Fractures Around a Total Knee Arthroplasty
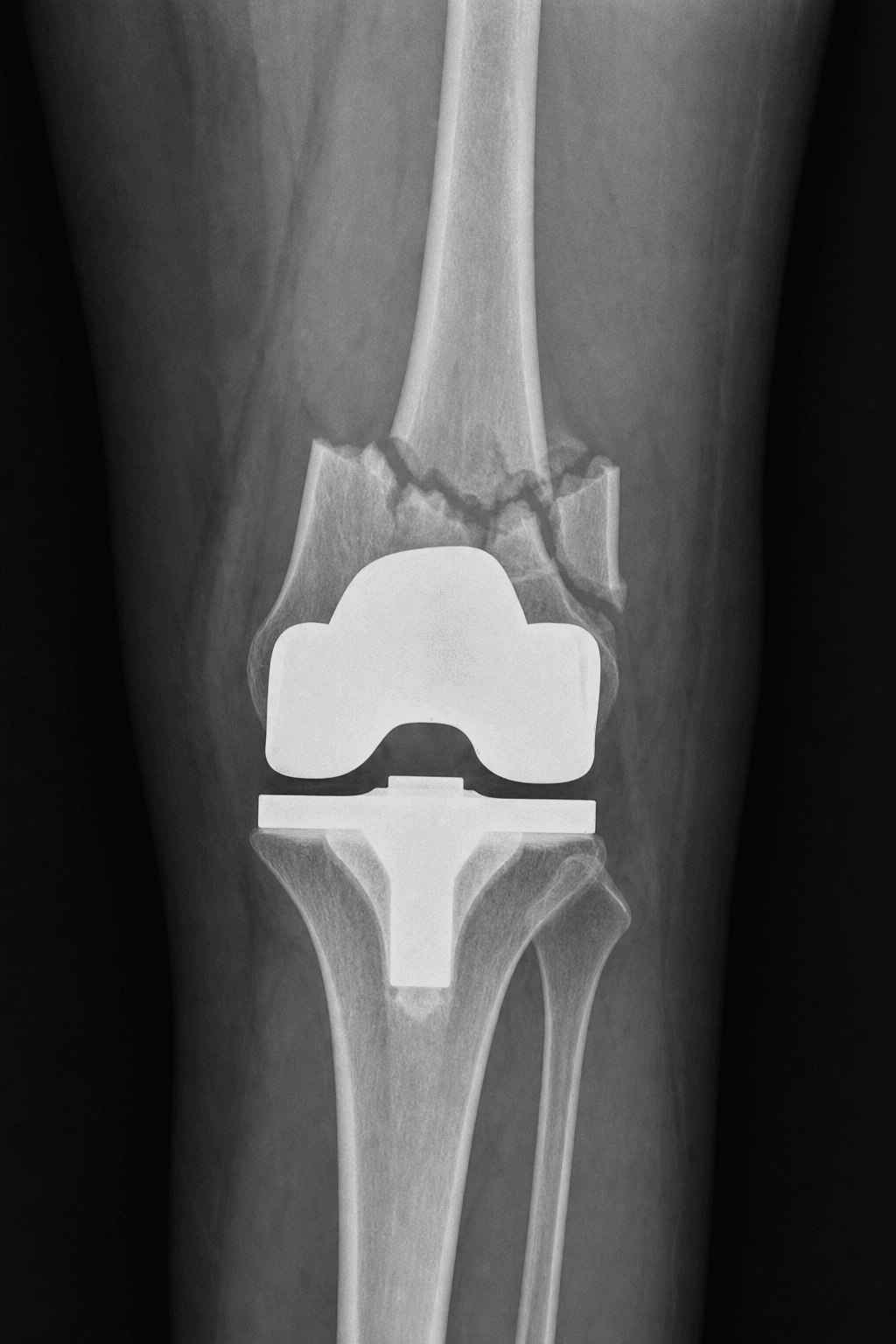
- The commonest periprosthetic fracture around a total knee arthroplasty is the SUPRACONDYLAR DISTAL FEMUR fracture (around the femoral component); tibial and patellar periprosthetic fractures are less common, and patellar fractures relate to resurfacing/maltracking/avascularity.
- RISK FACTORS include ANTERIOR FEMORAL NOTCHING (notching the anterior femoral cortex during TKA creates a stress riser), OSTEOPOROSIS, rheumatoid/steroid use, stiffness (a stiff knee transmits force to bone), neurological disease and falls, osteolysis/loosening, and revision or STEMMED implants (the stem tip is a stress riser).
- The two key CLASSIFICATIONS are the SU classification of supracondylar femoral fractures (Type I proximal to the femoral component, Type II at the level of the component, Type III extending distal to the upper edge of the anterior flange/involving the prosthesis), which guides the fixation strategy, and the LEWIS-RORABECK classification (Type I undisplaced with a well-fixed implant, Type II displaced with a well-fixed implant, Type III any displacement with a LOOSE or failing implant), which directly informs fix-versus-revise.
- TREATMENT is driven by COMPONENT FIXATION and DISTAL BONE STOCK, not the fracture pattern alone: a WELL-FIXED component with adequate distal bone is treated by FIXATION - a lateral DISTAL FEMORAL LOCKING PLATE or a RETROGRADE INTRAMEDULLARY NAIL (the latter requires an 'open-box'/nail-compatible femoral component), with the two broadly comparable and dual-implant (nail-plate) fixation used for complex patterns; modern evidence suggests retrograde nailing has limited adverse effect on TKA balance once the component is in place.
- A LOOSE component, or deficient/comminuted distal bone insufficient to hold fixation, is treated by REVISION arthroplasty or a DISTAL FEMORAL REPLACEMENT (megaprosthesis); DFR allows immediate weight-bearing and early mobilisation - valuable in frail elderly patients - but at the cost of higher longer-term implant-related complications.
- The ORIF-versus-DFR TRADE-OFF is important: comparative data in elderly patients show DFR gives immediate stability/mobilisation but has higher long-term periprosthetic joint INFECTION and revision rates, whereas ORIF carries higher rates of refracture and the need for additional fixation - with similar mortality - so the choice should be individualised. Fractures around STEMMED/revision implants, and INTERPROSTHETIC fractures (between a hip and knee implant), are higher-risk variants requiring spanning constructs that respect the stem as a stress riser.
- “Commonest periprosthetic knee fracture = SUPRACONDYLAR distal femur; ANTERIOR FEMORAL NOTCHING + osteoporosis + stemmed/revision implants are key risks.
- “Classify: SU (level vs component) + LEWIS-RORABECK (I undisplaced/well-fixed, II displaced/well-fixed, III loose implant). Treatment driven by COMPONENT FIXATION + distal bone stock.
- “Well-fixed + adequate bone -> locked plate or RETROGRADE NAIL (needs open-box component); loose/deficient -> revision / DISTAL FEMORAL REPLACEMENT. DFR: immediate mobilisation but higher long-term PJI/revision vs ORIF (which has more refracture).
Commonest = supracondylar distal femur around the TKA; risks = anterior notching, osteoporosis, stemmed/revision implants. Classify with Su and Lewis-Rorabeck (fixation/displacement).
Well-fixed component + adequate bone -> fixation (locked plate or retrograde nail); loose / deficient bone -> revision / distal femoral replacement.
Risk Factors, Classification & the Fix-vs-Replace Decision
The commonest periprosthetic knee fracture is the supracondylar distal femur around the femoral component; key risks are anterior femoral notching (a stress riser), osteoporosis, stiffness, osteolysis/loosening and revision/stemmed implants. Two classifications matter: the Su classification by level relative to the component, and the Lewis-Rorabeck classification (I undisplaced + well-fixed, II displaced + well-fixed, III any fracture with a loose implant). The treatment decision is driven by component fixation and distal bone stock, not the fracture pattern alone: a well-fixed component with adequate bone is fixed - a lateral locked plate or a retrograde intramedullary nail (the nail needs a 'nail-compatible/open-box' component), broadly comparable, with dual fixation for complex patterns; a loose component or deficient/ comminuted distal bone is treated by revision / distal femoral replacement.
| Component & bone | Lewis-Rorabeck | Typical treatment |
|---|---|---|
| Well-fixed, adequate distal bone (undisplaced) | Type I | Non-operative (rare) or fixation if any instability |
| Well-fixed, adequate distal bone (displaced) | Type II | Fixation: lateral locked plate or retrograde nail (open-box component) |
| Loose/failing component (any displacement) | Type III | Revision arthroplasty |
| Deficient/comminuted distal bone, low-demand elderly | (any) | Distal femoral replacement (immediate weight-bearing) |
Fixation, Replacement & the ORIF-vs-DFR Trade-off
- Locked plating: a lateral distal femoral locking plate - versatile, handles most patterns, spans to the component.
- Retrograde intramedullary nail: for suitable fractures with a 'nail-compatible/open-box' femoral component; modern evidence suggests limited adverse effect on TKA balance once the component is in place. Dual (nail-plate) fixation for complex/comminuted fractures.
- Revision / distal femoral replacement (DFR): for a loose component or distal bone insufficient to hold fixation - DFR allows immediate weight-bearing and early mobilisation (valuable in frail elderly).
- The ORIF-vs-DFR trade-off: DFR gives immediate stability but has higher long-term periprosthetic joint infection and revision rates; ORIF has higher refracture and additional-fixation rates - individualise.
- Stemmed/revision and interprosthetic variants: respect the stem tip as a stress riser and use spanning constructs that do not create a new stress riser (see the Interprosthetic Femoral Fracture topic)."
The decisive step in a periprosthetic knee fracture is determining whether the femoral component is well-fixed and whether the distal bone stock is adequate, because these - not the fracture pattern alone - decide between fixation and revision/replacement: a fracture with a loose component (Lewis-Rorabeck III) needs revision, and a distal fragment too small or osteoporotic to hold a plate/nail needs a distal femoral replacement. When fixing, respect the implant: a retrograde nail requires a nail-compatible (open-box) femoral component, and any construct around a stemmed or revision implant - or in an interprosthetic situation - must span adequately so it does not create a new stress riser. Finally, counsel the elderly patient on the genuine trade-off: a distal femoral replacement mobilises them immediately but carries higher long-term infection and revision risk than fixation, which in turn risks refracture - so the choice is individualised to the patient and bone.
Evidence & Key Studies
Distal femoral replacement vs ORIF for periprosthetic distal femur fractures in the elderly
- In propensity-matched elderly patients (698 per group), distal femoral replacement (DFR) had higher perioperative morbidity (wound disruption, transfusion) than ORIF.
- At 5 years DFR had higher periprosthetic joint infection (22.5% vs 5.3%), revision TKA (15.5% vs 3.3%) and subsequent knee procedures, whereas ORIF had higher refracture (55.3% vs 44.8%) and additional fixation; mortality was similar.
- There is a trade-off between the immediate stability/mobilisation of DFR and its longer-term implant-related complications, supporting individualised treatment selection.
Knee laxity after retrograde intramedullary nailing for periprosthetic distal femur fractures (cadaveric)
- Periprosthetic distal femur fractures are increasingly treated with intramedullary nailing as primary TKA volume rises.
- In a cadaveric model, retrograde IMN did not significantly affect the flexion gap when the femoral component was in place, and the extension gap was unchanged.
- The findings suggest limited clinical impact of retrograde IMN on knee balance in the context of modern TKA femoral preparation, supporting it as a fixation option for suitable fractures.
According to PubMed, the comparative ORIF-versus-distal-femoral-replacement outcomes in elderly periprosthetic distal femur fractures (DFR higher long-term infection/revision; ORIF higher refracture; similar mortality) come from the cited Boutany cohort, and the evidence that retrograde intramedullary nailing has limited adverse effect on TKA balance (supporting it as a fixation option) from the cited Rainey cadaveric study. The supracondylar predominance, anterior-notching and stemmed-implant risk factors, the Su and Lewis-Rorabeck classifications, and the component-fixation-and-bone-stock-driven fix-versus-replace algorithm are standard, well-established teaching. (See also our Interprosthetic Femoral Fracture and Periprosthetic Hip Fracture (Vancouver) topics.)
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“How do you classify and decide treatment for a periprosthetic distal femur fracture above a TKA?”
“In a frail elderly patient, how do you weigh ORIF against a distal femoral replacement?”
Mnemonics & Memory Aids
NOTCH
Hook:NOTCH: Notching risk, Operate by fixation+bone, Two classifications (Su/Lewis-Rorabeck), Component fixed -> fix, Hopeless bone/loose -> DFR.
Where & risks
- Commonest = supracondylar distal femur around the femoral component
- Risks: anterior femoral notching, osteoporosis, stiffness, osteolysis, stemmed/revision implants
- Tibial/patellar periprosthetic fractures less common
Classification
- Su: by level relative to the femoral component (I above, II at, III distal/interface)
- Lewis-Rorabeck: I undisplaced+well-fixed, II displaced+well-fixed, III loose implant
- Component fixation + bone stock drive treatment
Fixation
- Well-fixed component + adequate bone -> lateral locked plate or retrograde IMN (open-box component)
- Plate and nail broadly comparable; dual fixation for complex patterns
- Span adequately around stemmed/revision implants (stress riser) - see Interprosthetic Fracture
Replacement & trade-off
- Loose component or deficient distal bone -> revision / distal femoral replacement (DFR)
- DFR: immediate weight-bearing but higher long-term PJI/revision
- ORIF: more refracture/additional fixation; similar mortality - individualise