Osteoclast Hyperactivity | Bone Remodeling Disorder | Bisphosphonate Responsive
- Pathophysiology: Abnormal osteoclast activity leads to disorganized bone remodeling with woven bone
- Biochemistry: Elevated alkaline phosphatase (ALP) with normal calcium and phosphate
- Radiology triad: Bone expansion, cortical thickening, trabecular coarsening
- First-line treatment: Bisphosphonates (zoledronic acid single dose highly effective)
- Orthopaedic complications: Pathological fracture, deformity, arthritis, sarcomatous change
- “Normal calcium differentiates from hyperparathyroidism and malignancy
- “Flame-shaped or V-shaped lytic lesions on X-ray are pathognomonic
- “Sarcomatous transformation presents as sudden pain increase with soft tissue mass
- “Prophylactic bisphosphonates reduce perioperative bleeding for elective surgery
Elevated ALP with normal calcium and phosphate is the hallmark. Calcium elevation suggests immobilization hypercalcemia or malignancy. PTH is normal, distinguishing from hyperparathyroidism.
Lytic phase (osteoporosis circumscripta in skull), mixed phase (blade of grass in long bones), sclerotic phase (dense cotton wool appearance). Most lesions show mixed pattern.
Zoledronic acid 5mg single IV dose is now standard of care. Reduces bone pain, normalizes ALP in 90% by 6 months. Oral alendronate or risedronate are alternatives. Indications: symptoms, high-risk sites, preoperative.
1% lifetime risk but extremely poor prognosis. Suspect with sudden pain increase, soft tissue mass, lytic expansion on X-ray. Most are osteosarcoma. Requires wide resection or amputation with chemotherapy.
Overview and Epidemiology
Paget's disease of bone is a chronic disorder of excessive and disorganized bone remodeling. Second most common metabolic bone disease after osteoporosis.
- 3-4% prevalence over age 55
- Male predominance (M:F 3:2)
- 70-80% asymptomatic
- High in UK/Australia/NZ, rare in Asia/Africa
- Familial clustering (15-30% have affected relative)
Pathological fractures, deformity, secondary arthritis, increased operative bleeding, implant fixation challenges.
Pathophysiology and Bone Biology
Cellular Mechanism
Disease Progression
Excessive osteoclast activity with abnormally large multinucleated osteoclasts (up to 100 nuclei vs normal 3-5). Rapid bone resorption exceeds formation. Radiology shows advancing lytic fronts (flame-shaped or blade-of-grass lesions).
Osteoblasts attempt to repair but lay down disorganized woven bone instead of lamellar bone. Mosaic pattern on histology. Bone is mechanically weak despite increased mass. Most symptomatic disease occurs in this phase.
Osteoblast predominance with dense, sclerotic bone formation. Reduced turnover but bone remains structurally abnormal. Cotton-wool appearance on X-ray. May still have complications despite reduced activity.
The disorganized woven bone in Paget's is structurally weaker than normal lamellar bone despite appearing denser on imaging. This creates susceptibility to stress fractures (especially lateral femoral cortex, anterior tibial cortex) and pathological fractures with minimal trauma.
Etiology
Multifactorial: SQSTM1 gene mutations (15-30% familial cases), chromosome 18q abnormalities. Slow virus hypothesis (measles paramyxovirus) not proven. Geographic clustering and declining incidence suggest environmental trigger.
Principles and Core Concepts
The Pathognomonic Triad
Paget's disease is defined by three cardinal features:
1. Biochemical Hallmark: Elevated ALP with Normal Calcium
- Alkaline phosphatase reflects osteoblast activity (10-15x normal in active disease)
- Normal calcium distinguishes from malignancy and hyperparathyroidism
- Normal phosphate and PTH confirm isolated bone remodeling disorder
2. Radiological Hallmark: Bone Expansion with Cortical Thickening
- Increased bone diameter (expansion)
- Cortical thickening (widened cortex)
- Trabecular coarsening (thickened trabeculae)
- Mixed lytic-sclerotic pattern in active disease
3. Histological Hallmark: Mosaic Woven Bone
- Disorganized woven bone instead of lamellar bone
- Mosaic cement lines (multiple resorption-formation cycles)
- Giant osteoclasts (up to 100 nuclei)
- Mechanically weak despite increased bone mass
Clinical Principles
- 70-80% asymptomatic (incidental finding on X-ray or bloods)
- Geographic variation (high in UK/Australia, rare in Asia/Africa)
- Zoledronic acid single dose: 90% ALP normalization, 2+ year remission
- Preoperative bisphosphonates reduce bleeding 40-50%
- Pathological fractures need long implants bypassing pagetic bone
- Joint arthroplasty requires cemented long-stem components
- Hyperemic bone causes significant operative bleeding
- Deformity correction complicated by altered anatomy
Clinical Assessment
History
Most patients are asymptomatic (70-80% discovered incidentally). When symptomatic:
- Bone pain: Deep, aching, worse at night
- Deformity: Bowing of long bones, skull enlargement
- Fracture: Minimal trauma or stress fracture
- Arthritis pain: Hip, knee adjacent to pagetic bone
- High-output cardiac failure: Extensive disease (greater than 35% skeleton)
- Nerve compression: Skull base (CN VIII deafness), spine (stenosis)
- Hypercalcemia: During immobilization
- Warmth over bone: Increased vascularity
Examination
- Bone enlargement (skull circumference increased, tibial bowing, femoral bowing)
- Skin warmth over affected bone (hypervascularity)
- Gait abnormality (leg length discrepancy, joint deformity)
- Bone tenderness over active lesions
- Increased temperature over pagetic bone
- Joint effusions if secondary arthritis
- Cranial nerve examination (skull base involvement)
- Spinal cord signs if vertebral disease with stenosis
Patients may report needing larger hat sizes due to progressive skull enlargement. This is a classic history finding in advanced skull Paget's. Similarly, tibial bowing may require shoe modifications.
Biochemical and Imaging Investigations
Biochemistry
- Finding
- Elevated (10-15x normal)
- Interpretation
- Reflects osteoblast activity and disease extent
- Differential
- Liver disease, bone metastases, hyperparathyroidism
- Finding
- Normal
- Interpretation
- Distinguishes from malignancy and hyperPTH
- Differential
- Elevated if immobilized or rare hypercalcemia
- Finding
- Normal
- Interpretation
- Normal bone mineralization
- Differential
- Abnormal in renal osteodystrophy
- Finding
- Normal
- Interpretation
- Excludes primary hyperparathyroidism
- Differential
- Elevated in hyperPTH
- Finding
- Elevated (urine N-telopeptide, serum CTX)
- Interpretation
- Reflects osteoclast activity, monitors treatment
- Differential
- Used to assess treatment response
Elevated ALP with normal calcium and phosphate is diagnostic. If calcium is elevated, consider immobilization hypercalcemia, malignancy, or coexistent hyperparathyroidism. Check PTH and 25-OH vitamin D to differentiate.
Radiology
Plain radiographs are diagnostic in most cases:
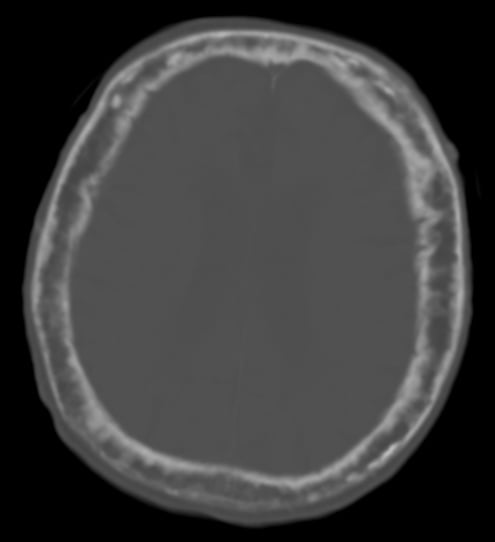
Skull Paget's Radiological Features
- Osteoporosis circumscripta (geographic lytic area)
- Cotton-wool appearance (patchy sclerosis)
- Cortical thickening (skull base, calvarium)
- Basilar invagination (platybasia)
- Cranial nerve foramina narrowing
- Inner table thickening
These findings help distinguish Paget's from other skull pathology.
Nuclear Medicine
Bone scan (Tc-99m MDP): Highly sensitive for active lesions. Shows increased uptake at pagetic sites. Useful for determining disease extent before treatment. Cannot distinguish from metastases (need X-ray correlation). Helpful for planning surgery, detecting polyostotic disease, and monitoring response.
Differential Diagnosis
The combination of an elevated ALP and a sclerotic/expanded bone has several mimics. The discriminators are serum calcium, PTH, the pattern of bone change, and whether multiple bones are involved.
- Calcium / PTH
- Normal calcium, normal PTH
- ALP
- Elevated (10-15x)
- Distinguishing features
- Bone expansion, cortical thickening, coarse trabeculae; flame/blade-of-grass front; spares hands/feet
- Calcium / PTH
- Calcium normal or high; PTH low/normal
- ALP
- Elevated
- Distinguishing features
- Multiple ill-defined sclerotic foci WITHOUT bone expansion; known primary; PSA may be raised
- Calcium / PTH
- HIGH calcium, HIGH PTH
- ALP
- Mildly elevated
- Distinguishing features
- Subperiosteal resorption, brown tumours, osteopenia - not bone expansion
- Calcium / PTH
- Low/normal calcium, HIGH PTH, HIGH phosphate
- ALP
- Elevated
- Distinguishing features
- Rugger-jersey spine, CKD context, abnormal phosphate
- Calcium / PTH
- Normal calcium/PTH
- ALP
- Normal or mildly elevated
- Distinguishing features
- Younger patient; ground-glass lytic lesions, shepherd's crook; no cortical thickening
- Calcium / PTH
- Normal calcium/PTH
- ALP
- Disproportionate rise
- Distinguishing features
- New lytic destructive lesion, cortical breach, soft-tissue mass on a background of Paget's
Bone expansion is the feature that most reliably separates Paget's from metastatic disease: pagetic bone enlarges and thickens its cortex, whereas metastases deposit within bone of normal size. Combined with normal calcium and PTH, this distinguishes Paget's from the metabolic mimics.
Management Algorithm
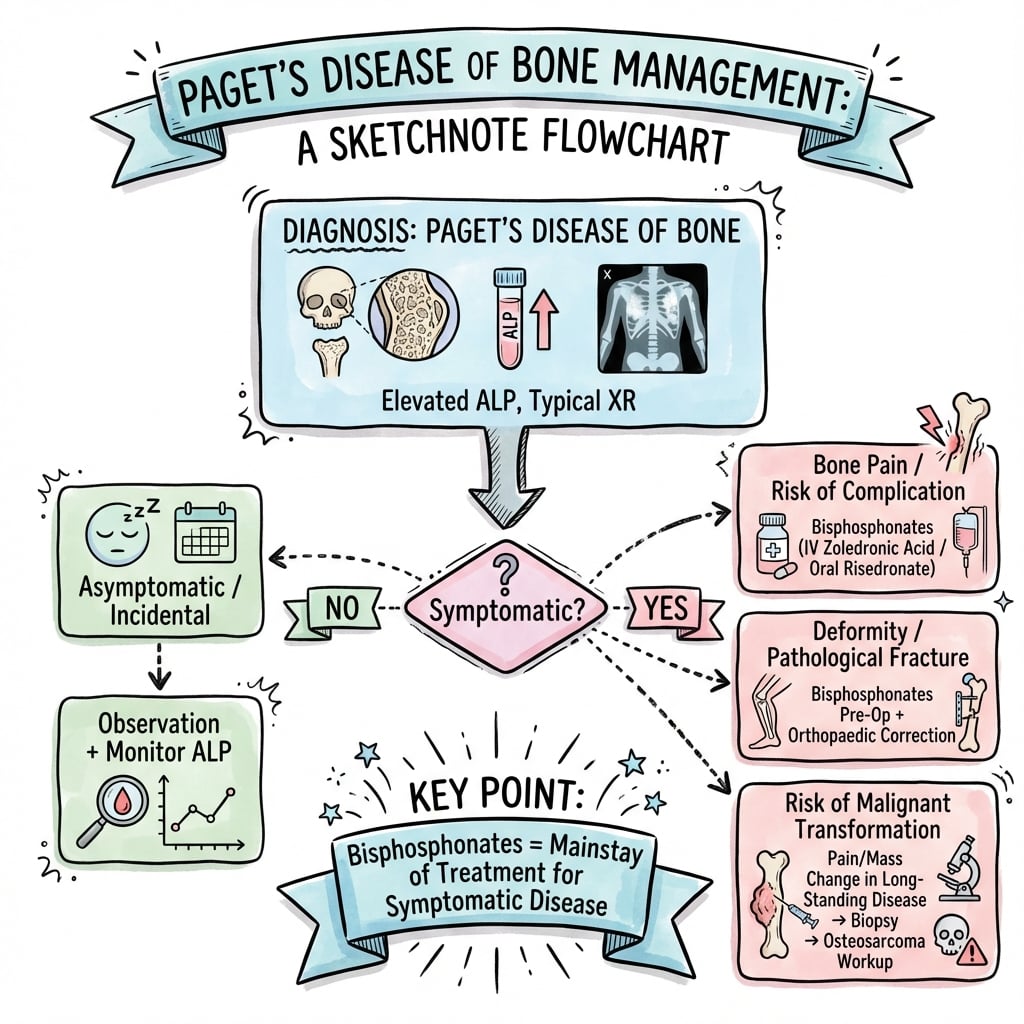
Bisphosphonates - First-Line Treatment
Mechanism: Inhibit osteoclast activity, reduce bone turnover, normalize ALP
- Dosing
- 5mg single infusion
- Efficacy
- 90% ALP normalization at 6 months, durable response years
- Indications
- First-line, convenient, high efficacy
- Dosing
- 40mg daily × 6 months
- Efficacy
- 70-80% ALP normalization
- Indications
- Alternative if IV not tolerated
- Dosing
- 30mg daily × 2-3 months
- Efficacy
- 75-85% ALP normalization
- Indications
- Oral option, shorter course
- Dosing
- 60-90mg infusions
- Efficacy
- Effective but multiple doses required
- Indications
- Second-line if zoledronic acid unavailable
Indications for Treatment
- Bone pain attributable to Paget's
- Neurological complications (nerve compression)
- High-output cardiac failure (rare)
- Weight-bearing long bones (risk of fracture/deformity)
- Skull base involvement (risk of cranial nerve compression)
- Spine with stenosis risk
- Juxta-articular disease (risk of secondary arthritis)
- Planned surgery on pagetic bone (reduce vascularity and bleeding)
- Give bisphosphonate 3-6 months before elective surgery
Acute phase reaction (fever, myalgia) occurs in 30% after IV bisphosphonate, managed with paracetamol. Rare complications: osteonecrosis of jaw (dental hygiene critical), atypical femoral fractures (long-term use). Ensure adequate calcium and vitamin D before treatment.
Calcium and Vitamin D Supplementation
Always coadminister:
- Calcium 1000-1200mg daily
- Vitamin D 800-1000 IU daily
- Prevents hypocalcemia after bisphosphonate treatment
- Optimizes bone health
Monitoring
ALP at 3, 6, 12 months (goal: normalize or 75% reduction). Rising ALP = reactivation. Bone turnover markers (NTX, CTX) more sensitive.
Surgical Management and Orthopaedic Complications
Indications for Surgery
- Pathological fractures: Fixation often required
- Stress fractures: Prophylactic fixation if high-risk (femoral neck)
- Nonunion: May require bone graft and revision fixation
- Joint arthroplasty: Secondary arthritis (hip most common)
- Corrective osteotomy: Severe deformity affecting function
- Decompression: Spinal stenosis, nerve root compression
Preoperative Optimization
- Reduces bone vascularity
- Decreases operative blood loss (up to 50% reduction)
- Normalizes bone turnover
- Improves fixation quality
- Pagetic bone highly vascular
- Risk of significant intraoperative bleeding
- Have blood products available
Operative Considerations
- Mechanism
- Hypervascularity of pagetic bone
- Management Strategy
- Preop bisphosphonate, tourniquet, cell saver, controlled hypotension
- Mechanism
- Bone expansion, deformity
- Management Strategy
- Preop CT for templating, custom implants if needed
- Mechanism
- Soft woven bone
- Management Strategy
- Cement augmentation, long-stem components, prophylactic cerclage
- Mechanism
- Weak bone during manipulation
- Management Strategy
- Gentle handling, prophylactic fixation extensions
Total Hip Arthroplasty in Paget's
Special considerations:
- Altered femoral anatomy (bowing, coxa vara)
- Acetabular protrusion common
- Use cemented long-stem femoral component (better fixation in soft bone)
- Consider cementless acetabular component with screw fixation
- Higher rate of heterotopic ossification (consider prophylaxis with indomethacin or radiation)
Cemented femoral stems provide better fixation in the soft woven bone of Paget's disease compared to press-fit cementless stems. Long-stem components bypass deformity and stress risers. Acetabular components can be cementless if bone quality adequate.
Complications
- Incidence
- 10-30% lifetime risk
- Presentation
- Minimal trauma fracture, stress fracture (femur, tibia)
- Management
- Fixation (often requires long plates/nails), bisphosphonates
- Incidence
- Common in hip/knee
- Presentation
- Progressive joint pain, stiffness, juxta-articular disease
- Management
- Arthroplasty (THA most common), preop bisphosphonate
- Incidence
- 1% lifetime risk
- Presentation
- Sudden pain increase, soft tissue mass, rapid lytic expansion
- Management
- Biopsy, staging, wide resection or amputation + chemo
- Incidence
- Common (tibia, femur)
- Presentation
- Progressive bowing, leg length discrepancy, gait abnormality
- Management
- Corrective osteotomy if severe functional impairment
- Incidence
- Skull base, spine
- Presentation
- Deafness (CN VIII), spinal stenosis, radiculopathy
- Management
- Bisphosphonates, surgical decompression if progressive
- Incidence
- Rare (immobilization)
- Presentation
- Polyuria, confusion, immobilization triggers
- Management
- Hydration, bisphosphonates, mobilize patient
Osteosarcoma (most common), fibrosarcoma, or malignant fibrous histiocytoma can arise in pagetic bone (1% lifetime risk). Suspect when sudden increase in pain, soft tissue mass, rapid radiological change. Prognosis is poor (5-year survival under 10%). Requires biopsy, staging MRI/CT, wide resection or amputation with chemotherapy. The full staging pathway, histology and reconstruction are developed in the dedicated Paget's sarcoma topic.
Cardiovascular Complications and High-Output Cardiac Failure
The one-pager and treatment indications repeatedly invoke high-output cardiac failure as a systemic complication of extensive Paget's, but the mechanism deserves explicit development because it is a classic basic-science viva stem and the reason "disease extent," not just symptoms, can justify treatment.
Why pagetic bone raises cardiac output
Actively remodelling pagetic bone is intensely hypervascular: dilated marrow sinusoids and increased blood flow through the affected bone and overlying skin behave functionally like a low-resistance arteriovenous shunt (clinically felt as warmth over the bone). Where a large fraction of the skeleton is involved, the summed increase in resting blood flow raises cardiac output and preload, producing a high-output state.
True high-output failure is rare and generally requires extensive polyostotic disease (classically more than 15% of the skeleton involved). Monostotic or limited disease does not cause it. This is why widespread active disease is itself a treatment consideration, independent of local bone pain.
The increased demand most often decompensates pre-existing cardiac disease (ischaemic heart disease, valvular disease) in an elderly population rather than causing failure in a healthy heart. Warmth and bounding pulses over pagetic limbs are supportive clinical signs.
Paget's is associated with an excess of calcific aortic valve disease and generalised vascular calcification, which compounds cardiac risk and can coexist with the high-output physiology.
Suppressing bone turnover with a bisphosphonate reduces pagetic bone vascularity and blood flow, and can improve the high-output state - the same hypervascularity that drives cardiac load is what makes preoperative bisphosphonate reduce surgical bleeding.
If asked why an asymptomatic patient with very widespread active Paget's might still be treated, the cardiovascular argument is a strong answer: extensive hypervascular bone (classically more than 15% of the skeleton) can raise cardiac output and decompensate an ageing heart, and bisphosphonate therapy that reduces bone blood flow can relieve it. Reserve this explanation for extensive polyostotic disease - it does not apply to monostotic Paget's.
Neurological Complications: Deafness, Basilar Invagination and Spinal Stenosis
The topic names CN VIII deafness, skull-base involvement, basilar invagination (platybasia), spinal stenosis and radiculopathy as complications but leaves them as bullet stubs. Because these are high-yield viva material - and because the mechanism dictates whether medical or surgical treatment comes first - they are developed here.
Hearing loss (the commonest neurological complication)
Deafness in skull Paget's is typically mixed sensorineural and conductive. The dominant contributor is thought to be pagetic remodelling and demineralisation of the cochlear (otic) capsule and cochlear structures, rather than simple compression of the eighth nerve at the internal auditory meatus; a conductive component can arise from involvement of the ossicles and temporal bone. Practically, established hearing loss responds poorly, so treatment aims to slow progression.
Skull base: basilar invagination and platybasia
Softening of the pagetic skull base allows the odontoid to migrate upward into the foramen magnum (basilar invagination / platybasia). This can produce brainstem and upper cervical cord compression, vertebrobasilar symptoms, and obstructive hydrocephalus from aqueduct/outflow compromise. It is a serious, though uncommon, complication of extensive calvarial disease.
Spine: stenosis, myelopathy and the vascular-steal phenomenon
Vertebral Paget's (picture-frame or ivory vertebra with bony expansion) narrows the canal and neural foramina, causing spinal stenosis, myelopathy, radiculopathy or cauda equina syndrome.
A characteristic feature of pagetic spinal syndrome is that some neurological deficit is due not only to mechanical compression but to a vascular steal, where blood is diverted from the spinal cord into adjacent hypervascular pagetic bone. Because of this, medical therapy that reduces bone blood flow (bisphosphonates; historically calcitonin) can improve neurology without surgery. A trial of medical treatment is therefore reasonable first-line for slowly progressive pagetic myelopathy, reserving urgent surgical decompression for rapidly progressive, severe or refractory deficits.
Hearing loss is the commonest neurological complication and is driven mainly by otic-capsule remodelling (so bisphosphonates aim to slow it, not reverse it). For spinal deficits, remember the vascular-steal concept: reducing pagetic bone blood flow can recover function, so a slowly progressive pagetic myelopathy warrants a trial of bisphosphonate before committing to decompression - whereas a rapidly progressive or severe deficit needs urgent surgery.
Guidelines, Registries & Global Practice
Global epidemiology: Strong geographic and ethnic gradient. Highest prevalence in populations of Anglo-Celtic / Western European descent (UK, Australia, New Zealand, North America, and emigrant communities), where it affects roughly 1-4% over age 55. Rare in Scandinavia, much of Asia and sub-Saharan Africa. Incidence and severity have declined markedly over recent decades across high-prevalence regions, supporting an environmental contribution alongside SQSTM1-related genetic susceptibility.
Side-by-Side Guideline Comparison
- When to treat
- Active disease at risk of complications; before pagetic-bone surgery
- First-line agent
- Single 5mg IV zoledronate
- Treatment target
- Symptom control; ALP/turnover marker response
- When to treat
- Bone pain attributable to disease; pre-surgery; selected high-risk sites
- First-line agent
- Zoledronate (potent, durable)
- Treatment target
- Symptom control rather than universal ALP normalization (PRISM-EZ)
- When to treat
- Mechanical complications: impending/actual fracture, deformity, arthritis, stenosis
- First-line agent
- Bisphosphonate plus surgery as indicated
- Treatment target
- Restore alignment, stable fixation, reduce perioperative bleeding
older guidance emphasised normalizing ALP in all active disease; the PRISM-EZ RCT showed no clinical benefit from intensive turnover suppression in established disease, so contemporary UK/European practice favours treating symptoms and high-risk sites rather than every elevated ALP.
Arthroplasty registries (NJR England & Wales, AOANJRR Australia, AJRR US, Swedish/Norwegian/NZ registries) and dedicated pagetic cohorts report 10-year hip implant survival around 90%, with bleeding/transfusion and heterotopic ossification as the dominant complications rather than early loosening.
Where IV zoledronate and DXA/bone scan are available, a single infusion with biochemical monitoring is standard. In limited-resource settings, oral risedronate/alendronate and serial ALP (a cheap, widely available marker) are pragmatic alternatives; plain radiographs alone are usually sufficient for diagnosis and surgical planning.
Controversies and Areas of Uncertainty
The PRISM-EZ RCT found that intensively suppressing bone turnover to normalize ALP gave no improvement in pain, quality of life or fractures over symptomatic treatment - and a non-significant trend to MORE fractures. Whether asymptomatic high-risk sites still warrant treatment remains unresolved.
Guidelines suggest treating active disease "at risk of complications," but robust evidence that bisphosphonates prevent fracture, deformity, deafness or arthritis is lacking (Cochrane). Practice varies from treat-all-active to treat-symptoms-only.
Classic teaching favours cemented long stems in soft woven bone, yet modern registry data (Di Martino 2021) show good survival with various fixation types. The dominant problems are bleeding and heterotopic ossification, not fixation failure.
The paramyxovirus (measles) "slow virus" hypothesis remains unproven and contested; declining incidence and SQSTM1 genetics point to a gene-environment interaction whose environmental trigger is still unidentified.
MCQ Practice Points
Q: What is the characteristic biochemical profile of Paget's disease of bone?
A: Elevated alkaline phosphatase (ALP) with NORMAL serum calcium and phosphate. This distinguishes Paget's from hyperparathyroidism (elevated calcium with elevated PTH) and malignancy (elevated calcium with suppressed PTH). ALP can be elevated 10-15x normal, reflecting high bone turnover.
Q: What are the three radiological phases of Paget's disease and their characteristic appearances?
A: Lytic phase: Osteoporosis circumscripta (skull), advancing V-shaped or flame-shaped lytic lesion (long bones). Mixed phase: Active remodeling with "blade of grass" appearance. Sclerotic phase: Dense cortical thickening, trabecular coarsening, "cotton wool" skull appearance. Most lesions show mixed pattern.
Q: What is the most commonly affected site in Paget's disease?
A: Pelvis (70% of polyostotic cases). Order of frequency: pelvis, spine (lumbar more than thoracic), femur, skull, tibia. Paget's typically affects the axial skeleton but spares hands and feet. Monostotic disease occurs in 15-30% of cases.
Q: What clinical features suggest sarcomatous transformation in a patient with known Paget's disease?
A: Sudden increase in pain with new soft tissue mass and rapid lytic expansion on imaging. Risk is approximately 1% lifetime but prognosis is devastating (median survival 6-12 months). Most are osteosarcoma (65%), followed by fibrosarcoma and chondrosarcoma. Requires wide resection/amputation with chemotherapy.
At a Glance
Paget's disease of bone is a chronic disorder of excessive and disorganized bone remodeling characterized by elevated alkaline phosphatase with normal calcium and phosphate—distinguishing it from hyperparathyroidism and malignancy. Three radiographic phases exist: lytic (osteoporosis circumscripta in skull), mixed (blade of grass/flame sign in long bones), and sclerotic (cotton wool appearance). Most patients are asymptomatic (70-80%); when symptomatic, zoledronic acid 5mg IV single dose is first-line treatment, normalizing ALP in 90% by 6 months. Orthopaedic complications include pathological transverse stress fractures, secondary arthritis, and sarcomatous transformation (1% risk) presenting as sudden pain increase with soft tissue mass—typically osteosarcoma with extremely poor prognosis.
PAGETPAGET - Key Features of Paget's Disease
Hook:PAGET - elevated Phosphatase, often Asymptomatic, Geographic pattern, bone Expansion, Trabecular changes
FASTCOMPLICATIONS - Orthopaedic Problems in Paget's
Hook:FAST complications require urgent orthopaedic assessment
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 68-year-old man has routine blood tests showing alkaline phosphatase of 850 U/L (normal 30-120 U/L). Calcium, phosphate, and PTH are normal. He has no bone pain or symptoms. Pelvic X-ray shows cortical thickening and trabecular coarsening of the left hemipelvis. How do you assess and manage this patient?”
“A 72-year-old woman with known Paget's disease affecting her right femur presents with sudden onset thigh pain after a minor fall. X-ray shows a complete transverse fracture through pagetic bone in the mid-femoral shaft. Discuss your management approach.”
“A 70-year-old man with a 12-year history of Paget's disease of the femur, previously stable on bisphosphonates, presents with a 6-week history of new, severe, constant thigh pain and a palpable soft-tissue swelling. His ALP has risen sharply. What is your concern and how do you proceed?”
Key Pathophysiology
- Abnormal osteoclast activity (up to 100 nuclei) leads to excessive bone resorption
- Osteoblasts lay down disorganized woven bone (not lamellar)
- Mosaic pattern on histology, mechanically weak despite increased mass
- Three phases: Lytic, Mixed (active), Sclerotic (burnt-out)
Biochemistry
- ALP elevated 10-15x normal (reflects osteoblast activity)
- Calcium NORMAL (key distinguishing feature)
- Phosphate NORMAL
- PTH NORMAL (excludes hyperparathyroidism)
Radiology Triad
- Bone expansion (increased diameter)
- Cortical thickening (widened cortex)
- Trabecular coarsening (thickened trabeculae)
- Flame/V-shaped lytic front (advancing edge), Cotton-wool sclerosis (skull)
Treatment Algorithm
- First-line: Zoledronic acid 5mg single IV dose
- Indications: Symptoms, high-risk sites (pelvis/long bones/skull/spine), preoperative
- Coadminister calcium 1000-1200mg + vitamin D 800-1000 IU daily
- Monitor ALP at 3, 6, 12 months (goal normalize or 75% reduction)
Surgical Pearls
- Preop bisphosphonate 3-6 months before elective surgery (reduces bleeding 40-50%)
- Cross-match blood (pagetic bone highly vascular)
- Long-stem cemented implants for arthroplasty (better fixation in soft bone)
- Gentle handling (risk of fracture propagation)
Complications
- Pathological fracture 10-30% (transverse stress fractures common)
- Secondary arthritis (hip/knee juxta-articular disease)
- Sarcomatous transformation 1% (sudden pain increase, soft tissue mass)
- Deformity (tibial/femoral bowing, skull enlargement)
Evidence Base and Key Studies
Single-Infusion Zoledronic Acid vs Risedronate (Landmark RCT)
- Two pooled identical double-blind RCTs, 347 evaluable patients: one 5mg IV zoledronic acid infusion vs oral risedronate 30mg daily for 60 days
- Therapeutic response at 6 months 96.0% (zoledronic acid) vs 74.3% (risedronate) (P less than 0.001)
- ALP fully normalized in 88.6% vs 57.9%; shorter median time to response (64 vs 89 days)
- During post-trial follow-up (median 190 days) loss of response occurred in 1/113 zoledronic acid vs 21/82 risedronate patients
Intensive vs Symptomatic Bisphosphonate Strategy (PRISM-EZ)
- 3-year extension of PRISM RCT, 502 patients: intensive treatment to normalize bone turnover vs treating symptoms only
- Despite significantly lower ALP in the intensive arm, no difference in quality of life or bone pain
- Intensive treatment showed a non-significant increase in fractures (HR 1.90, 95% CI 0.91-3.98) and orthopaedic procedures (HR 1.81)
- No clinical benefit from chasing biochemical normalization in established disease
Bisphosphonates for Paget's Disease (Cochrane Review)
- 20 RCTs, 3168 participants
- Bisphosphonates tripled the proportion achieving pain resolution vs placebo (31% vs 9%; RR 3.42), moderate-quality evidence
- Zoledronate gave better pain relief than pamidronate or risedronate in head-to-head data
- Insufficient evidence that biochemical control reduces fractures, orthopaedic surgery or improves quality of life
Sarcomas Arising in Paget's Disease (Largest Clinicopathologic Series)
- 70 sarcomas arising in Paget's disease; older men, predominantly axial skeleton (pelvis)
- 88% were osteosarcoma; all tumours high grade
- 5-year survival only 10%; no correlation with monostotic vs polyostotic disease or disease duration
- Prognosis unrelated to site or stage at presentation
Total Hip Arthroplasty in Paget's Disease (Registry + Institutional Cohort)
- Registry cohort of 66 pagetic THAs: 10-year implant survival 89.5%
- Institutional cohort: Harris Hip Score improved by a mean of 34 points; excellent result in 64%
- Heterotopic ossification in 52% of hips; blood transfusion required in 68% (allogenic)
- Implant survival only partly affected by fixation type or bone remodelling
SQSTM1/p62 Mutation in Paget's Disease (Genetic Basis)
- 24 French-Canadian families and 112 unrelated patients studied
- Recurrent P392L mutation in SQSTM1/p62, flanking the ubiquitin-associated (UBA) domain, identified as a major cause
- SQSTM1 links to the NF-kappaB / osteoclast signalling pathway
- Explains a high proportion of familial disease and underpins genetic counselling
Endocrine Society Clinical Practice Guideline
- GRADE-based guideline (with European Society of Endocrinology input)
- Plain radiographs to diagnose; radionuclide bone scan to map disease extent
- Single 5mg IV zoledronate is the treatment of choice for active disease at risk of complications
- Recommends bisphosphonate before surgery on pagetic bone and to slow hearing loss / adjacent osteoarthritis