Unfused Acromial Ossification Centre | Often an Incidental Finding | Seen on Axillary View | Conservative First
- Os acromiale = failure of fusion of an acromial ossification centre - fusion should be complete by age 22-25, so a persistent gap after 25 defines the condition
- Classified by the unfused centre: pre-acromion, meso-acromion (most common symptomatic), meta-acromion, basi-acromion - based on the four ossification centres (Park MR types A/B/C describe where the gap sits)
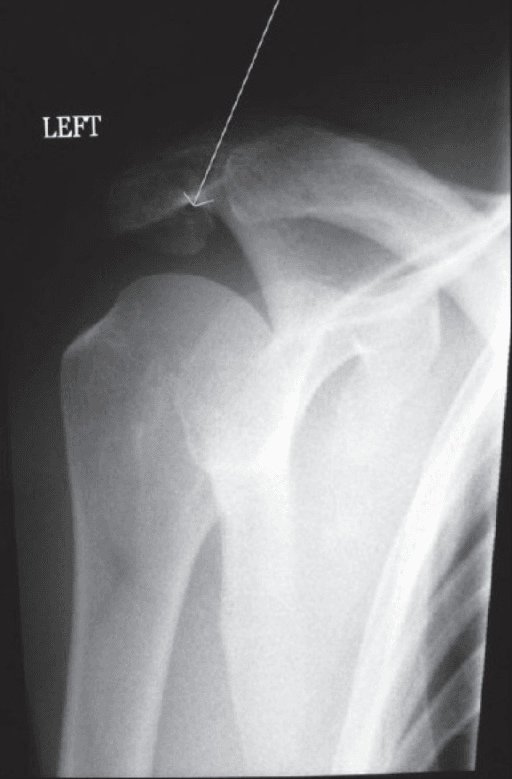
- Easily MISSED on the AP view - the gap is best seen on the axillary (axial) view; do not mistake it for a fracture
- Often asymptomatic and incidental - only treat the patient, not the X-ray; symptoms arise from an unstable mobile fragment, impingement, or an associated rotator cuff tear
- Conservative treatment first (activity modification, NSAIDs, physiotherapy, subacromial injection); surgery (fixation vs excision) only for refractory symptomatic cases
- “The single highest-yield fact: an os acromiale is best demonstrated on the AXILLARY view and is frequently missed on a standard AP shoulder series
- “Distinguish from an acromial fracture - an os acromiale has smooth, corticated, often sclerotic margins; a fracture has sharp irregular edges and a history of trauma
- “It is bilateral in roughly a third of cases - if you see one, image the other shoulder before calling it a fracture
- “Excising a LARGE fragment risks detaching the anterior deltoid origin and weakening flexion - large mobile fragments are fixed, small ones are excised
The classic trap. An os acromiale has smooth, rounded, corticated and often sclerotic margins, is frequently bilateral, and is usually painless. A fracture has sharp, irregular, non-corticated edges with a clear traumatic history. Mislabelling an os acromiale as a fracture leads to unnecessary intervention.
An os acromiale is commonly missed on the AP view and is best seen on the axillary (axial) projection. Always request an axillary view (or scapular Y / axial CT or MRI) when assessing shoulder pain - it is the single most reliable plain-film way to identify the fusion defect.
The majority of os acromiale are incidental and asymptomatic. Symptoms arise only from a mobile unstable fragment, secondary impingement, or an associated rotator cuff tear. Confirm the os is the genuine pain source (point tenderness, injection test) before operating.
A large mobile meso-acromion is reduced and fixed (preserving anterior deltoid origin) because excising it would detach deltoid and weaken flexion. A small fragment can be excised (or resected arthroscopically) with good results. Match the operation to fragment size.
Overview and Epidemiology
Os acromiale ("bone of the acromion") is a developmental anomaly in which one of the secondary ossification centres of the acromion fails to fuse with the rest of the acromion, leaving a persistent gap bridged by fibrocartilaginous (rather than bony) tissue. It is not a fracture and it is not, in itself, a disease - it becomes clinically relevant only when it produces symptoms.
Why it matters
- It is a recognised but under-appreciated cause of shoulder pain and secondary impingement, and a recognised cause of failed shoulder surgery when missed.
- It is easily mistaken for a fracture, which can lead to inappropriate treatment.
- It must be identified before subacromial surgery, because operating through or around an unstable os without addressing it can lead to persistent symptoms.
Epidemiology - what the studies show
According to PubMed, the reported prevalence varies widely with population and imaging method:
- The prevalence is generally quoted as 1% to 15%, and is described as particularly common in people of African descent (You et al., 2019, comprehensive review) DOI.
- In a prospective series of patients presenting with shoulder pain, os acromiale was found in 6.8%, was seen on the axillary view in every case, and most of those patients had been labelled with impingement or a cuff tear instead (Burbank et al., 2007) [DOI not indexed; PMID 17461398].
- A large Korean shoulder-clinic radiographic series found a much lower prevalence of 0.7%, illustrating real ethnic and methodological variation, and found no statistically significant association with rotator cuff tears in that population (Kumar et al., 2013) DOI.
- A review of more than 1,000 shoulder MRIs reported a frequency of 3.4%, with no significant sex difference and a tendency to right-sided dominance (Rovesta et al., 2017) DOI.
The headline for exams: prevalence is roughly 1-15%, the meso-acromion is the most common symptomatic type, and the condition is bilateral in around a third of cases.
Pathophysiology and Anatomy
Normal acromial development
The acromion forms from four secondary ossification centres that appear in adolescence (around 14-16 years) and normally fuse with one another and with the scapular spine. From anterior to posterior these are the pre-acromion, meso-acromion, meta-acromion and basi-acromion. Fusion is usually complete by age 22-25 years.
Key definition: A persistent unfused acromial centre after the age of about 25 years is termed an os acromiale. Before that age the gap may simply represent normal, incomplete physiological fusion (You et al., 2019) DOI.
Classification by site
The os is named by which centre has failed to fuse (more precisely, where the unfused gap lies):
- Pre-acromion - failure at the most anterior centre.
- Meso-acromion - the mid-segment is separate; this is the most common symptomatic form because it lies under the deforming pull of the deltoid.
- Meta-acromion - the posterior segment is separate.
- Basi-acromion - rare, at the base near the scapular spine.
Park and colleagues described MR imaging types A, B and C based on which junction had failed: type A (between meso- and meta-acromion) was by far the most common in their series of patients with rotator cuff disease, with type B (pre-/meso-) and type C (meta-/basi-) being uncommon (Park et al., 1994) DOI.
How it causes symptoms
There are three main mechanisms, and they often coexist:
- Instability / micromotion of the fragment - the unfused meso-acromion is mobile. The deltoid pulls the fragment downward during contraction, narrowing the subacromial space and irritating the rotator cuff. Motion at the synchondrosis itself can also be painful.
- Secondary subacromial impingement - the downward-tilting fragment and any reactive osteophytes at the gap margins reduce the space available for the supraspinatus, producing classic impingement symptoms.
- Associated rotator cuff pathology - os acromiale is associated with supraspinatus tendinopathy and tears. In MR series of patients with cuff disease, nearly all os acromiale shoulders had a supraspinatus lesion (tendinitis or tear), and osteophytic lipping was common at the gap margins (Park et al., 1994) DOI.
Classification

- Unfused Centre / Gap Location
- Most anterior tip is separate
- Clinical Note
- Often small; least common symptomatic
- Typical Surgical Strategy
- Excise if symptomatic (small fragment)
- Unfused Centre / Gap Location
- Mid-segment separate (gap between meso- and meta-acromion)
- Clinical Note
- MOST common symptomatic type; mobile under deltoid pull
- Typical Surgical Strategy
- Fix if large + mobile; excise/resect if small
- Unfused Centre / Gap Location
- Posterior segment separate
- Clinical Note
- Less commonly symptomatic in isolation
- Typical Surgical Strategy
- Address associated cuff / impingement pathology
- Unfused Centre / Gap Location
- Base near scapular spine separate
- Clinical Note
- Rare
- Typical Surgical Strategy
- Individualised - usually treat associated pathology
The meso-acromion is the type that comes up in exams: it is the most common symptomatic os acromiale, it is the one that is mobile because the anterior deltoid pulls it down, and it is the one you fix (rather than excise) when the fragment is large. Park's MR type A corresponds to this meso-/meta-acromion gap.
Clinical Presentation
History
- Often an incidental, asymptomatic finding on imaging done for another reason.
- When symptomatic: anterior-superior shoulder pain, frequently indistinguishable from ordinary subacromial impingement, with pain on overhead activity and sometimes night pain.
- A history of failed impingement treatment or persistent symptoms after subacromial surgery should raise suspicion of a missed os.
Examination
- Point tenderness directly over the acromial gap is the most useful specific sign - palpate the acromion carefully.
- Standard impingement signs may be positive (Neer, Hawkins-Kennedy) because of secondary impingement, which is exactly why it is mislabelled as routine impingement.
- Assess rotator cuff strength - weakness suggests an associated cuff tear.
- Examine the contralateral shoulder, given frequent bilaterality.
In the prospective shoulder-pain series, no patient was correctly given a primary diagnosis of os acromiale on history and examination alone - the diagnosis was made only when the radiographs (specifically the axillary view) were deliberately reviewed for it, and most of those patients had instead been labelled with impingement or a cuff tear (Burbank et al., 2007, PMID 17461398). The lesson: actively look for it on the axillary view, and do not anchor on an "impingement" label.
Investigations
Imaging Pathway for a Suspected Os Acromiale
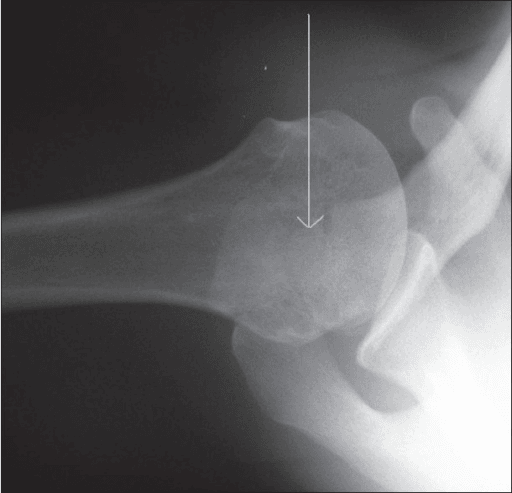
Request a full series: AP, scapular Y and axillary (axial) views. The os acromiale is frequently invisible on the AP view and is best seen on the axillary view, where the unfused fragment is demonstrated anterior to the rest of the acromion. Look for smooth, corticated, sclerotic margins to distinguish from a fracture, and image the other shoulder if there is doubt.
MRI shows the transversely oriented fusion defect with characteristic irregular margins, and crucially demonstrates bone-marrow oedema and interface oedema around a symptomatic, mobile os - features that help separate a genuinely painful os from a quiet incidental one. MRI also evaluates the rotator cuff and bursa.
CT best defines the bony anatomy, fragment size and any sclerosis or osteophytes at the gap - useful for surgical planning (fixation vs excision). In difficult or adolescent cases, SPECT-CT can demonstrate increased activity at a symptomatic synchondrosis, supporting it as the pain source.
Diagnosing os acromiale in adolescents
Because normal fusion may not complete until 22-25 years, calling an unfused centre an os acromiale in a teenager is contentious. According to PubMed, MRI can still distinguish the two: a true os acromiale shows a transverse interface orientation with irregular margins, whereas a normally developing centre shows an arched interface with lobulated margins. Using these features, adult cases were diagnosed with 100% accuracy and most adolescents were correctly identified as normal development, although a minority of adolescents did have genuine os acromiale - so diagnosis should be based on imaging features, not age alone (Winfeld et al., 2015) DOI.
Management
For symptomatic os acromiale, non-operative treatment is started first, exactly as for impingement (You et al., 2019) DOI:
Conservative Protocol
Reduce provocative overhead and loading activities. Reassure the patient if the os is incidental.
NSAIDs for pain and any reactive inflammation.
Rotator cuff and scapular stabiliser strengthening to optimise dynamic control and reduce secondary impingement.
A subacromial (or peri-os) corticosteroid/local-anaesthetic injection is both therapeutic and diagnostic - relief of pain localises the os/subacromial space as the pain source and predicts response.
A large proportion of patients settle with conservative care; surgery is reserved for those who fail an adequate trial (typically several months).
- Favours FIXATION
- Large meso-acromion
- Favours EXCISION / Resection
- Small fragment (e.g. pre-acromion)
- Favours FIXATION
- Must be preserved - large fragment carries deltoid
- Favours EXCISION / Resection
- Minimal deltoid attached - safe to remove
- Favours FIXATION
- Younger, good bone for union
- Favours EXCISION / Resection
- Older patient, poor union potential
- Favours FIXATION
- Primary procedure
- Favours EXCISION / Resection
- Salvage after failed fixation / nonunion
- Favours FIXATION
- Hardware irritation (~30% need removal)
- Favours EXCISION / Resection
- Risk of deltoid weakness if fragment too large
The Deltoid Origin: Why Fragment Size Dictates Fix vs Excise
The whole surgical strategy hinges on "preserving the anterior deltoid origin" — worth developing, because the deltoid origin is exactly what a large os carries.
- The deltoid arises from the acromion. The anterior deltoid originates from the anterior acromial border and the lateral third of the clavicle, the middle (acromial) deltoid from the lateral margin and superior surface of the acromion, and the posterior deltoid from the scapular spine. A meso-acromion therefore carries a substantial portion of the anterior and middle deltoid origin.
- Why you fix a large fragment. Excising a large meso-acromion detaches that deltoid origin, weakening forward flexion and abduction and leaving a poor functional result — so a large mobile fragment is reduced and fixed (preserving the origin) rather than removed. Only a small fragment carrying little deltoid can be safely excised.
- The os as a deliberate surgical window. Because the meso-acromion sits over the supraspinatus, a mobile os can be used as an acromion-splitting approach to expose and repair a massive rotator cuff tear, after which the acromion is re-fixed (analogous to a controlled acromial osteotomy).
- Contrast with acromioplasty. Removing bone from the acromial undersurface for impingement is safe because it does not detach the deltoid; excising the whole os is not — this is the anatomical reason the two operations differ.
Q: Why is a large meso-acromion fixed rather than excised, but a subacromial acromioplasty is harmless to the deltoid? A: The meso-acromion carries the anterior and middle deltoid origin, so excising it detaches the deltoid and weakens flexion/abduction — hence large mobile fragments are reduced and fixed. Acromioplasty only removes undersurface bone and leaves the deltoid origin intact. Only a small fragment carrying negligible deltoid is safe to excise.
Complications
Internal fixation of the os can fail to unite; historically nonunion rates were a concern, though modern tension-band and suture techniques report union rates of 96-100% in selected series (Peckett 2004; Guo 2019). Bone grafting improves union.
The subcutaneous acromion makes prominent K-wires/screws symptomatic - around a third of fixation patients need hardware removal. This drove the development of suture-based fixation techniques.
Excising a large fragment detaches the anterior deltoid origin, risking weakness of forward flexion and a poor functional result - the reason large mobile fragments are fixed rather than excised.
An unrecognised os acromiale is a cause of persistent symptoms after subacromial decompression - failing to obtain an axillary view or to address a mobile os leaves the pain generator untreated.
Clinical Relevance and Associations
- Association with rotator cuff disease: os acromiale is reported in association with subacromial impingement and supraspinatus tears, and reactive osteophytes at the gap margins narrow the subacromial space (Park et al., 1994) DOI. However, the strength of the cuff-tear association is population-dependent - a large Korean series found no statistically significant association between os acromiale and cuff tears (Kumar et al., 2013) DOI. For exams: state that there is a recognised association with impingement and cuff pathology, but that it is not invariable.
- Reverse total shoulder arthroplasty: an unstable os acromiale can become symptomatic or fracture after reverse shoulder arthroplasty because of altered deltoid tensioning - a point flagged in contemporary reviews (You et al., 2019) DOI.
- Pre-operative planning: because the os alters acromial bony anatomy and the deltoid origin, recognising it before any subacromial or arthroplasty surgery is essential to avoid intra-operative surprises and to plan whether to fix, excise or work around it.
Os Acromiale After Reverse Total Shoulder Arthroplasty
The clinical-relevance section and a viva follow-up both raise why an os becomes symptomatic after a reverse total shoulder arthroplasty (RTSA) — here is the mechanism and classification.
- Why RTSA loads the acromion. A reverse prosthesis medialises and distalises the centre of rotation and lengthens and tensions the deltoid. The now-tightened deltoid pulls harder on its acromial origin, greatly increasing the bending stress across the acromion — and across any weak, fibrocartilage-bridged os acromiale.
- The result — an acromial or scapular-spine stress fracture. This is a recognised cause of new pain and loss of active forward elevation with anterior/lateral tilt after an initially successful RTSA; an unstable os acts as a stress riser that predisposes to it.
- Levy classification of post-RTSA acromial/scapular-spine fractures:
- Type I — anterior acromion (only part of the middle deltoid origin involved).
- Type II — posterior acromion / more of the acromion (the entire middle deltoid origin).
- Type III — the scapular spine.
- Management is usually non-operative (immobilisation/bracing), because fixation in thin osteopenic acromial bone is difficult and frequently fails; the fracture nonetheless often leaves a worse functional result — which is the practical reason to recognise an os acromiale before performing an RTSA.
Q: A patient develops new pain and loss of active elevation months after a reverse shoulder replacement, with a known os acromiale — what has happened? A: An acromial (or scapular-spine) stress fracture through/around the os. RTSA lengthens and tensions the deltoid, raising bending stress across the acromion; the fibrocartilage-bridged os is a stress riser. Classify by Levy (I anterior acromion, II posterior/most of acromion, III scapular spine); most are managed non-operatively as fixation of thin bone often fails — recognise the os before RTSA.
Guidelines, Registries and Global Practice
There is no single dedicated international guideline for os acromiale; management is guided by the shoulder-impingement and rotator-cuff literature plus the os-specific case series above. The globally consistent principles are:
- Diagnosis depends on the axillary view (or axial CT/MRI). This is emphasised across US, European and Asian series alike, reflecting how often the condition is missed on the AP film (Burbank et al., 2007, PMID 17461398; Rovesta et al., 2017) DOI.
- Prevalence varies markedly by population - quoted at 1-15% generally and higher in people of African descent, but as low as 0.7% in a Korean radiographic series, underlining genuine ethnic and methodological variation rather than one universal figure (Kumar et al., 2013 DOI; You et al., 2019 DOI).
- Conservative treatment first, then size-matched surgery is the universally recommended pathway: fixation for large mobile fragments and excision/arthroscopic resection for small ones, with a global trend toward arthroscopic techniques to reduce morbidity and treat concomitant cuff/impingement pathology (You et al., 2019) DOI.
- Registry data are not specific to os acromiale; the relevant arthroplasty registries (NJR, AJRR, AOANJRR) capture reverse shoulder arthroplasty outcomes, within which an unstable os acromiale is recognised as a potential source of post-arthroplasty acromial complications.
According to PubMed, all evidence cited on this page is drawn from the referenced articles; please see the linked DOIs for the primary sources.
Memory Aids
PMMBThe Four Acromial Ossification Centres
Hook:Front to back: Pre, Meso, Meta, Basi - the gap is named by which centre failed to fuse, and MESO is the troublemaker.
SBCOs Acromiale Versus Fracture - Telling Them Apart
Hook:SBC = Smooth, Bilateral, Corticated - the three features that say os acromiale, not fracture.
TIPWhen to Suspect a Symptomatic Os Acromiale
Hook:Look for the TIP of the iceberg - point Tenderness, Impingement, Positive injection.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old presents to the emergency department after a fall onto the shoulder. The AP radiograph is reported as normal, but the axillary view shows a separate bony fragment at the anterior acromion with smooth, sclerotic margins. The patient has diffuse shoulder pain but no specific tenderness over the fragment. How do you interpret this and what do you do?”
“A 40-year-old labourer has 9 months of anterior shoulder pain with point tenderness over the acromion and positive impingement signs. Radiographs and CT confirm a large, mobile meso-acromion. He has failed physiotherapy and two subacromial injections that each gave temporary relief. MRI shows an intact rotator cuff. He wants to return to manual work. How do you manage him?”
Definition and Anatomy
- Os acromiale = failure of fusion of an acromial ossification centre (fibrocartilage bridges the gap)
- Four centres front to back: pre-acromion, meso-acromion, meta-acromion, basi-acromion
- Normal fusion complete by age 22-25 - a persistent gap after ~25 defines the condition
- Bilateral in about one third of cases
Classification
- Named by the unfused centre: pre-, meso-, meta-, basi-acromion
- MESO-acromion = most common SYMPTOMATIC type (mobile under deltoid pull)
- Park MRI types: A (meso-/meta) most common, B (pre-/meso), C (meta-/basi)
- Prevalence ~1-15% (population dependent; higher in African descent)
Diagnosis
- MISSED on the AP view - best seen on the AXILLARY (axial) view
- Os vs fracture: os has SMOOTH, sclerotic, corticated margins, no trauma, often bilateral
- MRI: transverse interface, irregular margins, marrow/interface oedema if symptomatic
- CT for fragment size/sclerosis (surgical planning); image the other shoulder
Management
- Most are incidental and asymptomatic - treat the patient, not the X-ray
- Conservative first: activity modification, NSAIDs, physiotherapy, subacromial injection (diagnostic + therapeutic)
- Surgery only after a failed adequate conservative trial and confirmation the os is the pain source
- FIX large mobile fragments (tension band/screws + graft; ~96% union); EXCISE/resect small ones
Pitfalls and Complications
- Excising a LARGE fragment detaches anterior deltoid - weakness of flexion (so fix it instead)
- Hardware irritation after fixation - ~one third need removal (suture fixation avoids this)
- Missed os = cause of failed subacromial decompression (always get an axillary view)
- Can become symptomatic / fracture after reverse total shoulder arthroplasty
Evidence Base
Os Acromiale on MRI in Rotator Cuff Disease - the Classic Type Description
- Retrospective MRI analysis of 10 patients over 25 years with os acromiale, subdivided into three types based on the site of the unfused junction
- Type A (meso-/meta-acromion gap) in 8 of 10; type B (pre-/meso-) in 1; type C (meta-/basi-) in 1
- Osteophytic lipping at the margins of the acromial gap in 9 of 10 cases
- Every patient had a supraspinatus lesion - tendinitis in 4 and a tendon tear in 6
- The os was identifiable on oblique sagittal and/or oblique coronal MR images
Incidence of Os Acromiale in Patients With Shoulder Pain - Why You Need the Axillary View
- Prospective series of 93 shoulders in 88 consecutive patients with shoulder pain, all imaged with AP, scapular Y and axillary views
- Os acromiale present in 6 of 88 patients (6.8%) and seen on the axillary view in EVERY case
- No patient was given a primary diagnosis of os acromiale on history and examination alone
- Five of the six had instead been labelled with impingement or a rotator cuff tear
Internal Fixation of Symptomatic Os Acromiale - 26-Case Series
- 26 patients with symptomatic meso-os acromiale, all having failed non-operative treatment, treated by internal fixation and bone grafting (K-wires or screws plus tension band)
- Union rate 96% (25/26) with mean time to union of about 4 months
- 92% (24/26) were satisfied with their result
- 8 patients (31%) had postoperative pain relieved by hardware removal; 2 postoperative fractures occurred
- 15 patients had associated cuff tears; 11 were repaired and 6 were irreparable
Suture Fixation of Os Acromiale - Avoiding Hardware Problems
- Retrospective series of 10 meso-acromion shoulders fixed with polyester sutures (arthroscopically in 9)
- Constant score improved from ~40.5 to ~75.6 and VAS fell from ~5.2 to ~1.6
- All patients showed bony union on CT at 12 months with good fragment position and no edge sclerosis
- No hardware irritation was reported