Shepherd Fracture | Cedell Fracture | FHL Impingement
POSTERIOR PROCESS FRACTURES
Critical Must-Knows
- Posterior process has 2 parts: Lateral tubercle (Shepherd fracture) and medial tubercle (Cedell fracture)
- FHL impingement: Lateral tubercle fracture can cause FHL tendon impingement - pain with great toe flexion
- Often missed: Subtle on X-ray, may be misdiagnosed as ankle sprain or os trigonum
- ORIF if displaced: Displacement greater than 2mm requires ORIF to prevent nonunion and FHL impingement
- Excision for small fragments: Small fragments causing impingement can be excised
Clinical Pearls
- "Shepherd fracture = lateral tubercle of posterior process, FHL impingement risk
- "Cedell fracture = medial tubercle of posterior process, rare
- "FHL impingement causes pain with great toe flexion (hallux flexor hallucis longus)
- "Often missed - high index of suspicion, CT if suspected
Critical Posterior Process Talus Fracture Exam Points
Two Parts
Posterior process has 2 parts: Lateral tubercle (Shepherd fracture) and medial tubercle (Cedell fracture). Lateral tubercle more common, causes FHL impingement. Medial tubercle rare.
FHL Impingement
Lateral tubercle fracture can cause FHL impingement - Flexor hallucis longus tendon runs between lateral and medial tubercles. Fracture causes pain with great toe flexion. ORIF or excision relieves impingement.
Often Missed
Often missed initially - Subtle on X-ray, may be misdiagnosed as ankle sprain or os trigonum. High index of suspicion needed. CT recommended if suspected but X-ray negative.
ORIF if Displaced
Displacement greater than 2mm requires ORIF - Prevents nonunion and FHL impingement. Small fragments causing impingement can be excised. Non-displaced fractures can be treated conservatively.
Posterior Process Talus Fractures - Quick Decision Guide
| Type | Location | Treatment | Complication |
|---|---|---|---|
| Lateral tubercle | Shepherd fracture | ORIF or excision | FHL impingement |
| Medial tubercle | Cedell fracture | ORIF if displaced | Rare |
| Both | Complete process | ORIF | FHL impingement |
SCPosterior Process Parts
| S | Shepherd Lateral tubercle fracture |
| C | Cedell Medial tubercle fracture (rare) |
| S | Shepherd Lateral tubercle fracture |
| C | Cedell Medial tubercle fracture (rare) |
Hook:SC: Shepherd (lateral), Cedell (medial)!
FHLFHL Impingement
| F | Flexor Flexor hallucis longus tendon |
| H | Hallucis Great toe flexor |
| L | Longus Runs between tubercles |
| F | Flexor Flexor hallucis longus tendon |
| H | Hallucis Great toe flexor |
| L | Longus Runs between tubercles |
Hook:FHL: Flexor Hallucis Longus - runs between lateral and medial tubercles, impingement causes pain with great toe flexion!
DOETreatment Decision
| D | Displaced Greater than 2mm requires ORIF |
| O | ORIF For large fragments |
| E | Excision For small fragments causing impingement |
| D | Displaced Greater than 2mm requires ORIF |
| O | ORIF For large fragments |
| E | Excision For small fragments causing impingement |
Hook:DOE: Displaced over 2mm ORIF, Excision for small fragments!
Overview and Epidemiology
Posterior process talus fractures are rare injuries involving the posterior process of the talus, which has two parts: the lateral tubercle (Shepherd fracture) and the medial tubercle (Cedell fracture). These fractures can cause FHL impingement and are often missed initially.
Definition
Posterior process talus fracture: Fracture of the posterior process of the talus, which has:
- Lateral tubercle: More common, Shepherd fracture
- Medial tubercle: Rare, Cedell fracture
- FHL groove: Between the two tubercles
Shepherd fracture: Lateral tubercle of posterior process
- More common than medial
- Causes FHL impingement
- Named after Shepherd
Cedell fracture: Medial tubercle of posterior process
- Rare
- Less common than lateral
- Named after Cedell
Epidemiology
- Incidence: Less than 1% of talus fractures
- Age: Peak 20-40 years (sports, trauma)
- Gender: No clear predominance
- Mechanism: Forced plantarflexion, direct trauma
- Associated injuries: Ankle injuries, other foot trauma
FHL Impingement
FHL (Flexor Hallucis Longus) tendon runs between lateral and medial tubercles of posterior process - Lateral tubercle fracture can cause FHL impingement, leading to pain with great toe flexion. ORIF or excision relieves impingement.
Anatomy and Pathophysiology
Posterior Process Anatomy
Posterior process of talus:
- Location: Posterior aspect of talus body
- Two parts: Lateral tubercle and medial tubercle
- FHL groove: Between the two tubercles
- Function: Attachment site for ligaments, forms FHL groove
Lateral tubercle (Shepherd):
- Size: Larger than medial
- Location: Lateral aspect of posterior process
- Function: Forms lateral border of FHL groove
- Fracture: More common, causes FHL impingement
Medial tubercle (Cedell):
- Size: Smaller than lateral
- Location: Medial aspect of posterior process
- Function: Forms medial border of FHL groove
- Fracture: Rare, less common than lateral
FHL (Flexor Hallucis Longus) tendon:
- Course: Runs between lateral and medial tubercles
- Function: Flexes great toe
- Impingement: Fracture can cause impingement
Pathophysiology
Injury mechanism:
- Forced plantarflexion: Classic mechanism
- Direct trauma: To posterior ankle
- Avulsion: Ligament avulsion
FHL impingement:
- Mechanism: Fracture fragment impinges on FHL tendon
- Symptoms: Pain with great toe flexion
- Treatment: ORIF or excision relieves impingement
Why often missed:
- Subtle on X-ray: May be obscured
- Misdiagnosed: As os trigonum or ankle sprain
- CT needed: Often requires CT for diagnosis
Classification Systems
Location-Based Classification
Lateral tubercle (Shepherd fracture):
- More common
- Causes FHL impingement
- Treatment: ORIF or excision
Medial tubercle (Cedell fracture):
- Rare
- Less common than lateral
- Treatment: ORIF if displaced
Both tubercles:
- Complete posterior process fracture
- Treatment: ORIF
Location determines treatment approach.
Clinical Assessment
History
Symptoms:
- Posterior ankle pain: Pain in posterior ankle
- FHL impingement: Pain with great toe flexion (lateral tubercle)
- Swelling: Localised to posterior ankle
- Difficulty walking: Pain with weight bearing
Mechanism:
- Forced plantarflexion
- Direct trauma to posterior ankle
- Sports injuries
Physical Examination
Inspection:
- Swelling in posterior ankle
- Ecchymosis (may be delayed)
- Deformity (rare)
Palpation:
- Tenderness over posterior process
- FHL impingement test (pain with great toe flexion)
- Ankle joint usually not tender
Range of Motion:
- Ankle ROM may be limited
- Great toe flexion painful (FHL impingement)
- Plantarflexion may be limited
Special tests:
- FHL impingement test: Pain with active great toe flexion
- Posterior process palpation: Tenderness over posterior process
Clinical Examination Key Point
FHL impingement test is key - Pain with active great toe flexion indicates FHL impingement from lateral tubercle fracture. This is pathognomonic for posterior process fracture with impingement.
Differential Diagnosis
The single most important distinction is an acute fracture versus a symptomatic os trigonum, because the treatment, prognosis and medicolegal consequences of a missed fracture differ greatly. Use the table below to structure the differential in the viva.
Differential Diagnosis of Posterior Ankle Pain
| Diagnosis | Key clinical clue | Imaging discriminator | Management contrast |
|---|---|---|---|
| Posterior process fracture | Acute trauma, point tenderness, pain on passive FHL stretch | Sharp irregular fracture line, marrow oedema on MRI, sclerotic acutely-displaced fragment on CT | May need ORIF or excision if displaced |
| Symptomatic os trigonum | Insidious, repetitive plantarflexion (dancers, footballers) | Smooth corticated ossicle with rounded margins, no marrow oedema | Rest, then excision/hindfoot endoscopy if refractory |
| Posterior ankle (os trigonum) impingement syndrome | Pain at end-range plantarflexion, positive forced-plantarflexion test | May show os trigonum or Stieda process, soft-tissue oedema | Activity modification, injection, endoscopic decompression |
| Isolated FHL tenosynovitis | Pain along FHL behind medial malleolus, crepitus, triggering | Fluid in FHL sheath on MRI, no bony fragment | Conservative, FHL release if refractory |
| Lateral process fracture (snowboarder's) | Dorsiflexion/inversion injury, lateral tenderness below fibula | Fragment at lateral process, not posterior, on mortise/CT | ORIF or excision per fragment size |
| Lateral ankle sprain | Inversion injury, ATFL tenderness, negative bony signs | Normal bone, soft-tissue swelling only | Functional rehabilitation |
Investigations
Standard X-ray Protocol
Lateral view (best view):
- Shows posterior process
- Look carefully - often subtle
- May be confused with os trigonum
AP view:
- May show fracture
- Less reliable than lateral
Key point: Often missed on initial X-rays - high index of suspicion needed.
Management Algorithm
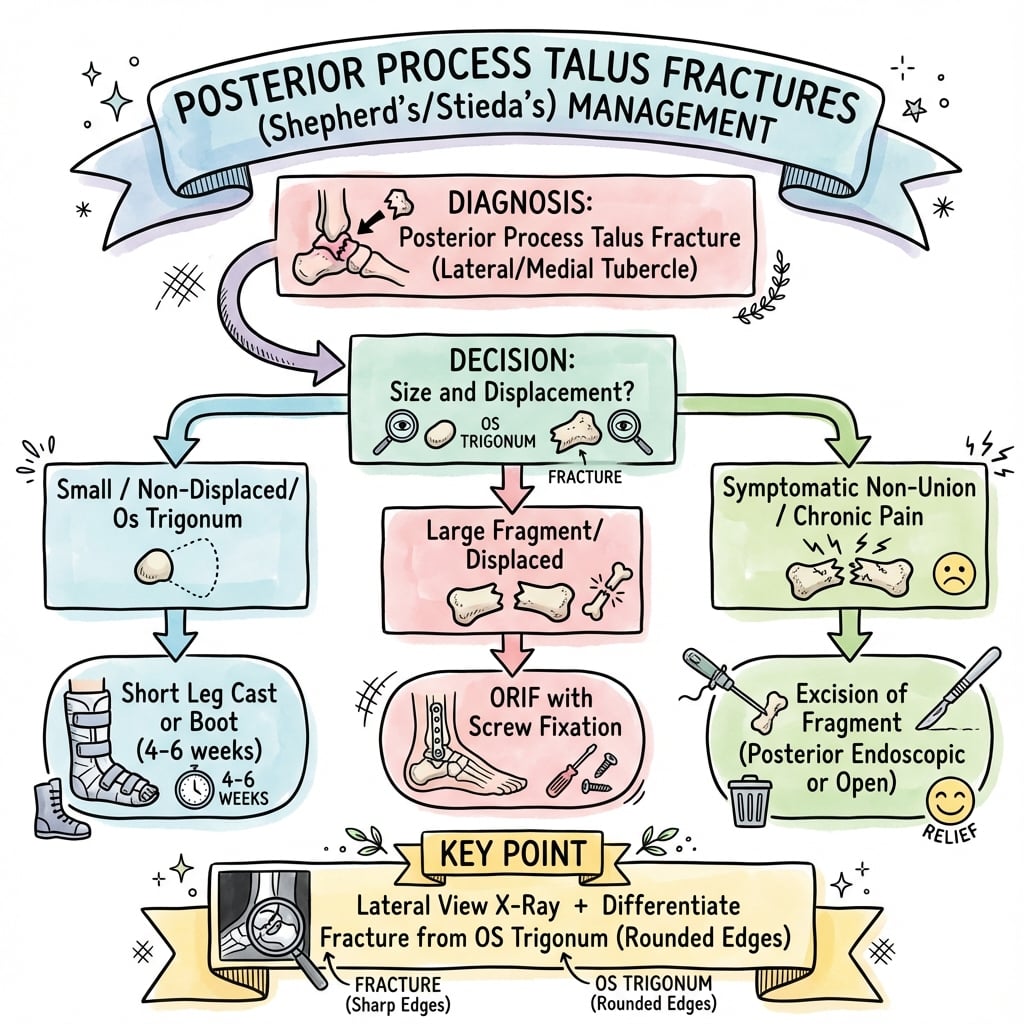
Management Pathway
Posterior Process Talus Fracture Management
Often missed initially - look carefully on lateral X-ray. CT recommended if suspected clinically but X-ray negative. FHL impingement test is key clinical test.
If non-displaced (less than 2mm step-off) and no FHL impingement, conservative treatment with cast and non-weight bearing for 6-8 weeks. Success rate 85-90%.
If displaced (greater than 2mm) and large fragment, ORIF preferred. Relieves FHL impingement, prevents nonunion. Success rate 80-90%.
If displaced and small fragment or causing FHL impingement, excision acceptable. Relieves impingement, better than malunion. Success rate 75-85%.
Surgical Technique
ORIF Technique (Preferred for Large Fragments)
Indications:
- Large fragment (reconstructible)
- Displaced (greater than 2mm)
- FHL impingement
Approach:
- Posteromedial or posterolateral approach
- Expose posterior process
- Protect FHL tendon
Technique:
- Exposure: Posteromedial or posterolateral approach
- Protection: Identify and protect FHL tendon
- Reduction: Anatomic reduction of fragment
- Fixation: Lag screws (2.0-2.7mm) or mini-fragment screws
- Verification: Confirm reduction and hardware position fluoroscopically
Advantages:
- Relieves FHL impingement
- Prevents nonunion
- Better outcomes than excision for large fragments
ORIF preferred for large fragments.
Complications
| Complication | Incidence | Risk Factors | Prevention/Management |
|---|---|---|---|
| FHL impingement | 20-30% | Lateral tubercle fracture | ORIF or excision relieves |
| Nonunion | 10-15% | Displacement, inadequate fixation | Rigid fixation, bone graft |
| Missed diagnosis | 30-40% | Subtle on X-ray | High index of suspicion, CT |
| Wound complications | 5-10% | Posterior approach | Careful technique |
FHL Impingement
20-30% incidence (if untreated):
- Cause: Lateral tubercle fracture impinges on FHL tendon
- Symptoms: Pain with great toe flexion
- Prevention: ORIF or excision relieves impingement
- Management: Surgical treatment (ORIF or excision)
Nonunion
10-15% incidence:
- Cause: Displacement, inadequate fixation
- Prevention: Rigid fixation, bone graft if needed
- Management: Revision fixation with bone graft
Postoperative Care
Immediate Postoperative
- Immobilisation: Short leg cast or boot
- Weight bearing: Non-weight bearing (6-8 weeks)
- ROM: Ankle ROM after cast removal
- PT: FHL stretching and strengthening
Rehabilitation Protocol
Weeks 0-6:
- Short leg cast, non-weight bearing
- Elevation to reduce swelling
- Ankle ROM exercises (if stable)
Weeks 6-8:
- Cast removal
- Transition to walking boot
- Progressive weight bearing
Weeks 8-12:
- Full weight bearing
- Progressive activity
- Return to sport (3-4 months)
Outcomes and Prognosis
Overall Outcomes
ORIF (large fragments):
- Success rate: 80-90% (union, pain relief)
- Functional outcomes: 75-85% return to pre-injury level
- FHL impingement: Relieved in 90-95%
Excision (small fragments):
- Success rate: 75-85% (pain relief)
- Functional outcomes: 70-80% return to pre-injury level
- FHL impingement: Relieved in 85-90%
Conservative (non-displaced):
- Success rate: 85-90% (union, pain relief)
- Functional outcomes: 80-85% return to pre-injury level
- FHL impingement: Rare if non-displaced
Long-Term Prognosis
FHL impingement resolution:
- With proper treatment: 90-95% relief of impingement
- Without treatment: 20-30% develop chronic impingement
- Risk factors: Displacement, delayed treatment
Evidence Base
Talar Process Fractures — Anatomy, Mechanism and Management
- Posterior process = medial + lateral tubercle, FHL groove between them
- Mechanism: forced hyperplantarflexion/inversion or PTFL avulsion
- Missed diagnosis risks malunion, nonunion and subtalar arthritis
Outcomes After Operative vs Nonoperative Treatment
- 29 patients, mean 6-year follow-up, mean AOFAS 78.7
- Operative management gave good function in extended fractures
- Non-operative care justified only in selected minor injuries
Medial Tubercle (Cedell) Fractures — Systematic Review
- 33 pooled Cedell cases; 58% sport, 73% misdiagnosed as sprain
- Diagnosis often delayed beyond one year
- Immobilisation, ORIF or excision all give reasonable-to-good results
Talar Fracture Patterns and Radiographic Sensitivity (CT)
- Posterior tubercle = 21% of talar body fractures
- Radiographic sensitivity only 74% vs CT
- High rate of associated dislocation and adjacent fracture
Safe Zone for Percutaneous Posterior Screw Fixation (3D CT)
- Lateral tubercle is optimal posterior-to-anterior screw entry
- Safe-zone geometry defined on 100 CT scans
- 3D planning may shorten surgery and reduce complications
Cedell Fracture — Diagnostic Dilemma and Fixation
- Painful passive FHL movement is a diagnostic clue
- 30-degree external-rotation lateral view aids detection
- Mini-open ORIF achieved union and full ROM at 6 months
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Lateral Tubercle Fracture with FHL Impingement
"A 28-year-old athlete presents with posterior ankle pain after forced plantarflexion injury. Clinical examination shows pain with active great toe flexion (FHL impingement test positive). Lateral X-ray shows fracture of lateral tubercle of posterior process. CT shows 3mm displacement."
Scenario 2: Small Fragment with FHL Impingement
"A 25-year-old dancer presents with posterior ankle pain and pain with great toe flexion. Clinical examination shows positive FHL impingement test. CT shows small comminuted fragment of lateral tubercle (under 25% of process) with 4mm displacement. The fragment is not reconstructible."
Scenario 3: Chronic 'Ankle Sprain' That Will Not Settle (Cedell)
"A 34-year-old recreational footballer is referred with 14 months of persistent posteromedial ankle pain after an inversion injury initially diagnosed and treated as a sprain. Plain films were reported as normal. He has posteromedial tenderness and pain on passive great toe extension. How do you approach this?"
MCQ Practice Points
Shepherd vs Cedell
Q: What is the difference between Shepherd and Cedell fractures? A: Shepherd fracture = lateral tubercle of posterior process (more common, causes FHL impingement) - Cedell fracture = medial tubercle of posterior process (rare). Both are parts of posterior process of talus.
FHL Impingement
Q: What causes FHL impingement in posterior process talus fractures? A: Lateral tubercle fracture impinges on FHL tendon - FHL (Flexor Hallucis Longus) tendon runs between lateral and medial tubercles. Lateral tubercle fracture causes pain with great toe flexion. ORIF or excision relieves impingement.
FHL Impingement Test
Q: How do you test for FHL impingement? A: Active great toe flexion test - Pain with active great toe flexion indicates FHL impingement from lateral tubercle fracture. This is pathognomonic for posterior process fracture with impingement.
Treatment Decision
Q: When is ORIF preferred over excision for posterior process talus fractures? A: Large fragments (reconstructible) with displacement greater than 2mm - ORIF preserves anatomy and relieves FHL impingement (80-90% good results). Excision is acceptable for small comminuted fragments causing impingement (75-85% good results).
Missed Diagnosis
Q: Why are posterior process talus fractures often missed initially? A: Subtle on X-ray, often misdiagnosed as os trigonum or ankle sprain - 30-40% are missed initially. High index of suspicion needed, especially with FHL impingement symptoms. CT recommended if suspected clinically but X-ray negative.
Controversies and Areas of Uncertainty
The evidence base for posterior process talus fractures is limited to small retrospective series and case reports — there are no randomised trials. The following points are genuine areas of debate worth raising in a viva.
ORIF vs excision threshold
There is no agreed fragment-size cut-off for fixation versus excision. The decision rests on whether the fragment is reconstructible, the degree of subtalar articular involvement and surgeon experience rather than a validated number. Excision (open or endoscopic) gives reliable symptom relief for small fragments.
Open vs endoscopic surgery
Two-portal hindfoot endoscopy is increasingly used for excision and even fixation, with good return-to-sport data in athletes, but comparative evidence against open techniques is absent and the learning curve and neurovascular proximity are real.
Displacement cut-off
The widely quoted "greater than 2mm" surgical threshold is pragmatic and extrapolated from intra-articular fracture principles, not derived from outcome studies specific to this fracture.
True mechanism and origin
Whether medial tubercle (Cedell) fractures are deltoid avulsions, FHL-retinaculum avulsions or direct compression injuries remains unresolved, with case evidence supporting more than one mechanism.
Guidelines, Registries & Global Practice
These are rare injuries with no dedicated society guideline and no registry capture (talar process fractures are not separately tracked by arthroplasty registries such as the NJR, AJRR or AOANJRR, which record joint replacements rather than fixation of small process fractures). Practice is therefore guided by trauma principles and the small published literature, summarised below for a global readership.
Where Recommendations Converge and Differ
| Source / framework | Position on posterior process fractures | Practical implication |
|---|---|---|
| AO Foundation (talus principles) | Anatomic reduction and stable fixation of displaced intra-articular talar fragments; protect FHL and neurovascular bundle via posteromedial/posterolateral approaches | Reconstruct large displaced fragments; lag-screw or mini-fragment fixation |
| EFORT Open Reviews (Majeed & McBride 2018) | No consensus on optimal treatment; decision driven by size, location, displacement, cartilage damage and subtalar instability | Individualise — non-op for non-displaced, ORIF or excision for displaced |
| Foot/ankle specialist literature (e.g. Amsterdam group) | Endorses two-portal hindfoot endoscopy for excision in athletes; supports operative management of extended fractures | Consider minimally invasive excision for small fragments in active patients |
| General trauma principle (all systems) | High index of suspicion; CT for any suspected but radiographically occult posterior ankle fracture | Plain-film sensitivity is only ~74% — image early to avoid missed injury |
Global epidemiology and practice variation
- Rarity and demographics: posterior process fractures are uncommon (the posterior tubercle accounts for around 21% of talar body fractures in CT-based trauma-centre data, but isolated process fractures are far rarer). They cluster in young, active adults — sport (especially football, dance, running and climbing) and falls from height are the dominant mechanisms worldwide.
- High-resource settings: ready CT/MRI access, fluoroscopy and hindfoot endoscopy support early diagnosis and minimally invasive excision or fixation; missed-diagnosis rates fall when CT is used liberally for unresolving posterior ankle pain.
- Limited-resource settings: reliance on plain radiographs increases missed and delayed diagnoses; pragmatic management leans toward immobilisation for presumed minor injuries and open excision/ORIF when surgery is indicated, since advanced imaging and endoscopic equipment may be unavailable.
Orthopaedic Exam Relevance
Posterior process talus fractures are a common viva topic. Know that Shepherd fracture = lateral tubercle (FHL impingement), Cedell fracture = medial tubercle (rare), FHL impingement test = pain with great toe flexion, displacement greater than 2mm requires ORIF, ORIF preferred for large reconstructible fragments, excision acceptable for small fragments, and that these injuries are frequently missed because plain-film sensitivity is only around 74% — request CT when suspected. Be prepared to discuss FHL impingement, the differential against os trigonum, and the ORIF-versus-excision decision.
POSTERIOR PROCESS TALUS FRACTURES
Clinical summary
Key Concepts
- •Posterior process has 2 parts: lateral tubercle (Shepherd) and medial tubercle (Cedell)
- •FHL tendon runs between lateral and medial tubercles
- •Lateral tubercle fracture causes FHL impingement
- •Often missed initially (30-40%) - high index of suspicion needed
Classification
- •Shepherd fracture: Lateral tubercle (more common, FHL impingement)
- •Cedell fracture: Medial tubercle (rare)
- •Non-displaced: Less than 2mm - conservative (85-90% good results)
- •Displaced: Greater than 2mm - ORIF or excision (75-85% good results)
- •Tubercle Location: Lateral (Shepherd) vs Medial (Cedell)
Treatment
- •Non-displaced, no impingement: Conservative (cast, NWB 6-8 weeks)
- •Large fragment, displaced: ORIF (relieves impingement, 80-90% good results)
- •Small fragment, impingement: Excision (relieves impingement, 75-85% good results)
- •FHL impingement: Requires surgical treatment (ORIF or excision)
Surgical Technique
- •ORIF: Posteromedial or posterolateral approach, protect FHL, lag screws (2.0-2.7mm)
- •Excision: Same approach, remove fragment, smooth edges
- •Protect FHL tendon throughout
- •Verify impingement relieved (test great toe flexion)
Complications
- •FHL impingement: 20-30% if untreated, 90-95% relief with surgery
- •Nonunion: 10-15% (prevent with rigid fixation)
- •Missed diagnosis: 30-40% initially missed
- •Wound complications: 5-10% (posterior approach)