Ledderhose Disease | Benign Plantar Nodules | Dupuytren Association | High Recurrence
- Benign fibroblastic proliferation of the plantar aponeurosis, NOT a true neoplasm
- Strong association with Dupuytren disease (10-65%), Peyronie disease, and knuckle pads
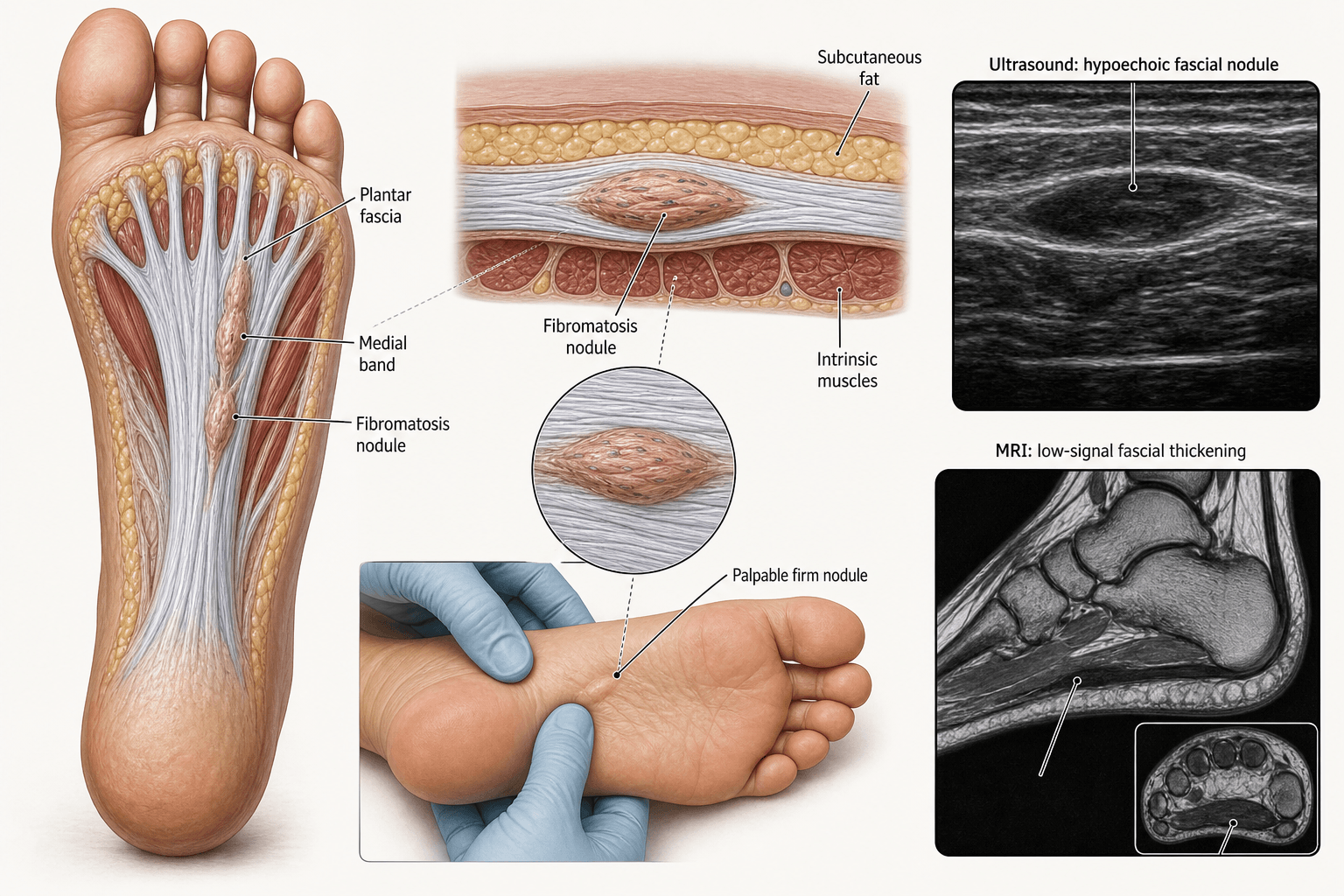
- Medial band of plantar fascia most commonly affected; nodules are firm and fixed to fascia
- Local excision carries recurrence rates up to 100%; wide fasciectomy reduces recurrence but increases morbidity
- Initial management is conservative: orthotics, steroid injection, physical therapy
- “Ledderhose = plantar equivalent of Dupuytren disease
- “Nodules are firm, non-tender initially, fixed to plantar fascia but NOT to skin
- “High recurrence after surgery is the key exam point
- “Always examine hands for Dupuytren and genitals for Peyronie (part of the fibromatosis triad)
Benign fibroblastic proliferation of the plantar aponeurosis driven by myofibroblasts producing type III collagen. It is a clonal proliferative disorder, NOT reactive. Histology mimics Dupuytren disease. Never confuse with plantar fasciitis (degenerative enthesopathy).
10-65% of patients have concomitant Dupuytren disease. The fibromatosis triad includes Dupuytren contracture, Ledderhose disease, and Peyronie disease. Knuckle pads (Garrod nodes) are a fourth association. Always examine the hands in a patient presenting with plantar nodules.
Recurrence after local excision approaches 100% in some series. Even with wide fasciectomy, recurrence ranges from 20-60%. This is the single most tested point. Conservative management is preferred initially; surgery is reserved for refractory, symptomatic disease.
Must distinguish from plantar fasciitis (diffuse heel pain, morning stiffness, no palpable nodule). Also differentiate from plantar fibrosarcoma (rapid growth, pain, deep fixation, imaging with necrosis and heterogeneous enhancement).
- Diagnosis
- Clinical examination, ultrasound confirms
- Treatment
- Observation, accommodative orthotics
- Key Pearl
- Most nodules never need surgery
- Diagnosis
- MRI to delineate extent, rule out sarcoma
- Treatment
- Steroid injection, extracorporeal shockwave, radiotherapy
- Key Pearl
- Exhaust conservative options before surgery
- Diagnosis
- MRI for surgical planning, assess medial band
- Treatment
- Wide fasciectomy or total plantar fasciectomy
- Key Pearl
- Counsel on 20-60% recurrence even with wide excision
LEADFibromatosis Triad and Associations
Hook:LEAD the exam: always check all four sites when you find one fibromatosis!
PIRDisease Stages (Matching Dupuytren Biology)
Hook:PIR — like a pirate, the disease has three phases before it burns out!
Overview and Epidemiology
Plantar fibromatosis is the plantar counterpart of Dupuytren disease and shares its fibroblastic proliferative biology. Unlike Dupuytren, it rarely causes contracture of the toes, but it produces firm, often painless nodules in the medial plantar arch that can become symptomatic with weight-bearing. The hallmark exam feature is the very high recurrence rate after surgical excision, making conservative management the cornerstone. Examiners frequently test the Dupuytren association and the rationale for non-operative management.
- Incidence: Less common than Dupuytren disease (approximately one-tenth the prevalence)
- Age: Peak onset 30-60 years
- Sex: Slight male predominance, though less pronounced than Dupuytren
- Bilateral: 25-50% of cases
- Ethnicity: Predominantly Northern European descent, same as Dupuytren
- Dupuytren disease: Strongest association (10-65% comorbidity)
- Family history: Autosomal dominant with variable penetrance suggested
- Diabetes mellitus: Metabolic association with fibromatoses
- Alcohol: Chronic heavy intake linked to Dupuytren and Ledderhose
- Anti-epileptic drugs: Particularly barbiturates and phenytoin
- Trauma: Recurrent microtrauma to plantar fascia debated as a trigger
- Liver disease: Especially alcohol-related cirrhosis
Pathophysiology
The plantar aponeurosis (plantar fascia) has three bands: medial, central, and lateral. The central band is thickest and strongest, arising from the medial calcaneal tubercle and inserting into the forefoot via slips to each toe. Plantar fibromatosis most commonly affects the medial band (not the central band that is inflamed in plantar fasciitis). The nodules are composed of myofibroblasts in a collagenous matrix, dominated by type III collagen (same as Dupuytren disease). The disease follows the same three-stage biology as Dupuytren: proliferative, involutional, and residual phases. TGF-beta (especially beta-1 and beta-2) is the key cytokine driving fibroblast proliferation and collagen synthesis.
- Plantar Fibromatosis (Ledderhose)
- Benign fibroblastic proliferation (myofibroblasts, type III collagen)
- Plantar Fasciitis
- Degenerative enthesopathy (micortears, angiofibroblastic hyperplasia)
- Plantar Fibromatosis (Ledderhose)
- Medial band of plantar fascia, mid-arch
- Plantar Fasciitis
- Central band origin at medial calcaneal tubercle
- Plantar Fibromatosis (Ledderhose)
- Firm, well-defined nodule(s) fixed to fascia
- Plantar Fasciitis
- Diffuse tenderness at calcaneal origin, no discrete nodule
- Plantar Fibromatosis (Ledderhose)
- Nodule with weight-bearing pain (or painless)
- Plantar Fasciitis
- Morning startup pain, post-rest stiffness, heel pain
- Plantar Fibromatosis (Ledderhose)
- Dupuytren, Peyronie, knuckle pads, diabetes
- Plantar Fasciitis
- Obesity, pes planus, calf tightness, running
- Plantar Fibromatosis (Ledderhose)
- Conservative first; surgery last due to high recurrence
- Plantar Fasciitis
- Stretching, orthotics, injection, ESWT; surgery rarely needed
Key cytokine: TGF-beta (beta-1 and beta-2) drives myofibroblast proliferation
Cell type: Myofibroblasts with contractile apparatus (alpha-smooth muscle actin positive)
Collagen: Predominantly type III (immature) in proliferative phase, transitioning to type I (mature) in residual phase
Genetics: Suggested autosomal dominant inheritance with variable penetrance; chromosomal abnormalities (trisomy 8, trisomy 14) reported in some nodules
Mechanical tension: Myofibroblasts align along lines of tension (same as Dupuytren)
Surgical trauma itself triggers TGF-beta release and myofibroblast activation
Field defect: The entire plantar fascia is predisposed to fibromatosis, not just the excised nodule
Incomplete excision: Microscopic disease extends beyond the palpable nodule
Tension on repair: Weight-bearing stresses the surgical site, promoting fibroproliferation
Genetic predisposition: Underlying propensity to fibromatosis cannot be excised
This is why even total plantar fasciectomy has measurable recurrence rates
Classification and Types
Staging by Disease Biology (Luck Classification Adapted)
- Histology
- Hypercellular, numerous myofibroblasts, minimal collagen
- Clinical Behaviour
- Rapid growth, nodule enlarging, may be tender
- Best Treatment Approach
- Conservative; avoid surgery in this phase (highest recurrence)
- Histology
- Myofibroblasts aligning along tension lines, increasing collagen
- Clinical Behaviour
- Growth slowing, nodule stabilizing
- Best Treatment Approach
- Steroid injection, shockwave, or radiotherapy
- Histology
- Acellular, dense collagen, few myofibroblasts
- Clinical Behaviour
- Static nodule, often painless, mature scar-like
- Best Treatment Approach
- Surgery if symptomatic (lowest recurrence rate if operated here)
Surgery performed during the proliferative phase has the highest recurrence rate because active myofibroblasts at the margins respond to surgical trauma with aggressive regrowth. Operating in the residual phase, when disease is acellular and burned out, gives the lowest recurrence.
An examiner will often broaden out from "what is Ledderhose?" to "classify the fibromatoses" - and the key is that plantar fibromatosis is a SUPERFICIAL (fascial) fibromatosis, a completely different clinical animal from the deep (desmoid) fibromatoses:
- Superficial / fascial fibromatoses - small, slow-growing, arise from fascia/aponeurosis, do NOT metastasise and are only minimally locally aggressive. This family is the "fibromatosis diathesis": palmar (Dupuytren), plantar (Ledderhose), penile (Peyronie), and knuckle pads (Garrod). Managed conservatively; surgery is for symptoms, with the high recurrence already discussed.
- Deep / musculoaponeurotic fibromatoses (desmoid tumours / aggressive fibromatosis) - arise from deep musculoaponeurotic structures, are locally infiltrative and aggressive (though still non-metastasising), and are biologically distinct: driven by beta-catenin / CTNNB1 mutations (sporadic) or APC mutations in familial adenomatous polyposis / Gardner syndrome. Subtypes are extra-abdominal, abdominal-wall and intra-abdominal. Management is very different (active surveillance, systemic therapy - e.g. tamoxifen/NSAIDs, tyrosine-kinase inhibitors, the newer gamma-secretase inhibitor nirogacestat - radiotherapy, and wide resection only when needed).
Exam point: do not lump Ledderhose with desmoid disease. Ledderhose is a benign superficial fibromatosis (Dupuytren of the foot); desmoid (deep) fibromatosis is a locally aggressive CTNNB1/APC-driven tumour with FAP/Gardner associations and a fundamentally different treatment pathway.
Clinical Assessment

- Onset: Insidious, patient notices lump in arch of foot
- Pain: Initially painless; pain develops with weight-bearing or shoe pressure
- Growth: Slowly progressive over months to years
- Function: Difficulty with footwear, pain on walking or standing
- Associations: Ask about hand contractures, penile curvature, family history
- Treatments tried: Orthotics, injections, previous surgery
- Inspect: Plantar surface for visible or palpable nodules, arch height
- Palpate: Firm, non-fluctuant nodules fixed to plantar fascia, mobile over deep structures, skin freely mobile over nodule
- Location: Most often medial band in mid-arch region
- Tenderness: Assess with weight-bearing pressure
- Toes: Check for toe contractures (rare but possible with extensive disease)
- Hands: Examine for Dupuytren cords, pits, and contractures
- Gait: Observe for antalgic gait or compensated weight-bearing
In any patient presenting with plantar fibromatosis, the examiner must assess:
- Both hands for Dupuytren disease (palmar pits, cords, MCP/PIP contractures)
- Genitalia for Peyronie disease (offer referral to urology; do not examine directly in orthopaedic clinic)
- PIP joints dorsally for knuckle pads (Garrod nodes)
- Contralateral foot for bilateral involvement (25-50%)
Failure to document these associations in the exam setting is a common error that costs marks.
- Key Features
- Firm nodule fixed to fascia, Dupuytren association
- Discriminating Finding
- Nodule continuous with plantar fascia fibers on ultrasound
- Key Test / Imaging
- Ultrasound or MRI: fascial-origin nodule
- Key Features
- Heel pain, no nodule, morning startup pain
- Discriminating Finding
- Tenderness at medial calcaneal tubercle, diffuse thickening
- Key Test / Imaging
- Ultrasound: fascia thickness greater than 4 mm at origin
- Key Features
- Single nodule, no Dupuytren or Peyronie
- Discriminating Finding
- Clinically identical; histology may show less cellularity
- Key Test / Imaging
- MRI: same appearance; distinction is clinical context
- Key Features
- Rapidly enlarging, painful, deep fixation
- Discriminating Finding
- Rapid growth, heterogeneous enhancement, possible necrosis
- Key Test / Imaging
- MRI with contrast; biopsy if suspicious features
- Key Features
- Soft, compressible, Tinel positive if nerve involved
- Discriminating Finding
- Often multiple, associated with neurofibromatosis type 1
- Key Test / Imaging
- MRI: target sign, associated with nerve
- Key Features
- Subcutaneous, not fixed to fascia, multiple
- Discriminating Finding
- History of RA, elevated rheumatoid factor, over bony prominences
- Key Test / Imaging
- Bloods: RF, anti-CCP; ultrasound: subcutaneous not fascial
Plantar fibromatosis is a distinct entity from plantar fasciitis. Ledderhose presents with a firm, well-defined nodule in the plantar arch arising from the fascia, associated with Dupuytren disease. Plantar fasciitis is a degenerative enthesopathy of the central band origin at the calcaneus, presenting with diffuse heel pain and no discrete nodule. The distinction is clinical and confirmed on imaging. Mistaking the two leads to inappropriate steroid injection at the heel (wrong location) and failure to screen for Dupuytren disease.
The epidemiology section notes that childhood plantar fibromatosis is "a distinct entity" - worth developing, because a plantar mass in a child is a different problem and a recognised paediatric foot-mass question:
- Different demographic and biology: it occurs in children/adolescents and lacks the Dupuytren/Peyronie diathesis that defines the adult disease - so there is no point screening a child's hands for cords.
- Different morphology: rather than a single discrete adult-type nodule, juvenile disease is often more diffuse and band-like / multinodular within the plantar fascia, and tends to be more locally persistent.
- Histological caution: in children the main differential is calcifying aponeurotic fibroma (a separate, infiltrative fibroblastic lesion of hands/feet with characteristic stippled calcification), which must not be mistaken for a sarcoma; biopsy interpretation needs a paediatric/soft-tissue pathologist.
- Management is still conservative: it is benign and often self-limiting; surgery has the same high recurrence problem (arguably worse, given the diffuse pattern), so excision is reserved for genuinely refractory symptomatic disease, with families counselled on recurrence.
Exam point: a firm plantar mass in a child is not simply "early Ledderhose" - it is juvenile plantar fibromatosis, has no Dupuytren association, is more diffuse, and its key differential is calcifying aponeurotic fibroma; manage conservatively and avoid over-diagnosing malignancy.
Investigations
Imaging Protocol
Findings: Fusiform or nodular thickening of the plantar fascia, continuous with fascial fibers, typically hypoechoic or isoechoic
Advantages: Quick, inexpensive, dynamic assessment, guides injection
Limitations: Operator-dependent, limited soft tissue characterization for atypical lesions
Sequences: T1, T2, fat-suppressed T2 (STIR), contrast-enhanced
Findings: Nodular mass arising from plantar fascia; T1 hypointense; T2 signal varies with stage (higher in proliferative, lower in residual)
Indications: Pre-operative planning, concern for sarcoma, failed conservative management
Key discriminator from sarcoma: Fascial origin, absence of necrosis, homogeneous enhancement, continuity with fascial fibers
Indication: Rapid growth, large size (greater than 5 cm), deep location, heterogeneous MRI enhancement, necrosis
Technique: Core needle biopsy under imaging guidance; avoid excisional biopsy as initial diagnostic step
Goal: Exclude fibrosarcoma, malignant fibrous histiocytoma, or synovial sarcoma
MRI is the gold standard for pre-operative planning and ruling out sarcoma. The key feature differentiating plantar fibromatosis from malignancy is its origin from and continuity with the plantar fascia, homogeneous signal characteristics, and absence of necrosis. If any atypical features are present (rapid growth, size greater than 5 cm, necrosis, deep extension), biopsy is mandatory before any excisional surgery.
Management Algorithm
Non-Operative Management (First Line for All Patients)
Goal: Symptom relief and functional improvement; disease may remain stable or even regress
Conservative Treatment Protocol
Observation: Many nodules are asymptomatic and never progress
Shoe modification: Accommodative orthotics with soft plantar arch support, wide toe box shoes, avoid hard insoles
Activity modification: Reduce direct pressure on nodule; cushioned footwear
Corticosteroid injection: Triamcinolone mixed with local anaesthetic, injected into the nodule under ultrasound guidance
Extracorporeal shockwave therapy (ESWT): Radial shockwave to the nodule area, weekly sessions for 3-5 weeks
Physical therapy: Plantar fascia stretching, calf stretching, deep tissue massage
Collagenase clostridium histolyticum (CCH): Off-label injection (approved for Dupuytren); small case series show nodule softening
Radiotherapy: Low-dose external beam radiotherapy (total 30 Gy in 10 fractions); used in European centres with reported disease control
Tamoxifen: Anti-estrogen with anti-fibrotic properties; limited evidence but reported in case series
Monitor: Serial clinical examination every 6-12 months for asymptomatic nodules
Repeat injection: Steroid injection can be repeated at 3-6 month intervals if initially effective
Patient education: Explain benign nature, Dupuytren association, high recurrence if surgery pursued
The vast majority of plantar fibromatosis nodules are asymptomatic or minimally symptomatic and never require surgery. The natural history is one of slow progression to a static residual phase. Conservative management is always first line because surgical recurrence rates are extremely high. Orthotics to offload the nodule and corticosteroid injection for pain are the mainstays.
STEPTreatment Approach for Ledderhose
Hook:Take it STEP by STEP — surgery is always the last step for Ledderhose!
Complications
- Incidence
- 20-100% depending on extent of excision
- Risk Factors
- Proliferative phase, Dupuytren diathesis, marginal excision
- Management
- Conservative management of recurrence; re-excision rarely indicated
- Incidence
- 10-20%
- Risk Factors
- Plantar incision under tension, diabetes, smoking, early weight-bearing
- Management
- Delayed primary closure, vacuum-assisted closure, flap coverage if severe
- Incidence
- Variable, up to 30%
- Risk Factors
- Total fasciectomy, loss of medial band support
- Management
- Custom orthotics, arch support, physical therapy
- Incidence
- 5-10%
- Risk Factors
- Large dead space after fasciectomy, inadequate drainage
- Management
- Evacuation if symptomatic, compressive dressing
- Incidence
- Less than 5%
- Risk Factors
- Diabetes, immunosuppression, plantar wound contamination
- Management
- Oral antibiotics for superficial; IV antibiotics and debridement for deep infection
- Incidence
- Less than 5%
- Risk Factors
- Dissection deep to fascia, extensive excision
- Management
- Neurolysis if persistent neuropathic pain
The most important concept for exam purposes is that recurrence after surgical excision of plantar fibromatosis is extremely common. Local excision alone has recurrence approaching 100% in published series. Even wide fasciectomy carries 20-60% recurrence. The disease process involves a field defect of the plantar fascia — removing one nodule does not eliminate the underlying predisposition. This is why conservative management is always first line, and surgery is reserved for refractory symptomatic disease after thorough patient counselling.
Outcomes and Prognosis
- Symptom Relief
- Good for mild symptoms
- Recurrence
- N/A (disease may progress but treatment is ongoing)
- Patient Satisfaction
- High compliance, low morbidity
- Symptom Relief
- 60-80% initial pain relief
- Recurrence
- Disease persists; nodule may recur if pain returns
- Patient Satisfaction
- Good short-term; may need repeat injection
- Symptom Relief
- 60-80% report symptom improvement
- Recurrence
- Disease control in 70-90% long-term
- Patient Satisfaction
- Good in European centres, limited availability elsewhere
- Symptom Relief
- Good pain relief if wound heals
- Recurrence
- 20-60% nodule recurrence
- Patient Satisfaction
- Moderate; morbidity offsets gains in some patients
- Symptom Relief
- Best disease control
- Recurrence
- 10-25% recurrence
- Patient Satisfaction
- Variable; arch morbidity reduces satisfaction
Best prognosis: Solitary nodule, residual phase disease, no Dupuytren diathesis, patient willing to manage conservatively
Poor prognosis: Multiple nodules, bilateral disease, strong Dupuytren diathesis (young onset, family history, multiple fibromatosis sites), proliferative phase at time of surgery
Key message: Plantar fibromatosis is a benign condition that rarely causes significant functional impairment. The treatment should be proportionate to symptoms. Aggressive surgical treatment of a minimally symptomatic nodule is inappropriate given the recurrence risk.
Guidelines, Registries & Global Practice
- Incidence: Significantly less common than Dupuytren disease, estimated at approximately one-tenth the prevalence
- Demographics: Predominantly Northern European descent (same ethnic predisposition as Dupuytren); increasingly recognized in other populations
- Age: Peak onset 30-60 years; rare in children (juvenile plantar fibromatosis is a distinct entity)
- Sex: Slight male predominance, less pronounced than the male dominance seen in Dupuytren
- Bilateral: 25-50% of patients have bilateral involvement
- High-resource centres: MRI for diagnosis and planning; access to radiotherapy, collagenase injection, and specialist foot and ankle surgery
- Limited-resource settings: Diagnosis is primarily clinical; ultrasound where available; orthotics fabricated locally; surgery limited to tertiary centres
- Radiotherapy availability: Widely used in Germany and other European countries for Ledderhose; much less available in North America, Australasia, and the UK
- Universal principle: Conservative first approach applies globally regardless of resources
- Diagnosis Emphasis
- Clinical diagnosis with ultrasound confirmation; MRI for atypical features
- Conservative Treatment
- Orthotics, steroid injection, radiotherapy (strong European experience)
- Surgical Approach
- Wide fasciectomy preferred if surgery needed; avoid local excision
- Diagnosis Emphasis
- Clinical diagnosis; imaging if sarcoma concern
- Conservative Treatment
- Orthotics first, then injection; ESWT if available
- Surgical Approach
- Surgery only after exhaustive conservative treatment; counsel on recurrence
- Diagnosis Emphasis
- MRI standard for pre-operative planning; biopsy if suspicious
- Conservative Treatment
- Orthotics, steroid injection; CCH off-label in specialist centres
- Surgical Approach
- Partial fasciectomy of affected band; total fasciectomy for extensive disease
- Diagnosis Emphasis
- Assess extent of disease and rule out sarcoma before any intervention
- Conservative Treatment
- Stepwise conservative algorithm; consider radiotherapy
- Surgical Approach
- Wide margins required; biopsy first if any atypical feature
There is no dedicated global registry for plantar fibromatosis. The evidence base consists of small retrospective case series and narrative reviews rather than randomized controlled trials. Management is principle-based rather than guideline-driven: diagnose clinically, confirm with imaging, treat conservatively first, and reserve surgery for refractory symptomatic disease after extensive counselling about recurrence.
Record in every patient with plantar fibromatosis:
- Examination of both hands for Dupuytren disease (document positive or negative)
- Assessment of contralateral foot for bilateral disease
- Discussion of the fibromatosis triad (Dupuytren, Ledderhose, Peyronie) documented
- Counselling about the benign nature and high surgical recurrence risk documented
- Conservative treatment trialled and documented before any surgical consideration
A patient who undergoes surgery without being counselled about the high recurrence rate — or without documented conservative treatment first — represents a significant medicolegal risk in any jurisdiction.
Controversies & Areas of Uncertainty
Low-dose external beam radiotherapy shows promising disease control in European centres (70-90% at 5 years), but there is no RCT evidence, long-term malignancy risk is theoretical but not zero, and availability is limited outside Europe. It remains an intermediate option for patients failing injection therapy but wishing to avoid surgery.
CCH is approved for Dupuytren cords but used off-label for Ledderhose. Small case series show nodule softening, but the plantar fascia is thicker and more robust than the palmar aponeurosis, potentially requiring different dosing. No RCTs exist for this indication, and cost is significant.
No consensus on the minimum adequate excision margin. Local excision has unacceptable recurrence; total fasciectomy has lowest recurrence but highest morbidity. Most surgeons favour partial fasciectomy of the affected band, but the precise margin (macroscopic vs microscopic) is not standardized.
The Luck classification (proliferative, involutional, residual) is widely referenced but difficult to apply clinically without biopsy. Determining disease stage from MRI signal characteristics has been proposed but not validated. Operating in the residual phase is theoretically optimal but practically difficult to time.
MCQ Practice Points
Q: A patient presents with plantar fibromatosis. What associated condition must you specifically look for? A: Dupuytren disease. The association rate is 10-65%, and both conditions share TGF-beta driven myofibroblast proliferation. Always examine both hands for palmar cords, pits, and contractures. The fibromatosis triad also includes Peyronie disease.
Q: What is the recurrence rate after local excision of a plantar fibromatosis nodule? A: Up to 100% in published series. Local excision alone is generally discouraged. Wide fasciectomy reduces recurrence to 20-60%, and total plantar fasciectomy to 10-25%, but at the cost of significantly greater morbidity including arch collapse.
Q: What cell type drives plantar fibromatosis and what collagen type predominates? A: Myofibroblasts are the key cell type, and type III collagen predominates in the proliferative phase. The biology mirrors Dupuytren disease exactly, with the same three-stage progression: proliferative (cellular), involutional (aligning), and residual (acellular collagen).
Q: How do you differentiate plantar fibromatosis from plantar fasciitis clinically? A: Plantar fibromatosis presents with a firm, well-defined nodule in the plantar arch (medial band), fixed to the fascia but mobile under the skin, often painless initially. Plantar fasciitis presents with diffuse heel tenderness at the medial calcaneal tubercle, morning startup pain, and no discrete nodule. The conditions affect different bands of the plantar fascia and have completely different pathophysiology.
Q: What is the first-line treatment for a symptomatic plantar fibromatosis nodule? A: Conservative management: accommodative orthotics with soft arch support, shoe modification, and activity modification. If symptoms persist, ultrasound-guided corticosteroid injection or extracorporeal shockwave therapy. Surgery is a last resort due to unacceptably high recurrence rates and is reserved for patients with refractory pain despite exhaustive conservative treatment.
Q: In which disease stage is surgery for plantar fibromatosis associated with the lowest recurrence? A: The residual (acellular) phase. In the residual phase, myofibroblasts are absent and the nodule is mature collagen. Operating during the proliferative phase (active myofibroblasts) has the highest recurrence because surgical trauma triggers aggressive myofibroblast regrowth at the margins.
Clinical Imaging
Plantar Fibromatosis — Imaging Findings
Imaging is primarily via MRI or ultrasound. MRI demonstrates nodular thickening of the plantar fascia, typically along the medial band, with low-to-intermediate signal on T1 and variable T2 signal depending on disease stage (cellular proliferative nodules may show higher T2 signal, while mature collagenous nodules are low on both T1 and T2). Ultrasound shows a hypoechoic or isoechoic fusiform nodule arising from the plantar fascia, continuous with the fascial fibers.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 42-year-old man presents with a 6-month history of a slowly enlarging painless lump in the arch of his right foot. He has noticed a similar smaller lump on the left foot recently. On examination, there are firm, non-tender nodules fixed to the plantar fascia bilaterally. You also notice thickening and tethering of the palmar skin over the ring and small fingers of both hands with early metacarpophalangeal flexion contractures. What is the diagnosis and how would you manage this?”
“A 50-year-old woman had a local excision of a plantar fibromatosis nodule 18 months ago. She now presents with recurrent nodules at the same site that are more painful than the original lesion. She has a history of Dupuytren disease affecting both hands, and her father had similar conditions. She is frustrated and wants definitive surgical treatment. How would you counsel her and what is your management plan?”
Key Facts
- Benign fibroblastic proliferation of the plantar aponeurosis (medial band most common)
- Myofibroblasts produce type III collagen; TGF-beta is the key cytokine
- Same three-stage biology as Dupuytren: proliferative, involutional, residual
- Bilateral in 25-50%; peak age 30-60 years; slight male predominance
Associations
- Dupuytren disease in 10-65% of patients (strongest and most tested association)
- Peyronie disease and knuckle pads complete the fibromatosis triad/tetrad
- Diabetes, alcohol, anti-epileptics, liver disease, family history are risk factors
- Always examine both hands and ask about the full fibromatosis spectrum
Diagnosis
- Clinical: firm nodule fixed to plantar fascia, freely mobile under skin, medial arch
- Ultrasound: fusiform nodule continuous with fascial fibers
- MRI: T1 hypointense; T2 signal varies with stage; rules out sarcoma
- Biopsy only if atypical features (rapid growth, size greater than 5 cm, necrosis)
Treatment Algorithm
- Step 1: Observation with accommodative orthotics (most patients never need more)
- Step 2: Corticosteroid injection, ESWT, physical therapy for symptomatic nodules
- Step 3: Radiotherapy (30 Gy) or collagenase injection in specialist centres
- Step 4: Wide partial fasciectomy (last resort, only after exhausting conservative Rx)
Recurrence and Complications
- Local excision: up to 100% recurrence — generally discouraged
- Wide fasciectomy: 20-60% recurrence; total fasciectomy: 10-25% recurrence
- Wound dehiscence 10-20%; arch pain up to 30% after total fasciectomy
- Recurrence is the rule after surgery — conservative management is always first line
Evidence Base and Key Trials
Ledderhose's Disease: An Up-to-Date Review of a Rare Non-Malignant Disorder
- Comprehensive up-to-date review of Ledderhose disease pathophysiology, diagnosis, and management
- Conservative management (orthotics, steroid injection) is first line; surgery reserved for refractory symptomatic disease
- Recurrence rates after local excision approach 100%, making conservative treatment the cornerstone
- MRI is the gold standard for pre-operative planning and excluding soft tissue sarcoma
Incidence and treatment of recurrent plantar fibromatosis by surgery and postoperative radiotherapy
- Recurrence after marginal excision is very high, supporting the field-defect nature of the disease
- Postoperative radiotherapy (30 Gy total) achieved long-term disease control in the majority of patients treated
- Combined surgery plus radiotherapy provided better outcomes than surgery alone for recurrent disease
- Recommend stepwise approach: orthotics, injection, radiotherapy, then surgery as last resort
Association of Morbus Ledderhose with Dupuytren's contracture
- Significant association between Ledderhose disease and Dupuytren contracture confirmed in an epidemiological study
- Patients with plantar fibromatosis have a markedly higher prevalence of Dupuytren disease than the general population
- Both conditions share similar demographic features including age, sex distribution, and bilateral involvement
- The association supports a common fibroproliferative diathesis affecting multiple fascial sites
Radiation therapy for early stages of morbus Ledderhose
- Patients treated with low-dose external beam radiotherapy for early-stage Ledderhose disease
- Symptom improvement (pain reduction, nodule softening) reported in the majority of patients
- Long-term disease control achieved with minimal acute toxicity
- Radiotherapy is most effective when delivered in the proliferative or early involutional stage
Recurrence Rate After Wide Resection of Plantar Fibromatosis: A Case Series and Systematic Literature Review
- Systematic literature review of recurrence rates after wide resection of plantar fibromatosis
- Even with wide resection, recurrence remains substantial (reported rates 20-60%)
- Local excision carries the highest recurrence risk and is discouraged as isolated treatment
- Wide fasciectomy provides the best balance of disease control and acceptable functional outcome
Radiotherapy in fascial fibromatosis: a case series, literature review and considerations for treatment of early-stage disease
- Case series and literature review demonstrating efficacy of radiotherapy for fascial fibromatosis including Ledderhose disease
- Low-dose radiotherapy (total 30 Gy in 10 fractions) achieved symptom control in the majority of treated patients
- Treatment was most effective when initiated in early-stage disease before significant fibrosis
- Minimal long-term toxicity reported with no radiation-induced malignancy in follow-up
Unusual Intranodular Collagenase Injection: A Case of Bilateral Ledderhose Disease
- Collagenase clostridium histolyticum (CCH), approved for Dupuytren cords, used off-label for bilateral Ledderhose disease
- Intranodular injection resulted in nodule softening and symptom improvement
- The plantar fascia is thicker and broader than palmar aponeurosis, potentially requiring tailored injection technique
- Evidence remains limited to case reports and small series; no RCT-level data for this indication