The Finger Drop
Key Definitions
Critical Must-Knows
- PIN Syndrome presents as 'Finger Drop' but sparing of wrist extension (ECRL is intact).
- Wrist extends in radial deviation (Radio-Carpal extension via ECRL).
- No sensory loss (Superficial Radial Nerve branches off proximally).
- The most common compression site is the Arcade of Frohse (proximal edge of Supinator).
- Lipomas are a common cause of 'spontaneous' PIN palsy.
- Rheumatoid synovitis at the elbow can also compress the PIN.
Clinical Pearls
- "If the patient has WRIST drop, the lesion is proximal to the PIN (High Radial Nerve).
- "In PIN palsy, the patient can extend the wrist (ECRL) but it deviates radially (due to ECU paralysis).
- "Pain alone is Radial Tunnel Syndrome, not PIN Syndrome.
The Trap: Tendon Rupture vs Palsy
The Diagnosis
Vaughan-Jackson? RA patients can have EDC tendon ruptures (Vaughan-Jackson) OR PIN palsy (synovitis). Missing the difference leads to the wrong surgery. Tendon rupture: Sudden 'ping', dropped fingers one by one (Ulnar to Radial). PIN Palsy: Slow onset (usually), all fingers affected together (or specific pattern).
The Test
Tenodesis Test Flex the wrist. If the fingers extend passively (Tenodesis), the tendons are intact (nerve issue). If the fingers remain floppy/flexed then it is a Tendon rupture. Ultrasound confirms.
| Condition | Motor Loss | Sensory Loss | Site |
|---|---|---|---|
| PIN Syndrome | Finger/Thumb Ext + ECU | None | Arcade of Frohse |
| Radial Tunnel | None (Pain only) | None | Arcade of Frohse |
| Wartenberg's | None | Dorsal Webspace | Fascia (Forearm) |
| High Radial | Wrist + Fingers + Sensation | Dorsal Webspace | Spiral Groove |
ASEMuscles Innervated (PIN)
| A | Abductor APL (Abductor Pollicis Longus). |
| S | Supinator Supinator muscle. |
| E | Extensors EDC, EIP, EDM, ECU, EPB, EPL. |
| A | Abductor APL (Abductor Pollicis Longus). |
| S | Supinator Supinator muscle. |
| E | Extensors EDC, EIP, EDM, ECU, EPB, EPL. |
Hook:The PIN supplies the deep (distal) forearm extensors after innervating the supinator; the superficial wrist extensor ECRL is supplied by the radial nerve proximally and is spared.
FREASSites of Compression
| F | Fibrous Fibrous bands anterior to Radiocapitellar joint. |
| R | Recurrent Recurrent Radial vessels (Leash of Henry). |
| E | ECRB Edge of ECRB (medial border). |
| A | Arcade Arcade of Frohse (Supinator edge). |
| S | Supinator Distal edge of Supinator. |
| F | Fibrous Fibrous bands anterior to Radiocapitellar joint. | A | Arcade Arcade of Frohse (Supinator edge). |
| R | Recurrent Recurrent Radial vessels (Leash of Henry). | S | Supinator Distal edge of Supinator. |
| E | ECRB Edge of ECRB (medial border). |
Hook:Radial nerve FREAS up.
E-E-EOrder of Recovery
| E | ECU Extensor Carpi Ulnaris (First). |
| E | Extensors EDC/EIP (Middle). |
| E | EPL EPL/Indices (Last). |
| E | ECU Extensor Carpi Ulnaris (First). |
| E | Extensors EDC/EIP (Middle). |
| E | EPL EPL/Indices (Last). |
Hook:Recovery follows the order of innervation. Note: in a HIGH radial nerve lesion, brachioradialis and ECRL recover first — the PIN muscles (ECU, EDC, EPL) recover later.
Overview
Definition
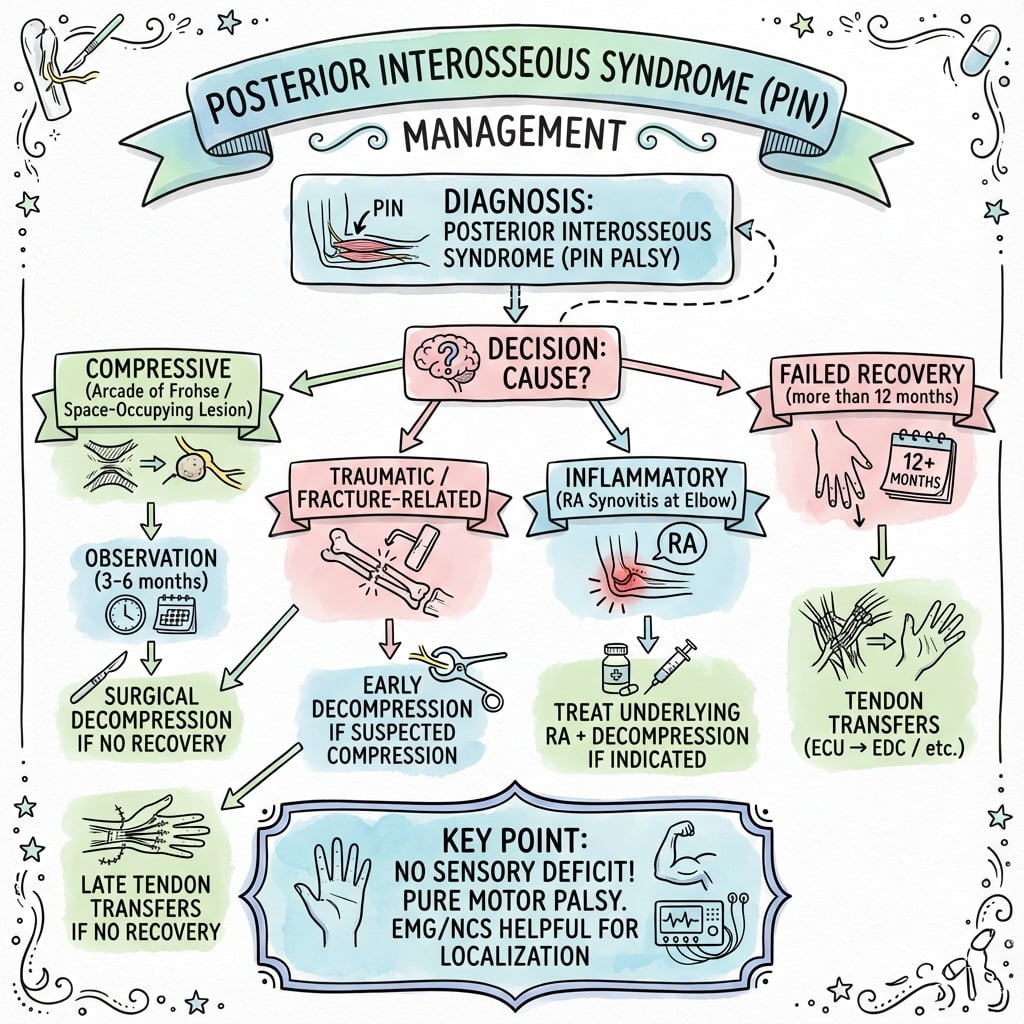
Posterior Interosseous Nerve (PIN) Syndrome is a compressive neuropathy of the deep motor branch of the Radial nerve. It typically occurs at the proximal forearm within the Radial Tunnel, most commonly at the Arcade of Frohse.
Clinically, it presents as weakness of finger and thumb extension ("Finger Drop"). Crucially, wrist extension is preserved (ECRL is innervated proximal to the PIN), but the wrist deviates radially during extension because the Extensor Carpi Ulnaris (ECU) is paralyzed.
Pathophysiology and Mechanisms
Course
- Division: The Radial Nerve divides into Superficial (Sensory) and Deep (Motor/PIN) at the level of the radio-capitellar joint.
- Entry: The PIN enters the "Radial Tunnel" under the edge of the ECRB.
- Supinator: It pierces the Supinator muscle between its two heads. The proximal edge is the Arcade of Frohse.
- Exit: Exits the supinator distally to supply the deep extensor compartment.
The course within the supinator is 4-5cm long.
Classification Systems
Clinical Types
- Type I (Complete PIN): All PIN muscles paralyzed. Finger drop + Thumb drop + ECU paralysis.
- Type II (Partial PIN): Only some muscles (e.g., just Thumb/Index). Mimics tendon rupture.
- Type III (Radial Tunnel): Pain only. Dynamic compression.
Type II often confuses diagnosis with tendon rupture.
Clinical Assessment
Physical Exam
- Inspection: "Finger Drop". Wrist can extend but deviates Radially (ECRL acts, ECU fails).
- Power: Test EDC (MCP extension), EIP (Index extension), EPL (Thumb extension).
- Tenodesis: Check passive extension to rule out tendon rupture.
- Pain: Vague ache in proximal forearm (unlike Lateral Epicondylitis which is at the epicondyle).
Pain + Weakness = PIN Syndrome.
Imaging and Electrodiagnostics
MRI
- Mandatory: For any non-traumatic PIN palsy.
- Purpose: To rule out a mass (Lipoma, Ganglion).
- Finding: Denervation edema in supinator/extensors. Mass lesion compressing nerve.
A negative MRI does not exclude dynamic compression.
Management Algorithm
Non-Operative
- Indication: Neuritis (Parsonage-Turner), Transient compression, No mass.
- Splinting: Cock-up dynamic splint (outrigger) to hold fingers in extension (prevent overstretching).
- Time: Observe for 3-6 months.
- Steroids: Limited role unless inflammatory.
Activity modification (avoid pronation/supination) is key.
Surgical Technique
Anterior Approach (Henry)
- Incision: Volar curvilinear.
- Interval: PT / BR.
- Deep: Identify Radial Nerve. Trace it distally.
- Release: Ligate Leash of Henry. Retract ECRB. Identify Arcade of Frohse.
- Action: Divide the arcade and the superficial head of supinator.
Stay on the nerve at all times visually.
Complications
Intraoperative Complications
- Iatrogenic Nerve Injury: Direct injury to PIN during release, especially at the Arcade of Frohse.
- Vascular Injury: Damage to Leash of Henry (radial recurrent vessels) causing significant bleeding.
- Incomplete Release: Failure to release all five compression sites (most commonly missing distal supinator edge).
- ECRB Denervation: Variable innervation can lead to unexpected weakness if motor branch damaged.
- Superficial Radial Nerve: Injury during anterior approach causes sensory loss on dorsal hand.
Meticulous technique with loupe magnification is essential.
Rehabilitation
- Dynamic Splint: Low profile radial nerve palsy splint with metacarpophalangeal extension assist.
- Purpose: Allows active flexion, passive extension. Prevents extensor overstretching.
- Wound Care: Keep incision clean and dry; suture removal at 10-14 days.
- Edema Control: Elevation and gentle active finger movements encouraged.
- Range of Motion: Active-assisted exercises to maintain joint mobility.
- Scar Management: Silicone gel or massage once wound healed.
- Continue Splinting: Night splinting particularly important to prevent contractures.
- Recovery Monitoring: Monitor for "flicker" of EDC - first sign of reinnervation.
- Order of Recovery: Brachioradialis → ECRL → ECRB → Supinator → EDC → EPL.
- Strengthening: Gentle isometrics progressing to resistance as power returns.
Recovery progresses at 1mm per day from site of compression. Sensory re-education is NOT required (pure motor nerve). Full recovery may take 6-12 months depending on severity.
Prognosis
Expected Outcomes by Etiology
- Compression (Arcade): Excellent recovery expected if decompression performed within 6 months; greater than 85% return to full function.
- Mass Lesion (Lipoma): Excellent with excision and neurolysis; function returns in 3-6 months post-surgery.
- Traumatic (Monteggia): Variable; depends on mechanism and timing. Neurapraxia recovers well, neurotmesis requires grafting.
- Inflammatory (RA): Good if synovectomy performed early; ongoing disease may cause recurrence.
- Radial Tunnel Syndrome: Unpredictable; 60-70% success rate for pain relief even with surgery.
Early intervention correlates strongly with better outcomes.
Differential Diagnosis
A "dropped finger" or refractory lateral elbow pain has a wide differential. The decisive discriminators are the presence of motor weakness, the sensory status, and the tenodesis effect.
| Diagnosis | Motor weakness | Sensory loss | Key discriminator |
|---|---|---|---|
| PIN syndrome | Yes (finger/thumb ext, ECU; ECRL spared) | None | Wrist extends but deviates radially; positive tenodesis (tendons intact) |
| Extensor tendon rupture (e.g. Vaughan-Jackson) | No true weakness (mechanical loss) | None | Negative tenodesis: fingers stay flexed on passive wrist flexion |
| High radial nerve palsy (spiral groove) | Yes plus wrist drop (ECRL/BR affected) | Dorsal first webspace | Wrist drop and sensory loss localise proximal to the elbow |
| Radial tunnel syndrome | None (pain only) | None | Pain ~4 cm distal to lateral epicondyle; controversial entity |
| Lateral epicondylitis (tennis elbow) | None | None | Maximal tenderness AT the epicondyle, not over the supinator |
| Wartenberg syndrome (superficial radial n.) | None | Dorsoradial hand | Pure sensory; positive Tinel over distal radial forearm |
| Neuralgic amyotrophy (Parsonage-Turner) | Yes, often patchy/hourglass fascicular | Variable | Antecedent severe pain then palsy; MRI may be mass-negative |
| C7/C8 radiculopathy | Yes, myotomal (multi-nerve) | Dermatomal | Weakness crosses peripheral nerve territories; neck signs |
| Central lesion (stroke) | Yes, upper motor neuron pattern | Variable | Spasticity, hyperreflexia, non-segmental distribution |
Controversies and Areas of Uncertainty
Does pain-only radial tunnel syndrome exist?
The original Roles and Maudsley concept (1972) framed refractory lateral elbow pain as a radial nerve entrapment by analogy to carpal tunnel syndrome. Rosenbaum (1999) argued this analogy is flawed and that true neurogenic compression should produce PIN motor weakness. Surgical decompression for pain alone has unpredictable results, and there are no high-quality randomised trials. State both positions in the viva.
- Anterior versus posterior approach: No randomised data show superiority of Henry versus Thompson exposures; choice is driven by the level of pathology (proximal/arcade favours anterior control; supinator masses favour posterior) and surgeon familiarity.
- Timing of surgery in compressive palsy: Common practice is to decompress a confirmed compressive lesion promptly and to observe imaging-negative palsy for roughly 3 months, but the exact threshold is not standardised. Outcomes worsen with age over 50 and with delay (McGraw, 2018).
- Nerve transfer versus tendon transfer: For recent lesions (under ~12 months), nerve transfer can give superior wrist motion and grip compared with tendon transfer (Bertelli, 2020), but tendon transfer remains the established, microsurgery-free salvage for late or irrecoverable palsy. The optimal algorithm is still debated.
- Hourglass fascicular constriction: Increasingly recognised in spontaneous palsy (within the neuralgic amyotrophy spectrum). Whether to observe, perform neurolysis, resect-and-graft, or transfer is unresolved, and intraoperative findings often dictate the decision.
- Role of imaging: MRI is favoured to exclude a mass, but high-resolution ultrasound increasingly detects fascicular constriction and dynamic compression; the comparative diagnostic accuracy for the specific question of operability is not well defined.
Evidence Base
Arcade of Frohse: the anatomical basis of PIN compression
- Classic anatomical dissection study correlating the arcade of Frohse with PIN paralysis
- The proximal margin of the superficial supinator head is tendinous (a fibrous arcade) in a substantial proportion of adult specimens
- The arcade is membranous, not tendinous, in fetal and infant specimens, suggesting the fibrous arch is acquired with development and use
- Established the arcade of Frohse as the principal site of entrapment in spontaneous PIN palsy
Radial tunnel syndrome: resistant tennis elbow as a nerve entrapment
- Original description of radial tunnel syndrome as a cause of refractory lateral elbow pain ('resistant tennis elbow')
- Patients presented with proximal forearm pain and tenderness over the supinator, without motor deficit
- Reported symptomatic improvement after radial nerve decompression in a series of resistant cases
- Framed the entity by analogy to carpal tunnel syndrome — a comparison later disputed
Disputed radial tunnel syndrome
- Critical review arguing that true neurogenic radial tunnel syndrome is uncommon and is identifiable by focal PIN motor weakness
- Challenges the Roles and Maudsley concept that proximal forearm pain alone represents nerve entrapment
- Recommends reserving the term 'radial tunnel syndrome' for genuinely neurogenic cases
- Calls for controlled evaluation of surgery for 'persistent tennis elbow' rather than adoption by analogy to carpal tunnel syndrome
PIN discontinuity due to lipoma compression
- Two cases of severe PIN compression by a benign lipoma at the elbow producing near-transection (Sunderland grade V) of the nerve
- Proposed a 'sandwich' mechanism: the mass compresses from below while a fibrous supinator band (arcade of Frohse or distal supinator edge) compresses from above
- Demonstrates that an occult soft-tissue mass can cause profound, irreversible nerve injury
- Reinforces that lipoma is a classic and treatable cause of spontaneous PIN palsy
Isolated spontaneous PIN palsy: aetiology and management review
- Comprehensive review categorising spontaneous PIN palsy into compressive and non-compressive (e.g. neuralgic amyotrophy with hourglass fascicular constriction)
- Evidence supports surgical decompression for compressive palsy; conservative management first when no compressive lesion is seen on imaging
- Poorer prognosis with age over 50 years, delay to surgery, and long-standing compression with severe fascicular thinning
- Provides an evidence-based treatment algorithm where one was previously lacking
Nerve versus tendon transfer for radial nerve paralysis
- Comparative series: 14 patients with radial nerve lesions under 12 months underwent nerve transfer (AIN to ECRB branch, FCR branch to PIN); 13 with longstanding palsy underwent tendon transfer (PT-ECRB, FCU-EDC, PL-EPL)
- Nerve transfer gave better wrist flexion–extension range and grasp strength than tendon transfer
- Half of the tendon transfer patients had to flex the wrist to fully extend the fingers; permanent radial deviation occurred in 5 of 13
- A roughly 30-degree thumb MCP extension lag (poor EPL recovery) persisted after BOTH procedures
Radial nerve tendon transfers (technique and outcomes review)
- Review of tendon transfer reconstruction for irrecoverable radial nerve palsy (loss of wrist, finger and thumb extension)
- Common donors: pronator teres (to ECRB) for wrist extension, wrist flexors and finger flexors for digital extension
- Transfer sets are classified by the donor used to power the extensor digitorum communis (FCU, FCR or FDS variants)
- Good functional results are typical because these are positional transfers that do not demand high power
Ultrasound of the radial nerve in palsy: imaging–surgical correlation
- Prospective study of 11 patients with radial nerve palsy after humeral shaft fracture, with US compared against surgical inspection in 5 operated cases
- US correctly identified the damaged nerve in all 5 surgically explored patients (entrapment between fragments, transection, laceration, nerve riding on a fragment, nerve buried in callus)
- US confirmed nerve continuity in all 6 conservatively managed patients who recovered
- Established high-resolution ultrasound as a feasible, accurate tool for assessing radial nerve injury
Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Spontaneous Drop
"A 45-year-old woman presents with inability to extend her fingers. It started gradually over 3 weeks. No trauma. Wrist extension is present but deviates. What is the diagnosis?"
Scenario 2: The Monteggia
"A child has a Monteggia fracture (Ulnar fracture, Radial head dislocation) reduced 6 weeks ago. Still cannot extend thumb."
Scenario 3: Pain Only
"A tennis player complains of lateral elbow pain. Treated as 'Tennis Elbow' for 6 months with no relief. Injections failed. Exam shows pain on resisted middle finger extension."
Scenario 4: Rheumatoid Patient
"A 55-year-old woman with known rheumatoid arthritis develops progressive weakness of finger extension over 4 weeks. She has swelling around the elbow. How do you differentiate the cause?"
MCQ Practice Points
Anatomy
Q: What is the most common site of PIN compression? A: The Arcade of Frohse (proximal edge of Supinator).
Clinical Signs
Q: Why does the wrist deviate radially in PIN palsy? A: ECRL (Radial N) is intact, but ECU (PIN) is paralyzed.
Diagnosis
Q: How do you differentiate PIN palsy from multiple tendon ruptures (Vaughan-Jackson)? A: Tenodesis test. Passive wrist flexion should extend the fingers if tendons are intact.
Syndromes
Q: What is Wartenberg's Syndrome? A: Compression of the Superficial Radial Nerve (Sensory only) causing dorsal hand paresthesia.
Mass Lesions
Q: What is the most common soft tissue mass causing spontaneous PIN palsy? A: Lipoma. Always order MRI for spontaneous PIN palsy to rule out a mass lesion.
Guidelines, Registries & Global Practice
PIN syndrome and radial tunnel syndrome are uncommon and have no dedicated society guideline or arthroplasty-style registry. The "evidence" is therefore best summarised as global epidemiology, where the major society positions converge or differ, and how practice changes with available resources.
Global Epidemiology:
- Compressive radial neuropathy at the elbow is rare relative to carpal and cubital tunnel syndrome; isolated spontaneous PIN palsy is described mainly in case series and reviews rather than population studies (McGraw, J Hand Surg Eur Vol 2018).
- No sex predominance is firmly established; reported cases span young adults (often neuralgic amyotrophy / Parsonage-Turner) to older adults (compressive and mass lesions).
- Recognised causes worldwide: the arcade of Frohse and supinator fibrous bands, space-occupying lesions (lipoma is the classic solid mass, also ganglion, synovial cyst, nerve sheath tumour), rheumatoid elbow synovitis, Monteggia and radial head fracture–dislocation, and iatrogenic injury during radial head or proximal radius surgery.
Side-by-Side Society Positions:
| Body / Source | Position relevant to PIN / radial tunnel |
|---|---|
| AAOS (US) | Lateral elbow pain pathways emphasise distinguishing lateral epicondylitis from radial tunnel syndrome; surgery for pain-only radial tunnel is regarded as having a weak evidence base. |
| BOA / BSSH (UK) | Spontaneous finger drop is a red flag requiring imaging (MRI) and hand-surgery referral to exclude a compressive mass before labelling it neuritis. |
| AO Foundation | PIN at risk in Monteggia and radial head/neck injuries and during proximal radius approaches; advocates nerve identification and protection, especially with the posterolateral (Kocher) and Thompson exposures. |
| EFORT / European consensus | Supports decompression for confirmed compressive motor palsy; recommends caution and shared decision-making for pain-only radial tunnel syndrome given controversial outcomes. |
Diagnostic and Treatment Convergence (where societies agree):
- A true motor PIN palsy with a compressive lesion warrants decompression; an imaging-negative palsy (possible neuralgic amyotrophy) is observed first.
- MRI is the key investigation for any non-traumatic PIN palsy to exclude a mass; ultrasound is a useful, operator-dependent adjunct and can be dynamic.
- Pain-only radial tunnel syndrome is the contested zone: most bodies advise exhausting non-operative care and counselling the patient that surgical results for pain relief are unpredictable.
High-Resource vs Limited-Resource Practice:
- High-resource settings: ready access to MRI, high-resolution nerve ultrasound, and electrodiagnostics; reconstruction may include nerve transfer for recent lesions (Bertelli, J Hand Surg Am 2020) as well as tendon transfer.
- Limited-resource settings: diagnosis is more clinical (finger drop with preserved radial-deviated wrist extension and normal sensation), imaging may be confined to radiographs and ultrasound, and tendon transfer is the dominant, durable salvage because it needs no microsurgical infrastructure and gives reliable positional results (Cheah, Hand Clin 2016).
- Rehabilitation everywhere centres on a dynamic radial-nerve-palsy outrigger splint to maintain digital extension and prevent overstretching while reinnervation or healing proceeds; serial clinical and (where available) electrodiagnostic review guides the timing of surgery.
Clinical summary
Anatomy
- •FREAS (Fibrous, Recurrent, ECRB, Arcade, Supinator)
- •Arcade of Frohse = #1 Site (70% fibrous)
- •ECRL Spared (innervated by Radial Nerve proximally)
- •PIN = pure motor branch of Radial nerve
- •Supinator course: 4-5cm within muscle
Clinical
- •Finger Drop (Not Wrist Drop = PIN vs High Radial)
- •Radial Deviation on wrist extension (ECRL intact, ECU paralyzed)
- •Tenodesis Test (rule out Vaughan-Jackson tendon rupture)
- •Normal sensation (Superficial Radial branches off proximally)
- •Middle Finger Test: pain/weakness 4cm distal to epicondyle
Treatment
- •MRI mandatory (rule out lipoma/mass)
- •Observe 3-6 months if no mass
- •Release (Henry or Thompson approach)
- •Transfers if no recovery at 1 year (PT-ECRB, FCU-EDC, PL-EPL)
- •Splint (dynamic outrigger) prevents overstretching