Pauwels Classification of Femoral Neck Fractures
- Forgetting it's an AP measurement. The Pauwels angle is measured on the AP radiograph against a horizontal pelvic reference — the lateral view shows sagittal displacement, not the Pauwels angle. Inter-observer reliability is only moderate, and minor rotation shifts the type.
- Fixing a young Pauwels III with parallel screws alone. Vertical (high-shear) fractures fail with simple screws — use a shear-resisting construct (fixed-angle device, medial buttress plate, cephalomedullary nail). A young Pauwels III is an emergency: urgent anatomical reduction.
- Fixing a displaced Pauwels III in elderly osteoporotic bone. Fixation failure rates are unacceptable — choose primary arthroplasty (THA for the active patient).
- Quoting Pauwels alone. It captures angle only — combine with the Garden (displacement) classification, plus age and bone quality, for the real prognosis.
- Blaming the angle for AVN. AVN follows displacement and the vascular insult to the retinacular vessels, not the fracture angle per se — so an anatomical reduction (and protecting those vessels) matters more than the number.
The Pauwels classification system
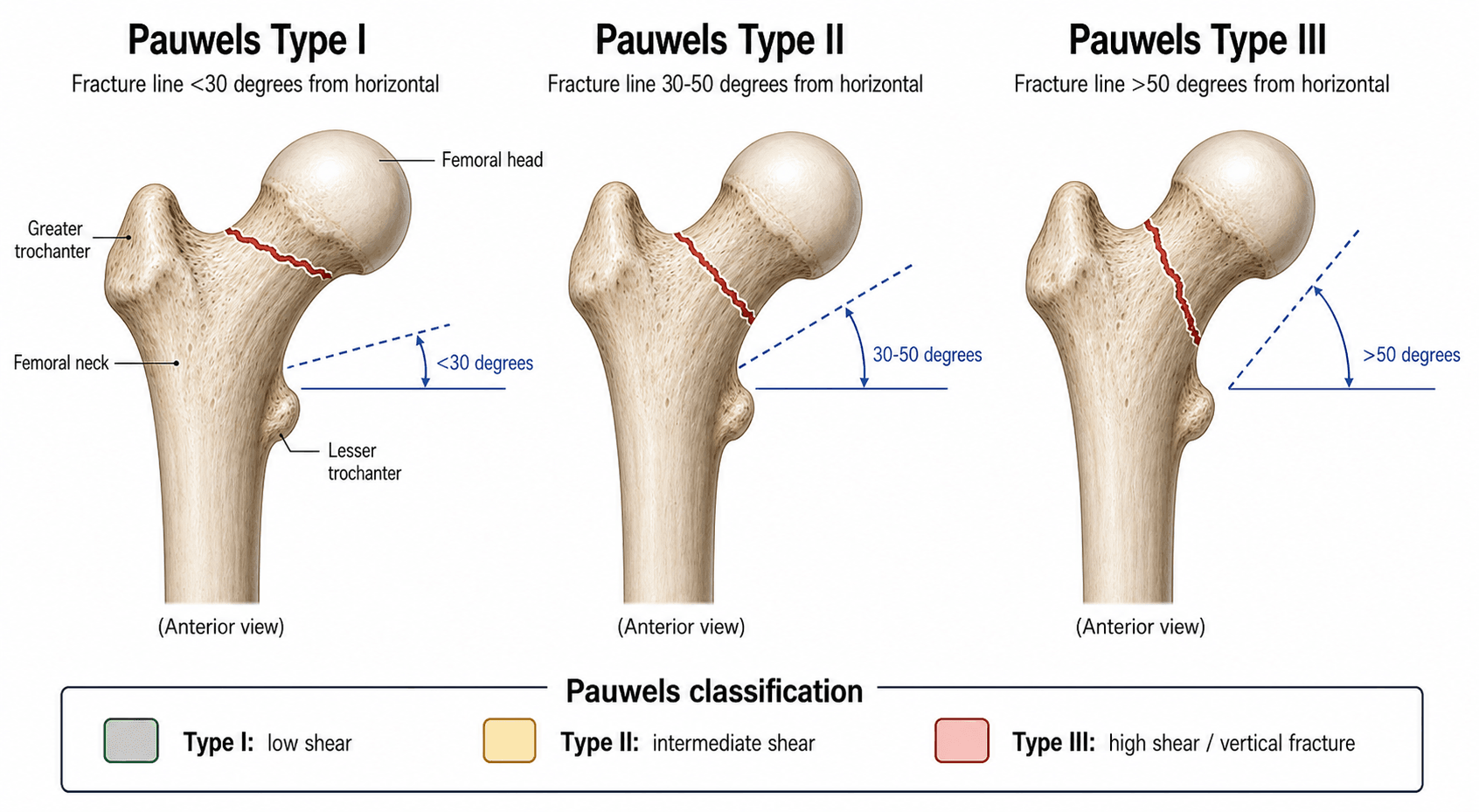

Pauwels divided femoral neck fractures into three types based on the inclination of the fracture line measured from the horizontal on a standard AP pelvic radiograph.
- Angle from horizontal
- Less than 30 degrees
- Dominant force
- Compression (axial load)
- Healing prognosis
- Favourable — compression promotes healing
- Angle from horizontal
- 30 to 50 degrees
- Dominant force
- Mixed compression and shear
- Healing prognosis
- Intermediate — shear begins to jeopardise stability
- Angle from horizontal
- Greater than 50 degrees
- Dominant force
- Shear (vertical force)
- Healing prognosis
- Unfavourable — shear displaces the fracture, high nonunion risk
Draw a horizontal reference line (along the superior margin of the sacral ala or the ischial tuberosities), then a line along the fracture plane; the angle between them is the Pauwels angle. A more vertical fracture is a higher type with a worse prognosis. Always measure on the AP radiograph — the lateral view assesses sagittal-plane displacement, not the Pauwels angle. Note that inter-observer reliability is only moderate, and minor hip/pelvis rotation can shift the measured type.
Biomechanics — why the angle matters
The femoral neck is loaded in compression during weight-bearing. A horizontal (low-angle) fracture is held together by axial compressive forces — the same force that drives healing. As the fracture line tilts toward vertical, an increasing component of the load becomes a shear force that slides the proximal fragment downward along the fracture plane.
- Type I (under 30 degrees): compression across the fracture exceeds shear; the surfaces are pressed together, promoting stability and union. Standard fixation (cannulated screws or sliding hip screw) works reliably.
- Type II (30 to 50 degrees): shear is significant; the fracture tends to displace inferoposteriorly. Fixation should add shear resistance — parallel cannulated screws in a valgus orientation, or a sliding hip screw with a derotation screw.
- Type III (over 50 degrees): shear dominates; the proximal fragment slides down and medially, causing varus collapse and screw cut-out. Simple parallel screws have a high failure rate; fixation must actively resist shear — a valgus-angled/fixed-angle device, a medial buttress plate, a cephalomedullary nail, or (in older patients) primary arthroplasty.
As the fracture line approaches vertical, the resolved shear component of joint load rises and the compressive component falls. This biomechanical shift is why Type III fractures fail with simple screw fixation — the screws are loaded in bending/shear and cut out, rather than being loaded in compression across an apposed fracture.
Higher shear means greater displacement risk, and each episode of displacement threatens the superior retinacular vessels (the main supply to the femoral head). This is the pathway to avascular necrosis: it is the displacement and vascular insult, more than the fracture angle itself, that drives AVN.
The topic invokes "the retinacular vessels" and "vascular insult" — here is the supply they refer to:
- The medial femoral circumflex artery (MFCA) is the dominant supply to the adult femoral head: its deep branch ascends along the posterosuperior neck and gives the lateral epiphyseal / superior retinacular vessels (running in the retinacula of Weitbrecht beneath the synovial reflection) that feed the weight-bearing head.
- The lateral femoral circumflex artery contributes less (anterior/inferior neck and head); both arise from the profunda femoris and form an extracapsular ring at the neck base feeding the ascending cervical (retinacular) branches.
- The artery of the ligamentum teres (foveal) is a minor adult supply — more important in children.
- Why an intracapsular fracture threatens the head two ways: (1) direct disruption of the retinacular vessels by the fracture/displacement, and (2) the intracapsular haematoma raising pressure (tamponade) that can further compromise retinacular flow — the rationale (debated) for early reduction and capsular decompression. This is why displacement and the vascular insult, more than the Pauwels angle, drive AVN.
Fixation strategy by Pauwels type
- 1Measure the angle and assign the typeAP radiograph: under 30° = I, 30–50° = II, over 50° = III. Also note displacement (Garden) and bone quality — they matter as much as the angle.
- 2Match the construct to the shearType I/II → parallel cannulated screws (inverted triangle) ± valgus orientation, or a sliding hip screw + derotation screw. Type III → a shear-resisting construct: fixed-angle device, medial buttress plate, or cephalomedullary nail.
- 3Young Type III = emergencyUrgent anatomical reduction (open if closed fails) and stable fixation as soon as the patient is fit — protect the retinacular blood supply; accept nothing less than an anatomical reduction.
- 4Elderly displaced = arthroplastyIn osteoporotic bone, fixation of a displaced Pauwels III has unacceptable failure rates — choose total hip arthroplasty for the active patient, hemiarthroplasty for the low-demand patient; aim for surgery within ~36 h.
- Young patient (under 60)
- Three parallel cannulated screws (inverted triangle)
- Elderly patient (over 65)
- Cannulated screws or sliding hip screw; consider arthroplasty if displaced or osteoporotic
- Young patient (under 60)
- Cannulated screws with valgus orientation, or sliding hip screw + derotation screw
- Elderly patient (over 65)
- Sliding hip screw with anti-rotation screw; low threshold for hemi- or total arthroplasty
- Young patient (under 60)
- Urgent anatomical reduction + fixed-angle device, medial buttress plate, or cephalomedullary nail
- Elderly patient (over 65)
- Primary total hip arthroplasty (cemented or uncemented); hemiarthroplasty if low demand
A Pauwels Type III fracture in a young patient is an orthopaedic emergency. Urgent anatomical reduction (open if necessary) and stable internal fixation should be performed as soon as the patient is fit for surgery. Delay and a non-anatomical reduction both increase the risk of avascular necrosis — the blood supply to the femoral head depends on restoring the anatomy.

The topic demands an "anatomical reduction" — the examiner wants the objective criteria for it:
- Garden alignment index: on the AP, the principal compression trabeculae of the head should meet the medial femoral cortex at about 160°; on the lateral they should be roughly colinear (about 180°). An acceptable reduction sits about 155 to 180° on both views; varus (under about 155°) or marked deviation predicts fixation failure and AVN.
- Lowell's lines: the cortical outlines of the head and neck should form continuous, smooth S- and reversed-S curves where a convex meets a concave; a tangency or cusp (two curves meeting at a point) signals malreduction.
- Also restore Shenton's line and avoid residual varus or posterior tilt.
- Quality over clock: reduction quality is the strongest surgeon-controllable predictor of union/AVN (in Liporace's series failures occurred even with good reduction — so accept nothing less than anatomical). A displaced fracture in a young patient is a surgical urgency: most advocate prompt reduction and fixation (commonly within about 24 hours, sooner where feasible) to limit AVN, though the exact time threshold remains debated.
Limitations & practical considerations
- Inter-observer reliability is moderate at best. Different surgeons measure the Pauwels angle differently on the same radiograph, and the same fracture can shift types with minor rotation of the hip or pelvis.
- The classification is purely biomechanical and does not account for patient age, bone quality, displacement, timing of surgery, or vascularity — all of which influence outcome as much as, or more than, the angle alone.
- Combine with the Garden (displacement) classification. A fully displaced (Garden IV) low-angle fracture may carry a worse prognosis than an undisplaced (Garden I) high-angle fracture treated urgently.
- Modern angular-stable implants have narrowed the outcome gap between types — locking plates, fixed-angle devices, medial buttress plates and cephalomedullary nails provide shear resistance that screw-only constructs could not.
- CT is increasingly used to define the fracture geometry more precisely than plain radiographs, especially for vertically oriented fractures where surgical planning depends on the exact geometry.
Viva practice
Exam viva
Practise clinical reasoning and management decisions out loud
“A 32-year-old man is involved in a high-speed motor vehicle collision. Radiographs show a vertical fracture line through the femoral neck, measured at 55 degrees from the horizontal. The fracture is minimally displaced. How do you classify and manage this?”
“A 68-year-old active woman sustains a fall at home. Radiographs show a femoral neck fracture with a Pauwels angle of 60 degrees and the fracture is displaced. She is independent, mobilises with no aids, and has mild osteoporosis (T-score minus 2.5). Discuss your management.”
Exam cheat sheet
30–50The three angles
Hook:As the angle climbs from horizontal toward vertical, shear climbs with it and prognosis worsens — 'Vertical is Villain'.
- Type I under 30° (compression), II 30–50° (mixed), III over 50° (shear). Higher angle = more shear = worse prognosis.
- Measure on the AP with a horizontal pelvic reference; reliability is only moderate.
- Young Pauwels III is an emergency — urgent anatomical reduction + shear-resisting fixation (fixed-angle device, medial buttress plate, CMN).
- Elderly displaced Pauwels III → primary arthroplasty (THA for the active patient).
- AVN follows displacement and vascular insult, not the angle alone; counsel on the substantial AVN/nonunion risk.
- Combine Pauwels (angle) with Garden (displacement) for the full picture.
The three types (angle from horizontal)
- Type I: less than 30 degrees — compression-dominated, favourable healing
- Type II: 30 to 50 degrees — mixed forces, intermediate risk
- Type III: greater than 50 degrees — shear-dominated, high nonunion and AVN risk
Fixation by type
- Type I: parallel cannulated screws or sliding hip screw
- Type II: cannulated screws with valgus orientation or SHS plus derotation screw
- Type III young: urgent anatomical reduction, shear-resisting fixation (fixed-angle device, medial buttress plate, CMN)
- Type III elderly: primary total hip arthroplasty (fixation failure rate too high)
Key principles for the exam
- Higher angle equals more shear equals worse prognosis
- Young Pauwels III is an emergency — urgent reduction, protect retinacular vessels
- Always state angle, type, biomechanical implication, and fixation rationale
- Pauwels measures angle only — combine with Garden (displacement)
- AVN risk depends on displacement and vascular insult, not the angle alone
Evidence Base
Results of internal fixation of Pauwels type-3 vertical femoral neck fractures
- Multicentre series of 76 high-shear-angle (Pauwels type-3) femoral neck fractures (mean age 42); 62 followed to union or revision.
- Despite good-to-excellent reduction in 95%, the nonunion rate was 19% with cannulated screws alone versus 8% with a fixed-angle device (a difference that did not reach statistical significance).
- Osteonecrosis occurred in 11%; the authors concluded the ideal implant for this challenging pattern remains undefined.
Efficacy of four internal fixation devices on femoral neck fractures in young adults: a systematic review and network meta-analysis
- Network meta-analysis of 34 studies (2291 young-adult femoral neck fractures) comparing internal-fixation devices.
- The medial buttress plate ranked best for Harris hip score, lowest complication rate and fastest fracture healing; the femoral neck system ranked best for operation time and least neck shortening.
- Inverted triangular cannulated screws had the lowest intraoperative bleeding — i.e. no single device wins on every metric, but augmented/angular-stable constructs lead on function and complications.
According to PubMed, the high failure rate of screw-only fixation in vertical fractures comes from Liporace et al. 2008 (DOI), the valgus-osteotomy head-preserving option from Magu et al. 2005 (DOI), the appraisal of the classification's reliability from Nandi 2021 (DOI), and the medial-buttress-plate advantage from Giordano et al. 2019 (DOI) and Yuan et al. 2024 (DOI).