Mechanosensing Cells | Lacunocanalicular Network | Wolff's Law | Sclerostin Regulation
Mechanotransduction Pathways
Critical Must-Knows
- Osteocytes are terminally differentiated osteoblasts embedded in bone matrix
- Lacunocanalicular network allows fluid flow and cell communication
- Mechanical loading induces fluid shear stress on osteocyte dendrites
- Sclerostin inhibition is the key anabolic response to loading
- Osteocyte apoptosis signals targeted remodeling via RANKL upregulation
Clinical Pearls
- "Wolff's Law is mediated by osteocyte mechanosensing
- "Disuse osteoporosis occurs via increased sclerostin production
- "Primary cilium acts as flow sensor - bending activates calcium channels
- "Gap junctions propagate signals through lacunocanalicular network
Critical Osteocyte Mechanotransduction Exam Points
Cellular Architecture
Osteocytes represent 90-95% of bone cells despite small volume fraction. Each osteocyte has 40-100 dendritic processes extending through canaliculi, creating a mechanosensory network.
Fluid Flow Mechanism
Mechanical loading induces interstitial fluid flow through lacunocanalicular system. Shear stress on dendrites (50-100 nanometers displacement) activates mechanoreceptors.
Sclerostin Regulation
Loading downregulates sclerostin (SOST gene). Reduced sclerostin disinhibits Wnt signaling in osteoblasts, promoting bone formation. Disuse increases sclerostin.
Apoptosis Signaling
Osteocyte death from microdamage or immobilization upregulates RANKL, recruiting osteoclasts for targeted remodeling. Occurs within 72 hours of apoptosis.
At a Glance
Osteocytes comprise 90-95% of all bone cells and function as the primary mechanosensors of the skeleton, embodying Wolff's Law at the cellular level. These terminally differentiated osteoblasts are embedded in bone matrix and connected via the lacunocanalicular network, where mechanical loading induces interstitial fluid flow that generates 50-100nm shear stress on dendritic processes to activate mechanotransduction pathways. The key anabolic response involves downregulation of sclerostin (SOST gene), which disinhibits Wnt signaling in osteoblasts to promote bone formation—conversely, disuse increases sclerostin and causes bone loss. Osteocyte apoptosis from microdamage or immobilization triggers targeted remodeling via RANKL upregulation within 72 hours, recruiting osteoclasts to sites requiring repair.
CHIEFMechanotransduction Pathway Components
| C | Cilium (primary) Flow sensor - bends with fluid movement |
| H | Hemichannels Release ATP and PGE2 - paracrine signaling |
| I | Integrins Matrix attachment - sense strain directly |
| E | E-eleven (connexin 43) Gap junctions - propagate calcium waves |
| F | Focal adhesions Mechanosensitive complexes activate MAPK |
| C | Cilium (primary) Flow sensor - bends with fluid movement | E | E-eleven (connexin 43) Gap junctions - propagate calcium waves |
| H | Hemichannels Release ATP and PGE2 - paracrine signaling | F | Focal adhesions Mechanosensitive complexes activate MAPK |
| I | Integrins Matrix attachment - sense strain directly |
Hook:The CHIEF sensors detect mechanical loading in the osteocyte network!
SCRAPOsteocyte Response to Loading
| S | Sclerostin decreased Loading suppresses SOST gene expression |
| C | Calcium signaling Intracellular calcium waves propagate |
| R | RANKL/OPG ratio falls Reduces osteoclast recruitment |
| A | ATP release Purinergic signaling to osteoblasts |
| P | Prostaglandin E2 PGE2 promotes bone formation |
| S | Sclerostin decreased Loading suppresses SOST gene expression | A | ATP release Purinergic signaling to osteoblasts |
| C | Calcium signaling Intracellular calcium waves propagate | P | Prostaglandin E2 PGE2 promotes bone formation |
| R | RANKL/OPG ratio falls Reduces osteoclast recruitment |
Hook:Loading causes osteocytes to SCRAP the bone resorption program and switch to formation!
Overview and Introduction
Osteocytes are the most abundant cells in bone, arising from osteoblasts that become entombed in the matrix during bone formation. These terminally differentiated cells orchestrate bone remodeling in response to mechanical stimuli through a process called mechanotransduction.
The transformation from osteoblast to osteocyte involves dramatic morphological changes including development of extensive dendritic processes, loss of secretory organelles, and establishment of gap junction connections with neighboring osteocytes and surface bone cells.
Why Mechanotransduction Matters Clinically
Understanding osteocyte mechanotransduction explains clinical phenomena including stress fractures (inadequate adaptation), disuse osteoporosis (reduced loading stimulus), and heterotopic ossification (ectopic mechanical signals). It also guides rehabilitation protocols emphasizing early weight-bearing.
Osteocyte Lifespan
- Lifespan: Decades (possibly entire lifespan)
- Embedded in mineralized matrix
- Maintain viability via lacunocanalicular network
- Cell body in lacuna (10-20 micrometers)
Network Architecture
- 40-100 dendritic processes per cell
- Extend through canaliculi (250-300 nm diameter)
- Connect to 10-12 neighboring osteocytes
- Gap junctions enable electrical/chemical coupling
Concepts and Molecular Mechanisms
Core Mechanotransduction Concepts
Central Paradigm: Wolff's Law at the Cellular Level
Wolff's Law states that bone adapts its structure to mechanical demands. Osteocytes are the cellular mediators of this principle, converting mechanical loading into biochemical signals that regulate bone formation and resorption.
Key Molecular Mechanisms:
- Fluid shear stress activates primary cilia and integrins
- Calcium waves propagate through gap junctions (connexin 43)
- Loading suppresses sclerostin (SOST gene), disinhibiting Wnt pathway
- ATP and PGE2 released via hemichannels signal to osteoblasts
Clinical Applications:
- Early weight-bearing promotes fracture healing via mechanotransduction
- Disuse osteoporosis results from increased sclerostin
- Romosozumab (anti-sclerostin antibody) mimics loading effects
Lacunocanalicular Network
Structural Organization
The lacunocanalicular network is the anatomical substrate for mechanotransduction. Each osteocyte cell body resides in a lacuna, with dendritic processes extending through canaliculi to contact neighboring cells and surface lining cells.
| Component | Dimensions | Function | Key Feature |
|---|---|---|---|
| Lacuna | 10-20 micrometers | Houses osteocyte cell body | Separated from matrix by pericellular space |
| Canaliculus | 250-300 nm diameter | Channels for dendrites | Permits fluid flow around processes |
| Dendritic Process | 100-500 nm thick | Mechanosensory antenna | 40-100 per osteocyte |
| Pericellular Space | 50-100 nm | Fluid-filled gap | Site of fluid shear stress |
Fluid Flow Dynamics
Mechanical loading of bone creates pressure gradients that drive interstitial fluid flow through the lacunocanalicular system. The narrow pericellular space amplifies shear stress on osteocyte dendrites by 10-100 fold compared to loading magnitude.
Mechanical Loading to Fluid Flow
External mechanical load causes bone matrix strain (typically 1000-3000 microstrain). Matrix deformation compresses lacunae and canaliculi, creating pressure gradients.
Differential pressures between compressed and tensioned regions drive fluid movement through lacunocanalicular network. Flow follows pressure gradients.
Fluid flowing past osteocyte dendrites in narrow pericellular space creates shear stress (1-3 Pascal). Primary cilium and membrane receptors detect flow.
Mechanical stimulus amplified 10-100 fold at cellular level. Small matrix strains produce significant cellular deformation and receptor activation.
Mechanotransduction Mechanisms
Mechanosensors
Osteocytes employ multiple mechanosensory systems to detect and respond to mechanical stimuli. These include flow sensors, strain sensors, and chemical sensors.
Primary Cilium Flow Sensor
The primary cilium is a solitary, non-motile microtubule-based organelle projecting from the osteocyte membrane into the pericellular space. It acts as a flow sensor, bending in response to fluid movement.
Mechanism:
- Cilium bends with fluid flow (50-100 nm displacement)
- Bending activates mechanosensitive ion channels
- Calcium influx initiates intracellular signaling
- Cilium deflection correlates with loading magnitude
Clinical Relevance: Defects in primary cilia (ciliopathies) cause skeletal dysplasias due to impaired mechanosensing. Loading exercises require sufficient magnitude to bend cilia.
Primary Cilium Pearl
Q: What is the minimum fluid flow required to activate osteocyte mechanotransduction? A: 50-100 nanometers of cilium deflection, corresponding to approximately 1000-3000 microstrain at tissue level or 1-3 Pascal shear stress at cellular level.
Molecular Responses to Loading
Sclerostin Regulation
Sclerostin, encoded by the SOST gene, is a Wnt signaling antagonist secreted by osteocytes. Mechanical loading rapidly suppresses sclerostin production, disinhibiting Wnt signaling in osteoblasts.
Sclerostin Response Timeline
Mechanical loading triggers intracellular signaling cascades in osteocytes. Calcium influx and MAPK activation occur within minutes of loading onset.
SOST gene transcription decreases. Sclerostin protein production falls. Existing sclerostin continues to inhibit Wnt signaling during this transition period.
Sclerostin protein levels decrease in lacunocanalicular network. Wnt signaling in osteoblasts begins to increase. Early anabolic gene expression starts.
With continued loading, sclerostin remains suppressed. Osteoblast proliferation and matrix synthesis increase. Bone formation response becomes measurable.
Clinical Translation: Anti-sclerostin antibodies (romosozumab) mimic mechanical loading's anabolic effect by blocking sclerostin function. This therapeutic approach demonstrates the clinical relevance of mechanotransduction pathways.
RANKL/OPG Ratio
Osteocytes regulate osteoclast recruitment through the RANKL/OPG system. Mechanical loading decreases RANKL expression and increases OPG, reducing osteoclast formation.
| Condition | RANKL | OPG | Bone Remodeling Effect |
|---|---|---|---|
| Mechanical Loading | Decreased | Increased | Reduced resorption, increased formation |
| Normal Activity | Baseline | Baseline | Balanced remodeling |
| Immobilization | Increased | Decreased | Increased resorption |
| Osteocyte Apoptosis | Markedly increased | Decreased | Targeted remodeling at damage |
Clinical Relevance and Applications
Wolff's Law
Wolff's Law states that bone adapts its structure to the mechanical demands placed upon it. Osteocyte mechanotransduction is the cellular mechanism underlying this principle.
Wolff's Law in Practice
Examples of Wolff's Law:
- Tennis players develop 30-40% greater cortical thickness in dominant arm
- Astronauts lose 1-2% bone mass per month in microgravity
- Bed rest causes measurable bone loss within 2 weeks
- Weight-bearing exercise increases bone density in loaded regions
All mediated by osteocyte mechanosensing.
Disuse Osteoporosis
Absence of mechanical loading causes bone loss through multiple mechanisms, all initiated by changes in osteocyte signaling.
Mechanisms:
- Increased sclerostin: Inhibits bone formation
- Increased RANKL/OPG ratio: Promotes resorption
- Reduced anabolic signals: PGE2 and NO decrease
- Osteocyte apoptosis: Loss of mechanosensory network
Clinical Scenarios:
- Prolonged bed rest (1-2% bone loss per week)
- Spinal cord injury (rapid bone loss below injury)
- Immobilization in cast (local bone loss)
- Spaceflight (microgravity environment)
Stress Fractures
Stress fractures occur when bone adaptation cannot keep pace with repetitive loading, representing a failure of mechanotransduction to maintain structural integrity.
Mechanotransduction and Stress Fractures
Pathophysiology: Repetitive loading without adequate rest prevents completion of targeted remodeling. Microdamage accumulates faster than repair, creating stress risers. Osteocyte apoptosis signals remodeling, but insufficient time for completion creates temporary weakness.
Prevention requires understanding the remodeling timeline: 3-4 months for complete BMU cycle.
Differential: Distinguishing the Bone Cells and Their Mechanobiology
A common viva trap is confusing the four bone cell types and their distinct roles in load sensing and remodeling.
| Cell | Origin | Mechano Role | Key Signal | Distinguishing Feature |
|---|---|---|---|---|
| Osteocyte | Embedded osteoblast | Primary mechanosensor | Sclerostin (off with load); RANKL | 90-95% of bone cells; dendritic, in lacunae |
| Osteoblast | Mesenchymal stem cell | Effector of formation | Responds to Wnt; lays osteoid | Cuboidal, on bone surface, synthesises matrix |
| Bone-lining cell | Quiescent osteoblast | Surface barrier / canopy | Gates BMU access | Flat, inactive surface cell |
| Osteoclast | Haematopoietic (monocyte) | Effector of resorption | Activated by RANKL; inhibited by OPG | Multinucleate; ruffled border, Howship lacuna |
Controversies and Areas of Uncertainty
The proximate mechanosensor
Whether the primary cilium, integrin-tethered dendrites, the pericellular matrix/glycocalyx, or membrane ion channels (e.g. Piezo1, TRPV4) is the dominant sensor remains debated. Piezo1 has emerged as a strong candidate in recent murine work, and the relative contribution of each likely varies with stimulus type.
Optimal loading prescription
The ideal magnitude, strain rate, cycle number and - importantly - rest-insertion between bouts to maximise the anabolic response in humans are not standardised. Few cycles of high-rate loading with rest periods appear more osteogenic than many monotonous cycles, but human dosing is unresolved.
Anabolic vs resorptive osteocyte RANKL
Osteocytes are the major RANKL source, yet how a single cell network coordinately suppresses RANKL under load while raising it around microdamage and in disuse is incompletely understood.
Romosozumab cardiovascular signal
The ARCH trial raised a cardiovascular safety signal not seen in FRAME. Whether this reflects sclerostin's extra-skeletal (vascular) roles or chance remains contested, and it shapes prescribing in patients at cardiovascular risk.
Evidence Base
Mechanical Loading Reduces Sost/Sclerostin Expression In Vivo
- Ulnar loading in rats dramatically reduced Sost transcripts and sclerostin protein in osteocytes
- Effect was strain-dependent: higher-strain cortical regions showed greater loss of sclerostin-positive osteocytes
- Hindlimb unloading conversely increased Sost expression in the tibia
- Sclerostin antagonises Lrp5/Wnt signalling, the key skeletal mechanotransduction pathway
Osteocytes Are the Major Source of RANKL in Bone Remodeling
- Purified osteocytes express far higher RANKL and support more osteoclastogenesis than osteoblasts or stromal cells
- Mice lacking RANKL specifically in osteocytes develop a severe osteopetrotic phenotype
- Establishes osteocytes - not surface osteoblasts - as the dominant in vivo RANKL source
- Repositions the osteocyte network as the master regulator of both formation and resorption
Targeted Ablation of Osteocytes Causes Fragile Bone and Defective Mechanotransduction
- Diphtheria-toxin ablation killed 70-80% of osteocytes without killing osteoblasts
- Osteocyte-ablated mice developed intracortical porosity, microfractures and trabecular bone loss resembling the aging skeleton
- Critically, osteocyte-less mice were resistant to unloading-induced bone loss
- Provides direct in vivo proof that osteocytes are the cells mediating mechanotransduction
Pulsating Fluid Flow Drives NO and PGE2 Release from Osteocytes
- Osteocytes (but not periosteal fibroblasts) responded to pulsating fluid flow at ~0.5 Pascal
- Flow produced a rapid 2 to 3-fold rise in nitric oxide release, maximal at 5 minutes
- PGE2 release followed, sustained over 60 minutes of flow
- NO synthase inhibition blocked both NO and PGE2 release, placing NO upstream
Connexin 43 Deficiency Attenuates the Anabolic Response to Load
- Cx43-null osteoblasts produced less PGE2 in response to cyclic stretch in vitro
- Osteoblast-specific Cx43 deletion reduced endosteal bone apposition after in vivo tibial loading
- Loading-induced anabolism was attenuated but NOT abolished by Cx43 loss
- Confirms gap-junction/hemichannel communication amplifies, rather than solely gates, mechanotransduction
Romosozumab (Anti-Sclerostin) Reduces Vertebral Fracture - FRAME Trial
- Randomised placebo-controlled trial of 7180 postmenopausal women with osteoporosis
- Romosozumab cut new vertebral fractures by 73% at 12 months (0.5% vs 1.8%)
- Clinical fractures fell 36% at 1 year; benefit persisted after transition to denosumab
- Demonstrates that pharmacologic sclerostin blockade reproduces the anabolic effect of mechanical loading
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Basic Mechanotransduction Mechanism
"Examiner asks: Explain how mechanical loading of bone is sensed by osteocytes and converted into a cellular response."
Scenario 2: Clinical Application - Disuse Osteoporosis
"A patient with spinal cord injury develops rapid bone loss below the level of injury. Explain the cellular mechanism and potential therapeutic interventions based on mechanotransduction principles."
Scenario 3: Stress Fractures and Targeted Remodeling
"A military recruit develops a tibial stress fracture during basic training. Using mechanotransduction and osteocyte biology, explain why this occurred and how bone normally protects itself from fatigue damage."
MCQ Practice Points
Osteocyte Proportion Question
Q: What percentage of bone cells are osteocytes? A: 90-95% - Despite their small volume fraction in bone, osteocytes vastly outnumber osteoblasts and osteoclasts, reflecting their role as the mechanosensory network.
Primary Cilium Function Question
Q: What is the primary mechanosensor for detecting fluid flow in osteocytes? A: Primary cilium - This solitary non-motile organelle projects into the pericellular space and bends with fluid flow, activating mechanosensitive ion channels when deflected 50-100 nanometers.
Sclerostin Response Question
Q: How does mechanical loading affect sclerostin expression? A: Loading suppresses sclerostin - SOST gene expression decreases within 1-6 hours of mechanical loading, reducing sclerostin protein levels and disinhibiting Wnt signaling in osteoblasts to promote bone formation.
Gap Junction Protein Question
Q: Which connexin protein is critical for osteocyte mechanotransduction? A: Connexin 43 (Cx43) - Forms gap junctions between osteocytes, enabling calcium wave propagation and coordinated responses to mechanical stimuli. Mutations cause skeletal abnormalities.
Osteocyte Apoptosis Question
Q: What signal does osteocyte apoptosis send for targeted remodeling? A: Increased RANKL expression - Dying osteocytes upregulate RANKL in surrounding viable cells within 24-72 hours, recruiting osteoclasts to remove damaged bone at specific locations.
Guidelines, Registries & Global Practice
Global Epidemiology and Clinical Burden
- Osteoporosis affects an estimated 500 million people worldwide; one in three women and one in five men over 50 will sustain a fragility fracture.
- Disuse-related bone loss is a universal problem: prolonged bed rest, spinal cord injury and microgravity all produce bone loss on the order of 1-2% per month at weight-bearing sites, all initiated by altered osteocyte signalling.
- Sclerostin biology underpins a now-global drug class (romosozumab), approved by the FDA, EMA and many national agencies for high fracture-risk osteoporosis.
Anti-Sclerostin Therapy: Side-by-Side Guidance
| Body | Position on romosozumab (anti-sclerostin) |
|---|---|
| AACE/ACE (US) | Recommended for patients at very high fracture risk; avoid in those with recent MI/stroke |
| Endocrine Society (US) | Option for severe osteoporosis with high fracture risk; followed by an antiresorptive |
| NICE / NOGG (UK) | Recommended for severe postmenopausal osteoporosis at very high fracture risk after prior fracture |
| IOF/ESCEO (Europe) | Anabolic-first sequencing for very high risk; mandatory transition to antiresorptive afterwards |
Convergent principle: all guidelines agree on two points derived directly from osteocyte mechanobiology - sclerostin blockade is anabolic, and its effect must be "locked in" with a subsequent antiresorptive because bone loss resumes on cessation.
Exam Relevance (FRCS, FRACS, EBOT, ABOS, DNB/MS, MRCS, SICOT)
- Osteocyte mechanotransduction and Wolff's Law are core basic-science viva and MCQ topics across all major fellowship exams.
- High-yield: lacunocanalicular fluid-flow mechanics, primary cilium vs integrin sensing, connexin 43 gap junctions/hemichannels, and sclerostin (SOST/Wnt-Lrp5) regulation.
- Examiners expect candidates to link the cell biology to clinical phenomena - disuse osteoporosis, stress fractures, and the mechanism of romosozumab.
Resource-Setting Practice Variation
- High-resource settings: anti-sclerostin and anabolic agents available; spinal-cord-injury units use standing frames and functional electrical stimulation to limit sublesional bone loss; early supervised weight-bearing after fracture.
- Limited-resource settings: emphasis shifts to low-cost, evidence-based loading - progressive weight-bearing, resistance and impact exercise, and falls-prevention programmes (e.g. Otago-type) - which exploit the same mechanotransduction pathway without pharmacotherapy.
Management Algorithm
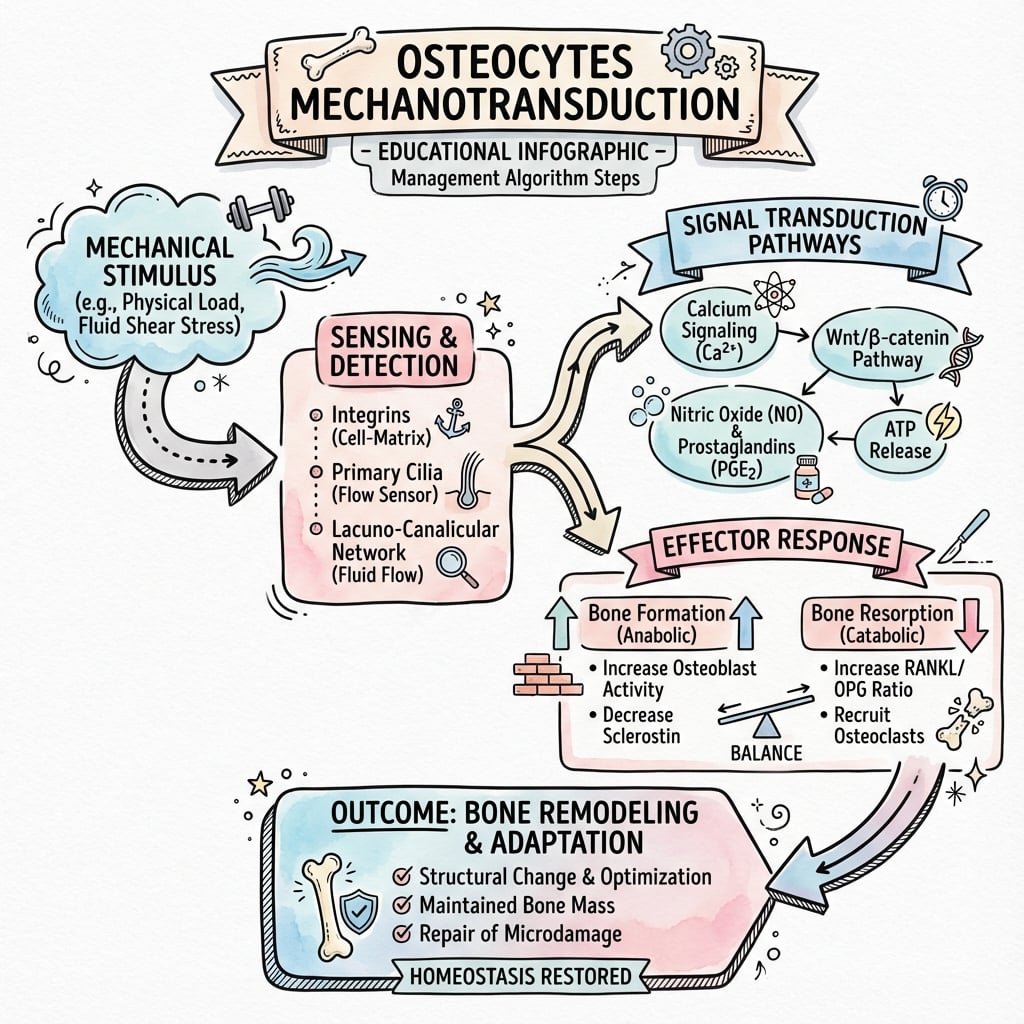
OSTEOCYTES AND MECHANOTRANSDUCTION
Clinical summary
Key Cellular Architecture
- •Osteocytes = 90-95% of all bone cells (most abundant)
- •40-100 dendritic processes per cell through canaliculi
- •Lacunocanalicular network enables fluid flow
- •Pericellular space = 50-100 nm (site of shear stress)
Mechanosensors
- •Primary Cilium = flow sensor (bends with 50-100 nm displacement)
- •Integrins = strain sensor (matrix attachment)
- •Connexin 43 Gap Junctions = cell-cell communication
- •Hemichannels = ATP/PGE2 release (paracrine signaling)
Molecular Responses to Loading
- •Sclerostin DECREASES (SOST gene suppressed)
- •RANKL/OPG ratio DECREASES (less resorption)
- •PGE2 and NO release INCREASES (anabolic)
- •Calcium waves propagate through network
Clinical Applications
- •Wolff's Law = structural adaptation via mechanotransduction
- •Disuse osteoporosis = increased sclerostin, increased RANKL
- •Stress fractures = inadequate remodeling response
- •Anti-sclerostin drugs (romosozumab) mimic loading
Timelines
- •0-1 hour: SOST gene transcription decreases
- •6-24 hours: Sclerostin protein levels fall
- •24-72 hours: Osteocyte apoptosis triggers RANKL
- •Weeks: Measurable bone formation response