ARISCAT Score | OSA Management | COPD Optimization | Postoperative Pulmonary Complications
ARISCAT RISK STRATIFICATION
Critical Must-Knows
- ARISCAT score predicts postoperative pulmonary complications - seven risk factors including age, SpO2, respiratory infection
- OSA affects 24% of surgical patients - STOP-BANG greater than 5 requires CPAP continuation perioperatively
- Smoking cessation under 4 weeks may worsen outcomes - minimum 4 weeks required for pulmonary benefit
- PFTs rarely change management in asymptomatic patients - reserve for moderate-severe COPD or unexplained dyspnea
- Neuraxial anesthesia reduces pulmonary complications by 30% compared to general anesthesia in lower limb surgery
Clinical Pearls
- "ARISCAT includes: age, SpO2 under 96%, respiratory infection in last month, preop anemia, upper abdominal/thoracic surgery, duration over 2 hours, emergency procedure
- "STOP-BANG: Snoring, Tired, Observed apnea, Pressure (BP), BMI over 35, Age over 50, Neck over 40cm, Gender male - score 5-8 = high OSA risk
- "FEV1 under 50% predicted or FEV1/FVC under 0.7 indicates moderate-severe COPD needing optimization
- "Continue CPAP perioperatively for known OSA - reduces atelectasis and hypoxemia
Critical Pulmonary Risk Assessment Exam Points
ARISCAT Score
Gold standard for pulmonary risk prediction. Seven factors: age over 50 (3-16 points), SpO2 under 96% (8 points), respiratory infection in last month (17 points), preop anemia Hb under 100 (11 points), upper abdominal/thoracic surgery (15 points), duration over 2h (16 points), emergency (8 points). Score over 44 = high risk (42% complication rate).
OSA Screening and Management
STOP-BANG over 5 = high OSA risk. Continue CPAP/BiPAP perioperatively. Avoid opioids in PACU. Neuraxial preferred over general anesthesia. Semiupright positioning. Extended monitoring 24-48h. Undiagnosed OSA major cause of postop respiratory failure.
COPD Optimization
Optimize 4-6 weeks before surgery. Bronchodilators, inhaled corticosteroids if FEV1 under 60%. Smoking cessation minimum 4 weeks. Antibiotics if acute exacerbation. Physiotherapy and incentive spirometry. Delay surgery if active infection or poorly controlled.
PFT Indications
PFTs rarely change management unless moderate-severe COPD (FEV1 under 60%), unexplained dyspnea, or lung resection planned. Do NOT order routinely. Clinical assessment (exercise tolerance, symptoms) more predictive than spirometry for elective orthopaedics.
At a Glance
The ARISCAT score is the gold standard for predicting postoperative pulmonary complications, incorporating seven factors: age, SpO₂ less than 96%, respiratory infection in last month, preoperative anemia, upper abdominal/thoracic surgery, duration greater than 2 hours, and emergency procedure. Scores greater than 44 indicate high risk (42% complication rate). OSA affects 24% of surgical patients; STOP-BANG greater than 5 indicates high risk requiring perioperative CPAP continuation. Smoking cessation requires minimum 4 weeks for pulmonary benefit—cessation less than 4 weeks may paradoxically worsen outcomes due to increased secretions. PFTs rarely change management in asymptomatic patients—reserve for moderate-severe COPD (FEV1 less than 60%) or unexplained dyspnea. Neuraxial anesthesia reduces pulmonary complications by 30% compared to general anesthesia in lower limb surgery.
ASTHMA RARISCAT Risk Score - 7 Predictors
| A | Age 50-80 years = 3 points, over 80 years = 16 points |
| S | SpO2 saturation 91-95% = 8 points, under 90% = 24 points (room air) |
| T | Thoracic/upper abdominal surgery 15 points - proximity to diaphragm impairs ventilation |
| H | Hemoglobin low Anemia Hb under 100 g/L = 11 points (impaired oxygen delivery) |
| M | Month - respiratory infection Within last month = 17 points (residual inflammation) |
| A | Acute/Emergency procedure 8 points - no time for optimization |
| R | Run time over 2 hours 2-3 hours = 16 points (prolonged anesthesia and atelectasis) |
| A | Age 50-80 years = 3 points, over 80 years = 16 points | H | Hemoglobin low Anemia Hb under 100 g/L = 11 points (impaired oxygen delivery) | R | Run time over 2 hours 2-3 hours = 16 points (prolonged anesthesia and atelectasis) |
| S | SpO2 saturation 91-95% = 8 points, under 90% = 24 points (room air) | M | Month - respiratory infection Within last month = 17 points (residual inflammation) | ||
| T | Thoracic/upper abdominal surgery 15 points - proximity to diaphragm impairs ventilation | A | Acute/Emergency procedure 8 points - no time for optimization |
Hook:Patients with ASTHMA R factors need enhanced pulmonary care! Score under 26 = low risk, 26-44 = intermediate, over 44 = high risk.
STOP-BANGSTOP-BANG Score for OSA Screening
| S | Snoring Loud snoring (louder than talking or heard through closed door) |
| T | Tired Tired, fatigued, or sleepy during daytime |
| O | Observed apnea Witnessed breathing stopped during sleep |
| P | Pressure - hypertension High blood pressure or on treatment for hypertension |
| B | BMI over 35 Body mass index greater than 35 kg/m� |
| A | Age over 50 Age greater than 50 years |
| N | Neck over 40cm Neck circumference greater than 40 cm (measure at cricothyroid membrane) |
| G | Gender male Male gender (2x risk of OSA vs females) |
| S | Snoring Loud snoring (louder than talking or heard through closed door) | P | Pressure - hypertension High blood pressure or on treatment for hypertension | N | Neck over 40cm Neck circumference greater than 40 cm (measure at cricothyroid membrane) |
| T | Tired Tired, fatigued, or sleepy during daytime | B | BMI over 35 Body mass index greater than 35 kg/m� | G | Gender male Male gender (2x risk of OSA vs females) |
| O | Observed apnea Witnessed breathing stopped during sleep | A | Age over 50 Age greater than 50 years |
Hook:Use STOP-BANG to catch OSA before they crash! Score 0-2 = low risk, 3-4 = intermediate, 5-8 = high risk. High risk needs CPAP perioperatively.
PRAPSPostoperative Pulmonary Complications
| P | Pneumonia Most serious PPC - 2-5% in orthopaedics, 30-day mortality 20% |
| R | Respiratory failure Hypoxemia requiring reintubation or NIV - associated with OSA |
| A | Atelectasis Most common PPC - alveolar collapse from hypoventilation and secretions |
| P | Pleural effusion Fluid accumulation - common after upper abdominal/thoracic surgery |
| S | Severe bronchospasm Exacerbation of reactive airway disease - COPD/asthma |
| P | Pneumonia Most serious PPC - 2-5% in orthopaedics, 30-day mortality 20% | P | Pleural effusion Fluid accumulation - common after upper abdominal/thoracic surgery |
| R | Respiratory failure Hypoxemia requiring reintubation or NIV - associated with OSA | S | Severe bronchospasm Exacerbation of reactive airway disease - COPD/asthma |
| A | Atelectasis Most common PPC - alveolar collapse from hypoventilation and secretions |
Hook:Watch for PRAPS after surgery - these pulmonary complications kill! Early mobilization and physiotherapy prevent most.
Overview and Core Principles
Why Pulmonary Risk Assessment Matters
Postoperative pulmonary complications (PPCs) are a leading cause of perioperative morbidity and mortality, particularly in orthopaedic surgery where patients are often elderly with multiple comorbidities. PPCs include pneumonia, respiratory failure, atelectasis, bronchospasm, and pleural effusion. These complications:
- Occur in 2-5% of elective orthopaedic procedures, 10-40% in high-risk patients
- Increase 30-day mortality by 2-20 fold depending on severity
- Prolong hospital stay by 5-10 days on average
- Cost an additional $20,000-50,000 per episode
- Are largely preventable through systematic risk assessment and optimization
The goals of pulmonary risk assessment are to: (1) identify high-risk patients requiring enhanced monitoring and intervention, (2) optimize modifiable risk factors before surgery, (3) guide anesthetic technique selection (neuraxial vs general), and (4) inform postoperative care planning (ward vs HDU/ICU).
Risk Stratification Tools
- ARISCAT score: validated PPC prediction (most widely used)
- AROZULLAR score: respiratory failure prediction
- STOP-BANG: OSA screening (8-item questionnaire)
- Gupta MICA: myocardial infarction or cardiac arrest
- Clinical assessment: exercise tolerance most predictive
Modifiable Risk Factors
- Smoking cessation: minimum 4 weeks preoperatively
- COPD optimization: bronchodilators, steroids if FEV1 under 60%
- Weight loss: BMI reduction if over 40
- Respiratory infections: delay surgery 4-6 weeks after infection
- OSA management: CPAP continuation perioperatively
Physiology and Core Concepts
The Physiology Behind Postoperative Pulmonary Risk
Postoperative pulmonary complications arise from a predictable chain of physiological insults. Understanding these mechanisms explains why each risk factor and each preventive measure works.
Reduced Functional Residual Capacity
General anaesthesia, supine positioning, and abdominal/thoracic incisions reduce functional residual capacity by 15-20%, promoting alveolar collapse (atelectasis). Atelectatic lung is poorly ventilated but still perfused, creating shunt, hypoxaemia, and a nidus for infection.
Impaired Cough and Clearance
Pain-related splinting, opioids, and residual neuromuscular blockade impair deep breathing and cough. Retained secretions plus atelectasis progress to pneumonia, especially in smokers and COPD patients with baseline mucociliary dysfunction.
Ventilatory Depression
Opioids and sedatives blunt central respiratory drive, while OSA adds dynamic upper-airway obstruction. The combination produces hypoventilation, hypercapnia and obstructive hypoxaemia, peaking on postoperative nights 1-3 during REM rebound.
Fixed vs Modifiable Risk
Risk is the product of patient factors (age, COPD, OSA, anaemia, baseline SpO2), procedure factors (site, duration, urgency) and anaesthetic/care factors (technique, opioids, mobilisation). Only the modifiable elements can change the trajectory - hence the focus on optimisation.
Why Site of Surgery Dominates Risk
Proximity of the incision to the diaphragm is the single strongest procedural predictor. Upper abdominal and thoracic surgery impair diaphragmatic excursion and carry the highest PPC rates; peripheral limb surgery (most orthopaedics) is comparatively protected. This is why ARISCAT assigns 15 points to upper-abdominal/thoracic incisions and why neuraxial lower-limb surgery is so favourable.
Clinical Relevance
Why This Matters in Orthopaedic Practice
Orthopaedic populations are increasingly elderly, obese and comorbid - exactly the profile that drives pulmonary risk. The clinically useful message is that a structured, low-cost assessment changes management at several decision points:
- Triage of monitoring level: a high ARISCAT or high STOP-BANG score moves a patient from ward to HDU/continuous oximetry, where early respiratory deterioration is caught before arrest.
- Choice of anaesthetic: lower-limb arthroplasty and hip-fracture surgery are amenable to neuraxial anaesthesia, which reduces pneumonia and 30-day mortality and is especially valuable in COPD/OSA.
- Timing of elective surgery: an active respiratory infection or COPD exacerbation is a reason to defer, not proceed - one of the highest-yield interventions available.
- Analgesic strategy: identifying OSA mandates an opioid-sparing, multimodal and regional plan, directly reducing the most lethal complication (respiratory depression).
The Hip Fracture Paradox
Hip-fracture patients combine the worst of both worlds - high baseline pulmonary risk and an emergency procedure that cannot be deferred for prolonged optimisation. The answer is not delay but rapid, parallel optimisation within 24-48 hours (correct anaemia, optimise bronchodilators, plan neuraxial anaesthesia and HDU monitoring) so that surgery proceeds promptly while pulmonary risk is actively mitigated.
ARISCAT Risk Score
ARISCAT Components and Calculation
The Assess Respiratory Risk in Surgical Patients in Catalonia (ARISCAT) score is the most validated tool for predicting postoperative pulmonary complications. Developed from a multicenter cohort of 2,464 patients undergoing noncardiac surgery, it identifies seven independent risk factors.
ARISCAT Score Components and Point Values
| Risk Factor | Category | Points | Rationale |
|---|---|---|---|
| Age | Under 50 / 50-80 / Over 80 | 0 / 3 / 16 | Decreased respiratory reserve, comorbidities |
| Preoperative SpO2 | Over 96% / 91-95% / Under 90% | 0 / 8 / 24 | Baseline hypoxemia indicates lung disease |
| Respiratory infection in last month | No / Yes | 0 / 17 | Residual inflammation and secretions |
| Preoperative anemia | Hb over 100 / Hb under 100 g/L | 0 / 11 | Impaired oxygen delivery to tissues |
| Surgical incision | Peripheral / Upper abdominal or thoracic | 0 / 15 | Proximity to diaphragm impairs ventilation |
| Duration of surgery | Under 2h / 2-3h / Over 3h | 0 / 16 / 23 | Prolonged anesthesia and atelectasis |
| Emergency procedure | No / Yes | 0 / 8 | No time for optimization |
ARISCAT Risk Stratification
Management: Standard perioperative care. Early mobilization. Incentive spirometry encouraged but not mandatory. Ward-level monitoring sufficient. Routine physiotherapy.
Management: Enhanced respiratory care bundle. Mandatory incentive spirometry Q2H while awake. Chest physiotherapy twice daily. Consider neuraxial anesthesia if appropriate. Aggressive early mobilization. Extended monitoring (telemetry). Avoid excessive opioids.
Management: Plan HDU or ICU bed. Respiratory therapist involvement. Consider neuraxial vs general anesthesia (neuraxial reduces PPC 30%). CPAP/BiPAP if OSA or respiratory failure risk. Minimize opioids - multimodal analgesia. Daily CXR if deteriorating. Low threshold for respiratory support.
ARISCAT Validation and Limitations
Validation: ARISCAT was derived and validated within a 2,464-patient cohort (split into development and validation subsamples) with excellent discrimination - area under the ROC curve 90% in development and 88% in validation. It predicts respiratory infection, respiratory failure, bronchospasm, atelectasis, pleural effusion, pneumothorax and aspiration pneumonitis. Limitations: Developed for a broad surgical population - may overestimate risk in peripheral orthopaedic procedures (TKA, THA). Does not include OSA or COPD severity. Clinical judgment remains essential - the score guides but does not replace assessment.
Obstructive Sleep Apnea Assessment
STOP-BANG Questionnaire
Obstructive sleep apnea (OSA) affects 24% of men and 9% of women in the surgical population, with 80-90% undiagnosed. Untreated OSA increases perioperative complications including respiratory failure (2-3x risk), cardiac events, and ICU admission. The STOP-BANG questionnaire is the validated screening tool.
STOP-BANG Interpretation
| Score | OSA Risk | Sensitivity | Perioperative Management |
|---|---|---|---|
| 0-2 | Low risk | 84% for moderate-severe OSA | Standard care, monitor O2 saturation 24h |
| 3-4 | Intermediate risk | 93% for moderate OSA | Extended monitoring, avoid opioids, semiupright positioning |
| 5-8 | High risk | 100% for severe OSA | Continue CPAP, consider autotitration, neuraxial preferred, HDU/ICU if general |
STOP-BANG Questionnaire Details
The 8 Questions (Yes = 1 point each):
- Snoring: Do you snore loudly (louder than talking or heard through closed door)?
- Tired: Do you often feel tired, fatigued, or sleepy during daytime?
- Observed apnea: Has anyone observed you stop breathing during sleep?
- Pressure: Do you have or are you being treated for high blood pressure?
- BMI: Is your BMI greater than 35 kg/m�?
- Age: Are you older than 50 years?
- Neck: Is your neck circumference greater than 40 cm (measure at cricothyroid level)?
- Gender: Are you male?
Scoring: Add 1 point for each "yes" answer. Total score 0-8.
When to Order Sleep Study
Do NOT delay elective surgery for sleep study if patient screens positive but no known OSA. Proceed with empiric CPAP/BiPAP in PACU and postop. Sleep study takes 4-12 weeks and rarely changes perioperative management. Exception: patients with severe cardiopulmonary disease where diagnosis changes surgical candidacy.
This approach ensures patient safety without unnecessary surgical delays.
COPD Optimization
Assessment and Severity Staging
Chronic obstructive pulmonary disease (COPD) affects 10-15% of patients over 65 undergoing orthopaedic surgery. COPD increases postoperative pulmonary complications 2-5 fold, particularly pneumonia and respiratory failure. Severity stratification guides optimization.
COPD Severity by Spirometry (GOLD Classification)
| GOLD Stage | FEV1 % Predicted | FEV1/FVC | Perioperative Implications |
|---|---|---|---|
| GOLD 1 - Mild | FEV1 over 80% | Under 0.70 | Low risk - standard care, smoking cessation |
| GOLD 2 - Moderate | FEV1 50-79% | Under 0.70 | Optimize bronchodilators, consider ICS, physiotherapy |
| GOLD 3 - Severe | FEV1 30-49% | Under 0.70 | High risk - pulmonology consult, aggressive optimization, HDU plan |
| GOLD 4 - Very Severe | FEV1 under 30% | Under 0.70 | Very high risk - consider candidacy, ICU plan, respiratory support |
4-6 Week COPD Optimization Protocol
Bronchodilator Therapy
Ensure adequate bronchodilation:
- Short-acting: Salbutamol PRN (rescue inhaler)
- Long-acting: Tiotropium (LAMA) daily if FEV1 under 60%
- Combination: LABA/LAMA if symptomatic despite single agent
- Inhaler technique: Verify correct use (common error)
- Start 4-6 weeks pre-op for maximal benefit
Inhaled Corticosteroids
Add ICS if frequent exacerbations:
- Indicated if FEV1 under 60% AND 2+ exacerbations/year
- Reduces inflammation and exacerbation frequency
- Combination LABA/ICS (e.g., fluticasone/salmeterol)
- NOT indicated for stable COPD without exacerbations
- Continue through perioperative period
Smoking Cessation
Minimum 4 weeks essential:
- Under 4 weeks may worsen sputum production
- 4 weeks: improved mucociliary clearance
- 8 weeks: maximal pulmonary benefit
- Offer nicotine replacement or varenicline plus structured counselling
- Document pack-year history
Pulmonary Rehabilitation
Physiotherapy and exercise:
- Incentive spirometry training (start pre-op)
- Breathing exercises and pursed-lip breathing
- Ambulation and exercise tolerance building
- Secretion clearance techniques
- Continue daily postoperatively
Acute Exacerbation Management
Delay elective surgery 4-6 weeks after COPD exacerbation. Active exacerbation dramatically increases PPC risk (pneumonia 10-20%, respiratory failure 5-10%). Optimize with antibiotics if purulent sputum, oral prednisolone 30-40mg daily for 5-7 days, increased bronchodilators. Confirm return to baseline symptoms and spirometry before proceeding.
This optimization protocol reduces postoperative pulmonary complications in COPD patients by 40-50%.
Postoperative Pulmonary Complications
Types and Prevention Strategies
Postoperative Pulmonary Complications
| Complication | Incidence | Risk Factors | Prevention Strategy |
|---|---|---|---|
| Atelectasis | 10-40% (most common) | Prolonged supine, opioids, obesity, upper abdominal surgery | Early mobilization, incentive spirometry, minimize opioids |
| Pneumonia | 2-5% elective, 10-20% emergency | Age over 70, COPD, aspiration risk, prolonged intubation | Smoking cessation 4 weeks, head-up positioning, oral hygiene |
| Respiratory Failure | 1-3% (requires reintubation or NIV) | OSA, obesity, COPD, excessive opioids, prolonged surgery | CPAP for OSA, neuraxial anesthesia, multimodal analgesia |
| Bronchospasm | 2-10% in COPD/asthma | Active asthma, COPD exacerbation, aspiration | Optimize bronchodilators pre-op, avoid triggers (cold air, aspiration) |
| Pleural Effusion | 5-15% (small effusions common) | Heart failure, hypoalbuminemia, fluid overload | Judicious fluid management, diuresis if CHF, correct albumin |
Prevention Bundle Timeline
Optimization: Smoking cessation minimum 4 weeks. COPD bronchodilator optimization. OSA CPAP compliance. Weight loss if BMI over 40. Treat respiratory infections (delay 4-6 weeks if acute). Incentive spirometry training.
Lung-protective strategies: Tidal volume 6-8 mL/kg ideal body weight. PEEP 5-8 cmH2O. Recruitment maneuvers if atelectasis. FiO2 titrate to SpO2 92-96% (avoid hyperoxia). Minimize airway pressures. Extubate fully awake.
Immediate recovery: Semiupright positioning (30-45 degrees). Supplemental O2 to SpO2 over 92%. CPAP if OSA or respiratory depression. Early incentive spirometry. Multimodal analgesia to minimize opioids. Monitor respiratory rate and effort.
Enhanced recovery: Incentive spirometry 10 breaths Q2H while awake. Early mobilization (out of bed within 24h). Physiotherapy twice daily. Minimize opioids - regional blocks preferred. Continuous pulse oximetry if high risk. CXR only if symptomatic.
Pneumonia Prevention
Postoperative pneumonia has 20-30% mortality in elderly orthopaedic patients. Prevention is critical: (1) Smoking cessation 4+ weeks pre-op reduces pneumonia 50%, (2) Head-up positioning 30 degrees reduces aspiration, (3) Early mobilization (out of bed within 24h) improves secretion clearance, (4) Incentive spirometry 10 breaths every 2 hours prevents atelectasis, (5) Oral hygiene (chlorhexidine mouthwash) reduces bacterial load. If pneumonia develops: prompt empirical antibiotics per local antimicrobial guidelines, respiratory physiotherapy, and consider bronchoscopy if lobar collapse.
Anesthetic Technique Considerations
Neuraxial vs General Anesthesia
Anesthetic Technique and Pulmonary Outcomes
| Technique | PPC Risk | Advantages | Disadvantages |
|---|---|---|---|
| Neuraxial (spinal/epidural) | Baseline (reference) | 30% PPC reduction, preserved airway reflexes, early mobilization, less opioids | Sympathetic block (hypotension), limited to lower limb/hip, anticoagulation concerns |
| General anesthesia | 1.3x higher PPC | Suitable for any surgery, airway control, no anticoagulation issues | Atelectasis, ventilator dependence, opioids, delayed mobilization |
| Combined (GA + regional block) | Similar to neuraxial | Optimal surgical conditions, reduced GA depth, multimodal analgesia | Complexity, time, requires both skill sets |
When to Prefer Neuraxial
- High pulmonary risk (ARISCAT over 44)
- Severe OSA (STOP-BANG 7-8)
- Moderate-severe COPD (FEV1 under 50%)
- Lower limb surgery (TKA, THA, femur fracture)
- Obesity (BMI over 40)
- Patient preference for awake surgery
When General Anesthesia Needed
- Upper limb or spine surgery (not amenable to neuraxial)
- Patient refusal of neuraxial
- Anticoagulation preventing neuraxial (recent DOAC/LMWH)
- Hemodynamic instability (severe AS, dehydration)
- Infection at injection site
- Coagulopathy or platelets under 70
Neuraxial PPC Reduction Mechanism
Why does neuraxial reduce pulmonary complications? Four mechanisms: (1) Preserved airway reflexes and spontaneous ventilation (no intubation trauma, no positive-pressure atelectasis), (2) Superior analgesia reduces splinting and allows deep breathing and cough, (3) Reduced opioid requirements minimize respiratory depression, (4) Earlier mobilization improves secretion clearance. The Cochrane overview by Guay et al. (2014) found neuraxial blockade reduced pneumonia (RR 0.45) and 0-30 day mortality (RR 0.71) compared with general anaesthesia.
Differential Diagnosis of Postoperative Hypoxaemia
The patient who desaturates or becomes breathless after orthopaedic surgery is a classic viva and ward scenario. Pulmonary complications must be distinguished from cardiac, embolic and mechanical causes - the management of each differs sharply.
Causes of Early Postoperative Hypoxaemia / Dyspnoea
| Diagnosis | Typical Timing & Clues | Key Discriminator | Initial Action |
|---|---|---|---|
| Atelectasis | First 24-48h, low-grade desaturation, basal crackles | Improves with deep breathing, recruitment and mobilisation | Incentive spirometry, physiotherapy, sit up, oxygen |
| Pneumonia | Day 2 onwards, fever, purulent sputum, focal signs | New infiltrate on CXR plus systemic sepsis | Cultures, empirical antibiotics, physiotherapy |
| Pulmonary embolism | Any time, sudden dyspnoea, tachycardia, pleuritic pain | Hypoxaemia with clear CXR; raised D-dimer, CTPA positive | Oxygen, anticoagulation, urgent CTPA |
| Fat embolism syndrome | 24-72h after long-bone/pelvic fracture or nailing | Triad of hypoxaemia, petechiae and confusion | Supportive oxygen/ventilation; largely a clinical diagnosis |
| Opioid / OSA hypoventilation | Postoperative nights, somnolent, low respiratory rate | Hypercapnia with obstruction; responds to stimulation/CPAP | Reduce opioids, naloxone if severe, CPAP, monitoring |
| Pulmonary oedema / fluid overload | Often day 1-2, orthopnoea, raised JVP, bilateral crackles | Cardiomegaly/upper-lobe diversion on CXR; responds to diuresis | Sit up, oxygen, diuretics, fluid balance review |
Do Not Anchor on Atelectasis
A common trap is to attribute every postoperative desaturation to atelectasis. In an orthopaedic patient, pulmonary embolism and fat embolism are time-critical alternatives - sudden dyspnoea with a clear chest film should prompt urgent evaluation for PE rather than reassurance.
Controversies & Areas of Uncertainty
Exact Smoking-cessation Window
The classic concern that cessation under 4 weeks transiently increases secretions is based largely on older observational data; several subsequent analyses have not confirmed early harm. The pragmatic consensus is that any cessation is beneficial and should always be encouraged, with the largest complication benefit from cessation 4 or more weeks before surgery.
Mandatory Sleep Studies
Whether a positive STOP-BANG screen should trigger formal polysomnography before elective surgery remains debated. Most perioperative guidance favours proceeding with an empirical OSA-precautions pathway rather than delaying surgery, reserving sleep studies for selected high-risk or symptomatic patients.
Strength of the Neuraxial Benefit
The pulmonary advantage of neuraxial over general anaesthesia is consistent for pneumonia, but the magnitude varies between meta-analyses and many constituent trials predate modern enhanced-recovery and lung-protective ventilation. The benefit is clearest in high-risk, lower-limb surgery.
Value of Routine Spirometry
Preoperative spirometry rarely reclassifies risk in patients with good exercise tolerance and is not recommended as a routine screen. Functional capacity and clinical assessment remain better predictors than absolute FEV1 for most orthopaedic surgery.
Evidence Base and Key Trials
ARISCAT Score Derivation and Validation (Canet)
- Prospective multicentre cohort of 2,464 patients in 59 hospitals, randomly split into development and validation subsamples
- A postoperative pulmonary complication occurred in 123 patients (5%); 30-day mortality was 19.5% with a PPC versus 0.5% without
- Seven independent predictors: low SpO2, recent respiratory infection, age, anaemia, upper abdominal/thoracic incision, surgery 2 hours or more, and emergency surgery
- Excellent discrimination - area under the ROC curve 90% (development) and 88% (validation)
STOP / STOP-BANG Derivation for OSA Screening (Chung)
- Developed and validated in 2,467 preoperative surgical patients without previously diagnosed OSA; 211 underwent polysomnography
- The 4-item STOP questionnaire alone had sensitivities of 66% / 74% / 80% for AHI over 5, over 15, and over 30
- Adding BMI, age, neck circumference and gender (STOP-BANG) raised sensitivity to 84% / 93% / 100% for the same AHI thresholds
- High sensitivity for moderate-to-severe OSA makes it an effective preoperative screen with a low false-negative rate
STOP-BANG Meta-analysis Across Populations (Nagappa)
- Systematic review and meta-analysis of 17 studies including 9,206 patients across sleep-clinic, surgical and general populations
- In the surgical population the probability of severe OSA rose stepwise with score: 15% at 3, 25% at 4, 35% at 5, 45% at 6 and 65% at 7-8
- In sleep-clinic patients sensitivity was 90% / 94% / 96% for any / moderate-to-severe / severe OSA
- Higher STOP-BANG score reliably increases the probability of moderate-to-severe OSA, supporting graded risk stratification
High-risk OSA and Postoperative Complications (Nagappa)
- Bayesian meta-analysis of 10 cohort studies including 23,609 surgical patients screened with STOP-BANG
- High-risk OSA carried roughly four-fold higher perioperative complications (odds ratio 3.93, 95% credible interval 1.85-7.77)
- Postoperative complication rate 6.86% in high-risk versus 4.62% in low-risk OSA patients
- Length of stay was about 2 days longer in high-risk OSA patients
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: High ARISCAT Score Patient
"72-year-old male for urgent hip fracture fixation. COPD (FEV1 45%), SpO2 93% on room air, smoker 60 pack-years, Hb 95 g/L. Calculate ARISCAT score and discuss perioperative pulmonary management."
Scenario 2: Undiagnosed OSA Screening
"58-year-old obese male (BMI 42) for elective TKA. Wife reports loud snoring and witnessed apneas. STOP-BANG score 7. No sleep study. How do you proceed?"
Scenario 3: PFT Interpretation and COPD Optimization
"65-year-old female for elective THA. Known COPD, current smoker 40 pack-years. Recent PFTs: FEV1 48% predicted, FEV1/FVC 0.58. On salbutamol PRN only. Surgery in 6 weeks. Your optimization plan?"
MCQ Practice Points
ARISCAT High Risk Threshold
Q: What ARISCAT score indicates high risk for postoperative pulmonary complications? A: Score greater than 44 indicates high risk with 42% predicted complication rate. Requires enhanced respiratory care including HDU monitoring, physiotherapy, incentive spirometry, and consideration of neuraxial vs general anesthesia.
STOP-BANG OSA Screening
Q: A patient scores 6 on STOP-BANG questionnaire. What is the appropriate management? A: High OSA risk (score 5-8) requires empiric perioperative CPAP, continuous pulse oximetry 24-48 hours, avoid opioids, neuraxial anesthesia preferred. Do NOT delay surgery for sleep study in most cases.
Smoking Cessation Timing
Q: What is the minimum smoking cessation duration to reduce postoperative pulmonary complications? A: 4 weeks minimum. Cessation under 4 weeks may paradoxically increase complications due to increased sputum production. Optimal benefit at 8 weeks (50-60% reduction).
PFT Indications
Q: When are PFTs indicated before elective orthopaedic surgery? A: Moderate-severe COPD without recent spirometry, unexplained dyspnea, or smoking over 40 pack-years with symptoms. NOT indicated routinely - exercise tolerance is more predictive than spirometry.
Guidelines, Registries & Global Practice
Global Epidemiology
Postoperative pulmonary complications are among the most common serious perioperative events worldwide, affecting roughly 2-5% of unselected surgical patients and a higher proportion of elderly and high-risk patients. OSA is estimated to affect up to a quarter of men and around 10% of women in the surgical population, the large majority undiagnosed at the time of surgery. COPD prevalence rises sharply with age and smoking exposure and is a leading global cause of morbidity, with substantial regional variation driven by tobacco use, biomass-fuel exposure and air quality.
Side-by-side Society Guidance
Major Society Recommendations on Perioperative Pulmonary Risk
| Body / Region | OSA Screening | Smoking Cessation | Key Position |
|---|---|---|---|
| SASM / ASA (US) | Screen all patients (e.g. STOP-BANG); proceed without mandatory polysomnography if a perioperative plan is in place | Advise cessation; offer pharmacotherapy and counselling | Emphasise opioid-sparing analgesia and postoperative monitoring for suspected OSA |
| NICE / GOLD (UK / global) | Identify and optimise OSA; GOLD guides COPD severity and inhaled therapy | Very brief advice plus pharmacotherapy at every contact (NICE) | Optimise inhaled therapy and treat exacerbations before elective surgery |
| ESAIC / ESA (Europe) | Use validated tools (ARISCAT) for PPC risk; targeted OSA screening | Recommend cessation 4 or more weeks preoperatively | Lung-protective ventilation and risk-adapted postoperative care |
| WHO / WFSA (limited-resource) | Clinical screening where polysomnography unavailable | Brief cessation advice; nicotine replacement where accessible | Prioritise pulse oximetry, early mobilisation and physiotherapy as low-cost measures |
Registry and Surveillance Signals
- Large national surgical-quality registries (e.g. ACS NSQIP in the US and equivalent audit programmes in Europe) consistently identify pneumonia and unplanned reintubation as high-impact, partly preventable pulmonary complications, and are used to benchmark institutional performance.
- Surgical-quality collaboratives have shown that untreated OSA, rather than OSA per se, drives excess cardiopulmonary events - supporting screening that leads to actual CPAP treatment.
High- vs Limited-resource Practice Variation
- High-resource settings: routine STOP-BANG screening, ready access to CPAP/BiPAP, HDU/ICU step-up beds, formal smoking-cessation services and inhaled COPD therapy, continuous postoperative pulse oximetry.
- Limited-resource settings: emphasis on low-cost, high-yield interventions - clinical risk screening, smoking-cessation advice, incentive spirometry, chest physiotherapy, early mobilisation, head-up positioning, and pulse oximetry (a WHO-prioritised safety standard). Neuraxial anaesthesia is often preferred for lower-limb surgery where it both reduces pulmonary risk and conserves scarce ventilatory and critical-care resources.
Documentation Principles (Global)
- Record the pulmonary risk assessment (ARISCAT, STOP-BANG, COPD severity) in the preoperative note.
- Ensure informed consent reflects patient-specific pulmonary complication risk.
- Document any patient declining optimisation (smoking cessation, CPAP) and the risks discussed - unrecognised OSA and failure to optimise COPD are recurrent themes in adverse-event reviews internationally.
Management Algorithm
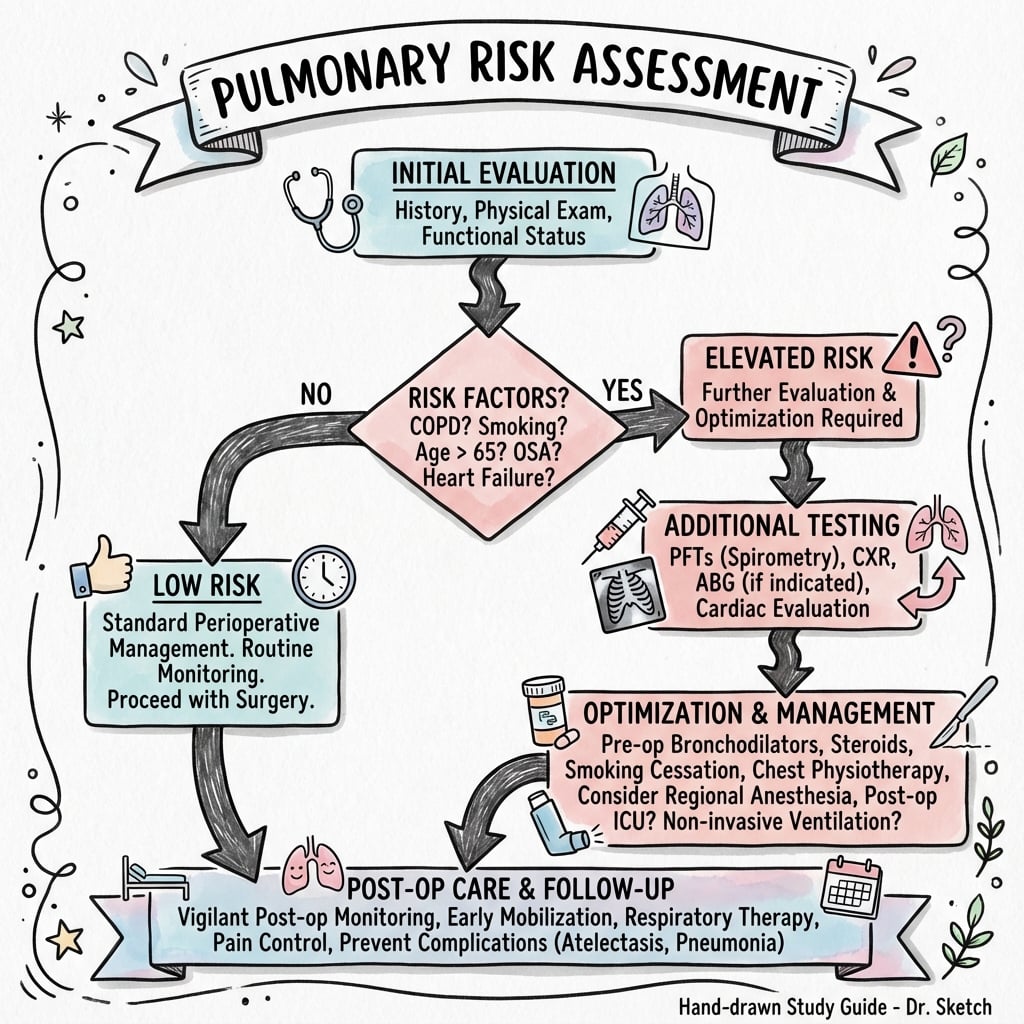
PULMONARY RISK ASSESSMENT
Clinical summary
ARISCAT Score (7 Predictors)
- •Age: under 50 (0), 50-80 (3), over 80 (16 points)
- •SpO2: over 96% (0), 91-95% (8), under 90% (24 points)
- •Respiratory infection last month (17 points)
- •Anemia Hb under 100 g/L (11 points)
- •Upper abdominal/thoracic surgery (15 points)
- •Duration 2-3h (16), over 3h (23 points)
- •Emergency procedure (8 points)
- •Score: under 26 low (1.6%), 26-44 intermediate (13.3%), over 44 high risk (42.1%)
STOP-BANG for OSA
- •Snoring, Tired, Observed apnea, Pressure (HTN), BMI over 35, Age over 50, Neck over 40cm, Gender male
- •Score 0-2 = low risk, 3-4 = intermediate, 5-8 = high OSA risk
- •High risk: continue CPAP periop, avoid opioids, neuraxial preferred, HDU monitoring
- •Do NOT delay surgery for sleep study - empiric CPAP treatment
COPD Optimization (4-6 Weeks)
- •Smoking cessation minimum 4 weeks (50% PPC reduction at 8 weeks)
- •Bronchodilators: LAMA (tiotropium) if FEV1 under 60%
- •ICS: add if FEV1 under 60% AND 2+ exacerbations/year
- •Delay surgery 4-6 weeks after acute exacerbation
- •Physiotherapy: incentive spirometry, breathing exercises
- •FEV1 under 50% = severe COPD, high risk, HDU planning
PFT Indications
- •Moderate-severe COPD without recent spirometry (over 6 months old)
- •Unexplained dyspnea disproportionate to comorbidities
- •Smoking over 40 pack-years with symptoms (cough, sputum, wheeze)
- •Do NOT order routinely - exercise tolerance more predictive
- •Obstruction: FEV1/FVC under 0.70 confirms COPD
Postoperative PPC Prevention
- •Incentive spirometry 10 breaths Q2H while awake
- •Early mobilization - out of bed within 24 hours
- •Physiotherapy twice daily for secretion clearance
- •Multimodal analgesia - minimize opioids (regional blocks)
- •Semiupright positioning 30-45 degrees (reduces aspiration)
- •CPAP/BiPAP for OSA or respiratory failure risk