FDG-PET for staging, response assessment and recurrence in bone and soft tissue tumours
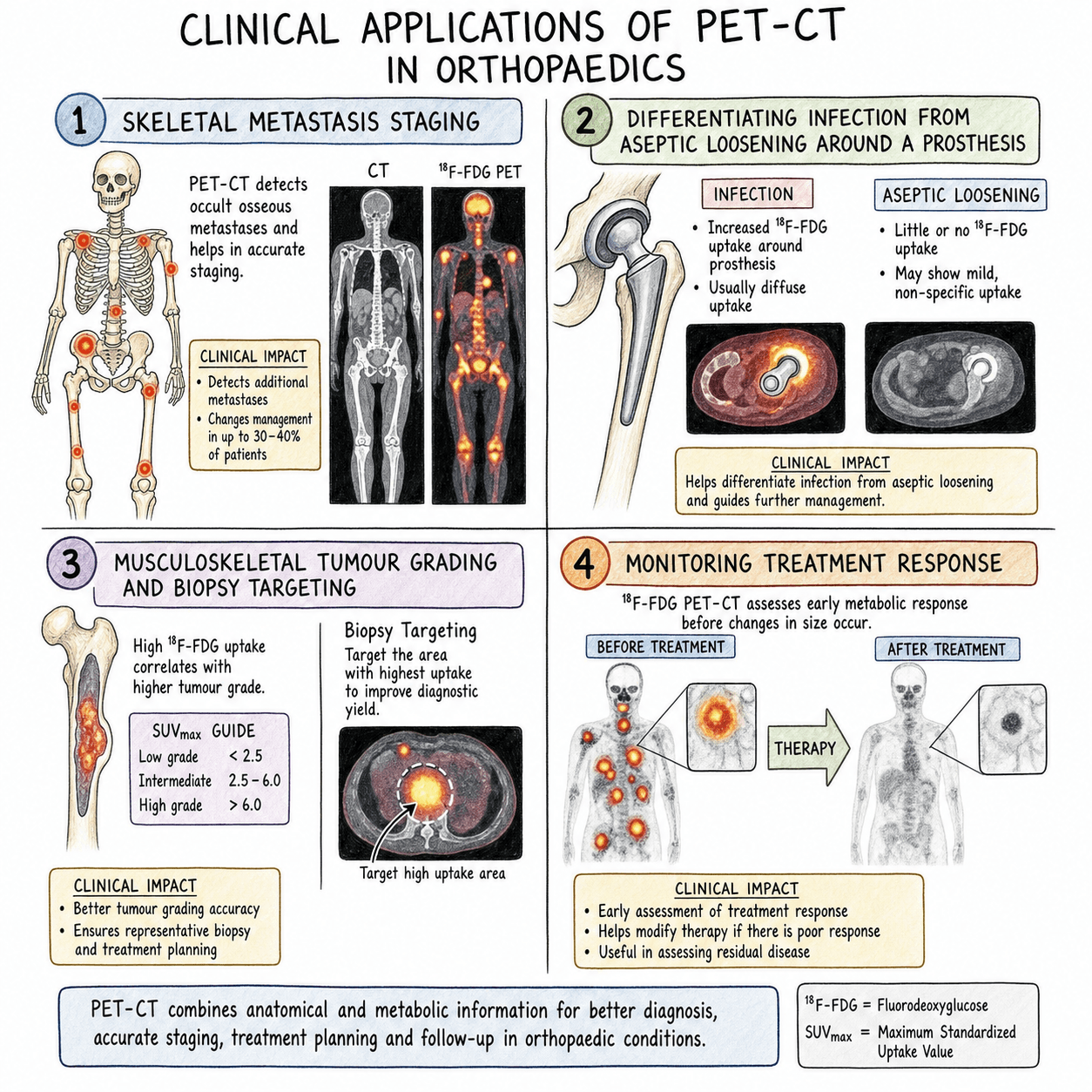
Staging: Whole body assessment for metastases
Response: Pre and post-treatment comparison
Recurrence: Detection of local or distant relapse
Biopsy guidance: Target metabolically active areas
Key: PET-CT is most valuable for high-grade malignancies and systemic staging
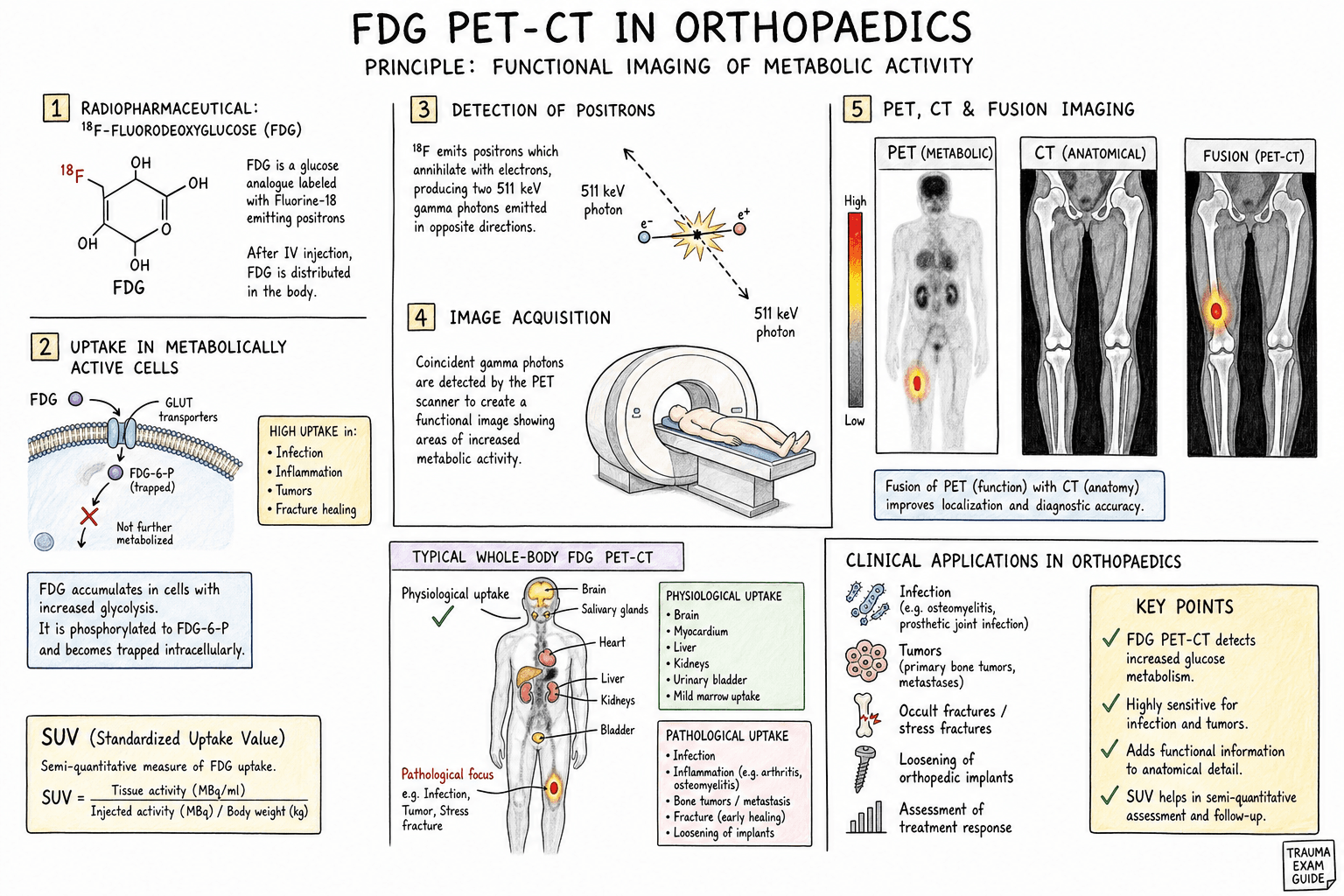
- FDG uptake reflects glucose metabolism (Warburg effect)
- High-grade tumours show higher FDG uptake than low-grade
- SUVmax is quantitative measure of uptake intensity
- PET-CT combines metabolic and anatomic information
- Used for staging, response assessment, and recurrence detection
- “Brain has high physiological FDG uptake (limits assessment)
- “Blood glucose must be controlled (less than 11 mmol/L)
- “False positives: infection, inflammation, recent surgery
- “Response: greater than 40% SUV decrease = metabolic response
- “Low-grade sarcomas may have minimal FDG uptake
PET-CT is increasingly used in orthopaedic oncology. Know that FDG uptake reflects glucose metabolism, not malignancy directly. Understand the indications (staging, response, recurrence) and limitations (false positives with infection/inflammation, low sensitivity for low-grade tumours).
FDG-PET Principles
| Step | Timing | Requirements |
|---|---|---|
| Patient preparation | 4-6 hours fasting | Blood glucose less than 11 mmol/L |
| FDG injection | Time 0 | 4-5 MBq/kg IV |
| Uptake period | 60 minutes | Rest, avoid talking/chewing |
| PET acquisition | 60 minutes post-injection | Whole body or regional |
| CT acquisition | Simultaneous or sequential | Low-dose for attenuation/localisation |
SUV = Standardised Uptake ValueSUV Interpretation
Hook:SUV is affected by blood glucose level, body habitus, and timing - standardise conditions for response assessment
FIB GRABCauses of False-Positive FDG Uptake
Hook:Always correlate FDG uptake with history and CT/MRI morphology - metabolic activity is not specific for malignancy
Indications in Orthopaedic Oncology
| Tumour Type | Role of PET-CT | Notes |
|---|---|---|
| Osteosarcoma | Detect lung/distant metastases, skip lesions | Complements bone scan, CT chest |
| Ewing sarcoma | Systemic staging, marrow involvement | Very FDG-avid |
| Soft tissue sarcoma | Stage high-grade lesions, detect nodal/distant disease | Low-grade may not be FDG-avid |
| Chondrosarcoma | Grade assessment, dedifferentiation | Low-grade shows low uptake |
| Metastatic disease | Whole body survey, unknown primary | Complementary to bone scan |
Specific Tumour Applications
| Tumour | FDG Avidity | Clinical Implications |
|---|---|---|
| Osteosarcoma | High | SUV correlates with histological response |
| Ewing sarcoma | Very high | Excellent for staging and response |
| High-grade STS | High | SUV predicts grade and outcome |
| Low-grade STS | Low to moderate | May not be reliably detected |
| Chondrosarcoma G1 | Low | Difficult to differentiate from enchondroma |
| Chondrosarcoma G2-3 | Moderate to high | Increased uptake suggests higher grade |
| GCT | Variable | Not reliably FDG-avid |
| Myeloma | Variable | FDG-PET useful for treatment response |
Limitations and Pitfalls
| Category | Cause | Mitigation |
|---|---|---|
| False positive | Infection/inflammation | Clinical correlation, follow-up |
| False positive | Recent surgery/biopsy | Wait 4-6 weeks post-procedure |
| False positive | Fracture healing | Correlate with history |
| False positive | Brown fat uptake | Patient warming, beta-blockers |
| False negative | Low-grade tumour | Limited sensitivity, MRI better |
| False negative | Small lesions (less than 1cm) | Resolution limits |
| False negative | Hyperglycaemia | Control glucose, repeat if needed |
Comparison with Other Modalities
| Feature | Bone Scan | PET-CT | MRI |
|---|---|---|---|
| Mechanism | Osteoblast activity | Glucose metabolism | Tissue characterisation |
| Whole body | Yes | Yes | Limited (WB-MRI emerging) |
| Anatomic detail | Poor | Good (CT component) | Excellent |
| Lytic metastases | May be cold | Usually positive | Positive (marrow) |
| Soft tissue | Limited | Good | Excellent |
| Response assessment | Limited | Good (SUV) | Moderate |
| Availability | Widely available | Limited centres | Widely available |
| Cost | Lower | Higher | Moderate |
| Entity | Typical SUVmax / Pattern | Discriminating Features |
|---|---|---|
| High-grade sarcoma | High (often greater than 6), focal intense | Soft tissue mass, cortical destruction, growth on serial imaging |
| Low-grade sarcoma / atypical lipomatous tumour | Low to moderate (often under 3) | May be PET-negative; MRI fat signal, slow growth |
| Infection / osteomyelitis / septic arthritis | Moderate to high, can mimic tumour | Clinical signs, raised inflammatory markers, marrow oedema, rim enhancement |
| Post-surgical / post-biopsy inflammation | Diffuse, linear uptake along tract | History; resolves over weeks (wait 4 to 6 weeks before imaging) |
| Fracture / healing callus | Moderate fusiform uptake at fracture line | History of trauma, fracture line on CT, settles with time |
| Brown fat (supraclavicular, paraspinal) | Symmetric, CT-negative fat density | Patient warming and benzodiazepine/beta-blocker reduce uptake |
| Reactive / inflammatory lymph node | Mild to moderate, oval, fatty hilum | Preserved hilum; biopsy if discordant with primary |
| Benign bone lesion (GCT, fibrous dysplasia, osteoid osteoma) | Variable, can be markedly FDG-avid | Characteristic CT/MRI morphology prevents over-call of malignancy |
Controversies & Areas of Uncertainty
Evidence
PERCIST 1.0: standardised metabolic response criteria
- Practical guide to PET Response Criteria in Solid Tumors (PERCIST 1.0), defining quality control needed to compare FDG-PET across time points.
- Response is measured using SUL peak (lean-body-mass corrected) in a reference lesion, not raw SUVmax, to reduce variability.
- Defines complete, partial, stable and progressive metabolic disease and clarifies measurement of unequivocal progression.
FDG-PET correlates with histological necrosis in osteosarcoma
- 11 osteosarcoma patients had FDG-PET before and after neoadjuvant chemotherapy correlated with histological necrosis.
- Post-chemotherapy SUV (SUV2) was much lower in good responders (mean 1.93) than poor responders (5.86); change in tumour size on MRI did not correlate with response.
- An SUV2 under 2.5 had 100% positive and negative predictive value for good histological response in this small series.
Baseline tumour SUV predicts response and survival in bone sarcoma
- 77 patients with localised Ewing sarcoma (45) and osteosarcoma (32) staged with FDG-PET/CT.
- Lower baseline SUVmax (under 6) predicted a higher good-response rate (72% vs 30% in Ewing; 64% vs 29% in osteosarcoma).
- Baseline SUVmax was the only independent pre-treatment prognostic factor for event-free survival on multivariate analysis.
SUVmax stratifies grade and prognosis in soft tissue sarcoma
- 50 adults with primary high-grade extremity soft tissue sarcoma and preoperative FDG-PET; mean SUVmax 12.9 (range 2.2 to 33.4).
- Lower SUVmax (under 10.3) was associated with better overall survival and lower local recurrence.
- Myxoid liposarcoma and synovial sarcoma were consistently low-uptake, limiting PET sensitivity in these subtypes.
FDG-PET differentiates benign from malignant chondroid tumours
- Systematic review of 8 studies and 166 chondroid lesions correlating SUVmax with histological grade.
- Mean SUVmax was lower for benign (1.6) than malignant (4.4) lesions and rose with grade (grade 0/1 = 2.0 vs grade 2/3 = 6.0).
- An SUVmax of 4.4 or greater was 99% specific for grade 2/3 chondrosarcoma.
Meta-analysis: PET/CT accuracy in chondrosarcoma diagnosis and grading
- Meta-analysis of 12 studies evaluating FDG-PET/CT for chondrosarcoma diagnosis and grading.
- Pooled PET/CT sensitivity 0.94 and specificity 0.89 for diagnosing chondrosarcoma.
- SUVmax separated low- from intermediate/high-grade chondrosarcoma but was limited at the benign-vs-G1 and G2-vs-G3 boundaries.
FDG-PET/CT outperforms bone scintigraphy for skeletal metastases in paediatric sarcoma
- Review of FDG-PET/CT in paediatric osteosarcoma, Ewing sarcoma and rhabdomyosarcoma.
- PET/CT has consistently better sensitivity and specificity than bone scintigraphy for detecting skeletal metastases.
- Its value for pulmonary metastases is limited (CT chest remains superior for small lung nodules) and its prognostic role outside osteosarcoma is unproven.
Guidelines, Registries & Global Practice
| Body | Position on FDG-PET/CT | Practical Point |
|---|---|---|
| NCCN (US) | Recommended for staging high-grade STS and bone sarcoma; option for restaging and equivocal recurrence | CT chest still required for lung metastases |
| ESMO / EURACAN (Europe) | PET-CT may aid staging, grading and response assessment in selected sarcomas | Emphasises management within sarcoma reference centres |
| NICE / BSG (UK) | Reserved for problem-solving; not routine surveillance | MRI primary site plus CT chest remain core staging |
| RCR / EANM (imaging societies) | Standardised acquisition and PERCIST-style reporting encouraged | Fasting, glucose control, fixed uptake time mandatory |
| SIOP / COG (paediatric) | Increasing use for skeletal staging in Ewing and osteosarcoma | Preferred over bone scan for marrow/bone disease |
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 16-year-old with newly diagnosed osteosarcoma of the distal femur is being staged. The oncologist requests PET-CT.”
“A patient with known high-grade soft tissue sarcoma of the thigh has PET-CT showing intense uptake in the primary tumour (SUVmax 12) and a 1.5cm inguinal lymph node with SUVmax 4.”
“A patient with a cartilage tumour in the proximal humerus has PET-CT. The lesion shows SUVmax of 3.5.”
FDG-PET Principles
- FDG = Fluorodeoxyglucose (glucose analogue)
- Warburg effect: Tumours use glycolysis
- Higher grade = higher SUV generally
- SUVmax = maximum standardised uptake value
Indications
- Staging: Metastases, skip lesions
- Response: SUV decrease greater than 30-40%
- Recurrence: Symptomatic patients
- Biopsy guidance: Target active areas
FDG Avidity by Tumour
- High: Osteosarcoma, Ewing, high-grade STS
- Variable: Chondrosarcoma (grade-dependent)
- Low: Low-grade STS, enchondroma
Limitations
- False +: Infection, inflammation, surgery
- False -: Low-grade tumours, small lesions
- Glucose control essential
- Cannot replace biopsy for diagnosis