FDG-PET for staging, response assessment and recurrence in bone and soft tissue tumours
Staging: Whole body assessment for metastases
Response: Pre and post-treatment comparison
Recurrence: Detection of local or distant relapse
Biopsy guidance: Target metabolically active areas
Key: PET-CT is most valuable for high-grade malignancies and systemic staging
- FDG uptake reflects glucose metabolism (Warburg effect)
- High-grade tumours show higher FDG uptake than low-grade
- SUVmax is quantitative measure of uptake intensity
- PET-CT combines metabolic and anatomic information
- Used for staging, response assessment, and recurrence detection
- “Brain has high physiological FDG uptake (limits assessment)
- “Blood glucose must be controlled (less than 11 mmol/L)
- “False positives: infection, inflammation, recent surgery
- “Response: greater than 40% SUV decrease = metabolic response
- “Low-grade sarcomas may have minimal FDG uptake
PET-CT is increasingly used in orthopaedic oncology. Know that FDG uptake reflects glucose metabolism, not malignancy directly. Understand the indications (staging, response, recurrence) and limitations (false positives with infection/inflammation, low sensitivity for low-grade tumours).
FDG-PET Principles
- Timing
- 4-6 hours fasting
- Requirements
- Blood glucose less than 11 mmol/L
- Timing
- Time 0
- Requirements
- 4-5 MBq/kg IV
- Timing
- 60 minutes
- Requirements
- Rest, avoid talking/chewing
- Timing
- 60 minutes post-injection
- Requirements
- Whole body or regional
- Timing
- Simultaneous or sequential
- Requirements
- Low-dose for attenuation/localisation
SUV = Standardised Uptake ValueSUV Interpretation
Hook:SUV is affected by blood glucose level, body habitus, and timing - standardise conditions for response assessment
FIB GRABCauses of False-Positive FDG Uptake
Hook:Always correlate FDG uptake with history and CT/MRI morphology - metabolic activity is not specific for malignancy
Indications in Orthopaedic Oncology
- Role of PET-CT
- Detect lung/distant metastases, skip lesions
- Notes
- Complements bone scan, CT chest
- Role of PET-CT
- Systemic staging, marrow involvement
- Notes
- Very FDG-avid
- Role of PET-CT
- Stage high-grade lesions, detect nodal/distant disease
- Notes
- Low-grade may not be FDG-avid
- Role of PET-CT
- Grade assessment, dedifferentiation
- Notes
- Low-grade shows low uptake
- Role of PET-CT
- Whole body survey, unknown primary
- Notes
- Complementary to bone scan
Specific Tumour Applications
- FDG Avidity
- High
- Clinical Implications
- SUV correlates with histological response
- FDG Avidity
- Very high
- Clinical Implications
- Excellent for staging and response
- FDG Avidity
- High
- Clinical Implications
- SUV predicts grade and outcome
- FDG Avidity
- Low to moderate
- Clinical Implications
- May not be reliably detected
- FDG Avidity
- Low
- Clinical Implications
- Difficult to differentiate from enchondroma
- FDG Avidity
- Moderate to high
- Clinical Implications
- Increased uptake suggests higher grade
- FDG Avidity
- Variable
- Clinical Implications
- Not reliably FDG-avid
- FDG Avidity
- Variable
- Clinical Implications
- FDG-PET useful for treatment response
Limitations and Pitfalls
- Cause
- Infection/inflammation
- Mitigation
- Clinical correlation, follow-up
- Cause
- Recent surgery/biopsy
- Mitigation
- Wait 4-6 weeks post-procedure
- Cause
- Fracture healing
- Mitigation
- Correlate with history
- Cause
- Brown fat uptake
- Mitigation
- Patient warming, beta-blockers
- Cause
- Low-grade tumour
- Mitigation
- Limited sensitivity, MRI better
- Cause
- Small lesions (less than 1cm)
- Mitigation
- Resolution limits
- Cause
- Hyperglycaemia
- Mitigation
- Control glucose, repeat if needed
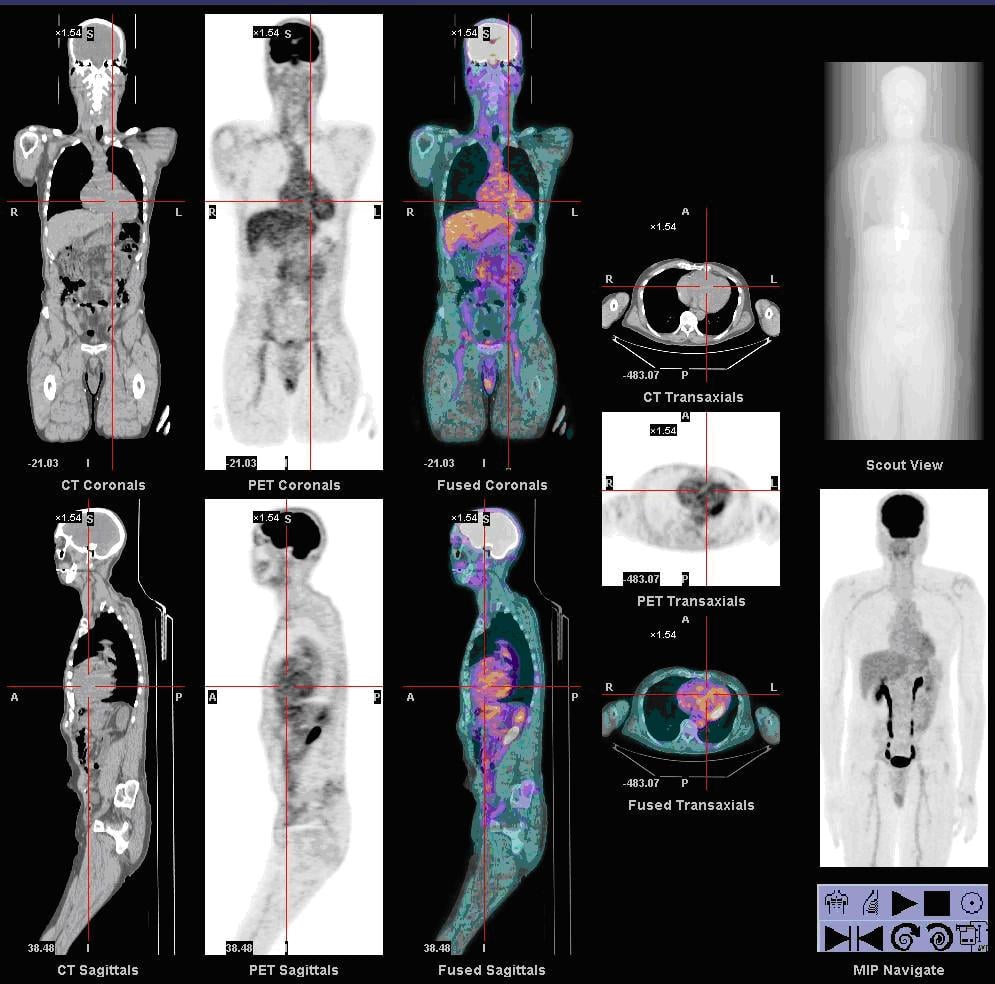
Normal Physiological FDG Biodistribution
The topic notes that the brain is intensely FDG-avid, that brown fat causes false positives, and that the protocol requires fasting and "avoiding talking/chewing" — all of which are consequences of where FDG normally goes. Reading a PET means judging pathology against this normal background, so it is worth setting out.
- Brain — an obligate glucose user, so it is the most FDG-avid normal tissue; this limits the assessment of intracranial lesions.
- Myocardium — variable depending on the fasting state (a prolonged fast and a low-carbohydrate/high-fat preparation can suppress it).
- Liver and blood pool — moderate, relatively uniform uptake; the liver is the standard internal reference background against which lesions and response are judged (PERCIST).
- FDG is renally excreted (unlike natural glucose, which is reabsorbed), so the kidneys, ureters and bladder are intensely active. This urinary activity can obscure lesions in the pelvis and bony pelvis — hydration and bladder emptying before imaging help.
-
Skeletal muscle if recently exercised (hence rest before and after injection), larynx/vocal cords if talking (hence "avoid talking"), and bowel (variable).
-
Brown adipose tissue — symmetric supraclavicular, paraspinal and mediastinal uptake that is fat-density (CT-negative); reduced by keeping the patient warm and by beta-blockade. Do not mistake it for nodal disease.
-
Bone marrow — mild physiological uptake that is diffusely increased after G-CSF or marrow recovery from chemotherapy, which can both mimic and mask marrow disease in the very sarcoma patients being imaged.
Reading Against the BackgroundJudge a lesion against the normal liver/blood-pool background. Remember FDG is renally excreted, so intense urinary activity can hide pelvic disease. Symmetric supraclavicular/paraspinal uptake is brown fat, not nodal disease, and diffuse marrow uptake after G-CSF or chemotherapy is reactive - correlate before calling marrow metastases.
Comparison with Other Modalities
- Bone Scan
- Osteoblast activity
- PET-CT
- Glucose metabolism
- MRI
- Tissue characterisation
- Bone Scan
- Yes
- PET-CT
- Yes
- MRI
- Limited (WB-MRI emerging)
- Bone Scan
- Poor
- PET-CT
- Good (CT component)
- MRI
- Excellent
- Bone Scan
- May be cold
- PET-CT
- Usually positive
- MRI
- Positive (marrow)
- Bone Scan
- Limited
- PET-CT
- Good
- MRI
- Excellent
- Bone Scan
- Limited
- PET-CT
- Good (SUV)
- MRI
- Moderate
- Bone Scan
- Widely available
- PET-CT
- Limited centres
- MRI
- Widely available
- Bone Scan
- Lower
- PET-CT
- Higher
- MRI
- Moderate
- Typical SUVmax / Pattern
- High (often greater than 6), focal intense
- Discriminating Features
- Soft tissue mass, cortical destruction, growth on serial imaging
- Typical SUVmax / Pattern
- Low to moderate (often under 3)
- Discriminating Features
- May be PET-negative; MRI fat signal, slow growth
- Typical SUVmax / Pattern
- Moderate to high, can mimic tumour
- Discriminating Features
- Clinical signs, raised inflammatory markers, marrow oedema, rim enhancement
- Typical SUVmax / Pattern
- Diffuse, linear uptake along tract
- Discriminating Features
- History; resolves over weeks (wait 4 to 6 weeks before imaging)
- Typical SUVmax / Pattern
- Moderate fusiform uptake at fracture line
- Discriminating Features
- History of trauma, fracture line on CT, settles with time
- Typical SUVmax / Pattern
- Symmetric, CT-negative fat density
- Discriminating Features
- Patient warming and benzodiazepine/beta-blocker reduce uptake
- Typical SUVmax / Pattern
- Mild to moderate, oval, fatty hilum
- Discriminating Features
- Preserved hilum; biopsy if discordant with primary
- Typical SUVmax / Pattern
- Variable, can be markedly FDG-avid
- Discriminating Features
- Characteristic CT/MRI morphology prevents over-call of malignancy
Guidelines, Registries & Global Practice
- Position on FDG-PET/CT
- Recommended for staging high-grade STS and bone sarcoma; option for restaging and equivocal recurrence
- Practical Point
- CT chest still required for lung metastases
- Position on FDG-PET/CT
- PET-CT may aid staging, grading and response assessment in selected sarcomas
- Practical Point
- Emphasises management within sarcoma reference centres
- Position on FDG-PET/CT
- Reserved for problem-solving; not routine surveillance
- Practical Point
- MRI primary site plus CT chest remain core staging
- Position on FDG-PET/CT
- Standardised acquisition and PERCIST-style reporting encouraged
- Practical Point
- Fasting, glucose control, fixed uptake time mandatory
- Position on FDG-PET/CT
- Increasing use for skeletal staging in Ewing and osteosarcoma
- Practical Point
- Preferred over bone scan for marrow/bone disease
What SUV Actually Is (and Why There Is No Universal Cut-off)
SUV is quoted throughout this topic (a "2.5 cut-off," SUVmax, SUVmean, and PERCIST's "SUL peak"), and a whole controversy turns on there being "no universal cut-off" — so it is worth defining what the number actually is.
Definition. The standardised uptake value is a semi-quantitative, dimensionless ratio that normalises the FDG activity concentration measured in a region to the injected dose and the patient's size: SUV = tissue activity concentration (e.g. MBq/mL) divided by [injected dose (MBq) / body weight (g)]. In effect it asks "how much brighter is this lesion than it would be if the tracer were spread evenly through the body?" It is a stand-in for metabolic rate, not a direct measurement of malignancy.
The common variants:
- What it measures
- The single hottest voxel in the region
- Strength / weakness
- Most reproducible and most reported; but sensitive to image noise (one bright voxel)
- What it measures
- The average across a drawn region of interest
- Strength / weakness
- Less noisy, but depends heavily on how the ROI is contoured
- What it measures
- A fixed ~1 cm3 volume around the hottest area, normalised to LEAN body mass
- Strength / weakness
- The PERCIST metric — chosen because lean-mass normalisation and a fixed volume make it the most reproducible for response assessment
Why a single threshold cannot be transferred. Absolute SUV is not comparable between centres or time points because it depends on blood glucose (high glucose competes with FDG and lowers tumour SUV), uptake time (SUV keeps rising for an hour or more, so the scan delay must be fixed), body habitus / lean mass (fat dilutes weight-based SUV — hence SUL), scanner model and reconstruction algorithm, and the partial-volume effect (lesions below roughly twice the scanner resolution falsely read low). This is exactly why a number like 2.5 cannot reliably separate benign from malignant across all settings, and why PERCIST mandates tightly controlled, identical conditions and uses the normal liver (or blood pool) as an internal reference for response. (The general physics of PET acquisition is developed in the nuclear-medicine-orthopaedics topic.)
Controversies & Areas of Uncertainty
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 16-year-old with newly diagnosed osteosarcoma of the distal femur is being staged. The oncologist requests PET-CT.”
“A patient with known high-grade soft tissue sarcoma of the thigh has PET-CT showing intense uptake in the primary tumour (SUVmax 12) and a 1.5cm inguinal lymph node with SUVmax 4.”
“A patient with a cartilage tumour in the proximal humerus has PET-CT. The lesion shows SUVmax of 3.5.”
FDG-PET Principles
- FDG = Fluorodeoxyglucose (glucose analogue)
- Warburg effect: Tumours use glycolysis
- Higher grade = higher SUV generally
- SUVmax = maximum standardised uptake value
Indications
- Staging: Metastases, skip lesions
- Response: SUV decrease greater than 30-40%
- Recurrence: Symptomatic patients
- Biopsy guidance: Target active areas
FDG Avidity by Tumour
- High: Osteosarcoma, Ewing, high-grade STS
- Variable: Chondrosarcoma (grade-dependent)
- Low: Low-grade STS, enchondroma
Limitations
- False +: Infection, inflammation, surgery
- False -: Low-grade tumours, small lesions
- Glucose control essential
- Cannot replace biopsy for diagnosis
Evidence
PERCIST 1.0: standardised metabolic response criteria
- Practical guide to PET Response Criteria in Solid Tumors (PERCIST 1.0), defining quality control needed to compare FDG-PET across time points.
- Response is measured using SUL peak (lean-body-mass corrected) in a reference lesion, not raw SUVmax, to reduce variability.
- Defines complete, partial, stable and progressive metabolic disease and clarifies measurement of unequivocal progression.
FDG-PET correlates with histological necrosis in osteosarcoma
- 11 osteosarcoma patients had FDG-PET around neoadjuvant chemotherapy (9 imaged both before and after) correlated with histological necrosis.
- Post-chemotherapy SUV (SUV2) was much lower in good responders (mean 1.93) than poor responders (5.86); change in tumour size on MRI did not correlate with response.
- An SUV2 under 2.5 had 100% positive and negative predictive value for good histological response in this small series.
Baseline tumour SUV predicts response and survival in bone sarcoma
- 77 patients with localised Ewing sarcoma (45) and osteosarcoma (32) staged with FDG-PET/CT.
- Lower baseline SUVmax (under 6) predicted a higher good-response rate (72% vs 30% in Ewing; 64% vs 29% in osteosarcoma).
- Baseline SUVmax was the only independent pre-treatment prognostic factor for event-free survival on multivariate analysis.
SUVmax stratifies grade and prognosis in soft tissue sarcoma
- 50 adults with primary high-grade extremity soft tissue sarcoma and preoperative FDG-PET; mean SUVmax 12.9 (range 2.2 to 33.4).
- Lower SUVmax (under 10.3) was associated with better overall survival and lower local recurrence.
- Myxoid liposarcoma and synovial sarcoma were consistently low-uptake, limiting PET sensitivity in these subtypes.
FDG-PET differentiates benign from malignant chondroid tumours
- Systematic review of 8 studies and 166 chondroid lesions correlating SUVmax with histological grade.
- Mean SUVmax was lower for benign (1.6) than malignant (4.4) lesions and rose with grade (grade 0/1 = 2.0 vs grade 2/3 = 6.0).
- An SUVmax of 4.4 or greater was 99% specific for grade 2/3 chondrosarcoma.
Meta-analysis: PET/CT accuracy in chondrosarcoma diagnosis and grading
- Meta-analysis of 12 studies evaluating FDG-PET/CT for chondrosarcoma diagnosis and grading.
- Pooled PET/CT sensitivity 0.94 and specificity 0.89 for diagnosing chondrosarcoma.
- SUVmax separated low- from intermediate/high-grade chondrosarcoma but was limited at the benign-vs-G1 and G2-vs-G3 boundaries.
FDG-PET/CT outperforms bone scintigraphy for skeletal metastases in paediatric sarcoma
- Review of FDG-PET/CT in paediatric osteosarcoma, Ewing sarcoma and rhabdomyosarcoma.
- PET/CT has consistently better sensitivity and specificity than bone scintigraphy for detecting skeletal metastases.
- Its value for pulmonary metastases is limited (CT chest remains superior for small lung nodules) and its prognostic role outside osteosarcoma is unproven.