Congenital Popliteal & Multiple Webbing
- A PTERYGIUM is a congenital SKIN/SOFT-TISSUE WEB that bridges the FLEXOR aspect of a joint and tethers it in FIXED FLEXION; the pterygium syndromes are a group in which such webs cause congenital contractures, and the orthopaedic challenge is that the web contains shortened skin, fascia, muscle/tendon and - critically - NEUROVASCULAR structures.
- POPLITEAL PTERYGIUM SYNDROME (PPS) is a rare AUTOSOMAL-DOMINANT condition (IRF6 mutations, allelic with Van der Woude syndrome) featuring a POPLITEAL WEB that produces a FIXED FLEXION DEFORMITY of the KNEE, commonly together with OROFACIAL CLEFTING (cleft lip/palate, lower-lip pits), GENITAL anomalies, SYNDACTYLY and FOOT deformity (e.g. equinovarus) - so it is a multisystem syndrome, not just a knee problem.
- The MULTIPLE PTERYGIUM SYNDROME (Escobar) has WEBS across MULTIPLE joints (neck, axilla, antecubital fossa, popliteal fossa) with multiple congenital contractures, SCOLIOSIS, short stature and characteristic facies (a lethal antenatal form also exists) - it is a distinct, more generalised entity.
- The CRITICAL surgical point is that the NEUROVASCULAR bundle, including the SCIATIC NERVE, is often SHORTENED and abnormally placed (superficially, within the free edge of the popliteal web), so the limiting factor in correcting the knee flexion is usually the SHORTENED NERVE rather than skin alone, and the nerve is at risk during release.
- ASSESSMENT therefore requires careful evaluation of the contracture, the soft-tissue deficiency, and the neurovascular anatomy (imaging/angiography as needed), plus identification of the associated anomalies (clefting, genital, foot) and the genetic diagnosis; the whole child is assessed, not just the web.
- MANAGEMENT is STAGED SURGICAL release and reconstruction with rehabilitation: skin lengthening (multiple Z-PLASTY / local flaps), excision of the fibrotic band, release of the contracted soft tissues, and correction of associated foot deformity - protecting (and, where the shortened nerve is the limit, addressing) the neurovascular bundle; full correction in one stage is often impossible because of the shortened nerve, so gradual/staged correction and realistic functional goals are key.
- CORRECTION IS OBTAINABLE BUT NOT DURABLE, and this is the number most candidates miss. Gradual Ilizarov correction straightened every knee in the largest PPS series, yet 6 of 8 children needed the whole correction REPEATED at a mean of 3-4 years, and 5 developed posterior tibial subluxation or dislocation, always alongside recurrence. Counsel the family for repeat surgery and watch the knee for posterior subluxation.
- THERE IS NO GUIDELINE. The pooled world literature is about 58 patients and 87 limbs from 32 mostly single-case reports, and both the meta-analysis and the recent case reports state that no treatment guideline or classification exists. In that pooled comparison the Ilizarov fixator gave the best mobility but the most sessions and highest complication rate, while FEMORAL SHORTENING OSTEOTOMY achieved correction with the fewest sessions and no reported complications - a favourable but uncontrolled signal, not proven superiority.
- “Pterygium = congenital flexor-surface web -> fixed flexion deformity (skin, fascia + NEUROVASCULAR structures shortened within it).
- “Popliteal pterygium syndrome = autosomal dominant (IRF6, allelic with Van der Woude): popliteal web + fixed knee flexion + orofacial CLEFTING + genital/syndactyly/foot anomalies. Escobar = MULTIPLE-joint webs + scoliosis.
- “KEY: the SCIATIC NERVE/neurovascular bundle is shortened and abnormally superficial WITHIN the popliteal web - it (not skin) often limits correction and is at risk. Treat by STAGED release (Z-plasty/band excision/contracture release) + rehab; protect the nerve.
- “RECURRENCE IS THE RULE: Ilizarov straightened 11/11 knees, but 6 of 8 children needed re-correction at 3-4 years and 5 had posterior tibial subluxation/dislocation. No guideline exists - the whole literature is ~58 patients/87 limbs.
A popliteal web with fixed knee flexion + orofacial clefting, genital/syndactyly/foot anomalies = popliteal pterygium syndrome (autosomal dominant, IRF6). Escobar = webs across multiple joints + scoliosis.
The sciatic nerve/neurovascular bundle is shortened and lies superficially within the web - it usually limits correction and is at risk during release. Plan staged correction.
The Entities & The Surgical Challenge
A pterygium is a congenital flexor-surface web that tethers a joint in fixed flexion, containing shortened skin, fascia and neurovascular structures. Popliteal pterygium syndrome (autosomal dominant, IRF6, allelic with Van der Woude) gives a popliteal web with fixed knee flexion plus orofacial clefting, genital anomalies, syndactyly and foot deformity. Multiple pterygium syndrome (Escobar) has webs across multiple joints (neck/axilla/elbow/knee) with congenital contractures and scoliosis. The critical surgical issue is that the sciatic nerve/neurovascular bundle is shortened and abnormally superficial within the web, so the shortened nerve - not the skin - often limits correction and is at risk during release.
Assessment & Management
- Assess: the contracture, soft-tissue deficiency, and neurovascular anatomy (imaging/angiography as needed); identify associated anomalies (clefting, genital, foot) and make the genetic diagnosis.
- Surgery (staged): skin lengthening with multiple Z-plasty/local flaps, excision of the fibrotic band, release of contracted soft tissues, and correction of foot deformity - protecting the neurovascular bundle.
- Limited by the nerve: because the shortened sciatic nerve often limits knee extension, plan gradual/ staged correction (and accept realistic functional goals) rather than forcing full one-stage correction.
- Multidisciplinary: plastic/orthopaedic surgery, genetics, and management of the cleft/genital anomalies.
The defining surgical hazard in popliteal pterygium syndrome is the neurovascular bundle within the web. The sciatic nerve (and the popliteal vessels) is frequently shortened and lies abnormally superficially, often along the free edge of the web, so the limiting structure when correcting the fixed knee flexion is usually the shortened nerve rather than the skin or fascia. Attempting to straighten the knee fully in a single stage risks traction injury to the nerve and vascular compromise; correction must instead be planned in stages, with careful identification and protection of the neurovascular bundle, skin lengthening by multiple Z-plasty or flaps, excision of the fibrotic band and graded release, sometimes accepting a degree of residual flexion to preserve nerve function. Because popliteal pterygium syndrome is a multisystem condition, the child also needs assessment and management of the associated orofacial clefting, genital anomalies and foot deformity, and genetic diagnosis/ counselling, within a multidisciplinary team.
The Genetics of Escobar Syndrome
- The gene and inheritance. Escobar syndrome is autosomal recessive, caused by CHRNG mutations - the gene for the gamma subunit of the fetal acetylcholine receptor (the AChR used at the neuromuscular junction before birth, later replaced by the adult epsilon-subunit receptor). This is a different gene and inheritance from popliteal pterygium syndrome (IRF6, autosomal dominant).
- Why the webs form. Loss of fetal AChR function impairs fetal neuromuscular transmission, causing reduced fetal movement (akinesia); joints held immobile in utero develop contractures and pterygia across the flexor surfaces - part of the fetal akinesia deformation sequence (with pulmonary hypoplasia, micrognathia, IUGR, and antenatally cystic hygroma/polyhydramnios).
- The lethal end. Lethal multiple pterygium syndrome is the severe end of the same fetal-akinesia/AChR-deficiency spectrum (CHRNG and other fetal-AChR-pathway genes), causing fetal or neonatal death from severe akinesia and pulmonary hypoplasia.
Q: What is the genetic basis of Escobar (multiple pterygium) syndrome, and how does it differ from popliteal pterygium syndrome?
A: Escobar = autosomal recessive, CHRNG mutation (the gamma subunit of the fetal acetylcholine receptor) → impaired fetal neuromuscular transmission → reduced fetal movement (akinesia) → contractures + multi-joint pterygia (the fetal akinesia deformation sequence, with pulmonary hypoplasia/IUGR). The lethal multiple pterygium syndrome is the severe end (CHRNG + other fetal-AChR genes → fetal/neonatal death). This contrasts with popliteal pterygium syndrome (IRF6, autosomal dominant, allelic with Van der Woude).
Correcting the Knee When the Nerve Is the Limit
Start by saying there is no guideline. The entire world literature on correcting a popliteal pterygium amounts to roughly 58 patients (87 limbs) pooled from 32 mostly single-case publications. Both the 2024 meta-analysis and the largest case reports state explicitly that no treatment guideline or classification exists. Any confident algorithm offered in a viva should be framed as reasoning from principles, not as established practice.
- Gradual correction with an external fixator (Ilizarov). Because the sciatic nerve cannot be acutely stretched, a circular fixator gradually distracts the knee straight over weeks. It works: in the largest PPS-specific series (8 children, 11 knees, treated 1986-2007, follow-up 1-21 years) complete extension was achieved in every knee. But quote the price in the same breath - 6 of those 8 children needed the whole correction repeated, at a mean interval of 3-4 years, and five developed posterior tibial subluxation or frank dislocation (four partial, one complete), every one of them associated with recurrence. The pooled meta-analysis likewise found the fixator gave the best knee and ankle mobility but carried the highest number of surgical sessions and the highest complication rate of any modality.
- Femoral shortening (extension) osteotomy. Shortening the femur lets the knee extend without stretching the fixed-length neurovascular bundle - trading limb length for extension and nerve safety. In the pooled comparison it achieved correction with the fewest sessions and no reported complications, which is the single most favourable signal in the dataset; the caveat is that the numbers behind it are small and uncontrolled, so this is a promising comparison, not a proven superiority.
- Isolated skin/soft-tissue procedures and hamstring release. Both improved the flexion contracture and mobility in the pooled data, and both required several procedures to do so. Posterior release with multiple Z-plasty or local flaps and excision of the fibrotic cord remains the foundation of most reconstructions.
- Microsurgical nerve and vessel lengthening. Interposition grafting - vein graft to the popliteal artery, autograft and allograft to the tibial and peroneal nerves - has been reported to allow correction of an 80-degree contracture in a one-year-old with free walking and restored touch sensibility at three years, though a foot orthosis was still needed for the resulting leg-length difference. An intraneural fascicular-shifting lengthening technique has also been described. Both rest on single cases; the meta-analysis classed nerve surgery as having too little data to compare.
- The realistic goal (and salvage). Accept a degree of residual flexion to preserve nerve function. For a severe unreconstructable or failed knee, arthrodesis or, rarely, amputation/knee disarticulation may be needed for bracing or prosthetic fitting - again with too few reported cases to quantify.
Complete extension is achievable in essentially every popliteal pterygium knee with gradual distraction - and that figure alone is misleading. In the largest PPS series, six of eight children required the entire correction to be repeated within three to four years, and five sustained posterior tibial subluxation or dislocation, always in company with recurrence. A separate Ilizarov series of severe congenital knee flexion reported that every single patient developed pin-track and skin complications and concluded that minor recurrence must be expected in all cases - though note only 2 of its 8 patients had PPS, the rest having arthrogryposis or tibial hemimelia, so that series cannot be quoted as PPS-specific. The honest counselling position is that correction is reliably obtainable but not reliably durable, and the family should be prepared for repeat surgery and for the knee to be watched for posterior subluxation.
Q: What are the correction techniques for the fixed knee flexion when the shortened nerve is the limiting factor, and how well do they work?
A: There is no established guideline - the pooled literature is about 58 patients and 87 limbs from 32 mostly single-case reports. (1) Ilizarov gradual correction achieves complete extension and the best knee/ankle mobility, but has the most surgical sessions and highest complication rate, and in the largest PPS series 6 of 8 children needed re-correction at 3-4 years with 5 posterior tibial subluxations/dislocations. (2) Femoral shortening osteotomy achieved correction with the fewest sessions and no reported complications in that pooled comparison - the most favourable signal, though uncontrolled. (3) Skin/soft-tissue procedures and hamstring release work but need several procedures. (4) Microsurgical nerve/vessel grafting has produced free walking with preserved sensibility at 3 years in a single case. (5) Accept residual flexion; salvage with arthrodesis or amputation.
Mnemonics & Memory Aids
PTERYGIUM
Hook:PTERYGIUM: Popliteal web, Tethered flexor surface, Escobar (multiple), Reconstruct in stages, don't Yank (nerve in web), Genetics IRF6, Investigate associations.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A child has a web across the back of the knee holding it flexed, with a cleft lip. What is the diagnosis and what is the key surgical consideration?”
What they are
- Pterygium = congenital flexor-surface web -> fixed flexion deformity
- Web contains shortened skin, fascia AND neurovascular structures
- Group of congenital-contracture syndromes
Popliteal pterygium syndrome
- Autosomal dominant (IRF6; allelic with Van der Woude)
- Popliteal web + fixed knee flexion
- Orofacial clefting/lip pits, genital anomalies, syndactyly, foot deformity
The surgical key
- Sciatic nerve/neurovascular bundle shortened + abnormally superficial within the web
- The shortened nerve (not skin) usually limits correction and is at risk
- Plan staged/gradual correction; don't force one-stage extension
Management
- Staged release: multiple Z-plasty/flaps, fibrotic-band excision, graded contracture release
- Correct associated foot deformity; protect (and lengthen) the nerve as needed
- Multidisciplinary (plastics/orthopaedics/genetics); Escobar = autosomal recessive CHRNG, multi-joint webs + scoliosis
Outcomes - know these numbers
- No guideline or classification exists; pooled literature ~58 patients / 87 limbs from 32 mostly single-case reports
- Ilizarov: complete extension in all 11 knees of the largest series, BUT 6 of 8 children needed re-correction at mean 3-4 years
- 5 posterior tibial subluxations/dislocations, every one associated with recurrence - the warning sign
- Pooled: fixator = best mobility, most sessions, highest complications; femoral osteotomy = fewest sessions, no reported complications (uncontrolled)
- Microsurgical nerve/vessel grafting: free walking + restored touch sensibility at 3 years in a single case
Evidence & Key Studies
Comparative analysis of surgical treatment modalities for a popliteal pterygium: a meta-analysis
- PRISMA meta-analysis of the entire field: 183 papers screened, data extracted from 32 articles, yielding just 58 patients and 87 limbs - the whole reported world experience of treating a popliteal pterygium.
- Ilizarov fixator gave improved knee and ankle mobility postoperatively but had a relatively high number of surgical sessions and high complication rates. Femoral osteotomy achieved successful correction of knee posture with fewer sessions and no reported complications.
- Isolated skin/soft-tissue procedures and hamstring release both improved contracture and mobility but required several procedures each. Nerve surgery and amputation had too little data to compare.
- The authors conclude that no classification or guideline for treating this deformity exists and that further research is needed - so no modality can be presented as standard of care. Limitations: the pooled units are overwhelmingly single cases, published across four decades with no common outcome measure, no control arm and inevitable publication bias toward success.
Popliteal pterygium knee contracture: treatment with the Ilizarov technique
- Consecutive series of 8 children (11 knees) with popliteal pterygium syndrome treated at a single Paris centre between 1986 and 2007; preoperative knee flexion 40-120 degrees, with contracture over 90 degrees in 10 of the 11 knees. Follow-up 1-21 years.
- Complete extension was obtained in ALL cases by gradual Ilizarov correction - the popliteal cutaneous band and the shortened sciatic nerve were confirmed as what made realignment complex.
- RECURRENCE WAS THE RULE, NOT THE EXCEPTION: 6 of the 8 children required the correction to be repeated by the same technique, at a mean interval of 3-4 years.
- Four progressive partial posterior tibial dislocations and one complete dislocation occurred during follow-up - every one of them associated with recurrence of the flexion contracture, so the subluxing knee is the warning sign that the deformity is coming back.
- Limitations: retrospective, single centre, 8 patients across a 21-year era spanning changes in technique, no comparison group and a follow-up range (1-21 years) so wide that the recurrence rate is almost certainly an underestimate for the shortest-followed children.
Orthopaedic surgical management of complicated congenital popliteal pterygium syndrome
- A SINGLE CASE REPORT (level V), not a series - it demonstrates that the described approach is possible, and can say nothing about how often it succeeds.
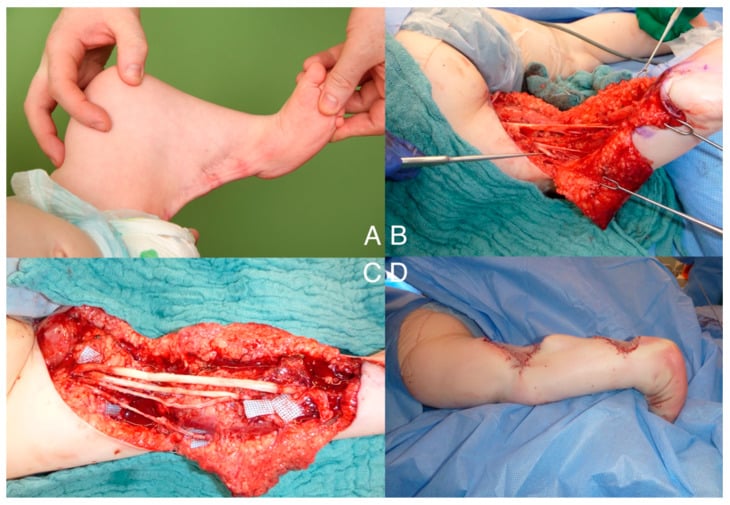
- In that patient the sciatic nerve was shortened within the web and required a fascicular-shifting lengthening technique; correction used staged multiple Z-plasty and fibrotic-band excision with meticulous protection of the neurovascular bundle.
- Associated anomalies (undescended testes, syndactyly, foot deformity) required additional staged soft-tissue reconstruction - underscoring the multisystem, staged nature of management.
Walking ability after microsurgical reconstruction of paediatric popliteal pterygium syndrome
- Single case report: a one-year-old with a unilateral 80-degree knee flexion contracture, treated by large Z-plasty, vein grafting to lengthen the popliteal vessels, autograft and allograft lengthening of the tibial and peroneal nerves, and capsular and tendon releases.
- At three years the child walked freely, touch sensibility of the foot was restored and perfusion remained stable through growth; a foot orthosis was still required to balance the leg-length difference and support the midfoot deformity.
- The authors state plainly that no established treatment guidelines exist for PPS and that care must be individualised - one case cannot establish that microsurgical lengthening is preferable to gradual correction or femoral shortening.
The pooled modality comparison, the total of 58 patients and 87 limbs, and the statement that no classification or guideline exists come from the Aman meta-analysis (DOI). The recurrence in 6 of 8 children at a mean 3-4 years and the five posterior tibial subluxations/dislocations come from Solignac (DOI). The microsurgical nerve and vessel grafting outcome at three years comes from Aman's case report (DOI), and the fascicular-shifting technique from Hasan (DOI) - both single cases. The observation that every patient developed pin-track and skin complications, and that minor recurrence should be expected in all, comes from Leonchuk's Ilizarov series of severe congenital knee flexion (DOI), in which only 2 of 8 patients had PPS - it is quoted here as related evidence, not as PPS-specific data. The IRF6 genetics (allelic with Van der Woude), the orofacial-clefting and genital associations, the CHRNG basis of Escobar syndrome, and the anatomy of the shortened, superficially placed neurovascular bundle are standard, well-established teaching.
Be clear about what does not exist. There is no randomised or even prospectively controlled trial in this condition, no validated classification of pterygium severity, no agreed threshold of residual flexion that constitutes success, and no published surveillance interval for recurrence or posterior tibial subluxation. Every comparison above is between small uncontrolled case collections published across four decades.