Imaging patients with orthopaedic hardware
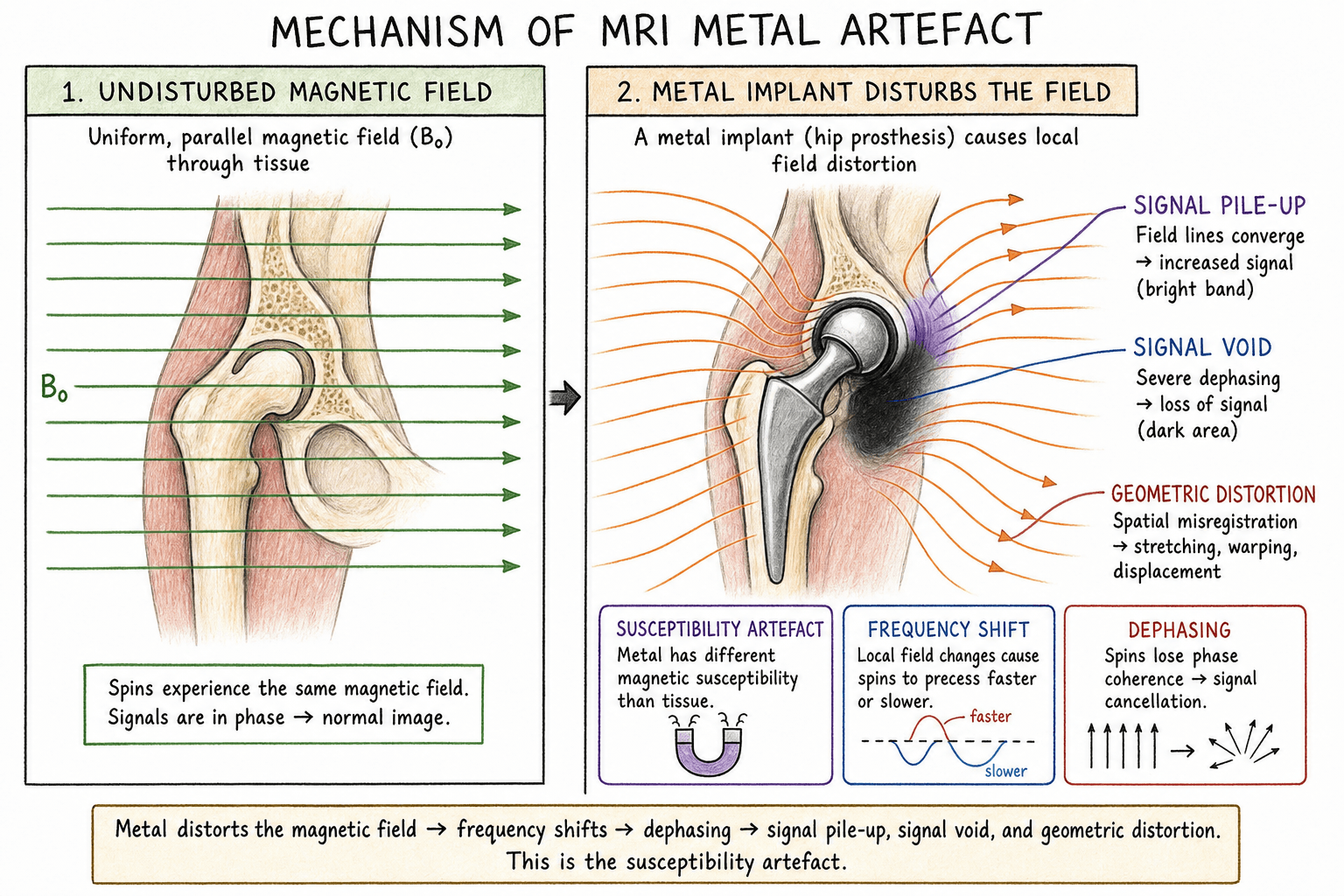
Susceptibility: Different magnetic properties cause local field distortion
Signal void: No signal from metal itself
Geometric distortion: Spatial mismapping of signal
Pile-up artefact: Signal displaced and concentrated
Key: MARS techniques address susceptibility and geometric distortion
- Metal artefact = signal void + geometric distortion
- Titanium causes less artefact than stainless steel or cobalt-chrome
- 1.5T preferred over 3T for metal artefact reduction
- MARS sequences: SEMAC, MAVRIC, VAT (View Angle Tilting)
- Increase bandwidth, use spin echo over gradient echo
- “Susceptibility artefact proportional to field strength
- “Stainless steel: 10x more artefact than titanium
- “Short tau inversion recovery (STIR) better than fat-sat near metal
- “Thinner slices and higher matrix reduce artefact
- “ALTR assessment around MoM hips requires MARS MRI
Understanding metal artefact reduction is increasingly important with the rising number of patients with orthopaedic implants. Know which materials cause most artefact (stainless steel worst), why 1.5T is preferred, and the basic MARS techniques. ALTR assessment around metal-on-metal hips is a common application.
Physics of Metal Artefact
| Artefact Type | Cause | Appearance |
|---|---|---|
| Signal void | No mobile protons in metal | Black region at metal location |
| Susceptibility artefact | Local field inhomogeneity | Blooming, signal distortion around metal |
| Geometric distortion | Frequency mismapping | Spatial displacement of anatomy |
| Pile-up artefact | Signal misregistration | Bright bands adjacent to void |
| Fat-saturation failure | Off-resonance effects | Incomplete fat suppression near metal |
MARS = Material, Alignment, Resolution, SequenceFactors Affecting Artefact Severity
Hook:Artefact severity is proportional to field strength - use 1.5T over 3T when imaging around metal
Implant Material Properties
| Material | Susceptibility | Artefact Severity | Common Uses |
|---|---|---|---|
| Titanium alloy | Low | Minimal | Plates, screws, stems, spinal implants |
| Cobalt-chrome | Moderate | Moderate-high | Femoral heads, tibial trays, bearing surfaces |
| Stainless steel | High | Severe | Older implants, some screws, wires |
| Tantalum | Low | Minimal | Trabecular metal, acetabular augments |
| Oxinium (Zr) | Very low | Minimal | Ceramic-like bearing surfaces |
| PEEK | None | None | Spinal cages, radiolucent |
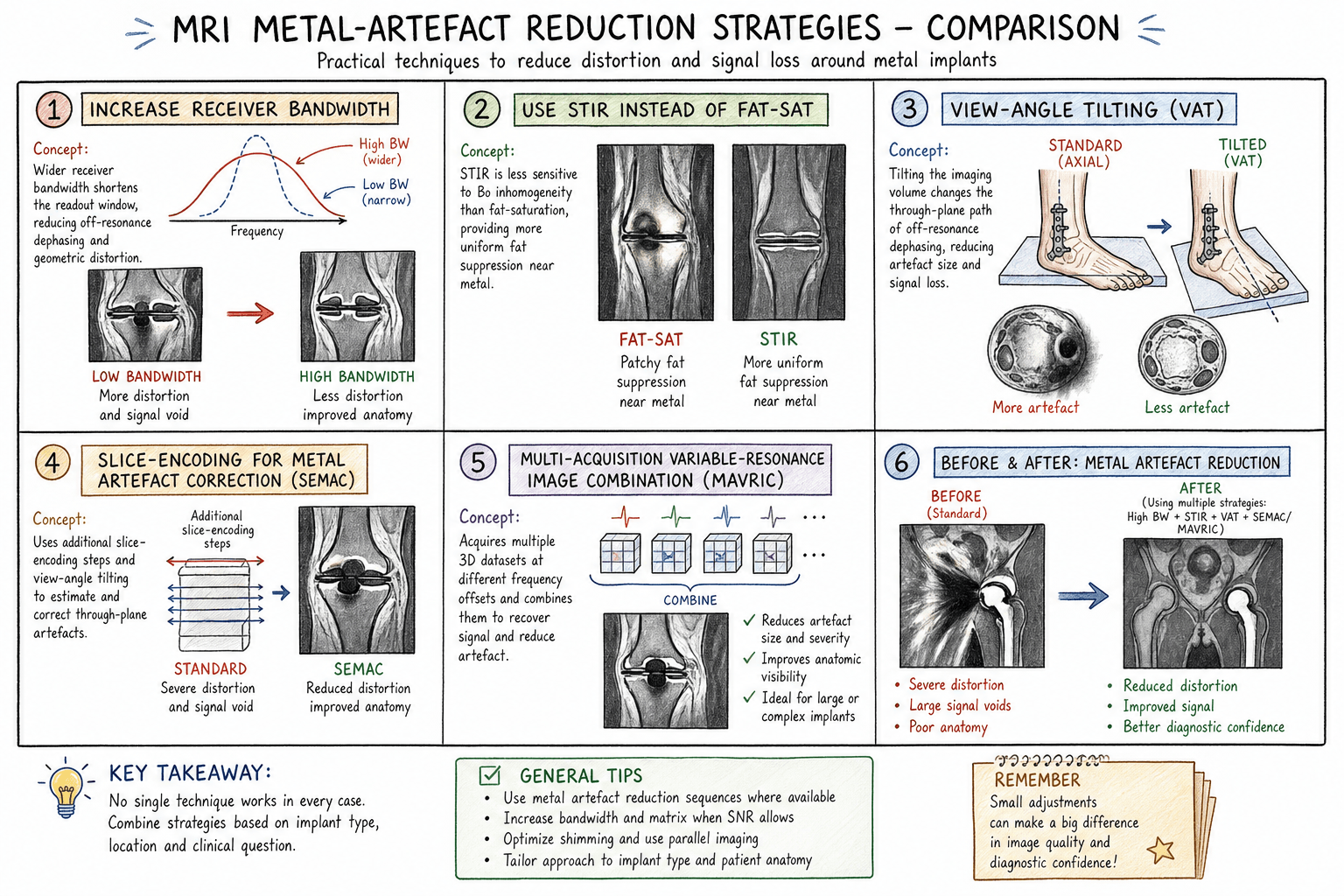
Standard Protocol Optimisation
| Parameter | Adjustment | Effect |
|---|---|---|
| Field strength | Use 1.5T over 3T | Artefact proportional to B0 |
| Receiver bandwidth | Increase (wide bandwidth) | Reduces geometric distortion |
| Slice thickness | Decrease (thin slices) | Reduces through-plane distortion |
| Matrix size | Increase (high resolution) | Improves spatial resolution |
| Sequence type | Spin echo over gradient echo | Less susceptibility-sensitive |
| Fat suppression | STIR over chemical fat-sat | STIR works despite field inhomogeneity |
| Echo train length | Optimise (not too long) | Balance SNR and blurring |
BLAST = Bandwidth up, Low field, Avoid gradient echo, Slices thin, STIRProtocol Levers to Cut Metal Artefact
Hook:These simple levers alone often suffice for small titanium implants; reserve full 3D SEMAC/MAVRIC for large cobalt-chrome arthroplasty.
Advanced MARS Techniques
| Technique | Mechanism | Scan Time | Availability |
|---|---|---|---|
| VAT | In-plane distortion correction | Moderate increase | Widely available |
| SEMAC | Through-plane encoding | Significant increase | GE, Siemens, Philips |
| MAVRIC | Multi-frequency acquisition | Significant increase | GE |
| MAVRIC-SL | Combined SEMAC + MAVRIC | Long | GE |
| WARP | VAT + optimisation | Moderate increase | Siemens |
Clinical Imaging Applications
| Finding | MRI Appearance | Significance |
|---|---|---|
| Pseudotumour | Cystic or solid mass adjacent to hip | May compress neurovascular structures |
| Fluid collection | T2 bright, may have debris | Periarticular, trochanteric bursa |
| Muscle damage | Oedema (T2 high) or atrophy (T1 fat) | Abductors commonly affected |
| Tendon disruption | Discontinuity, retraction | May affect surgical approach |
| Metallosis | Low signal debris, synovial thickening | Metal particle deposition |
Protocol Selection
| Indication | Field Strength | Key Sequences | MARS Technique |
|---|---|---|---|
| MoM hip surveillance | 1.5T | PD fat-sat, STIR, T1 | MARS (MAVRIC, SEMAC, WARP) |
| THA periprosthetic soft tissue | 1.5T | PD, STIR | VAT or MARS |
| Post-fusion spine | 1.5T | T1, T2, STIR sagittal/axial | VAT, MARS if available |
| Fracture fixation | 1.5T | STIR (oedema), T1 | Standard optimisation often sufficient |
| Shoulder arthroplasty | 1.5T | PD fat-sat, STIR | MARS if available |
Differential Diagnosis of Periprosthetic Masses on MARS MRI
| Entity | Typical Patient | MARS MRI Features | Discriminators |
|---|---|---|---|
| ALTR / pseudotumour | MoM hip, raised Co/Cr ions | Peri-articular cystic or solid mass, variable wall thickness, synovitis | Communicates with joint, abductor/tendon damage, ion levels elevated |
| Prosthetic joint infection | Pain, raised CRP/ESR, sinus | Lamellated synovitis, fluid collections, reactive marrow oedema, sinus tract | Systemic inflammatory markers, positive aspirate; ions normal |
| Particle-disease osteolysis (polyethylene wear) | Older non-MoM bearing | Expansile low-signal synovial masses, focal osteolysis around implant | Bearing is metal-on-poly/ceramic; ions normal |
| Haematoma / seroma | Recent surgery or anticoagulation | Well-defined collection, blood-degradation signal, no enhancing solid component | Temporal relation to surgery, resolves over time |
| Trochanteric bursitis | Lateral hip pain | Fluid in greater trochanteric bursa, no intra-articular mass | Confined to bursa, no abductor destruction |
| Soft-tissue sarcoma | No bearing-related cause, growing mass | Heterogeneous enhancing mass, may not respect joint planes | Independent of implant, biopsy required if atypical |
Evidence Base
SEMAC — Original Slice-Encoding Technique
- SEMAC extends a view-angle-tilting (VAT) spin-echo sequence with additional z-phase encoding, resolving distorted excitation profiles that cause through-plane distortion.
- VAT suppresses in-plane distortion while z-phase encoding corrects through-plane distortion, so spins are repositioned to their true spatial locations.
- The method requires no additional hardware and was validated in phantom and in vivo spine and knee studies with feasible scan times.
MAVRIC vs Conventional FSE After Arthroplasty
- In 122 patients (74 hip, 27 shoulder, 21 knee arthroplasties), MAVRIC showed significantly better visualisation of synovium and periprosthetic bone than metal-artefact-reduction FSE at all three joints.
- Synovitis and periprosthetic osteolysis were detected only on MAVRIC images in a substantial proportion of subjects.
- Supraspinatus tendon tears in 44% of relevant subjects were seen only on MAVRIC and not on FSE.
MAVRIC-SL at 3T in Hip Arthroplasty
- In 21 hips, MAVRIC-SL reduced measured artefact area versus 2D FSE by 59.9% at the level of the hip and 31.3% at the femur (both significant).
- Joint capsule and obturator externus/iliopsoas attachment sites were better depicted, and abnormal findings were significantly better shown with MAVRIC-SL.
- MAVRIC-SL increased diagnostic confidence even at 3T, a field strength normally avoided around large metal implants.
Controversies and Areas of Uncertainty
Guidelines, Registries & Global Practice
| Body | Region | Position on Imaging |
|---|---|---|
| MHRA Medical Device Alert | UK | Risk-stratified follow-up of MoM hips; cross-sectional imaging (MARS MRI or ultrasound) indicated for symptomatic patients or rising/raised metal ions |
| FDA guidance on MoM hips | US | Recommends clinical follow-up and considers cross-sectional imaging (MRI/US/CT) in symptomatic patients or with abnormal ion levels |
| AAOS / arthroplasty society guidance | US | Supports a combined algorithm of symptoms, examination, radiographs, serum metal ions and MARS MRI for evaluating the painful MoM hip |
| BOA / BHS consensus | UK | Endorses surveillance pathways using metal ions plus MARS MRI or ultrasound for soft-tissue/pseudotumour assessment |
| EFORT / European consensus | Europe | Aligns with stratified surveillance; cross-sectional imaging for symptomatic or high-risk implants |
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A patient with a painful metal-on-metal hip replacement is referred for MRI. Blood cobalt level is 12 ppb (elevated). You are asked about optimal imaging.”
“A patient 2 years post lumbar fusion with persistent leg pain is referred for MRI. The spine surgeon wants to assess for recurrent disc herniation.”
“You are asked to explain why MRI around metal implants is challenging. An orthopaedic trainee asks what material causes the least artefact.”
Material Artefact Severity
- Titanium: Least artefact
- Tantalum/Oxinium: Low artefact
- Cobalt-chrome: Moderate-high
- Stainless steel: Severe (10x titanium)
Protocol Optimisation
- 1.5T over 3T (artefact proportional to B0)
- Spin echo over gradient echo
- Increase receiver bandwidth
- STIR not chemical fat-sat
- Thin slices, high matrix
MARS Techniques
- VAT: In-plane correction
- SEMAC: Through-plane encoding
- MAVRIC: Multi-frequency acquisition
- WARP: Siemens combined technique
Clinical Applications
- MoM hip ALTR surveillance
- Post-fusion spine assessment
- Periprosthetic soft tissue
- PJI soft tissue extent