Sarcomatous Transformation of Paget Disease | Usually Osteosarcoma | Poor Prognosis
- Paget sarcoma = secondary high-grade bone sarcoma arising in a bone previously affected by Paget disease
- Lifetime risk of sarcomatous transformation in Paget is less than 1 percent (older series quoted 5-10 percent, modern estimates lower)
- Osteosarcoma accounts for 50-60 percent; fibrosarcoma / MFH and chondrosarcoma account for most of the remainder
- Classic clinical pattern: NEW or WORSENING pain, a palpable mass or a pathological fracture in a patient with long-standing Paget
- Biopsy MUST be performed by the musculoskeletal tumour service - core needle, tract planned for later resection
- Prognosis is markedly worse than primary osteosarcoma in adolescents - 5-year survival around 5-25 percent
- “Paget sarcoma is the prototypical SECONDARY bone sarcoma - elderly patient, girdle bones, no prior radiation required
- “Suspect malignant change when pain in a Paget bone changes character, escalates, becomes CONSTANT, or wakes the patient at night
- “A new SOFT TISSUE MASS or PATHOLOGICAL FRACTURE in Paget bone is malignant until proven otherwise
- “ALP may already be elevated from Paget - a FURTHER sustained rise raises suspicion but is not diagnostic
- “Biopsy should be the LAST investigation, not the first - full imaging first to identify the most representative target
Paget sarcoma = high-grade bone sarcoma arising in a bone affected by Paget disease. Almost always arises in polyostotic or long-standing Paget. Median age 60-70 years. Osteosarcoma is the dominant subtype.
NEW or WORSENING pain in a Paget bone, NEW palpable mass, PATHOLOGICAL FRACTURE through a Paget bone. Constant / night pain is malignant until proven otherwise. Rising ALP above a stable baseline is suspicious but not specific.
Pelvis, proximal femur, proximal humerus dominate because they are the most common sites of Paget disease. Spine, tibia and skull can also be involved. Polyostotic Paget carries higher risk than monostotic.
Wide surgical resection (limb-sparing when oncologically safe) plus multi-agent chemotherapy for osteosarcoma subtype. Radiotherapy reserved for unresectable or margin-positive disease. Bisphosphonates / denosumab for ongoing Paget activity.
- Diagnosis
- X-ray + MRI + core biopsy (tumour service)
- Treatment
- Wide resection + chemotherapy if osteosarcoma
- Key Pearl
- Biopsy is the LAST investigation
- Diagnosis
- CT chest + bone scan + core biopsy
- Treatment
- Multimodal: surgery + chemo +/- radiotherapy
- Key Pearl
- Prognosis worse than primary osteosarcoma
- Diagnosis
- X-ray + ALP trend, no urgent biopsy
- Treatment
- Optimise bisphosphonate / denosumab for Paget
- Key Pearl
- Most Paget pain is NOT sarcomatous change
- Diagnosis
- MRI, biopsy, whole-body staging
- Treatment
- Treat the actual lesion (curettage for GCT, etc.)
- Key Pearl
- GCT in Paget is a SEPARATE entity, not sarcoma
CHANGERed Flags in a Paget Bone
Hook:Any CHANGE in a Paget bone - pain, mass, ALP, X-ray, site or extension - must raise suspicion of sarcoma!
MORBIDPaget Sarcoma Prognostic Stigmata
Hook:MORBID outcomes: Paget sarcoma is MORBID because of late presentation, axial location and biology.
Overview and Epidemiology
Paget sarcoma is uncommon but uniquely testable because it ties two of the most heavily examined musculoskeletal topics together: Paget disease of bone and primary malignant bone tumours. Candidates who know the percentage risk, the dominant histology and the presentation pattern score easily. Candidates who cannot differentiate Paget sarcoma from a giant cell tumour arising in Paget (a separate, often benign entity) lose marks.
- Incidence: less than 1 percent of patients with Paget disease develop sarcomatous transformation (modern cohorts)
- Older literature quoted 5-10 percent - the true risk is lower, but the ABSOLUTE NUMBER of cases is high because Paget affects 1-2 percent of adults over 55 in European populations
- Age: median 60-70 years (decades older than primary osteosarcoma)
- Sex: slight male predominance
- Distribution: more common in polyostotic Paget; pelvic and long-bone sites dominate
- Survival: 5-year overall survival 5-25 percent - markedly worse than primary osteosarcoma in adolescents
- Function: most patients require major resection (often pelvic or proximal femur) or amputation
- Morbidity: pathological fracture at presentation in up to 25 percent
- Disease burden: lung metastases at presentation in 10-25 percent
The topic repeatedly calls Paget sarcoma "the prototypical secondary bone sarcoma" - an examiner will often ask you to list the whole family of secondary (non-de-novo) osteosarcomas:
- Paget disease (this topic - the commonest cause of secondary osteosarcoma in the elderly)
- Prior radiation (post-radiation osteosarcoma)
- Fibrous dysplasia (rare malignant transformation, higher in polyostotic / McCune-Albright)
- Bone infarct (e.g. in sickle-cell / caisson disease / steroid-related infarcts)
- Chronic osteomyelitis (rare; more classically Marjolin-type squamous change, but sarcoma is reported)
- Genetic predisposition (hereditary retinoblastoma [RB1], Li-Fraumeni [p53], Rothmund-Thomson) - though these are arguably "primary" in a predisposed host
For post-radiation sarcoma, know Cahan's criteria: (1) the tumour arises within a previously irradiated field; (2) a latency period of (classically) at least 3-5 years; (3) the sarcoma is histologically distinct from / different in type to the original irradiated lesion; and (4) histological proof of sarcoma. Paget sarcoma differs in that it needs no prior radiation - the pagetoid bone itself is the substrate.
Exam point: if asked "causes of secondary osteosarcoma," lead with Paget and prior radiation, then add fibrous dysplasia, bone infarct, chronic osteomyelitis and genetic syndromes - and be ready to recite Cahan's criteria for the radiation-induced subset.
Pathophysiology
Paget disease is a disorder of dysregulated bone remodelling driven by abnormal osteoclasts containing characteristic nuclear and cytoplasmic inclusions (paramyxovirus-like on EM, possibly viral in origin) and somatic mutations in the SQSTM1/p62 gene. The relentless remodelling cycle (lytic, mixed, sclerotic) creates a high bone turnover state with disordered matrix. Over years, genomic instability accumulates - p53 mutations, chromosomal aneuploidy - leading to a clonal high-grade sarcoma, almost always osteosarcoma. The longer the disease has been active, and the more bones involved, the higher the cumulative risk.
- Paget Disease
- Dysregulated but polyclonal remodelling
- Paget Sarcoma
- Clonal malignant mesenchymal proliferation
- Paget Disease
- SQSTM1/p62 (sequestosome 1) common
- Paget Sarcoma
- p53 loss / mutation frequent in sarcoma
- Paget Disease
- Mosaic pattern of cement lines, large osteoclasts
- Paget Sarcoma
- Pleomorphic spindle cells, malignant osteoid (osteosarcoma)
- Paget Disease
- Benign, controlled by bisphosphonates
- Paget Sarcoma
- Aggressive, metastasises to lungs
Step 1: SQSTM1/p62 mutation drives abnormal osteoclast signalling (NF-kB pathway)
Step 2: Chronic high-turnover state, disordered lamellar bone
Step 3: Decades of cellular stress, p53 mutation
Step 4: Clonal high-grade sarcoma - osteoid matrix by malignant cells
Result: An aggressive bone-forming sarcoma in an elderly patient
Patient factors: older age, comorbidities limit chemotherapy dose-intensity
Tumour factors: axial / pelvic location limits resectability
Histology: high grade at presentation in the majority
Biology: p53-driven, often chemo-resistant
Stage: lung metastases common at diagnosis
Classification and Types
Classification by Histology
- Frequency
- 50-60 percent (most common)
- Behaviour
- Aggressive, osteoid producing, lung mets
- Treatment
- Wide resection + multi-agent chemo
- Frequency
- 20-25 percent
- Behaviour
- Spindle cell, lytic, soft tissue mass
- Treatment
- Wide resection +/- radiotherapy
- Frequency
- 10-15 percent
- Behaviour
- Cartilaginous matrix, may dedifferentiate
- Treatment
- Wide resection (chemo less effective)
- Frequency
- less than 10 percent
- Behaviour
- Variable
- Treatment
- Subtype-specific protocols
Osteosarcoma dominates; the histological subtype drives chemotherapy sensitivity, with chondrosarcoma being relatively chemo-resistant.
Unlike primary osteosarcoma, which is almost always a solitary lesion, Paget sarcoma can be multicentric (synchronous in more than one pagetoid bone) - because every bone affected by long-standing Paget carries the same malignant potential. This is a recognised and testable distinction.
- Staging implication: a whole-body bone scan or PET is not just for lung-met-related skip lesions - it is needed to detect a second synchronous sarcoma in another Paget site, which completely changes prognosis and resectability.
- Don't assume solitary: a new aggressive lesion in one Paget bone should prompt scrutiny of every other involved bone; a second focus of intense, destructive uptake (often with a photopenic centre, distinct from the diffuse uptake of active Paget) is suspicious.
- Prognosis: multicentric Paget sarcoma behaves as disseminated high-grade disease and is generally treated palliatively.
Exam point: "How is Paget sarcoma staged differently from a teenager's primary osteosarcoma?" - the answer includes that Paget sarcoma may be multifocal, so you image the entire skeleton, not just the symptomatic bone and the chest.
Clinical Assessment
- Background: known Paget disease (often polyostotic, many years)
- Change in pain: NEW onset, ESCALATING or NIGHT pain in a known Paget site
- Constitutional: weight loss, fatigue (suggests high-grade malignancy)
- Functional: limp, reduced range, inability to weight-bear
- Fracture: pathological fracture after minimal trauma
- Inspect: deformity of Paget bone, NEW swelling, asymmetry
- Palpate: HARD, often FIXED mass; warm overlying skin
- Move: restricted range, pain at end-range
- Neurovascular: rule out nerve or vessel compromise (especially pelvic lesions)
- Systemic: lymphadenopathy (rare), chest signs if lung mets
New constant pain in a known Paget bone PLUS a palpable mass PLUS a rising ALP = malignancy until proven otherwise. Arrange urgent MRI of the painful segment, CT chest and referral to a musculoskeletal tumour service. Do NOT start bisphosphonates empirically and do NOT reassure - the earlier Paget sarcoma is biopsied and treated, the better the chance of cure.
- Discriminating features
- Constant pain, mass, pathological fracture
- Imaging clue
- Cortical destruction, soft tissue mass
- Key test
- Core needle biopsy via tumour service
- Discriminating features
- Pain, lytic lesion, usually epiphyseal
- Imaging clue
- Well-defined lytic lesion, no soft tissue mass
- Key test
- Curettage / histology; often benign
- Discriminating features
- Known primary, weight loss, multiple lesions
- Imaging clue
- Multiple lytic / blastic lesions
- Key test
- Whole-body staging, biopsy of accessible site
- Discriminating features
- Acute pain after fall, deformity, no mass
- Imaging clue
- Fracture line through pagetoid trabeculae
- Key test
- MRI to exclude underlying sarcoma
- Discriminating features
- Fever, raised inflammatory markers
- Imaging clue
- Periosteal reaction, sinus tract, soft tissue oedema
- Key test
- Aspiration, blood cultures, biopsy
A giant cell tumour arising in a bone affected by Paget disease is a SEPARATE, usually benign entity. It is histologically identical to conventional GCT but the patient is older (50-70), the Paget involvement is often polyostotic, and the lesion is most often in the skull, facial bones, pelvis or spine. Do not call every Paget-associated bone tumour "sarcoma" - GCT in Paget is curetted, not widely resected.
Investigations

Imaging and Staging Protocol
Views: AP and lateral of the painful segment, including the whole bone plus the joint above and below
Look for: cortical destruction, periosteal reaction, soft tissue mass, pathological fracture
Comparison with prior films: any change in the Paget appearance is suspicious
Indication: every suspected Paget sarcoma
Findings: marrow oedema beyond expected Paget, soft tissue mass, neurovascular involvement
Sequences: T1, STIR, post-contrast T1 fat-sat; include skip lesions
Indication: better cortical detail than MRI, surgical planning
Findings: cortical breakthrough, fracture lines, matrix mineralisation
Use: biopsy trajectory planning and endoprosthetic sizing
CT chest: lungs are the FIRST site of metastasis in osteosarcoma
Bone scan / PET: identify other Paget-involved bones and any skip lesions
Baseline: provides a comparator for post-treatment surveillance
Who: musculoskeletal radiologist or surgeon from the tumour centre
Where: via a planned tract that will be excised at definitive surgery
How many cores: at least 3-4 cores from the SOLID, VIABLE part of the tumour
Avoid: contaminating uninvolved compartments; draining haematoma away from the resection bed
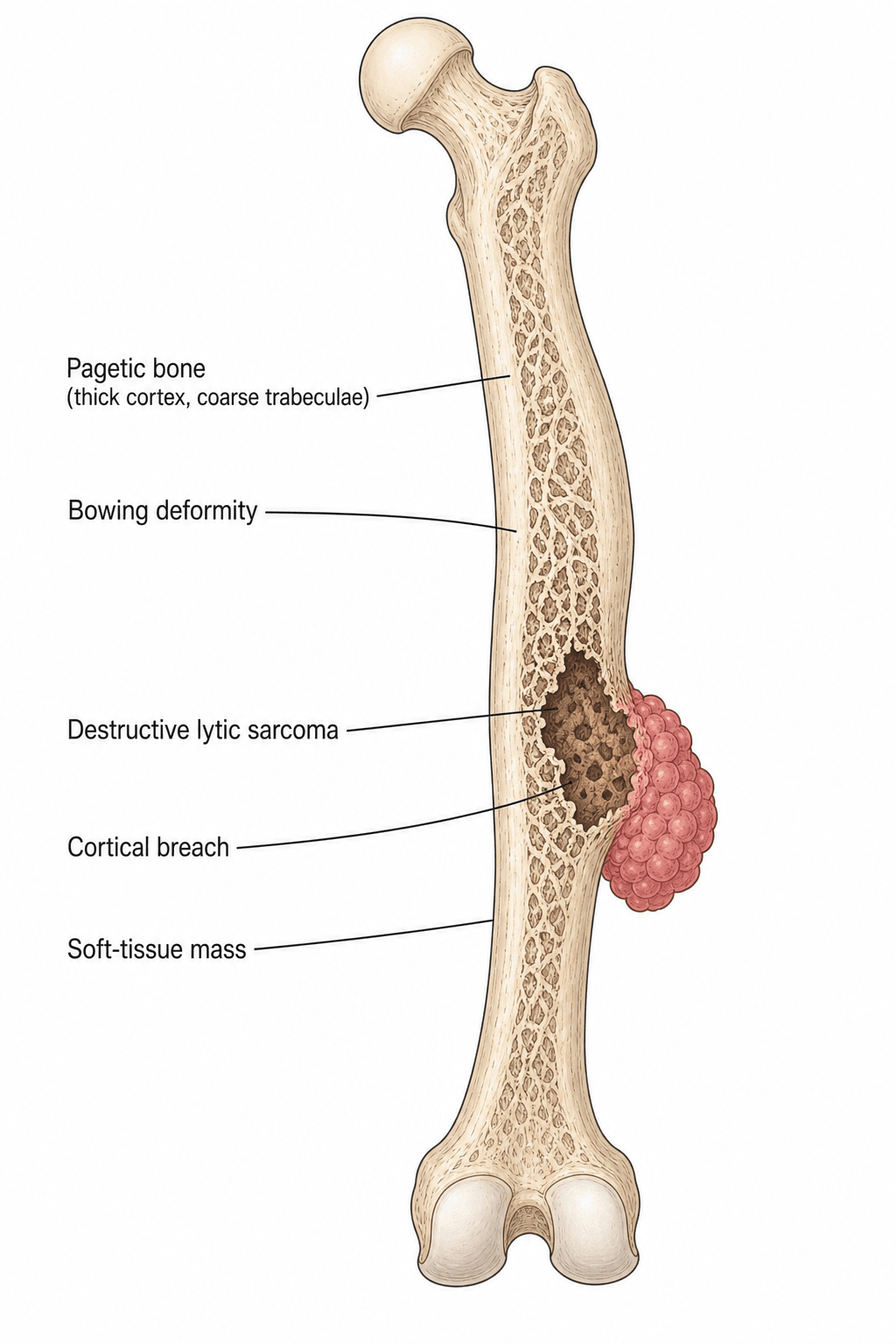
Paget disease on X-ray shows a coarsened trabecular pattern, cortical thickening and bone enlargement. Paget SARCOMA on X-ray shows a DESTRUCTIVE pattern - cortical lysis, a soft tissue mass, or pathological fracture superimposed on the pagetoid bone. Compare with prior films - any NEW finding within a Paget bone is malignant until proven otherwise.
- Paget disease alone
- Coarsened trabeculae, cortical thickening, enlargement
- Paget sarcoma
- Cortical lysis, soft tissue mass, fracture
- Comment
- Most useful single sign is a new finding
- Paget disease alone
- Marrow oedema in active Paget, no soft tissue mass
- Paget sarcoma
- Soft tissue mass, neurovascular involvement
- Comment
- Best modality for local staging
- Paget disease alone
- Increased uptake in active Paget segments
- Paget sarcoma
- New focus of INTENSE uptake, often with photopenic centre
- Comment
- Useful for skip lesions and other Paget sites
- Paget disease alone
- Mild to moderate uptake in active Paget
- Paget sarcoma
- Markedly increased FDG avidity (SUV greater than 5)
- Comment
- Helps pick biopsy target and stage disease
- Paget disease alone
- Often elevated (reflects Paget activity)
- Paget sarcoma
- Sustained rise above patient's own baseline
- Comment
- Trend over months is more useful than single value
- Paget disease alone
- Usually normal
- Paget sarcoma
- Hypercalcaemia uncommon (unlike myeloma / mets)
- Comment
- If raised, look for immobility or concurrent pathology
BIOPSYPaget Sarcoma Workup
Hook:Never incise or biopsy first - full imaging and a planned BIOPSY through the future resection tract is non-negotiable.
Management Algorithm
Resectable Limb Lesion (Proximal Femur / Humerus / Tibia)
Goal: Wide (R0) surgical resection with limb-sparing reconstruction when oncologically safe, combined with multi-agent chemotherapy for osteosarcoma subtype.
Treatment Protocol
Confirm: histology, imaging, fitness for chemotherapy
Members: sarcoma surgeon, medical oncologist, radiologist, pathologist, specialist nurse
Document: planned surgical margins, reconstruction, neoadjuvant / adjuvant chemo
Regimens: cisplatin / doxorubicin / high-dose methotrexate (varies by centre)
Aim: downstage tumour, treat micrometastatic disease, assess response histologically
Caveat: elderly patients often tolerate dose-reduced regimens poorly
Aim: WIDE (R0) margins with the biopsy tract EN-BLOC
Reconstruction: endoprosthetic replacement, allograft-prosthetic composite, or amputation if required
Bone quality: pagetoid bone is porotic and sclerotic - fixation is challenging
Adjuvant chemo: complete the planned osteosarcoma regimen if tolerated
Radiotherapy: consider for positive or close margins, or unresectable disease
Bisphosphonate / denosumab: control ongoing Paget activity in other sites
Chest CT: every 3 months for 2 years, then 6-monthly
Local imaging: MRI of the surgical bed at 3, 6, 12 months then as indicated
Functional: physiotherapy, prosthesis refinement
Limb-sparing surgery is achievable in the majority of appendicular Paget sarcomas but requires wide margins and PROPER handling of pagetoid bone (porotic, sclerotic, deformed). Plan endoprosthetic reconstruction around the abnormal anatomy, not around a "normal" template. Amputation is reserved for neurovascular involvement, fungation, or unreconstructable bone loss.
Complications
- Incidence
- 30-50 percent within 2 years
- Risk Factors
- High grade, axial site, large tumour
- Management
- Pulmonary metastasectomy if resectable; otherwise palliative chemo
- Incidence
- 20-40 percent (higher axial)
- Risk Factors
- Positive margins, extracompartmental disease
- Management
- Re-resection or radiotherapy for palliation
- Incidence
- 15-25 percent at presentation
- Risk Factors
- Lytic destruction, proximal femur / humerus
- Management
- Stabilise before chemo; definitive fixation at resection
- Incidence
- 10-20 percent at 5 years
- Risk Factors
- Paget bone quality, age, weight
- Management
- Revision arthroplasty
- Incidence
- Common in elderly
- Risk Factors
- Renal (methotrexate), cardiac (doxorubicin), marrow
- Management
- Dose reduction, growth factor support
- Incidence
- Common
- Risk Factors
- Polyostotic Paget, ongoing activity
- Management
- Bisphosphonates (zoledronate) or denosumab
Paget bone is sclerotic, porotic, vascular and deformed. Drilling produces bone that cuts like wet balsa, then streams blood. Screws strip. Plates do not contour. Cement behaves unpredictably. Plan for it: have augmentative fixation strategies ready (intramedullary nails, cemented stems, custom prostheses). Tourniquet time, blood loss and surgical duration are higher than for the same operation in normal bone.
Outcomes and Prognosis
- Treatment
- Wide resection + chemo
- Expected Outcome
- 5-year survival 20-30 percent
- Long-term Function
- Limb preserved in most; functional loss around resection
- Treatment
- Surgery (if feasible) + chemo + RT
- Expected Outcome
- 5-year survival 5-10 percent
- Long-term Function
- Major functional loss; amputation rate 20-30 percent
- Treatment
- Palliative chemo + local control
- Expected Outcome
- Median survival under 12 months
- Long-term Function
- Focus on pain control and quality of life
- Treatment
- Re-resection / radiotherapy
- Expected Outcome
- Median survival 12-18 months
- Long-term Function
- High symptom burden - early palliative care
Better prognosis: appendicular site, small tumour, no pathological fracture, R0 margins, patient able to tolerate full-dose chemotherapy.
Worse prognosis: axial / pelvic site, large size (greater than 8 cm), pathological fracture at presentation, positive margins, lung metastases at diagnosis, poor performance status.
The single biggest adverse factor is AXIAL LOCATION, because resectability and chemotherapy tolerance are both compromised. Patients with a small, peripheral Paget sarcoma diagnosed early have the best chance of cure.
Guidelines, Registries & Global Practice
- Paget disease is most prevalent in British descent populations (UK, Australia, New Zealand, North America) and least common in Scandinavia, Asia and Africa
- Paget sarcoma therefore clusters in the same populations, peaking in the seventh and eighth decades
- Male:female ratio approximately 1.5:1
- Polyostotic Paget carries a higher sarcomatous transformation risk than monostotic
- High-resource: dedicated musculoskeletal tumour centres with MDT, core-needle biopsy, endoprosthetic reconstruction, multi-agent chemotherapy
- Limited-resource: open incisional biopsy by the resecting surgeon, cement-augmented internal fixation for palliation, single-agent chemotherapy or radiotherapy for symptom control
- Universal principle: biopsy is the LAST investigation, not the first; the tract must be planned with the future surgery in mind
- Paget control: zoledronate 5 mg IV annually is the global standard; denosumab is used in refractory or renal-impaired patients
- Diagnosis emphasis
- MDT review, planned core biopsy, MRI + CT chest staging
- Treatment emphasis
- Wide resection + multi-agent chemo (osteosarcoma regimens)
- Prognosis
- 5-year survival 5-25 percent, registry-dependent
- Diagnosis emphasis
- Referral to designated sarcoma centre before any intervention
- Treatment emphasis
- Surgery in specialist centre, chemo on case-by-case basis
- Prognosis
- Outcomes audited by NHS sarcoma database
- Diagnosis emphasis
- Compare with prior films, MRI whole bone, biopsy by tumour service
- Treatment emphasis
- Limb-sparing when R0 feasible; amputation otherwise
- Prognosis
- Prognosis worse than primary osteosarcoma
- Diagnosis emphasis
- Optimise underlying Paget control with zoledronate
- Treatment emphasis
- Paget control does not prevent sarcoma but reduces fracture risk
- Prognosis
- Advocates research registries for Paget sarcoma
There is no dedicated international Paget sarcoma registry, but Paget cases are captured within national sarcoma registries (NCCN, NHS, SEER). The evidence base for Paget sarcoma is dominated by single-centre retrospective series and histology reviews, with very few prospective trials because the disease is rare. Modern management extrapolates from primary osteosarcoma trials, acknowledging that elderly Paget patients tolerate chemotherapy less well.
Record in every Paget patient with new pain:
- Comparison with prior imaging and ALP trend
- MRI and CT chest performed before biopsy
- Biopsy tract documented on a diagram in the notes
- MDT outcome communicated in writing to the patient and GP
- Prognosis discussed honestly with patient and family
A missed Paget sarcoma - "treated as Paget pain" with a bisphosphonate boost - is a recurring cause of late-stage presentation and complaints worldwide. When in doubt, image the painful segment and refer to the tumour service.
Controversies & Areas of Uncertainty
No high-quality evidence shows that bisphosphonates or denosumab reduce the risk of Paget sarcoma. They control Paget activity (bone turnover, pain, deformity) and reduce fracture risk, but the malignant potential of pagetoid bone is not abolished. The reduction in fracture may even delay detection by making a fracture the presenting sign less common.
Evidence from primary osteosarcoma supports multi-agent chemotherapy in patients able to tolerate it. In Paget sarcoma, the decision is individualised by age, comorbidity, histology and patient preference. Some centres offer dose-modified regimens or single-agent doxorubicin in older patients; others reserve chemo for osteosarcoma subtype only.
Wide (R0) margins are the surgical goal, but Paget bone is poorly defined macroscopically, so margins are technically harder to achieve. Amputation rates in pelvic Paget sarcoma exceed 20 percent. Functional outcomes after limb-sparing surgery are often comparable to amputation in the long term, but immediate morbidity differs.
SQSTM1/p62 and NF-kB pathway biology is under investigation as a targetable driver. Trials of denosumab, immune checkpoint inhibitors and SQSTM1-directed agents are early-phase. Until results are available, multimodal surgery and chemotherapy remain the standard of care.
MCQ Practice Points
Q: What is the approximate lifetime risk of sarcomatous transformation in a patient with Paget disease of bone? A: Less than 1 percent in modern cohorts (older literature quoted 5-10 percent, but contemporary series are lower). The risk is higher in polyostotic Paget and in those with a family history. The ABSOLUTE number of cases remains clinically meaningful because Paget is common in older adults.
Q: What is the most common histological subtype of Paget sarcoma? A: Osteosarcoma, accounting for 50-60 percent. The remainder are mostly fibrosarcoma / malignant fibrous histiocytoma and chondrosarcoma. The histological subtype matters for chemotherapy sensitivity - osteosarcoma is the most chemo-sensitive, chondrosarcoma the least.
Q: What clinical pattern should make you suspect malignant transformation in a Paget bone? A: A change in pain character - new onset, escalating or constant pain, night pain - in a bone with known Paget disease, especially when accompanied by a palpable mass or pathological fracture. A rising ALP above the patient's own baseline is supportive but not specific.
Q: Why must biopsy be the last investigation in a suspected Paget sarcoma? A: Because the biopsy tract must lie within the planned surgical resection corridor. An improperly placed biopsy contaminates uninvolved compartments and can convert a limb-sparing operation into an amputation. Biopsy should be performed by the musculoskeletal tumour service that will do the definitive surgery.
Q: What is the cornerstone of treatment for resectable Paget sarcoma? A: Wide (R0) surgical resection combined with multi-agent chemotherapy for osteosarcoma subtype. Limb-sparing surgery is preferred when oncologically safe; amputation is reserved for neurovascular involvement or unreconstructable bone loss. Radiotherapy is added for positive margins or unresectable disease.
Q: Why is the prognosis of Paget sarcoma worse than primary osteosarcoma? A: Patient age (60-70 years) limits chemotherapy dose-intensity, axial sites (pelvis, sacrum) are commonly involved and difficult to resect, lung metastases are common at presentation, and the underlying biology (p53-driven) is often chemo-resistant. Five-year overall survival is 5-25 percent compared with greater than 60 percent for primary extremity osteosarcoma in adolescents.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 72-year-old man with known polyostotic Paget disease of the pelvis and proximal femur presents with 6 weeks of escalating pain in the right ilium, waking him at night. On examination there is a firm, fixed mass over the right iliac fossa. His ALP has risen from a stable baseline of 450 to 980 U/L. X-ray shows cortical destruction and a soft tissue mass arising from the ilium. How would you manage this?”
“A 68-year-old woman with known Paget disease of the proximal femur presents with acute pain in the right hip after tripping on a rug. X-ray shows a pathological fracture through a lytic lesion in the subtrochanteric femur. There is no prior imaging for comparison. How do you proceed?”
Definition and Risk
- Paget sarcoma = high-grade bone sarcoma arising in a bone affected by Paget disease
- Lifetime risk less than 1 percent in modern cohorts (older 5-10 percent estimates are too high)
- Risk rises with polyostotic Paget, family history, and duration of disease activity
- Median age 60-70 years, slight male predominance
Pathology
- Osteosarcoma accounts for 50-60 percent - the dominant subtype
- Fibrosarcoma / MFH and chondrosarcoma account for most of the remainder
- SQSTM1/p62 mutation drives Paget; p53 loss is enriched in Paget sarcoma
- Biology is high-grade, often chemo-resistant, lung-seeking
Sites and Presentation
- Pelvis, proximal femur, proximal humerus - the most common Paget sites
- Pelvic and sacral lesions have the worst prognosis because of resectability
- New constant pain, night pain, palpable mass or pathological fracture are the red flags
- Rising ALP above the patient's own baseline is supportive but not specific
Imaging and Staging
- Plain X-ray of the painful segment plus the joint above and below - compare with priors
- MRI of the WHOLE bone for local staging and soft tissue extent
- CT chest for lung metastases (most common distant site)
- Bone scan or PET to identify other Paget-involved bones and skip lesions
Biopsy Rules
- Biopsy is the LAST investigation, not the first - image first
- Core needle biopsy by the musculoskeletal tumour service
- Biopsy tract placed along the planned future resection corridor
- Multiple cores from the SOLID, VIABLE part of the tumour - 3-4 cores minimum
Treatment
- Resectable appendicular disease: wide R0 resection + multi-agent chemo (osteosarcoma regimens)
- Pelvic / axial disease: combined surgery + chemo + radiotherapy, often unresectable
- Unresectable / metastatic: palliative chemo, radiotherapy, surgical stabilisation
- Paget activity elsewhere: control with zoledronate or denosumab
Prognosis
- 5-year overall survival 5-25 percent - markedly worse than primary osteosarcoma
- Median survival under 12 months in metastatic disease
- Single biggest adverse factor: axial / pelvic location
- Lung metastases at presentation in 10-25 percent
Avoid the Traps
- Treating new pain in a Paget bone as Paget pain without imaging - the commonest error
- Biopsy through a tract that contaminates uninvolved compartments
- Internal fixation of a pathological fracture through a Paget bone before excluding malignancy
- Underestimating blood loss and technical difficulty in pagetoid bone
Evidence Base and Key Trials
Osteogenic sarcoma associated with Paget's disease of bone. A clinicopathologic study of 65 patients
- Landmark large series of 65 patients defining the histological spectrum of Paget sarcoma
- Osteosarcoma was the dominant subtype, followed by fibrosarcoma and malignant fibrous histiocytoma
- Pelvis, femur and humerus were the most common sites because they are the most common Paget sites
- Survival was markedly worse than for primary osteosarcoma in younger patients
Osteosarcoma in Paget's disease of bone
- Review of the molecular pathogenesis of Paget sarcoma
- SQSTM1/p62 mutations are common in familial and sporadic Paget disease
- p62 / sequestosome-1 activates NF-kB signalling, driving osteoclast activity
- p53 mutations are enriched in Paget sarcoma compared with Paget disease alone - a stepwise model: SQSTM1 driver, p53 second hit for malignant transformation
Paget's osteosarcoma and post-radiation osteosarcoma: secondary osteosarcoma at Middlemore Hospital, New Zealand
- Single-institution series of secondary osteosarcoma including Paget osteosarcoma and post-radiation osteosarcoma
- Paget osteosarcoma presents at significantly older age than primary osteosarcoma and is overwhelmingly axial/pelvic
- Wide surgical margins were achievable in appendicular cases but pelvic lesions had high positive-margin rates
- Outcome is markedly worse than primary osteosarcoma - confirming the high-grade biology of Paget sarcoma
Osteosarcoma in patients older than 65 years
- Multi-institutional study of osteosarcoma in patients over 65 years, the typical age band for Paget sarcoma
- Secondary osteosarcoma (Paget, post-radiation) forms a major subgroup in this age range
- Limb-sparing surgery was feasible in the majority but complication rates were higher than in adolescent primary osteosarcoma
- Five-year survival was markedly lower than primary osteosarcoma in adolescents - reflecting older age, axial location and biology
From the archives of the AFIP. Radiologic spectrum of Paget disease of bone and its complications with pathologic correlation
- Radiology review of the imaging hallmarks of Paget disease and its complications, including sarcomatous transformation
- Cortical destruction, soft tissue mass, pathological fracture and new bone formation are the cardinal signs of malignant change
- Comparison with prior imaging is the single most useful diagnostic manoeuvre
- MRI is best for soft tissue extent; CT is best for cortical detail and matrix