion — commonly occiput to C2 (C0–C2) — using an occipital plate and C1/C2 (± occipital) screw-rod constructs with bone graft. Isolated atlanto-axial instability (transverse-ligament rupture, os odontoideum) may be treated by C1–C2 fusion, whereas occipito-atlantal disruption requires inclusion of the occiput. In rheumatoid disease, decompression and fusion address instability/cranial settling and myelopathy. Milder, stable unilateral ligamentous injuries may be managed non-operatively. Recognising the injury early, before deterioration, is the key to survival and outcome.
Complications
- Complication
- Death / devastating cord-brainstem injury
- Note
- AOD is frequently fatal; survival hinges on early recognition before deterioration
- Complication
- Missed diagnosis
- Note
- AOD is easily missed when the bones look aligned - measure the CCI actively
- Complication
- Traction-induced over-distraction
- Note
- Applying traction to a distraction injury can worsen neurology or kill - contraindicated
- Complication
- Progressive myelopathy, cranial settling/basilar invagination
- Note
- Superior dens migration through the foramen magnum threatens the cervicomedullary cord
- Complication
- Vertebral artery injury, dural tear/CSF leak, hardware failure/nonunion
- Note
- CCJ instrumentation is technically demanding; the vertebral artery is at risk at C1-C2
- Complication
- Loss of CCJ motion
- Note
- Occipitocervical fusion sacrifices ~half of cervical rotation/flexion - counsel the patient
The two ways to kill this patient are missing the injury and applying traction to it. Measure the C1-condyle interval on every high-energy craniocervical CT, immobilise rigidly WITHOUT traction, and escalate to early occipitocervical stabilisation - deterioration can be sudden and fatal.
Mnemonics & Memory Aids
- CCJ stability is ligamentous — transverse (odontoid–atlas), alar (rotation/distraction), tectorial membrane; the bone alone is insufficient.
- AOD is highly lethal and easily missed — children predisposed; diagnose on CT (C1-condyle interval most sensitive; Harris BDI/BAI under ~12 mm; Powers ratio).
- NEVER apply traction to a distraction injury — rigid immobilisation instead.
- Atraumatic at-risk groups: rheumatoid arthritis (pannus, cranial settling), Down syndrome (laxity/os odontoideum), congenital os odontoideum/dysplasias — screen them.
- Unstable → posterior occipitocervical fusion (C0–C2); C1–C2 for isolated atlanto-axial instability.
- Milder stable unilateral injuries can be non-operative — CCJ injury is a spectrum.
CCJThe junction
Hook:CCJ: check the ligaments, CT-measure it, and (just) no traction - fuse occiput to C2.
DROPDrop the traction
Hook:DROP the traction in AOD: distraction, rheumatoid/Down at risk, occipitocervical fusion, Powers/CCI/Harris.
CRODAt-risk atraumatic groups
Hook:CROD: Congenital, Rheumatoid, Os odontoideum, Down - the atraumatic CCJ-instability groups to screen.
Viva practice
Viva practice
Practise clinical reasoning and management decisions out loud
“A young patient after a high-speed motor-vehicle collision has neck pain and a subtle neurological deficit. Why must you consider atlanto-occipital dissociation, what stabilises the craniocervical junction, and how would you diagnose it?”
“How would you manage a confirmed unstable atlanto-occipital dissociation, what must you avoid, and in which non-traumatic patients do you worry about craniocervical instability?”
Exam cheat sheet
Anatomy
- CCJ stability is LIGAMENTOUS (shallow bony joints)
- Transverse ligament (odontoid-atlas), alar (rotation/distraction), tectorial membrane
- Occiput-C1-C2 provide ~half of cervical flexion/rotation
Causes
- Traumatic: atlanto-occipital dissociation (high-energy, highly lethal, children predisposed)
- Rheumatoid arthritis: atlanto-axial instability + cranial settling/basilar invagination
- Down syndrome (laxity/os odontoideum), congenital os odontoideum, dysplasias
Diagnosis
- CT: C1-condyle interval (most sensitive), Harris BDI/BAI (under ~12 mm), Powers ratio
- MRI for ligaments/cord/oedema
- AOD frequently missed - look for it actively
Management
- Distraction AOD: NO traction - rigid immobilisation
- Unstable: posterior occipitocervical fusion (C0-C2); C1-C2 for isolated atlanto-axial
- Milder stable unilateral injuries: non-operative with follow-up; screen RA/Down before anaesthesia
Evidence Base
Atlanto-occipital dissociation
- Series of 7 AOD patients (mean age 19.6 years, all from car accidents): AOD is rare, highly unstable, with very high morbidity and mortality (4 died early during CPR; 2 more within 3 days).
- The diagnostic method of choice is CT assessment of the C1-condyle interval (CCI) together with cervical MRI.
- Standard treatment of stable patients with an unstable AOD injury is posterior occipitocervical stabilisation and fusion (C0-C2).
Computed tomography parameters for atlantooccipital dislocation in adult patients: the occipital condyle-C1 interval
- 81 adults (22 with AOD): mean occipital condyle-C1 interval (CCI) was 0.89 mm without AOD vs 3.35 mm with AOD.
- A CCI cutoff of 1.5 mm (and condylar sum 3.0 mm) gave a sensitivity of 1.0 for AOD with excellent interrater reliability.
- The older criteria were far less sensitive: Powers 0.55, Wholey 0.46, Harris 0.27, Sun 0.23, Wackenheim 0.41, Lee 0.41.
Unilateral atlanto-occipital injury: A case series and detailed radiographic description
- 8 patients with unilateral atlanto-occipital injury: all had a widened condyle-C1 interval (over 2 mm).
- Three patients were managed without surgery; there were no delayed neurologic injuries or deaths.
- The authors propose craniocervical ligamentous injury functions as a spectrum rather than a dichotomous diagnosis, a subset of which can be safely managed non-operatively.
Prognostic factors in traumatic atlanto-occipital dislocation
- Literature review of 141 traumatic AOD patients from 60 studies, analysed for predictors of mortality.
- Associated traumatic brain injury was the dominant predictor of death (OR 8.05) - patients with TBI were ~8x more likely to die.
- Spinal cord injury, age, sex, polytrauma and the Traynelis AOD classification did not reach statistical significance for mortality.
The lethality and CCI-plus-MRI diagnostic pathway come from Vachata et al. 2020 (DOI); the quantified CCI cutoff (1.5 mm, sensitivity 1.0) and the relative insensitivity of Harris/Powers from Martinez-Del-Campo et al. 2015 (DOI); the spectrum concept from Lepard et al. 2022 (DOI); and the TBI-as-prognosticator data from Fard et al. 2016 (DOI). The stabilising-ligament anatomy, the Harris lines and Powers ratio, and the no-traction caution are standard, well-established craniocervical teaching. (See also our Jefferson Fracture and Rheumatoid Cervical Spine material.)