Paraspinal Abscess
Visual One-Pager
Purulent collection in paraspinal muscle - diagnosis, source control and antibiotics
Paraspinal abscesses are collections of purulent material within the paraspinal musculature, distinct from epidural abscesses. They require high clinical suspicion, prompt imaging diagnosis, and appropriate antimicrobial therapy with or without surgical drainage. The condition can be primary (hematogenous) or secondary (direct extension from vertebral osteomyelitis, discitis, or epidural abscess).
Key Recognition Features:
- Back pain with fever and elevated inflammatory markers
- Paravertebral muscle swelling and tenderness
- MRI showing rim-enhancing fluid collection in paraspinal muscles
- May coexist with vertebral osteomyelitis or epidural abscess
Critical Management Pathway:
- Blood cultures and inflammatory markers (CRP, ESR, WCC)
- Urgent contrast-enhanced MRI whole spine
- CT-guided aspiration for culture and sensitivities
- Empiric broad-spectrum antibiotics (adjust per culture)
- Surgical drainage if failed medical therapy or neurological deficit
High-Yield Exam Points:
- Staphylococcus aureus most common organism (60-70% cases)
- MRI with gadolinium contrast is gold standard imaging
- Indications for surgery: failed medical therapy, neurological deficit, large abscess greater than 3 cm, coexisting epidural abscess requiring decompression
- Duration of antibiotics typically 6-12 weeks IV then oral
Anatomy & Pathophysiology
Paraspinal Muscle Anatomy
The paraspinal compartment contains multiple muscle layers susceptible to abscess formation:
Superficial Layer:
- Trapezius and latissimus dorsi
- Relatively resistant to deep infection
Intermediate Layer:
- Erector spinae group (iliocostalis, longissimus, spinalis)
- Most common site for abscess formation
- Supplied by posterior branches of spinal arteries
Deep Layer:
- Multifidus, rotatores, interspinales, intertransversarii
- Close proximity to neural foramina and epidural space
- Direct communication pathway for infection spread
Fascial Compartments:
- Thoracolumbar fascia creates potential spaces
- Infection can track longitudinally within fascial planes
- May extend from cervical to lumbar regions
Pathogenesis Mechanisms
Paraspinal abscesses arise by three principal routes: direct extension from vertebral osteomyelitis or discitis (the commonest, roughly 50-60%), haematogenous seeding of muscle from a distant focus (30-40%), and iatrogenic or penetrating inoculation (facet/epidural injections, surgery, trauma). The rich segmental vascular supply of the erector spinae makes it the most frequently involved muscle group, and the continuity of fascial planes allows longitudinal tracking across several spinal levels.
High Yield
At a Glance
Paraspinal abscesses are purulent collections within paraspinal musculature, most commonly from direct extension from vertebral osteomyelitis/discitis (50-60%) or haematogenous seeding (30-40%). Staphylococcus aureus is the causative organism in 60-70% of cases (MRSA increasing). MRI with gadolinium is the gold standard, showing rim-enhancing fluid collection. Initial management includes blood cultures, CT-guided aspiration for culture, and empiric broad-spectrum antibiotics (6-12 weeks IV then oral). Surgical drainage is indicated for failed medical therapy, neurological deficit, abscess greater than 3cm, or coexisting epidural abscess requiring decompression.
SPREADSPREAD Mechanism of Paraspinal Infection
| S | Seeding (hematogenous) Bacteremia from distant source (skin, urinary, respiratory) |
| P | Procedural (iatrogenic) Post-injection, post-surgical, post-epidural |
| R | Retrograde (extension) Direct spread from vertebral osteomyelitis or discitis |
| E | Epidural communication Extension from epidural abscess via neural foramina |
| A | Adjacent organ Spread from psoas abscess, renal infection, or retroperitoneal source |
| D | Direct trauma Penetrating injury or contiguous soft tissue infection |
| S | Seeding (hematogenous) Bacteremia from distant source (skin, urinary, respiratory) | R | Retrograde (extension) Direct spread from vertebral osteomyelitis or discitis | A | Adjacent organ Spread from psoas abscess, renal infection, or retroperitoneal source |
| P | Procedural (iatrogenic) Post-injection, post-surgical, post-epidural | E | Epidural communication Extension from epidural abscess via neural foramina | D | Direct trauma Penetrating injury or contiguous soft tissue infection |
Hook:Infection SPREADS through multiple pathways to reach paraspinal muscles
Hematogenous Seeding:
- Accounts for 30-40% of primary paraspinal abscesses
- Bacteremia leads to muscle microabscess formation
- Rich vascular supply facilitates bacterial deposition
- Common sources: skin infections, endocarditis, IV drug use
Direct Extension:
- Most common pathway (50-60% of cases)
- Vertebral osteomyelitis with posterior extension
- Discitis with paravertebral phlegmon progression
- Epidural abscess breakthrough via neural foramina
Iatrogenic Causes:
- Facet joint injections
- Medial branch blocks
- Trigger point injections
- Spine surgery with inadequate debridement
Microbiology
Staphylococcus aureus (60-70%):
- Most common pathogen overall
- MRSA increasing in prevalence (20-40% of S. aureus)
- Forms biofilm and tissue destruction
- Toxin production enhances virulence
Mycobacterium tuberculosis (10-20%):
- Higher prevalence in endemic regions
- Cold abscess formation (less acute inflammation)
- Granulomatous inflammation
- Requires extended treatment duration (9-12 months)
Gram-negative organisms (10-15%):
- E. coli, Pseudomonas, Klebsiella
- Associated with urinary source
- Elderly and immunocompromised patients
- Often polymicrobial
Streptococcus species (5-10%):
- Group A and B Streptococcus
- May follow pharyngitis or skin infection
- Generally more antibiotic sensitive
Anaerobes (rare):
- Bacteroides, Peptostreptococcus
- Associated with GI source or polymicrobial infection
- Foul-smelling purulent material
Clinical Presentation
Classic Presentation Triad
Back Pain (98% of cases):
- Localized to affected spinal level
- Constant, progressive intensity
- Worse with movement and axial loading
- Night pain disrupting sleep
- May radiate to flank or lower limbs
Fever (70-85% of cases):
- Temperature greater than 38.0 degrees Celsius
- May be absent in immunocompromised
- Rigors suggest bacteremia
- Low-grade fever common in chronic abscess
Inflammatory Response (95% of cases):
- Elevated CRP (often greater than 100 mg/L)
- Elevated ESR (often greater than 50 mm/hr)
- Leukocytosis (WCC greater than 11,000/µL)
- Procalcitonin elevated in bacterial infection
Physical Examination Findings
Inspection:
- Paravertebral muscle swelling or fullness
- Erythema over affected area (variable)
- Loss of normal spinal contour
- Antalgic posture or gait
- Surgical scars (if post-operative)
Palpation:
- Exquisite tenderness over paraspinal muscles
- Palpable fluctuance (large superficial abscess)
- Warmth compared to contralateral side
- Muscle spasm and guarding
- Percussion tenderness over spinous processes
Range of Motion:
- Restricted spinal flexion, extension, and rotation
- Patient resists active and passive movement
- Splinting and protective muscle spasm
Neurological Assessment:
- Usually neurologically intact (key distinction from epidural abscess)
- May have radicular pain if foraminal compression
- Lower limb weakness suggests epidural extension
- Sphincter dysfunction rare unless epidural involvement
Red Flag Features
Indicating Epidural Extension:
- Progressive neurological deficit
- Bilateral radicular symptoms
- Bladder or bowel dysfunction
- Saddle anaesthesia
- Upper motor neuron signs
Indicating Sepsis:
- Hemodynamic instability
- Tachycardia greater than 100 bpm
- Hypotension (systolic less than 90 mmHg)
- Altered mental status
- Oliguria
Indicating Vertebral Osteomyelitis:
- Severe vertebral body tenderness
- Kyphotic deformity
- Mechanical instability pain pattern
Investigations
Laboratory Studies
Imaging Studies
Plain Radiographs (limited utility):
- May show paravertebral soft tissue shadow
- Vertebral endplate erosion if osteomyelitis present
- Loss of disc height in discitis
- Useful to exclude fracture or deformity
- Not adequate to diagnose or exclude abscess
MRI with Gadolinium Contrast (Gold Standard):
- Sensitivity 95%, specificity 92% for paraspinal abscess
- T1-weighted: hypointense to muscle
- T2-weighted: hyperintense fluid signal
- Post-contrast T1 with fat saturation: rim enhancement
- STIR sequences: high signal inflammation and edema
MRI Key Diagnostic Features:
- Well-defined fluid collection within paraspinal muscles
- Peripheral rim enhancement (abscess capsule)
- Central non-enhancing purulent material
- Surrounding muscle edema and enhancement
- Assessment of epidural space for extension
CT with Contrast:
- Alternative if MRI contraindicated
- Hypodense fluid collection with rim enhancement
- Better definition of bony anatomy
- Useful for CT-guided aspiration planning
- Lower soft tissue resolution than MRI
Ultrasound:
- Operator-dependent modality
- Useful for superficial abscess detection
- Can guide needle aspiration
- Limited in obese patients or deep abscess
- Real-time imaging for drainage procedures
Tissue Diagnosis
CT-Guided Aspiration:
- Diagnostic yield 70-85% for organism identification
- Obtain before antibiotic initiation when possible
- Send for Gram stain, culture, AFB, fungal studies
- Minimum 5 mL purulent material preferred
- Simultaneous therapeutic drainage possible
Indications for Aspiration:
- Uncertain diagnosis
- Negative blood cultures
- Need for organism-specific therapy
- Large abscess amenable to drainage
- Treatment failure on empiric antibiotics
Open Surgical Biopsy:
- Reserved for failed percutaneous attempts
- When operative drainage planned
- Tissue sample superior to fluid aspirate
- Multiple samples from abscess wall and contents
- Fresh tissue for microbiological analysis
Differential Diagnosis
Paraspinal Abscess vs Key Differentials
| Feature | Paraspinal Abscess | Epidural Abscess | Vertebral Osteomyelitis | Muscle Hematoma |
|---|
Other Differential Diagnoses:
Psoas Abscess:
- Located in iliopsoas muscle
- Hip flexion contracture and positive iliopsoas sign
- May extend to lumbar paraspinal region
- Often associated with vertebral osteomyelitis or GI source
Malignancy:
- Metastatic disease to paraspinal muscles
- Primary sarcoma (rare)
- Less acute presentation
- MRI shows mass effect without rim enhancement
Inflammatory Myositis:
- Autoimmune etiology
- Bilateral symmetric involvement
- Muscle enzyme elevation (CK, aldolase)
- Muscle biopsy shows inflammatory cells without infection
Management
Conservative (Medical) Management
COMBATCOMBAT Strategy for Initial Antibiotic Therapy
| C | Cultures first Blood cultures before antibiotics; CT aspiration if possible |
| O | Organism coverage Empiric therapy covers Staph aureus, Gram-negatives |
| M | MRSA consideration Vancomycin if risk factors or high local prevalence |
| B | Broad spectrum initial Combination therapy until cultures available |
| A | Adjust to culture De-escalate based on sensitivities |
| T | Total duration 6-12 weeks IV 4-6 weeks then oral based on response |
| C | Cultures first Blood cultures before antibiotics; CT aspiration if possible | M | MRSA consideration Vancomycin if risk factors or high local prevalence | A | Adjust to culture De-escalate based on sensitivities |
| O | Organism coverage Empiric therapy covers Staph aureus, Gram-negatives | B | Broad spectrum initial Combination therapy until cultures available | T | Total duration 6-12 weeks IV 4-6 weeks then oral based on response |
Hook:COMBAT the infection with strategic antibiotic therapy
Empiric Antibiotic Regimens (representative; always follow local antibiogram and microbiology advice):
Standard Regimen (no MRSA risk):
- Anti-staphylococcal beta-lactam: flucloxacillin (or cefazolin / nafcillin depending on region) 2 g IV 6-hourly PLUS
- Ceftriaxone 2 g IV daily OR gentamicin 4-7 mg/kg IV daily for Gram-negative cover
- Covers MSSA, Streptococcus, Gram-negatives
MRSA Risk Factors Present:
- Vancomycin 25-30 mg/kg IV loading, then 15-20 mg/kg IV 12-hourly (adjust to trough) PLUS
- Ceftriaxone 2 g IV daily
- MRSA risk factors: previous MRSA, IV drug use, recent hospitalization, nursing home resident
Penicillin Allergy:
- Vancomycin (as above) PLUS
- Gentamicin 4-7 mg/kg IV daily OR ciprofloxacin 400 mg IV 12-hourly
Duration of Therapy (evidence-based):
- Default 6 weeks for uncomplicated pyogenic infection (Bernard non-inferiority RCT showed 6 weeks equals 12 weeks)
- Early oral switch is acceptable once a suitable bioavailable agent and source control are confirmed (OVIVA trial: oral non-inferior to IV)
- Extend to 12 weeks (or longer) only for specific indications: undrained collection, endocarditis, retained implant, difficult-to-treat organism, or extensive osteomyelitis
- Tuberculous infection requires prolonged anti-tuberculous therapy (typically 9-12 months)
- Oral options once sensitivities known: anti-staphylococcal beta-lactam, first-generation cephalosporin, clindamycin, or a fluoroquinolone plus rifampicin per local guidance
Indications for Surgical Intervention
Absolute Indications:
- Progressive neurological deficit
- Spinal cord compression (coexisting epidural abscess)
- Septic shock despite medical therapy
- Spinal instability requiring stabilization
Relative Indications:
- Abscess greater than 3 cm diameter
- Failed medical therapy (persistent fever, rising CRP after 3-5 days)
- Inability to obtain microbiological diagnosis
- Coexisting vertebral osteomyelitis requiring debridement
- Immunocompromised host with large abscess
Conservative Management Criteria:
- Abscess less than 3 cm
- No neurological deficit
- Hemodynamically stable
- Microbiological diagnosis obtained (blood culture or aspiration)
- Improving inflammatory markers on antibiotics
Surgical Techniques
Monitoring and Follow-Up
Inpatient Phase:
- Daily temperature and inflammatory markers
- CRP and ESR every 3-4 days
- Weekly full blood count
- Antibiotic levels (vancomycin, gentamicin)
- Neurological examination daily
Response to Treatment Criteria:
- Afebrile by day 5-7
- CRP declining (expect 50% reduction by week 2)
- Clinical improvement (pain reduction, mobility)
- No new neurological deficit
Outpatient Follow-Up:
- Weekly review first 4 weeks
- CRP and ESR monitoring
- Ensure antibiotic compliance
- Assess for recurrence or complications
- Repeat MRI at 6-8 weeks to confirm resolution
Complications
RELAPSERELAPSE Complications of Paraspinal Abscess
| R | Recurrence Inadequate drainage or antibiotic duration |
| E | Epidural extension Spread to epidural space causing cord compression |
| L | Longitudinal spread Tracking along fascial planes to adjacent levels |
| A | Antibiotic resistance MRSA, VRE, or multi-drug resistant organisms |
| P | Psoas involvement Extension to iliopsoas with hip flexion contracture |
| S | Sepsis Systemic inflammatory response and organ dysfunction |
| E | Epidural scarring Chronic pain and neurological symptoms |
| R | Recurrence Inadequate drainage or antibiotic duration | A | Antibiotic resistance MRSA, VRE, or multi-drug resistant organisms | E | Epidural scarring Chronic pain and neurological symptoms |
| E | Epidural extension Spread to epidural space causing cord compression | P | Psoas involvement Extension to iliopsoas with hip flexion contracture | ||
| L | Longitudinal spread Tracking along fascial planes to adjacent levels | S | Sepsis Systemic inflammatory response and organ dysfunction |
Hook:Don't let the patient RELAPSE with inadequate treatment
Early Complications (less than 4 weeks):
Sepsis and Septic Shock:
- Incidence: 10-15% of cases
- Risk factors: delayed diagnosis, MRSA, immunocompromise
- Management: ICU admission, vasopressor support, source control
- Mortality: 5-10% if septic shock develops
Epidural Abscess Extension:
- Occurs in 20-30% of paraspinal abscesses
- Presents with progressive neurological deficit
- Requires emergency surgical decompression
- Associated with worse neurological outcomes
Vertebral Osteomyelitis:
- Coexistent in 40-50% of cases
- May lead to vertebral collapse and instability
- Requires longer antibiotic duration (12 weeks)
- May need staged anterior reconstruction
Late Complications (greater than 4 weeks):
Recurrence:
- Incidence: 5-10% of treated cases
- Risk factors: inadequate drainage, short antibiotic course, immunosuppression
- Presents with recurrent pain and fever
- Requires repeat imaging and extended antibiotics or surgery
Chronic Pain:
- Incidence: 20-30%
- Mechanisms: muscle fibrosis, epidural scarring, facet joint arthropathy
- Management: multimodal analgesia, physiotherapy, pain clinic referral
Spinal Deformity:
- Kyphotic deformity if vertebral collapse
- Scoliosis from asymmetric muscle scarring
- May require corrective fusion surgery
Evidence-Based Management
Image-Guided Percutaneous Drainage of Deep Muscle Abscess
- Catheter insertion technically successful in all patients
- Muscular component successfully drained in 82% overall (85% muscle-only vs 77% with adjacent skeletal involvement)
- Catheter drainage plus antibiotics avoided any surgery in 65.6% of patients
- Adjacent skeletal (bone or joint) infection was the strongest predictor of drain failure (p=0.0001)
6 vs 12 Weeks of Antibiotics (DTS / Bernard RCT)
- Clinical cure at 1 year: 90.9% (6 weeks) vs 90.9% (12 weeks) - identical
- Difference 0.05% (95% CI -6.2 to 6.3), within the 10% margin: 6 weeks non-inferior
- Adverse events comparable between arms (50 vs 51 patients)
- Supports a default 6-week course for uncomplicated pyogenic spondylodiscitis
Oral vs IV Antibiotics for Bone and Joint Infection (OVIVA)
- Definitive treatment failure at 1 year: 14.6% IV vs 13.2% oral
- Oral therapy non-inferior to IV (within 7.5 percentage-point margin)
- Fewer catheter complications and shorter hospital stay in the oral group
- Early oral switch is appropriate once a suitable agent and source control are confirmed
MRI Criteria for Spinal Infection: Rules or Myths
- Paraspinal or epidural inflammation present in 97.7% (highest-sensitivity sign)
- Disc enhancement 95.4% and T2 fluid-equivalent disc signal 93.2% sensitive
- Endplate erosion 84.1% sensitive; reduced disc height only 52.3% and T1 disc hypointensity only 29.5%
- Classic criteria can be absent in atypical presentations
IDSA Guideline: Native Vertebral Osteomyelitis
- MRI is the imaging modality of choice for suspected spinal infection
- Obtain blood cultures and image-guided biopsy/aspirate before empirical antibiotics in the stable patient
- Hold empirical antibiotics in haemodynamically stable patients to maximise microbiological yield
- Monitor response with ESR/CRP; reserve surgery for neurological deficit, instability, or failed medical therapy
Long-Term Outcomes and Relapse Drivers
- Mortality 11%; residual disability in over one-third of survivors
- Relapse occurred in 14% of patients
- Independent risk factors for adverse outcome: neurological compromise, time to diagnosis, hospital-acquired infection
- Paravertebral abscesses, recurrent bacteraemia and chronic draining sinuses were independently associated with relapse
Staphylococcus aureus Spinal Infection: Clinical Features
- Epidural, paraspinous or psoas abscess present on imaging in 60% of patients
- Neurological abnormalities in 48%; methicillin-susceptible S. aureus in 67.5%
- Organism recovered by fine-needle aspiration in 74% and blood cultures in 68%
- IV antibiotics for at least 8 weeks was the only factor associated with cure
Controversies & Areas of Uncertainty
Antibiotic duration and route. The 6-week default (Bernard RCT) and early oral switch (OVIVA) are now well supported for uncomplicated disease, yet many units still default to prolonged IV courses. The evidence applies to uncomplicated pyogenic infection with adequate source control; how far it extends to large undrained paraspinal collections, retained hardware, or endocarditis remains uncertain, and these scenarios still warrant individualised, often longer therapy.
Withholding antibiotics to improve culture yield. Guidelines advise obtaining cultures and an image-guided sample before empirical antibiotics in the haemodynamically stable patient. In practice, clinicians frequently start antibiotics early, lowering microbiological yield. The safe window for delay in a stable patient is not precisely defined, and there is no role for delay in sepsis or progressive neurological deficit.
Size threshold for drainage. A "greater than 3 cm" cut-off for surgery is widely quoted but is a pragmatic convention rather than a validated threshold; decision-making should integrate accessibility, loculation, response to antibiotics, comorbidity and the presence of osteomyelitis rather than size alone.
Percutaneous vs open source control. Image-guided drainage avoids surgery in roughly two-thirds of deep muscle collections, but coexisting bone or joint infection markedly increases drain failure. The optimal sequencing of repeat percutaneous attempts versus early open debridement in this group is not standardised.
Role of biomarkers for stopping therapy. CRP/ESR trends guide response, but neither has a validated stopping threshold; persistent mild elevation does not reliably indicate ongoing active infection, risking unnecessarily prolonged treatment.
Guidelines, Registries & Global Practice
Global Epidemiology
- Pyogenic spinal infection (the usual context for a paraspinal collection) has a rising global incidence, attributed to an ageing population, increasing instrumentation/injection procedures, diabetes, immunosuppression and injecting drug use.
- Staphylococcus aureus is the dominant pathogen worldwide; the proportion that is MRSA varies by region and risk profile.
- Tuberculous (Pott) disease remains a leading cause of paraspinal "cold" abscess in high-burden regions of South Asia, sub-Saharan Africa and parts of East Asia, and must be actively considered in patients from or exposed to these settings.
- Brucella spondylitis is an important regional cause around the Mediterranean, Middle East and Central Asia, often with prominent paravertebral involvement.
Side-by-Side Guidance
| Body | Emphasis | Practical point |
|---|---|---|
| IDSA (US, 2015) | Diagnosis and antimicrobial management of native vertebral osteomyelitis | MRI first-line; cultures/biopsy before antibiotics when stable; ESR/CRP to monitor |
| BOA / UK spinal infection consensus | Multidisciplinary "spinal infection MDT", early MRI, source control | Neurology and instability drive surgical urgency |
| AO Spine | Surgical decision-making, debridement and stabilisation principles | Address instability and deformity alongside infection clearance |
| EFORT / European consensus (SponDT-type evidence) | Duration of therapy | Supports a 6-week default for uncomplicated pyogenic spondylodiscitis |
Where high-quality randomised evidence exists (Bernard 6-vs-12 weeks; OVIVA oral-vs-IV), recommendations converge internationally; remaining differences are largely in empirical regimen choice driven by local resistance patterns.
Registry & Evidence Notes
- There is no dedicated international "paraspinal abscess registry"; the evidence base is built from RCTs (Bernard, OVIVA), large single- and multi-centre cohorts (e.g. McHenry 253-patient series) and society guidelines.
- Implant/instrumentation-related spinal infection data are captured indirectly through national spine surgery and device surveillance datasets rather than a disease-specific registry.
High- vs Limited-Resource Practice Variation
- High-resource settings: rapid contrast MRI, interventional-radiology-led image-guided drainage, therapeutic drug monitoring, early oral switch with outpatient parenteral/oral antibiotic programmes.
- Limited-resource settings: greater reliance on plain radiographs, ultrasound and CT; higher proportion of tuberculous and late-presenting disease; open surgical drainage may be the default source-control option where interventional radiology is unavailable; empirical anti-tuberculous therapy is started earlier where TB is endemic.
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Diabetic Patient with Paraspinal Abscess
""
Scenario 2: Post-Operative Paraspinal Abscess
""
Scenario 3: Chronic Paraspinal/Psoas Cold Abscess
""
Exam Day Cheat Sheet
One-line answer: Paraspinal abscess = back pain + fever + raised CRP with a rim-enhancing paraspinal muscle collection on gadolinium MRI. Confirm with contrast MRI whole spine, secure blood cultures and image-guided aspirate before antibiotics (if stable), give empirical anti-staphylococcal cover, and pursue source control with image-guided drainage; reserve open surgery for neurological deficit, instability, failed drainage, or concomitant osteomyelitis. Default duration is 6 weeks (Bernard RCT) with early oral switch acceptable (OVIVA).
A detailed point-by-point rapid-revision sheet follows at the end of this topic.
MCQ Practice Points
Clinical Pearl
Q: What is the classic presentation of a psoas abscess secondary to spinal tuberculosis?
A: Pott's disease causes cold abscess tracking along psoas muscle presenting as groin/thigh mass or hip flexion contracture. Patient holds hip in flexed, externally rotated position. Psoas sign positive. Associated with thoracolumbar spine TB. Night sweats, weight loss may be present. MRI shows psoas collection with vertebral destruction.
Clinical Pearl
Q: What imaging features distinguish tuberculous from pyogenic spinal infection?
A: TB spine: Multiple level involvement, relative disc preservation initially, large paraspinal abscess, subligamentous spread, anterior vertebral body destruction, gibbus deformity. Pyogenic: Single level, early disc destruction, smaller abscess, endplate erosion. TB abscesses are disproportionately large compared to bone destruction.
Clinical Pearl
Q: What are the indications for surgical drainage of paraspinal abscess?
A: Surgical indications: Neurological deficit, spinal instability, failure of percutaneous drainage, large abscess (greater than 2.5cm), epidural extension with cord compression. CT-guided drainage appropriate for isolated psoas abscess without neurological compromise. Tissue sample essential for culture and histology.
Clinical Pearl
Q: What is the most common organism causing pyogenic paraspinal abscess?
A: Staphylococcus aureus causes 50-70% of pyogenic spinal infections. MRSA increasingly common. Other organisms: Streptococci, gram-negatives (especially with urinary source), Pseudomonas (IVDU). TB in endemic areas. Brucella in appropriate geographic/occupational exposure. Always obtain tissue for culture.
Clinical Pearl
Q: What is the recommended duration of antibiotic therapy for vertebral osteomyelitis with paraspinal abscess?
A: Minimum 6 weeks IV antibiotics for pyogenic vertebral osteomyelitis. Some protocols allow oral switch at 2-3 weeks if responding well (OVIVA trial). TB spine requires 12-18 months of antituberculous therapy. Monitor ESR/CRP for response. Longer treatment for immunocompromised or retained instrumentation.
Management Algorithm
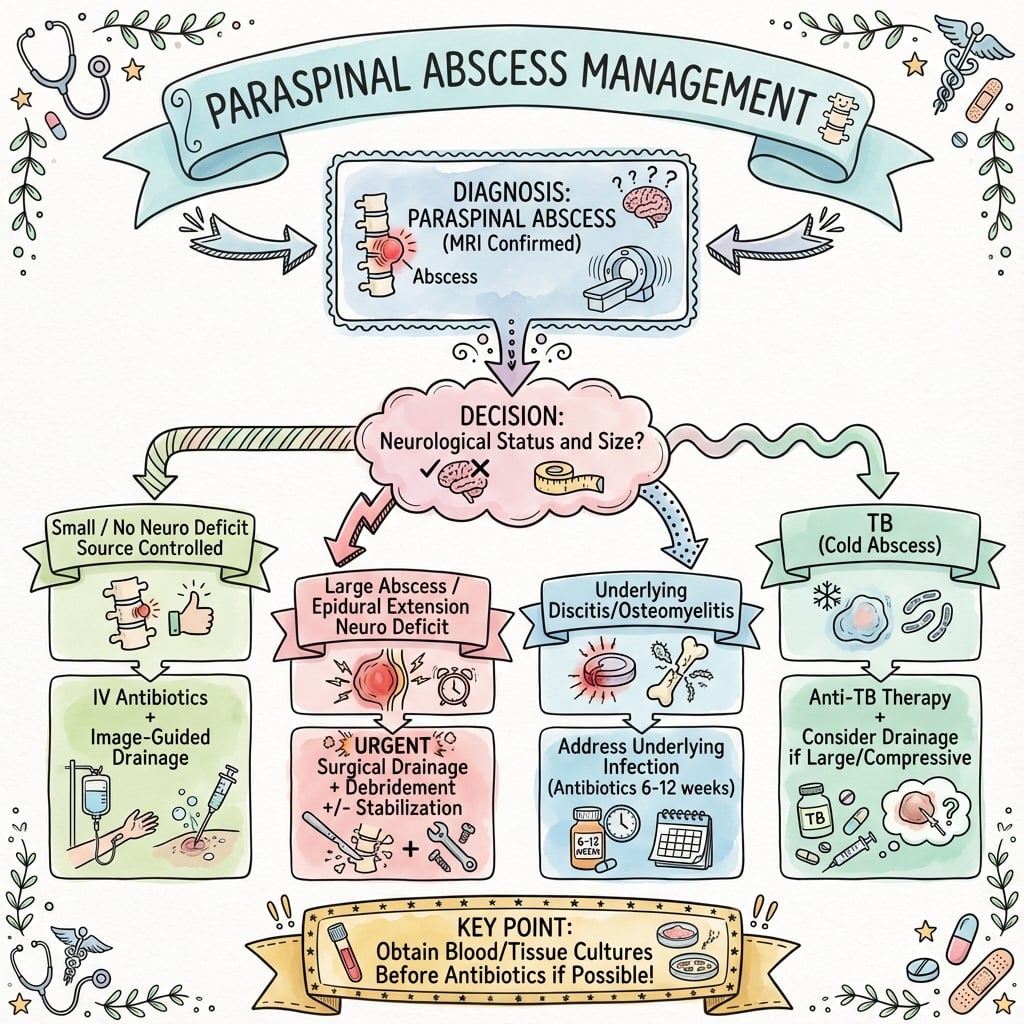
Clinical summary
Rapid Assessment
- •Back pain + fever + elevated CRP → Think paraspinal abscess
- •Check neurology (intact = paraspinal, deficit = epidural extension)
- •Order MRI with contrast whole spine urgently
Immediate Management
- •Blood cultures × 2 before antibiotics
- •Empiric: vancomycin 25-30 mg/kg load + ceftriaxone 2 g IV (covers MRSA and Gram-negatives)
- •CT-guided aspiration for culture if available
- •Admit under spinal surgery
Surgery Indications
- •Absolute: neurological deficit, spinal cord compression, septic shock, instability
- •Relative: abscess greater than 3 cm, failed medical therapy (fever persisting greater than 5 days)
- •Also relative: immunocompromised, cannot obtain diagnosis
Surgical Approach
- •CT-guided drainage first-line if accessible and unilocular
- •Open posterior midline if multiloculated, large (greater than 5 cm), or failed percutaneous
- •Wiltse approach for lateral abscess
- •Debride necrotic tissue, copious irrigation (6-9 L), drain placement
Antibiotic Duration
- •Total 6-12 weeks; IV minimum 4-6 weeks
- •Oral switch when afebrile 3-5 days + CRP declining
- •Isolated paraspinal = 6 weeks
- •With vertebral involvement = 12 weeks
- •MRSA may need longer
Monitoring
- •CRP/ESR every 3-4 days (expect 50% CRP reduction by week 2)
- •Daily neurology exam
- •Repeat MRI at 6-8 weeks or if deterioration
- •Remove drains when output less than 30 mL/24h
Red Flags
- •New neurological deficit = epidural extension (emergency MRI + decompression)
- •Persistent fever day 5-7 = treatment failure (repeat imaging, consider surgery)
- •Rising CRP = inadequate source control
Common Organisms
- •Staph aureus 60-70% (MRSA 20-40% of these)
- •Gram-negatives 10-15% (E. coli, Pseudomonas)
- •TB 10-20% (endemic areas, chronic presentation)
- •Strep 5-10%
Key Differentials
- •Epidural abscess (neurological deficit common)
- •Vertebral osteomyelitis (vertebral body involvement)
- •Psoas abscess (hip flexion contracture)
- •Hematoma (no fever, no CRP elevation, trauma history)
Viva Talking Points
- •MRI with gadolinium is gold standard (95% sensitive)
- •CT-guided drainage 60-70% success rate
- •MRSA risk factors: IVDU, recent hospitalization, prior MRSA
- •Diabetes = higher treatment failure
- •Size greater than 3 cm favors surgery
- •Always assess epidural space for extension
References
-
Berbari EF, Kanj SS, Kowalski TJ, et al. 2015 Infectious Diseases Society of America (IDSA) Clinical Practice Guidelines for the Diagnosis and Treatment of Native Vertebral Osteomyelitis in Adults. Clin Infect Dis. 2015;61(6):e26-46. PMID 26229122.
-
Bernard L, Dinh A, Ghout I, et al. Antibiotic treatment for 6 weeks versus 12 weeks in patients with pyogenic vertebral osteomyelitis: an open-label, non-inferiority, randomised, controlled trial. Lancet. 2015;385(9971):875-82. PMID 25468170.
-
Li HK, Rombach I, Zambellas R, et al. Oral versus Intravenous Antibiotics for Bone and Joint Infection. N Engl J Med. 2019;380(5):425-436. PMID 30699315.
-
Ledermann HP, Schweitzer ME, Morrison WB, Carrino JA. MR imaging findings in spinal infections: rules or myths? Radiology. 2003;228(2):506-514. PMID 12802004.
-
McHenry MC, Easley KA, Locker GA. Vertebral osteomyelitis: long-term outcome for 253 patients from 7 Cleveland-area hospitals. Clin Infect Dis. 2002;34(10):1342-1350. PMID 11981730.
-
Priest DH, Peacock JE Jr. Hematogenous vertebral osteomyelitis due to Staphylococcus aureus in the adult: clinical features and therapeutic outcomes. South Med J. 2005;98(9):854-62. PMID 16217976.
-
Cronin CG, Gervais DA, Hahn PF, Arellano R, Guimaraes AR, Mueller PR. Treatment of deep intramuscular and musculoskeletal abscess: experience with 99 CT-guided percutaneous catheter drainage procedures. AJR Am J Roentgenol. 2011;196(5):1182-8. PMID 21512090.
This guide provides evidence-based, globally applicable coverage of paraspinal abscess for orthopaedic fellowship examination preparation (FRCS, FRACS, EBOT, ABOS, DNB/MS, MRCS, SICOT).