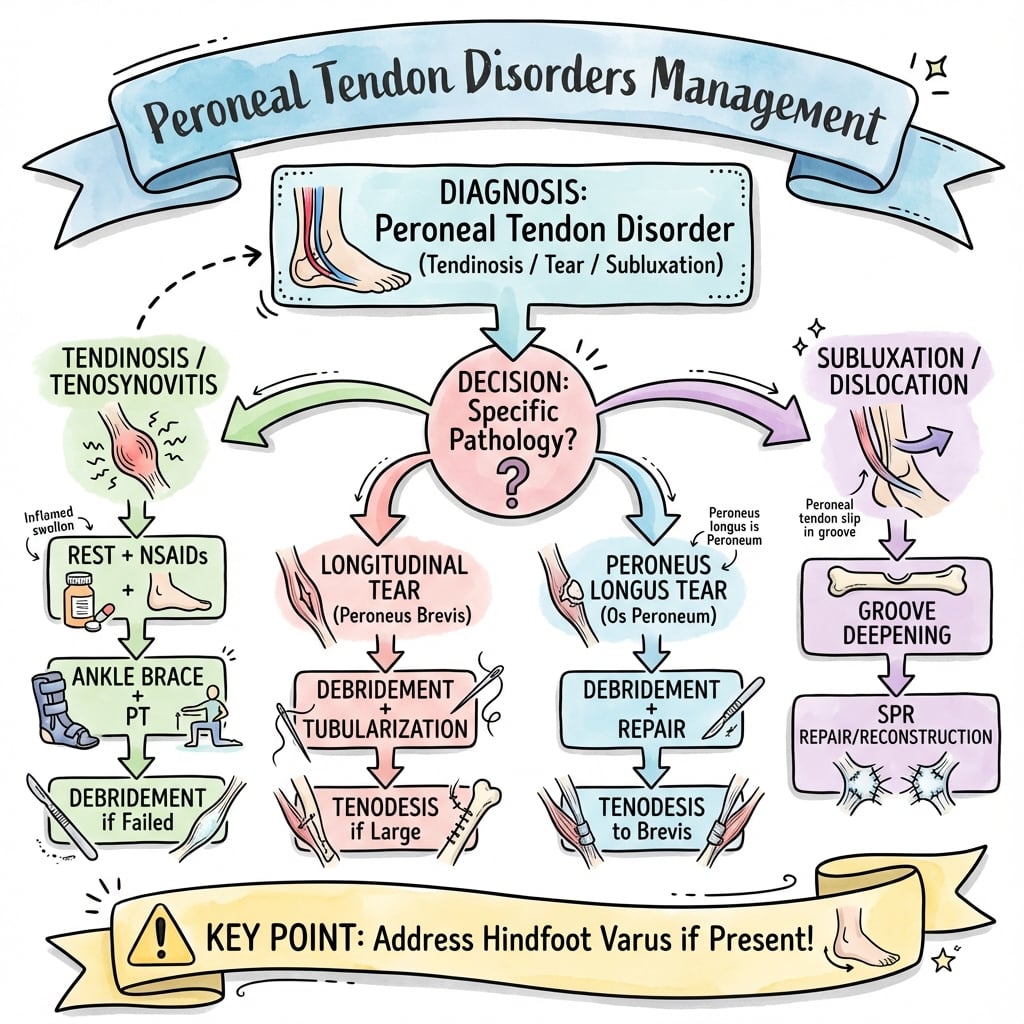
Lateral Ankle Pain | Subluxation and Tears | SPR Repair | Tenodesis
PERONEUS BREVIS TEARS CLASSIFICATION
Critical Must-Knows
- Peroneus brevis most commonly torn - lies anterior, compressed against fibula
- Superior peroneal retinaculum (SPR) injury causes subluxation - attach fibular groove rim
- Low-lying peroneus brevis muscle belly anatomical variant increases tear risk
- MRI gold standard - demonstrates split tears, subluxation, muscle edema patterns
- Acute SPR repair superior to delayed - 90% vs 60% return to sport
Clinical Pearls
- "Peroneal subluxation tests: Passive dorsiflexion-eversion with active resistance - feel snap
- "Split tears: Linear high signal on MRI, 'comma sign' on axial imaging (retracted tendon)
- "Oden classification for subluxation guides SPR repair vs groove deepening vs both
- "Tenodesis indication: Over 50% tendon loss, severe degeneration, failed primary repair
Clinical Imaging
Imaging Gallery



Critical Peroneal Tendon Exam Points
Anatomy Distinction
Peroneus brevis lies anterior. Inserts 5th metatarsal base. More commonly torn (compressed against fibular groove). Peroneus longus posterior, travels under foot to 1st metatarsal/medial cuneiform. Subluxation affects both but brevis tear dominates.
SPR Anatomy
Superior peroneal retinaculum attaches from lateral fibular ridge to lateral calcaneus. Width 1-2cm, just posterior to lateral malleolus. Injury mechanism: forced dorsiflexion-eversion, avulsion from fibula. Oden Types I-IV guide repair strategy.
Surgical Indications
Acute SPR repair: within 6 weeks, active patients. Chronic subluxation: failed conservative, recurrent snapping, sports. Tendon repair: over 50% width tear, grade 2-3. Tenodesis: irreparable brevis, over 50% tendon loss.
Critical Timing
Acute SPR repair: Operate within 6 weeks - 90% return to sport vs 60% delayed. Split tear debridement: Early intervention prevents propagation. Postop protocol: NWB 4 weeks in equinus cast, protect repair healing before loading.
Quick Decision Guide - Peroneal Pathology
| Clinical Scenario | Pathology | Treatment | Key Pearl |
|---|---|---|---|
| Acute subluxation, sports injury, under 6 weeks | Oden Type I SPR avulsion | Open SPR repair to fibula | Early repair critical - 90% return to sport |
| Chronic subluxation, shallow groove, failed conservative | Oden Type II-III, groove pathology | SPR repair + groove deepening | Combined procedure for anatomical deficiency |
| Lateral ankle pain, MRI shows longitudinal split under 50% | Grade 1 peroneus brevis tear | Debridement, synovectomy | Conservative if minimal - PT for 3 months first |
| Lateral ankle pain, MRI shows over 50% tendon width tear | Grade 2-3 peroneus brevis tear | Tubularization repair or tenodesis | Tenodesis if over 50% loss or severe degeneration |
BALFPeroneal Tendon Anatomy
| B | Brevis is Anterior Lies anterior in fibular groove, compressed against bone - more tears |
| A | At 5th metatarsal base Peroneus brevis insertion site - avulsion fractures occur here |
| L | Longus travels Long way Posterior tendon, travels under foot to 1st metatarsal/medial cuneiform |
| F | Fibular groove posterior Posterior to lateral malleolus, SPR prevents subluxation |
| B | Brevis is Anterior Lies anterior in fibular groove, compressed against bone - more tears | L | Longus travels Long way Posterior tendon, travels under foot to 1st metatarsal/medial cuneiform |
| A | At 5th metatarsal base Peroneus brevis insertion site - avulsion fractures occur here | F | Fibular groove posterior Posterior to lateral malleolus, SPR prevents subluxation |
Hook:BALF - Brevis At front, Longus Further back in the fibular groove!
FAGSSuperior Peroneal Retinaculum (SPR) Injury Classification - Oden
| F | Fibular avulsion (Type I) SPR avulsed from fibular insertion - most common acute injury |
| A | Attenuated SPR (Type II) Stretched but intact SPR, often with shallow groove |
| G | Groove deficiency (Type III) Shallow or convex fibular groove, SPR intact but insufficient |
| S | Scarred/healed (Type IV) Chronic healed SPR injury with persistent subluxation |
| F | Fibular avulsion (Type I) SPR avulsed from fibular insertion - most common acute injury | G | Groove deficiency (Type III) Shallow or convex fibular groove, SPR intact but insufficient |
| A | Attenuated SPR (Type II) Stretched but intact SPR, often with shallow groove | S | Scarred/healed (Type IV) Chronic healed SPR injury with persistent subluxation |
Hook:FAGS classification - From acute avulsion to chronic scarred states, guides surgical approach!
DRGTSurgical Treatment Options for Peroneal Disorders
| D | Debridement Grade 1 tears under 50% - remove degenerative tissue, synovectomy |
| R | Repair (tubularization) Grade 2 tears - side-to-side suture, restore tubular contour |
| G | Groove deepening Shallow groove - remove 2-3mm cortical bone, preserve lateral ridge for SPR |
| T | Tenodesis Grade 3 irreparable - brevis to longus tenodesis, sacrifice function |
| D | Debridement Grade 1 tears under 50% - remove degenerative tissue, synovectomy | G | Groove deepening Shallow groove - remove 2-3mm cortical bone, preserve lateral ridge for SPR |
| R | Repair (tubularization) Grade 2 tears - side-to-side suture, restore tubular contour | T | Tenodesis Grade 3 irreparable - brevis to longus tenodesis, sacrifice function |
Hook:DRGT - Debride, Repair, Groove, Tenodesis - escalating surgical intervention ladder!
Overview and Epidemiology
Why Peroneal Disorders Matter
Peroneal tendon pathology is underdiagnosed - often attributed to chronic lateral ankle pain or recurrent sprains. Peroneus brevis splits occur in over three-quarters of symptomatic cases due to compression in the fibular groove. Superior peroneal retinaculum (SPR) injuries cause painful subluxation, particularly in athletes during cutting sports. Early recognition and surgical intervention within 6 weeks for acute injuries achieves superior outcomes compared to chronic management.
Demographics
- Age: 20-40 years most common for acute tears and subluxation
- Gender: Male athletes higher risk for SPR injury (forced eversion)
- Sports: Basketball, soccer, skiing - forced dorsiflexion-eversion
- Chronic: Over 40 years - degenerative splits, low-lying muscle belly variant
Clinical Impact
- Lateral ankle pain - often misdiagnosed as ankle sprain or ATFL injury
- Functional limitation - difficulty with lateral push-off, cutting sports
- Recurrent subluxation - painful snapping, instability sensation
- Progression - untreated splits propagate, tendon degeneration accelerates
High-Risk Anatomical Variants
Low-lying peroneus brevis muscle belly extends into the fibular groove (15-20% population) - increases compression, doubles tear risk. Shallow fibular groove (Oden Type III) predisposes to subluxation even with intact SPR. Peroneal tubercle hypertrophy on lateral calcaneus can cause chronic friction and splitting. Identify these on MRI preoperatively to guide surgical planning.
Pathophysiology and Anatomy
Fibular Groove Anatomy - Critical to Understand Pathology
The retrofibular groove is a concave depression on the posterior lateral malleolus, approximately 1cm wide and 2-3mm deep. Peroneus brevis lies anterior within this groove, directly against bone, while peroneus longus is posterior. The groove acts as a pulley during ankle dorsiflexion-plantarflexion and eversion. Compression of brevis against the fibula during eversion generates shear forces that cause longitudinal splitting. The superior peroneal retinaculum (SPR) originates from the lateral fibular ridge (Wagstaffe tubercle area) and inserts on the lateral calcaneus, spanning the tendons to prevent anterior subluxation.
Peroneal Tendon Anatomy Comparison
| Feature | Peroneus Brevis | Peroneus Longus |
|---|---|---|
| Position in groove | Anterior - against fibula | Posterior - against brevis |
| Insertion | 5th metatarsal base (dorsal) | 1st metatarsal base, medial cuneiform (plantar) |
| Function | Ankle eversion, plantarflexion | Ankle eversion, 1st ray plantarflexion, arch support |
| Tear frequency | 77% of peroneal tears | 23% of peroneal tears |
| Mechanism of tear | Compression in groove, shear | Usually associated brevis tear or trauma |
Superior Peroneal Retinaculum (SPR)
- Origin: Lateral fibular ridge (Wagstaffe tubercle), 1-2cm wide band
- Insertion: Lateral calcaneus, just posterior to malleolus
- Function: Prevents anterior subluxation during eversion, stabilizes tendons
- Blood supply: Branches from peroneal artery - repair preserves vascularity
- Injury: Avulsion from fibula (Type I), stretch (Type II), chronic attenuation (Type IV)
Fibular Groove Variants
- Normal: Concave, 2-3mm depth, smooth cortical surface
- Shallow: Under 2mm depth (Oden Type III) - predisposes to subluxation
- Convex: Outward bulge - pathological, requires groove deepening
- Irregular: Post-fracture, hypertrophic spurring - friction source
- Widened: Chronic subluxation stretches groove, retinaculum incompetent
Biomechanics of Peroneal Tendon Pathology
Compression mechanism: During ankle eversion, peroneus brevis is compressed between the fibula and peroneus longus. The anterior position of brevis within the groove concentrates shear stress on its posterior surface, leading to longitudinal splitting that propagates proximally and distally.
Low-lying muscle belly variant: When the muscle belly extends into the fibular groove (15-20% prevalence), the increased tissue bulk within the constrained space further elevates compression forces during ankle motion, accelerating degenerative changes.
Subluxation mechanism: With SPR insufficiency (avulsion or attenuation), dorsiflexion-eversion causes the tendons to subluxate anteriorly over the lateral malleolus. The snapping sensation represents reduction back into the groove with plantarflexion. Chronic subluxation causes SPR stretching and groove rim wear.
Classification Systems
Peroneus Brevis Tear Grading
| Grade | Tear Extent | Tendon Integrity | Treatment | Prognosis |
|---|---|---|---|---|
| Grade 1 | Less than 50% width | Majority intact, functional | Debridement, synovectomy | Excellent - 90% return to sport |
| Grade 2 | 50-100% width, repairable | Compromised but reparable | Tubularization, side-to-side repair | Good - 80% return to sport with PT |
| Grade 3 | Over 50% tendon substance loss | Severe degeneration, irreparable | Tenodesis to longus, allograft | Fair - 60% return, accept function loss |
Grading Determination Intraoperatively
The 50% threshold is critical. Tears involving less than 50% of tendon width can be debrided and retain sufficient strength for function. Tears over 50% require tubularization repair to restore mechanical strength. Grade 3 with over 50% substance loss (not just split width but actual tendon tissue gone) necessitates tenodesis because repair under tension will fail. Assess intraoperatively - MRI often underestimates extent.
Clinical Assessment
History - Key Features
- Pain location: Lateral ankle, posterior to malleolus, aggravated by activity
- Mechanism: Forced dorsiflexion-eversion (acute SPR tear), insidious onset (chronic split)
- Snapping sensation: Palpable or audible snap with ankle motion (subluxation)
- Functional limitation: Difficulty with lateral push-off, cutting, running
- Chronic ankle sprains: Recurrent lateral ankle pain, attributed to ligamentous injury
- Prior treatment: Failed conservative management, ankle bracing ineffective
Examination - Specific Tests
- Inspection: Swelling posterior to lateral malleolus, asymmetry vs contralateral
- Palpation: Tenderness along peroneal tendons, fibular groove, SPR insertion
- Peroneal subluxation test: Passive dorsiflexion-eversion with active resistance - feel snap
- Resisted eversion: Pain with resisted eversion suggests tendon pathology
- Circumduction test: Ankle circumduction reproduces snapping or pain
- Neurovascular: Common peroneal nerve function (dorsiflexion, EHL), pulses intact
Beware the Occult Peroneal Tear
Chronic lateral ankle pain in the absence of acute injury or obvious instability may represent peroneal tendon pathology. Misdiagnosis as chronic ankle sprain is common, leading to failed conservative treatment. Consider peroneal pathology when:
- Lateral ankle pain posterior to malleolus (not anterior ATFL distribution)
- Failed physiotherapy for presumed sprain over 3 months
- Snapping sensation or audible pop with ankle motion
- Tenderness directly over fibular groove or peroneal tendons MRI is gold standard to confirm diagnosis and avoid delayed treatment.
Physical Examination Maneuvers
Peroneal Subluxation Test (Specificity 90%):
- Patient seated, ankle relaxed in neutral position
- Examiner passively dorsiflexes and everts ankle
- Patient actively resists eversion while maintaining dorsiflexion
- Positive test: Palpable or visible snap as tendons subluxate anteriorly over lateral malleolus
- Tendons reduce with plantarflexion - audible or palpable clunk
Circumduction Test:
- Passively circumduct the ankle through full ROM
- Positive: Pain or snapping at specific arc (usually dorsiflexion-eversion)
- Reproduces patient's symptoms
Resisted Eversion Strength:
- Compare to contralateral side
- Weakness suggests significant tendon pathology (over 50% tear or chronic degeneration)
- Pain without weakness: minor tear or tendinopathy
Differential Diagnosis of Chronic Lateral Ankle Pain
Differential Diagnosis - Lateral Ankle Pain
| Condition | Pain Location / Pattern | Key Discriminating Feature | Confirmatory Test |
|---|---|---|---|
| Peroneal tendon tear / tendinopathy | Posterior to lateral malleolus, worse with activity and eversion | Tenderness along tendon sheath, pain on resisted eversion | MRI (split, comma sign) or dynamic ultrasound |
| Peroneal subluxation / dislocation | Snapping posterior to malleolus, instability sensation | Palpable tendon snap on dorsiflexion-eversion against resistance | Dynamic ultrasound; positive subluxation test |
| ATFL lateral ankle instability | Anterolateral, giving way on uneven ground | Anterior drawer / tilt positive, tenderness anterior to malleolus | Stress radiographs, MRI of ATFL/CFL |
| Sinus tarsi syndrome | Anterolateral, in the sinus tarsi opening | Point tenderness in sinus tarsi, relief with local anaesthetic injection | Diagnostic injection, MRI (oedema/scar in sinus tarsi) |
| Lateral talar / talar dome OCD | Deep ankle pain, catching, swelling | Pain on weight-bearing, effusion, not localized to tendon | MRI; CT for bony detail |
| Calcaneofibular / distal fibula stress or os peroneum pathology | Lateral/plantar-lateral pain, may have midfoot component | Os peroneum tenderness at cuboid, painful resisted 1st ray plantarflexion | Radiograph (os peroneum), MRI of peroneus longus |
Investigations
Imaging Protocol for Peroneal Pathology
Views: AP, lateral, mortise ankle. Oblique foot if 5th metatarsal base pain. Look for:
- Fibular groove abnormalities (shallow, convex, spurs)
- Os peroneum fragmentation (peroneus longus injury)
- 5th metatarsal base avulsion (brevis insertion injury)
- Ankle fracture (11% association with peroneal injury)
- Lateral calcaneal spurring (chronic friction)
Sensitivity: Low for soft tissue pathology, but essential baseline.
Protocol: Axial, sagittal, coronal sequences. T1, T2, STIR. Fat-suppressed imaging critical. Key findings:
- Longitudinal split: Linear high signal within tendon on all sequences
- Comma sign: Axial view shows retracted split tendon edge (pathognomonic)
- Low-lying muscle belly: Muscle extending into fibular groove
- SPR injury: Discontinuity, edema, avulsion from fibula
- Subluxation: Tendons anterior to lateral malleolus on axial view
- Tendinosis: Increased T2 signal, tendon thickening, peritendinous edema
Sensitivity/Specificity: 90% for tears, 80% for subluxation (dynamic component missed).
Advantage: Real-time dynamic evaluation during ankle motion - can visualize subluxation. Findings: Hypoechoic split, tendon thickening, subluxation during dorsiflexion-eversion. Limitation: Operator-dependent, less detailed than MRI for intrasubstance tears. Use case: When MRI unavailable or confirms dynamic subluxation clinically suspected.
Indication: Preoperative planning for fibular groove anatomy in Oden Type III. Advantage: Precise bony anatomy, groove depth measurement, surgical planning. Limitation: No soft tissue detail - does not show tendon or SPR pathology.
MRI Interpretation Pearls
Comma sign on axial MRI: The retracted edge of a longitudinal split peroneus brevis creates a C-shaped or comma appearance - highly specific for split tear. Low-lying muscle belly: Look for muscle signal extending into the fibular groove on axial images - this predicts increased risk of recurrent tearing even after repair. SPR avulsion: Focal high T2 signal at fibular insertion site with discontinuity - indicates acute injury suitable for primary repair. Tendinosis vs tear: Diffuse high T2 signal without discrete linear split suggests tendinopathy - may respond to conservative treatment.
Management Algorithm
Non-Operative Treatment Indications
Appropriate for:
- Grade 1 tears (under 50% width) in low-demand patients
- Mild subluxation without mechanical symptoms (snapping tolerable)
- Tendinopathy without discrete tear
- First-line for all patients without acute SPR avulsion
Conservative Protocol - 3 Month Trial
Goals: Reduce inflammation, protect tendons from further injury.
- Immobilization: CAM boot or ankle brace, limit eversion activity
- Ice: 15-20 minutes TDS, reduce acute edema
- NSAIDs: Consider short course (2 weeks) if no contraindications
- Activity modification: Avoid cutting sports, lateral movements
Goals: Restore strength, proprioception, gradual return to function.
- Physiotherapy: Eccentric peroneal strengthening, balance training
- Ankle mobilization: Restore dorsiflexion ROM without eversion stress
- Proprioception: Single-leg balance, wobble board, sport-specific drills
- Taping: Athletic taping or bracing for sport if tolerated
Criteria: Pain-free ADLs, full strength vs contralateral, no subluxation symptoms.
- Gradual progression: Walk → jog → run → cutting → full sport
- Bracing: External ankle support may be needed long-term
- Re-evaluation: If symptoms persist at 12 weeks, consider MRI and surgical consultation
When Conservative Treatment Fails
Indications for surgical referral:
- Persistent pain or subluxation after 3 months conservative treatment
- Recurrent subluxation causing mechanical symptoms or activity limitation
- Progressive tendon degeneration on repeat MRI
- Acute SPR avulsion in active patients (surgical window 6 weeks)
- Grade 2-3 tears with functional impairment
Do not delay surgery in acute SPR injuries - outcomes deteriorate significantly after 6 weeks.
Surgical Technique
Patient Positioning and Setup
Positioning Checklist
Supine or lateral decubitus (surgeon preference). Ipsilateral hip bump for supine to internally rotate leg.
- Head: Secured on donut, neutral cervical spine
- Torso: Flat on table, bump under ipsilateral hip (10-15 degrees rotation)
- Contralateral leg: Flat, secured with leg holder or tape
- Operative leg: Free draped from tourniquet to toes
- Tourniquet: High thigh, well-padded, inflated to 250-300mmHg (or LOP + 100)
- Exsanguination: Elevate limb 2 minutes, Esmarch bandage from toes to tourniquet
- Prep: Betadine or chlorhexidine, toes to mid-calf, allow dry time
- Drape: Free drape foot and ankle, exclude toes (but keep visible for positioning checks)
- Implants: 2-3 suture anchors (3.0-3.5mm) for SPR repair, have extras
- Suture: 2-0 FiberWire or Ethibond for tendon repair, 0 or 1 for SPR
- Instruments: Small joint set, periosteal elevator, bone rongeur for groove deepening
- Power: Sagittal saw or burr for groove deepening (if planned)
- C-arm: Not typically needed, but available if fracture fixation required
Surgical Approach - Lateral Ankle
Lateral Approach to Peroneal Tendons
Landmarks: Posterior border of fibula, from 6cm proximal to tip of lateral malleolus to 3cm distal. Length: 8-10cm curvilinear incision, following posterior fibular border. Orientation: Slightly curved posteriorly to avoid sural nerve anteriorly. Technique: Sharply through skin and subcutaneous tissue with knife, preserve cutaneous nerves.
Critical step: Sural nerve runs with short saphenous vein in subcutaneous tissue, anterior to incision.
- Location: Typically 1-2cm anterior to posterior fibular border
- Identify: Look for nerve-vessel bundle in subcutaneous fat after skin incision
- Protect: Retract anteriorly with skin flap, avoid traction injury
Sural Nerve Injury
Sural nerve injury causes lateral foot numbness and painful neuroma. Incidence 5-10% in lateral ankle surgery. Prevention: Keep incision posterior along fibular border, gentle handling of nerve when identified, avoid traction on anterior skin flap. If nerve injured, consider primary repair with microsurgical technique or bury nerve end in muscle to prevent neuroma.
Layer: Superficial peroneal fascia overlying tendons, just deep to subcutaneous fat. Technique: Longitudinal incision over palpable tendons, parallel to skin incision. Identify: Superior peroneal retinaculum (SPR) as thickened band at level of lateral malleolus. Preserve: SPR initially - do not divide until pathology assessed.
Incise SPR: Longitudinal incision through SPR, directly over tendons (will repair later). Open sheath: Continue incision proximally and distally to fully expose tendon sheath. Synovectomy: Remove inflamed synovium to visualize tendons clearly. Identify pathology: Inspect both peroneus brevis (anterior) and longus (posterior) for tears, subluxation, low-lying muscle belly.
Avoid the Sural Nerve
The sural nerve is the most at-risk structure in lateral ankle surgery. It runs 1-2cm anterior to the posterior fibular border, within the subcutaneous fat. Prevention strategy: Make skin incision directly over posterior fibular border or slightly posterior, identify nerve early in dissection, retract anteriorly with skin flap. If injured: Consider primary repair if sharp transection, or bury nerve end in peroneus brevis muscle to prevent symptomatic neuroma.
Intraoperative Troubleshooting
Common Intraoperative Problems and Solutions
| Problem | Cause | Solution |
|---|---|---|
| Cannot reduce tendons into groove | Chronic subluxation, scarring, low-lying muscle belly | Synovectomy, release adhesions, consider groove deepening if shallow |
| SPR tissue quality poor | Chronic injury, attenuated SPR | Augment with local fascia or periosteum, consider reconstruction with graft |
| Tendon repair gaps with ankle motion | Over-tensioned repair, insufficient tendon substance | Release tension, consider tenodesis instead of primary repair |
| Sural nerve injury recognized intraoperatively | Nerve transected during approach | Primary nerve repair with 6-0 or 7-0 nylon under loupe magnification, or bury end in muscle |
| Bleeding from peroneal artery branches | Injury during retraction or groove deepening | Identify vessel, bipolar cautery or tie with 3-0 Vicryl, ensure hemostasis before closure |
Complications
| Complication | Incidence | Risk Factors | Prevention/Management |
|---|---|---|---|
| Sural nerve injury (numbness, neuroma) | 5-10% | Anterior skin incision, rough handling | Posterior incision, identify and protect nerve; If injured: primary repair or bury in muscle |
| Recurrent subluxation | 10-15% overall, 40% if groove deepening alone | SPR not repaired, shallow groove not addressed, Oden Type III | Combine SPR repair with groove deepening; Revision: SPR reconstruction with graft |
| Re-tear of peroneus brevis | 5-10% after repair | Over-tensioned repair, early mobilization, low-lying muscle belly variant | Tension-free repair, protect 4 weeks NWB; Revision: tenodesis if re-tear |
| Wound complications (dehiscence, infection) | 3-5% | Thin subcutaneous tissue, diabetes, smoking | Meticulous hemostasis, gentle handling, elevation; Manage with local wound care, VAC, antibiotics |
| Ankle stiffness, loss of ROM | 5-10% | Prolonged immobilization, adhesions | Early ROM after 4-6 weeks, PT for mobilization; Revision: tenolysis if severe adhesions |
| Peroneal artery injury (rare) | Under 1% | Deep dissection, groove deepening | Identify and ligate or repair; Vascular consult if significant bleeding |
Recurrent Subluxation - Most Common Failure Mode
Recurrent subluxation after SPR repair occurs in 10-15% of cases, higher if groove deepening performed without SPR repair (40% failure). Causes: Inadequate SPR repair tension, failure to address shallow groove (Oden Type III), anchor pullout, chronic tissue attenuation. Prevention: Intraoperative stress testing (dorsiflex-evert ankle, confirm tendons stay reduced), combine SPR repair with groove deepening in Type III patients, use sufficient anchors (2-3) for load distribution. Revision strategy: SPR reconstruction using local tissue (peroneus longus slip) or allograft, consider bone block if severe groove deficiency.
Postoperative Care and Rehabilitation
Postoperative Rehabilitation Timeline
Goals: Protect tendon and SPR repair, prevent subluxation, allow healing.
- Immobilization: Short leg cast or CAM boot, slight plantarflexion-eversion position
- Weight-bearing: Non-weight bearing (NWB) with crutches
- Elevation: Elevate limb above heart level to reduce swelling
- DVT prophylaxis: Low molecular weight heparin or aspirin as per protocol
- Wound care: Dry dressing, suture removal at 2 weeks, check wound healing Rationale: Tendon and SPR repairs require 4-6 weeks for initial healing - loading before this risks failure.
Goals: Gradual loading, restore ankle ROM, begin gentle strengthening.
- Immobilization: Transition to removable CAM boot at week 4
- Weight-bearing: Progressive weight-bearing - 25% week 4, 50% week 5, 75% week 6, full by week 8
- ROM exercises: Gentle ankle plantarflexion-dorsiflexion (avoid eversion initially)
- Strengthening: Isometric ankle exercises, no resistance eversion yet Physiotherapy: Begin formal PT at week 6 - focus on ROM and proprioception.
Goals: Restore peroneal strength, improve proprioception, functional activities.
- Weight-bearing: Full weight-bearing in supportive shoe
- ROM: Full ankle ROM by week 12 (may take longer if stiffness)
- Strengthening: Progressive resistance peroneal exercises - theraband, weights
- Proprioception: Single-leg balance, wobble board, perturbation training
- Functional: Walking progression, elliptical, swimming (no push-off initially)
Goals: Sport-specific training, gradual return to full activity.
- Criteria for progression: Pain-free ADLs, full ROM, 80% strength vs contralateral
- Sport-specific drills: Jogging (week 12-16), cutting drills (week 16-20), plyometrics (week 20-24)
- Bracing: Lace-up ankle brace or taping for initial return to sport
- Return to competition: Typically 5-6 months for contact sports, 4 months for non-contact Red flags: Recurrent subluxation sensation, persistent lateral ankle pain, weakness - consider MRI and specialist review.
Premature Weight-Bearing Risks Repair Failure
Weight-bearing before 4 weeks after tendon or SPR repair significantly increases failure risk. Mechanism: Loading generates tensile stress on repair site before adequate healing, causing gap or rupture. Evidence: Studies show 20-30% re-tear rate with early weight-bearing vs 5-10% with protected weight-bearing. Patient education: Emphasize importance of compliance with NWB protocol - short-term inconvenience for long-term success. Alternative: Consider accelerated protocol only if debridement without repair performed.
Outcomes and Prognosis
| Procedure | Return to Sport | Patient Satisfaction | Re-operation Rate | Key Outcome Factors |
|---|---|---|---|---|
| Acute SPR repair (within 6 weeks) | 90% | 85-90% satisfied | 5-10% | Timing critical - early repair achieves best outcomes |
| Delayed SPR repair or reconstruction | 60-70% | 70-80% satisfied | 15-20% | Tissue quality poor, higher failure rate |
| Peroneus brevis tubularization repair | 80% | 80-85% satisfied | 5-10% re-tear | Tension-free repair, early PT important |
| Tenodesis (brevis to longus) | 60% | 70-75% satisfied | Under 5% revision | Accept some eversion weakness, functional limitation |
Predictors of Poor Outcome
Poor prognostic factors:
- Delayed surgery - Over 6 weeks from acute SPR injury (60% vs 90% return to sport)
- Low-lying muscle belly variant - Recurrent tears common even after repair
- Severe tendon degeneration - Tissue quality poor, repair under tension fails
- Oden Type III with shallow groove - Higher recurrent subluxation if groove not deepened
- Worker's compensation claims - Poorer outcomes regardless of surgical technique
Optimal outcome profile: Young athlete, acute SPR avulsion within 6 weeks, Oden Type I, normal groove anatomy, compliant with rehab protocol - expect over 90% return to pre-injury sport level.
Long-Term Outcomes and Function
Sport-specific return rates:
- Cutting sports (soccer, basketball): 80-85% return to same level, 5-6 months timeline
- Running sports (track, cross-country): 90% return, 4-5 months timeline
- Contact sports (rugby, AFL): 75-80% return, 6-8 months timeline
- Recreational athletes: 90% return, accept lower intensity if needed
Functional limitations after tenodesis:
- Loss of isolated peroneus brevis function (5th metatarsal base eversion)
- Compensated by peroneus longus (preserves overall eversion strength)
- Patients may notice weakness with single-leg lateral push-off
- Generally well-tolerated in non-athletes, recreational athletes accept trade-off
Controversies and Areas of Uncertainty
Where the Evidence Is Weak - Be Ready to Discuss
The entire field rests on Level III-IV case series and a handful of systematic reviews - there are no randomized trials and no registry. State this honestly in a viva.
Imaging - MRI vs Ultrasound
Meta-analysis shows MRI is specific but can be insensitive for peroneal tears (brevis sensitivity around 73 percent, longus around 60 percent), while ultrasound is more sensitive and dynamic (Ghandour 2025). A normal MRI does not exclude a tear in a convincing clinical picture. The "gold standard" label for MRI is therefore qualified - dynamic ultrasound and tendoscopy retain a clear role.
Anatomical Variants - Cause or Coincidence?
The low-lying muscle belly is strongly associated with tears in operative series (Mirmiran 2015, Dombek 2003), but asymptomatic-ankle MRI studies fail to confirm several presumed variant-pathology links (Galli 2015). Whether to routinely debulk a low-lying belly, and which groove shape truly predisposes to subluxation, remain debated.
The 6-Week Window
The threshold for "acute" retinacular repair (commonly cited as 6 weeks) and the magnitude of the early-versus-late difference are based on consensus and small series, not high-level data. The direction (earlier is better) is widely accepted; the precise cut-off and percentages are soft.
Groove Deepening and Repair Choice
Whether to add groove deepening routinely, when SPR reconstruction beats imbrication, autograft versus allograft, and the role of tendoscopic/minimally invasive stabilization are all unresolved. Tendoscopy shows excellent pooled scores but lacks randomized comparison with open surgery (Tham 2025).
Evidence Base and Key Studies
Peroneal Tendon Tears - Pattern of Pathology and Coexisting Lesions
- Retrospective review of 40 patients undergoing peroneal tendon repair (mean age 42 years)
- Peroneus brevis tears in 88%, combined brevis-and-longus tears in 37%
- Low-lying peroneus muscle belly in 33% and lateral ligament incompetence in 33% coexisted
- Most common cause was ankle sprain or other trauma (58%); peroneal subluxation in 20%
- 98% returned to full activity without pain; clinically significant complications in 10%
Diagnostic Accuracy of MRI and Ultrasound for Peroneal Tendon Tears
- Systematic review and meta-analysis, 12 studies (8 MRI, 3 US, 1 both)
- Peroneus brevis tear: MRI pooled sensitivity 73% (95% CI 56-87), specificity 88%
- Peroneus brevis tear: ultrasound pooled sensitivity 93%, specificity 85%
- Peroneus longus tear: MRI sensitivity only 60%, ultrasound sensitivity 94%
- All included studies at high risk of bias; results heterogeneous
Low-Lying Peroneus Brevis Muscle Belly - Prevalence and Association
- 50 consecutive primary peroneal tendon surgeries with MRI-intraoperative correlation
- Low-lying muscle belly seen intraoperatively in 62% of chronic lateral ankle pain patients
- Low-lying belly present in 80.65% of those with a peroneus brevis tear
- MRI sensitivity high for tear (85.71%) but very low for low-lying belly (3.23%) and subluxation (10%)
- 9 of 10 patients with intraoperative subluxation had a concomitant low-lying muscle belly
Peroneal Subluxation - Surgical Results in Athletic Patients
- 31 athletic patients treated for symptomatic subluxating peroneal tendons (single surgeon)
- Mean return to activity 3.2 +/- 0.8 months; postoperative AOFAS 97.0 +/- 5.3
- Patients with concomitant tendon tears were older and took significantly longer to return
- 4 patients had postoperative complications but all returned to sport
- Procedures: isolated retinacular repair, repair plus brevis repair, or plus lateral stabilization
Tenodesis of Peroneus Longus to Brevis for Os Peroneum Pathology
- 12 patients with irreparable peroneus longus tears and os peroneum pathology
- Treated with os peroneum excision, debridement and tenodesis of longus to brevis
- AOFAS hindfoot score improved from 61 to 91.7 at mean 63 months follow-up
- VAS pain fell from 6.3 to 1.0; SF-36 physical component 36 to 52
- Complications: 2 sural neuritis, 3 superficial wound-healing issues (all non-operative)
Peroneal Tendoscopy - Indications, Diagnostic Utility and Outcomes
- Systematic review of 8 studies (190 patients, 195 ankles), mean age 32 years
- Postoperative AOFAS pooled 96.6 with mean gain +19.8; return to sport at 13.3 weeks
- Low complication burden 7.6% and failure rate 1.5% across procedures
- Composite preoperative diagnosis: high specificity 0.97 but moderate sensitivity 0.76
- Low-lying muscle belly frequently under-recognized on preoperative imaging
Diagnosis and Operative Treatment of Peroneal Tendon Tears (Review)
- Narrative review summarizing diagnosis and operative algorithm for peroneal tears
- Limited single-tendon tears: debridement and primary tubularization repair
- Advanced single-tendon tears: excision of non-viable segment and tenodesis to adjacent tendon
- Irreparable tears of both tendons: flexor tendon transfer and/or allograft reconstruction
- Emphasizes that many tears are advanced by the time of surgery, favoring tenodesis
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Acute Peroneal Subluxation in Athlete
"A 24-year-old basketball player presents with acute onset lateral ankle pain after landing from a jump with forced dorsiflexion and eversion. He reports feeling a pop and now has a painful snapping sensation with ankle motion. On examination, you palpate a subluxating structure posterior to the lateral malleolus during dorsiflexion-eversion. What is your assessment and management?"
Scenario 2: Chronic Lateral Ankle Pain - Peroneus Brevis Tear
"A 35-year-old recreational runner presents with 6 months of lateral ankle pain posterior to the malleolus, worse with activity. Multiple physiotherapy sessions have not helped. MRI demonstrates a longitudinal split tear of the peroneus brevis involving 60 percent of the tendon width. Walk me through your surgical approach and technique for this pathology."
Scenario 3: Recurrent Subluxation After Failed SPR Repair
"A 28-year-old footballer underwent SPR repair 18 months ago but has recurrent painful subluxation of the peroneal tendons. MRI shows attenuated SPR tissue and a shallow fibular groove. He wants to return to competitive sport. How do you manage this complex revision case?"
MCQ Practice Points
Anatomy Question
Q: Which peroneal tendon is more commonly torn and why? A: Peroneus brevis is torn in 77 percent of cases. It lies anterior within the fibular groove, directly compressed against the fibula during ankle eversion. This compression generates shear forces on the posterior surface of the tendon, leading to longitudinal splitting. Peroneus longus lies posterior to brevis, protected from direct bony compression, and is less commonly torn (23 percent).
Classification Question
Q: What does the Oden classification for peroneal subluxation guide? A: Oden classification categorizes SPR injury patterns and guides surgical strategy. Type I: Fibular avulsion (acute, primary repair). Type II: Attenuated SPR (imbrication or reconstruction). Type III: Shallow or convex fibular groove (requires groove deepening plus SPR repair). Type IV: Chronic healed SPR (reconstruction). Surgical management must address the specific Oden type - for example, Type III requires combined groove deepening and SPR repair, as groove deepening alone has 40 percent failure rate.
Investigation Question
Q: What is the comma sign on MRI and what does it indicate? A: The comma sign is a pathognomonic finding for peroneus brevis longitudinal split tear. On axial MRI sequences, the retracted edge of the split tendon creates a C-shaped or comma appearance. This represents the posterior portion of the tendon that has split and retracted laterally within the fibular groove. High specificity for split tear diagnosis - when seen, proceed with surgical planning for debridement or repair.
Treatment Question
Q: What is the evidence for timing of acute SPR repair and how does it affect outcomes? A: Acute repair of the superior peroneal retinaculum is favoured over delayed surgery: tissue quality is better and primary reattachment is feasible before retraction and scarring set in. The widely quoted 6-week window is a pragmatic threshold - beyond it, primary repair becomes difficult and reconstruction (groove deepening, retinacular reconstruction, or tendon rerouting) is more often required. Athletic series report high return to sport (AOFAS around 97, return to activity at roughly 3 months) after stabilization of subluxation. Clinical implication: Early diagnosis and referral are essential for optimal outcomes in active patients with acute peroneal subluxation.
Surgical Technique Question
Q: What is the threshold for performing tenodesis versus primary repair of a peroneus brevis tear? A: Grade 1 tears (less than 50 percent tendon width) - debridement only, sufficient tendon remains for function. Grade 2 tears (50-100 percent width, repairable) - tubularization repair with side-to-side sutures. Grade 3 tears (over 50 percent tendon substance loss, severe degeneration) - tenodesis to peroneus longus, as primary repair under tension will fail. Intraoperative decision: Assess tissue quality and remaining tendon substance - if repair gaps with ankle ROM or tension excessive, proceed to tenodesis.
Complications Question
Q: What is the most common complication after peroneal tendon surgery and how is it prevented? A: Sural nerve injury occurs in 5-10 percent of lateral ankle surgeries, causing lateral foot numbness or painful neuroma. Prevention: Skin incision along posterior border of fibula (nerve is 1-2cm anterior), identify nerve early in dissection, retract anteriorly with skin flap, avoid rough handling or traction. If injured: Consider primary nerve repair with microsurgical technique if sharp transection, or bury nerve end in peroneus brevis muscle to prevent symptomatic neuroma formation.
Guidelines, Registries & Global Practice
Global Epidemiology
- Under-recognized: Peroneal pathology is a frequent but missed cause of chronic lateral ankle pain, often labelled "recurrent sprain"
- Acute subluxation/dislocation: Classically in skiers, footballers, basketball and dancers - forced dorsiflexion-eversion
- Coexisting lesions: Low-lying muscle belly (around one third of operated cases) and lateral ligament incompetence are common (Dombek 2003)
- Demographics: Acute subluxation in young athletes (20-40); degenerative splits in older, lower-demand patients
Diagnostic Practice
- No dedicated society guideline exists specifically for peroneal tendon disorders; practice is driven by case series and expert review
- Imaging consensus: MRI is specific but can be insensitive (especially for longus tears); dynamic ultrasound is sensitive and shows subluxation in real time (Ghandour 2025)
- Tendoscopy: Increasingly used as a diagnostic-therapeutic adjunct where MRI is equivocal (Tham 2025)
Society and Expert Guidance - Side by Side
| Body / Source | Emphasis | Position on Imaging | Position on Surgery |
|---|---|---|---|
| AAOS / AOFAS (US) review consensus | Reparable vs irreparable framework | MRI first-line, US for dynamic subluxation | Repair single salvageable tendon; tenodese to adjacent tendon if irreparable; reconstruct if both lost |
| BOA / BOFAS (UK) practice | Exclude mimics, structured non-operative trial first | MRI for persistent lateral ankle pain after failed rehab | Surgery for failed conservative care or mechanical subluxation |
| AO Foundation (trauma context) | Recognize subluxation with distal fibula fractures | CT for groove/bony anatomy, MRI for tendon | Acute retinacular repair when fracture fixation undertaken |
| EFORT / European expert reviews | Address all components (tendon, retinaculum, groove) | Ultrasound widely used as first-line in many centres | Combine groove deepening with retinacular repair for groove deficiency |
Registry and Evidence Notes
- No arthroplasty-style registry captures peroneal tendon surgery; the evidence base is Level III-IV case series and a small number of systematic reviews
- Best pooled data: tendoscopy series report AOFAS around 96 and return to sport near 13 weeks with low failure rates (Tham 2025); open athletic series report AOFAS around 97 and return at roughly 3 months (Saxena 2010)
- Practice variation: high-resource centres increasingly favour tendoscopic/minimally invasive techniques and dynamic ultrasound, while diagnosis elsewhere still relies on clinical examination plus MRI where available
High- vs Limited-Resource Practice
- High-resource: MRI plus dynamic ultrasound, tendoscopy, suture-anchor retinacular repair, allograft reconstruction available; structured supervised rehabilitation
- Limited-resource: diagnosis rests on careful examination (subluxation test, focal tenderness) with selective imaging; open repair, groove deepening and local tendon transfer (e.g. tenodesis to peroneus longus) are durable, low-cost options that avoid graft cost and availability problems
- Universal principles: early treatment of acute retinacular injury, tension-free repair, protect the repair before loading, and address coexisting lateral ligament instability
Avoiding Delayed Diagnosis - A Global Pitfall
Peroneal tendon pathology is commonly mistaken for a chronic ankle sprain, delaying effective treatment worldwide. Reduce this risk by:
- Documenting findings that distinguish peroneal pathology from ATFL injury (tenderness posterior to the malleolus, positive subluxation test)
- Imaging (MRI or dynamic ultrasound) when symptoms persist beyond 6 weeks despite rehabilitation for a presumed sprain
- Keeping a broad differential for chronic lateral ankle pain (ATFL instability, sinus tarsi syndrome, osteochondral lesion, peroneal pathology)
- Referring to a foot and ankle specialist if structured non-operative care fails at 3 months
PERONEAL TENDON DISORDERS
Clinical summary
Key Anatomy
- •Peroneus brevis = anterior in groove, inserts 5th metatarsal base, torn 77% of cases
- •Peroneus longus = posterior, inserts 1st metatarsal/medial cuneiform, torn 23%
- •Superior peroneal retinaculum (SPR) = lateral fibular ridge to calcaneus, prevents subluxation
- •Fibular groove = retrofibular, 1cm wide, 2-3mm deep (shallow if less than 2mm = Oden Type III)
- •Low-lying muscle belly variant = 15-20% prevalence, doubles tear risk, extends into groove
- •Sural nerve = 1-2cm anterior to posterior fibular border, at-risk in lateral approach
Classification
- •Peroneus brevis tears: Grade 1 (under 50% width) = debridement, Grade 2 (50-100% repairable) = tubularization, Grade 3 (over 50% loss) = tenodesis
- •Oden Type I = SPR fibular avulsion (acute, primary repair)
- •Oden Type II = SPR attenuated (imbrication or reconstruction)
- •Oden Type III = shallow/convex groove (deepening + SPR repair)
- •Oden Type IV = chronic scarred SPR (reconstruction)
- •Comma sign on MRI = retracted split tendon edge, pathognomonic for longitudinal tear
Treatment Algorithm
- •Acute SPR avulsion (within 6 weeks) = open SPR repair with suture anchors (90% return to sport)
- •Delayed SPR injury (after 6 weeks) = SPR reconstruction with autograft or allograft (60% return)
- •Grade 1 brevis tear = debridement, synovectomy (90% return, accelerated rehab possible)
- •Grade 2 brevis tear = tubularization repair with 2-0 FiberWire (80% good outcomes)
- •Grade 3 irreparable tear = tenodesis to longus (60% return, accept eversion weakness)
- •Oden Type III = combine groove deepening (2-3mm bone removal) + SPR repair (never alone)
Surgical Pearls
- •Lateral approach = posterior fibular border incision, protect sural nerve anteriorly
- •Tension-free repair = test with ankle ROM, must not gap or restrict motion
- •Groove deepening = remove 2-3mm cortical bone, preserve lateral ridge for SPR
- •SPR repair = 2-3 suture anchors to fibular ridge, tie with ankle in neutral-slight plantarflexion
- •Postop protocol = 4 weeks NWB in cast (slight plantarflexion-eversion), then progressive WB
- •Return to sport = 5-6 months for SPR repair, 4-5 months for tendon repair alone
Complications
- •Sural nerve injury = 5-10% (numbness, neuroma), prevent with posterior incision and early identification
- •Recurrent subluxation = 10-15% overall, 40% if groove deepening without SPR repair
- •Re-tear of brevis = 5-10% after repair (higher if low-lying muscle belly or over-tensioned)
- •Wound complications = 3-5% (thin subcutaneous tissue), manage with local care, VAC, antibiotics
- •Ankle stiffness = 5-10%, prevent with early ROM after 4-6 weeks, aggressive PT
- •Revision surgery needed = 10-15%, lower success rate (70-80% vs 90% primary)