Congenital vs Acquired Instability
- Radiocapitellar Line: A line drawn through the center of the radial neck must bisect the capitellum in ALL views.
- Monteggia Lesion: Any ulnar fracture must have a reduced radial head. If not, it's a Monteggia.
- Nursemaid's Elbow: Subluxation of the annular ligament, not a true dislocation. Reduction is clinical (Hyperpronation).
- Congenital Signs: Bilateral, Dome shaped radial head (convex), Hypoplastic capitellum.
- “Always x-ray the Elbow in any forearm fracture.
- “Check the PIN (Finger extension) - commonly injured in anterior dislocations.
- “In children, plastic deformation of the ulna can cause radial head dislocation (Bado Type I equivalent).
The most common cause of legal litigation in paediatric orthopaedics. Always check the Radiocapitellar line.
The PIN wraps around the radial neck. Anterior dislocation often causes PIN neuropraxia.
A 'bowed' ulna in a child is a fracture. If the ulna is bowed and the head is out, it must be reduced (often requiring osteoclasis of the ulna).
Do not attempt to reduce a congenital dislocation! Look for the convex head and hypoplastic capitellum.
| Condition | Features | Treatment | Pearl |
|---|---|---|---|
| Nursemaid's Elbow | Child 1-4yo, pull on arm, held in pronation | **Closed Reduction** | First line: Hyperpronation (More effective than Supination/Flexion) |
| Acute Monteggia | Ulnar Fracture + Head out | **ORIF Ulna** | Anatomic ulna reduction reduces the head. |
| Chronic Missed Monteggia | Greater than 4 weeks, Ulnar malunion | **Ulnar Osteotomy** | Lengthen/Angulate ulna to reduce head. |
| Congenital | Bilateral, painless, convex head | **Observe** | Excise head in adulthood if painful. |
MUGRBado Classification (Monteggia)
Hook:See Bado types below: 1 (Ant), 2 (Post), 3 (Lat), 4 (Both).
Center-CenterRadiocapitellar Line
Hook:Neck centers on Cape.
Thumb UpPIN Palsy Signs
Hook:The Thumbs Down sign.
Overview and Epidemiology
Definitions:
- Dislocation: Complete loss of articular contact.
- Subluxation: Partial loss (e.g., Nursemaid's).
- Congenital: Developmental anomaly, present at birth.
- Traumatic: Acquired, usually high energy.
Epidemiology:
- Children: Common. Peak age 4-10 (Monteggia) or 1-4 (Nursemaid's).
- Adults: Rare as isolated injury. Usually associated with complex fracture-dislocations (Terrible Triad, Monteggia).
- Mechanism:
- Nursemaid's: Axial traction on pronated forearm.
- Monteggia: Fall on outstretched hand (FOOSH) with pronation (Type 1) or flexion (Type 2).
Anatomy
Bony Anatomy:
- Radial Head: Concave, articulates with convex capitellum. It is not perfectly circular (more oval).
- Safe Zone: The "Safe Zone" for hardware is the 90 degree arc that does not articulate with the ulna (Non-articular surface). This corresponds to the tripod position (lateral).
- Radial Notch: Indentation on proximal ulna for radial head.
- Relation: The radius moves with the ulna during flexion/extension but rotates around it during pronation/supination.
- Capitellum: The center of rotation for the radiocapitellar joint.
- Proximal Radio-Ulnar Joint (PRUJ): A trochoid (pivot) joint.
Stabilizers (Primary & Secondary):
- Primary:
- Ulnohumeral Joint: The coronoid is the primary stabilizer against posterior subluxation.
- MCL (Anterior Bundle): Primary stabilizer against Valgus.
- LCL (LUCL): Primary stabilizer against Varus and Posterolateral Rotatory Instability (PLRI).
- Secondary:
- Radial Head: An important secondary stabilizer against Valgus (if MCL is cut).
- Capsule: Anterior capsule resists extension.
- Annular Ligament: Primary stabilizer of the PRUJ. It arises from the anterior and posterior margins of the sigmoid notch. It is tighter around the neck than the head (funnel shape), preventing distal migration (Nursemaid's).
Nerves:
- PIN: Winds around the radial neck within the supinator muscle. Highly susceptible to injury in Anterior (Type 1) or Lateral (Type 3) dislocations.
- Safe Zone: The PIN is safe if the forearm is Pronated during lateral dissection. Supination brings the nerve closer to the surgical field in the Kaplan approach.
- Median Nerve: Can be entrapped in the joint in rare medial dislocations.
- Ulnar Nerve: Risk in Type 4 Monteggia or during medial approach for coronoid.
Vascular:
- Recurrent Radial Artery: The "Leash of Henry". Must be ligated to mobilize the supinator.
- Radial Artery: Anterior to the bicipital tuberosity.
- Blood Supply to Radial Head: Extra-osseous supply from the radial recurrent artery enter the neck. Intra-osseous supply is poor. "Watershed" area in the lateral portion of the head (Safe Zone).
Biomechanics:
- Load Transmission: The Radial Head transmits 60% of axial load at the elbow.
- Longitudinal Stability: The Radial Head prevents proximal migration of the radius (with IOM). Excision leads to proximal migration (Ulnar Variance becomes positive) leading to DRUJ pain.
Classification Systems
Based on the direction of the Radial Head dislocation (and Ulna apex).
- Type I (Anterior): Most common in kids (70%). Anterior head dislocation. Anterior ulna apex.
- Type II (Posterior): Most common in adults (80%). Posterior head dislocation. Posterior ulna apex. Associated with radial head fractures.
- Type III (Lateral): Lateral head dislocation. Lateral ulna apex. (Rare, associated with PIN palsy).
- Type IV: Fracture of both Radius and Ulna with dislocation.
Clinical Assessment
History:
- Child (1-4y): "Pulled up by arm", crying, arm held by side.
- Trauma: FOOSH.
- Chronic: Loss of ROM, prominence on lateral elbow (radial head).
Physical Exam:
- Nursemaid's: Arm held in extension + pronation. Resists supination. No swelling (if acute).
- Fracture: Swelling, bruising, deformity of ulna.
- Palpation: Palpate the radial head. Is it in the joint? Does it rotate?
- PIN: Check thumb extension.
Differential Diagnosis:
| Diagnosis | Discriminating Feature | Imaging Clue | Key Action |
|---|---|---|---|
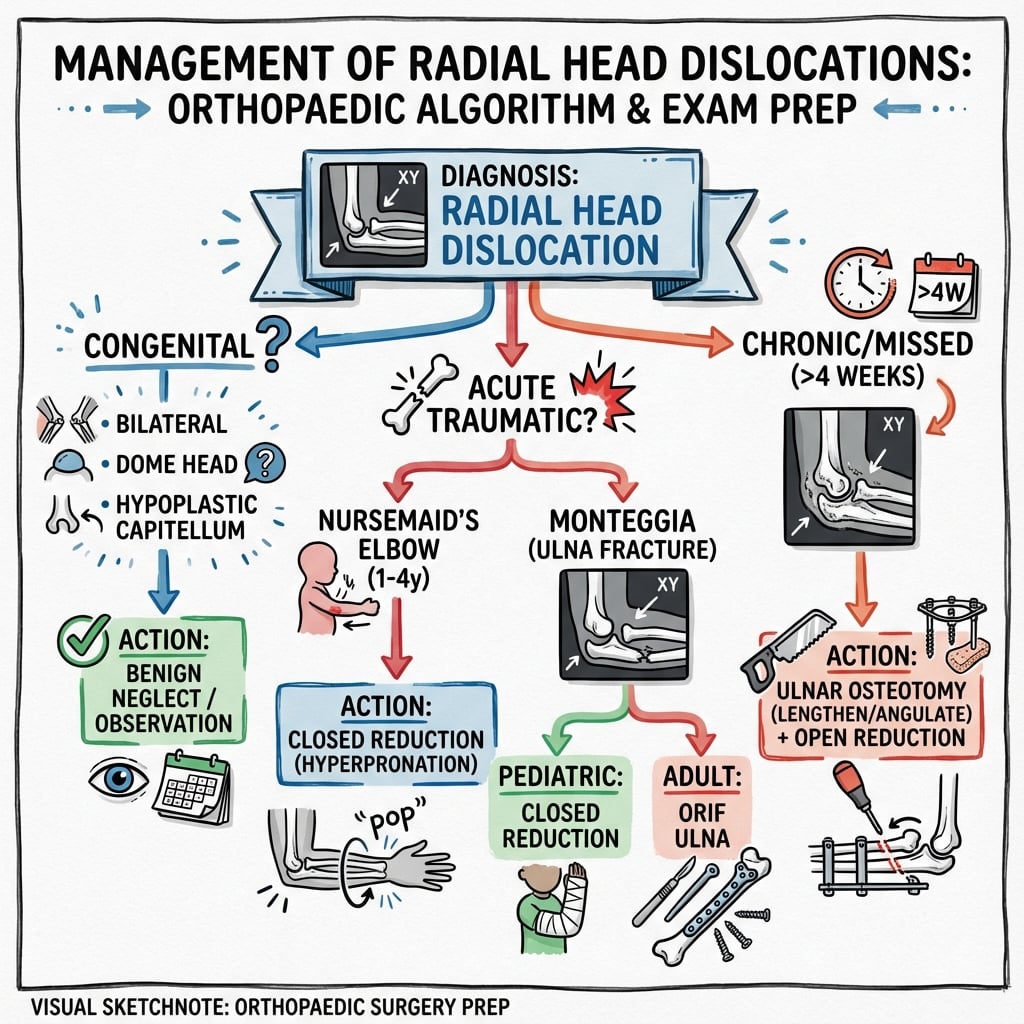
| Nursemaid's elbow (subluxation) | Age 1-4, axial pull, arm pronated and refused use, no swelling | Radiographs normal (often not needed) | Closed reduction (hyperpronation) |
| Acute / plastic Monteggia | Trauma, ulnar tenderness, head out on imaging | Disrupted radiocapitellar line + ulnar fracture or bow sign | Restore the ulna (reduce/ORIF or osteoclasis) |
| Chronic / missed Monteggia | Lateral prominence, lost rotation, weeks-months after injury | Ulnar malunion, convex remodelled head, dome capitellum | Ulnar osteotomy + open reduction |
| Congenital dislocation | Painless, often bilateral, frequently syndromic | Dome/convex head, hypoplastic capitellum, short ulna | Do NOT reduce; observe (excision in adulthood if painful) |
| Radial head/neck fracture | Localised tenderness, painful rotation, effusion | Fracture line, fat pad sign, head congruent | Treat fracture (non-op / ORIF / replacement) |
| Essex-Lopresti / longitudinal instability | Wrist (DRUJ) pain with elbow injury, axial load mechanism | Positive ulnar variance, proximal radial migration | Preserve/replace radial head; never excise alone |
Investigations
X-rays:
- Elbow AP/Lat: Mandatory.
- Check: Radiocapitellar Line.
- Check: Ulnar bowing (Plastic deformation).
- Check: Capitellum shape (Round vs Flat).
- Forearm: Exclude shaft fractures.
- Wrist: Exclude Galeazzi.
CT Scan:
- Indicated for chronic cases to assess articular congruity and ulnar deformity planning.
- Adult Type II Monteggia (Check for coronoid fracture).
- 3D Reconstruction: Essential for understanding the "shotgun" deformity of the proximal ulna in comminuted Monteggia fractures.
Radiographic Parameters (Detailed):
| Parameter | Normal Value | Pathology | Technique |
|---|---|---|---|
| Radiocapitellar Line | Intersects Capitellum | Dislocation | Draw line through center of radial neck shaft. Must hit capitellum in ALL views. |
| Ulnar Bow | Straight posterior border | Plastic Deformation | Draw line along posterior border of proximal ulna. Max deviation greater than 1mm suggests deformation. |
| Radial Head Shape | Concave | Congenital | Convex or dome-shaped head indicates congenital dislocation. |
| Ulnar Variance | Neutral | Longitudinal Instability | Positive variance (=Proximal migration of radius) suggests Essex-Lopresti lesion. |
Associated Injuries (The Checklist):
- Coronoid Fracture: 10-15% of radial head dislocations. Pathognomonic for Terrible Triad.
- LCL Rupture: Always present in dislocation. Usually avulses from the Lateral Epicondyle.
- MCL Rupture: Present in valgus instability or high energy trauma.
- DRUJ Injury: Present in Type 4 Monteggia or Essex-Lopresti (Longitudinal instability). Always examine the wrist!
- Capitellar Shear Fracture: The radial head can shear off the capitellum/trochlea as it dislocates.
MRI:
- Rarely indicated in acute setting.
- Useful in chronic "painful clicking" to assess for loose bodies or plica.
- Can assess integrity of the PIN in non-recovering nerves.
Management Algorithm
Pulled Elbow (Subluxation):
- Reduction:
- Hyperpronation: Hold elbow at 90. Firmly pronate wrist. Usually clicks. High success rate.
- Supination-Flexion: Supinate wrist, then flex elbow.
- Post-Reduction: Child should use arm within 10-15 mins. No cast needed.
Surgical Techniques
Indications: Irreducible acute dislocation or Chronic reconstruction.
- Approach: Kocher (Interval: Anconeus/ECU) or Kaplan (EDC/ECRB).
- Technique:
- Position: Supine, arm over chest or on hand table. Tourniquet high arm.
- Incision: Lateral over the RH, extending distally towards the ulna.
- Interval (Kocher): Between Anconeus (Radial n) and ECU (PIN). The internervous plane is safe distally but the PIN is at risk proximally if extending too far anteriorly.
- Dissection: Elevate Anconeus posteriorly. Incise capsule anterior to the LUCL.
- Identify R-C joint.
- Maneuver: Remove interposed soft tissue (Annular ligament may be folded in).
- Reduction: Flexion and pronation usually reduces the head.
- Repair: Annular Ligament repair is difficult. If stable, leave it. If unstable, reconstruct (Bell-Tawse procedure using Triceps strip).
- Closure: Close the interval (Anconeus fascia) securely.
Pre-Operative Planning:
- Templating: Measure the normal side (if bilateral films available) to estimate radial head size.
- Ulna Length: If chronic, measure the ulnar length discrepancy. You may need to lengthen the ulna by 1-2cm.
- Implants: Have small fragment set (3.5mm), mini-fragment set (2.0/2.4mm for head/coronoid), and radial head replacement options (Simplex or Modular) available.
Surgical Pearls:
- The "Shotgun" Approach: For comminuted proximal ulna fractures, extend the incision distally. Expose the shaft. Reduce the shaft first to restore length. The proximal fragments often "explode" outwards.
- Coronoid Check: After fixing the ulna, check the coronoid. If fractured, it MUST be fixed (suture lasso or screws) as it prevents posterior instability.
- Head Height: If replacing the head, do not "overstuff" the joint. The prosthetic head should be level with the coronoid tip. Overstuffing causes stiffness and capitellar wear.
- LCL Repair: Reattach the LCL to the isometric point on the lateral epicondyle (center of curvature of the capitellum). Use suture anchors.
- Scope: If unsure about reduction, an arthroscope can be placed (if available) to view the R-C joint from inside.
Complications
- PIN Palsy:
- Common in Type I and III.
- Usually resolves after reduction.
- Iatrogenic risk during Kaplan approach.
- Recurrent Dislocation:
- Failure to anatomically reduce the ulna.
- Failure to recognize plastic deformation.
- Stiffness:
- Loss of Pronation/Supination.
- Common after open reduction.
- Radio-Ulnar Synostosis:
- Risk with single incision or extensive dissection.
Postoperative Care
- Acute Reduced:
- Splint in Supination (Type I) or Extension (Type II).
- Weekly X-rays for 3 weeks.
- Post-Op:
- Splint for 2 weeks.
- Protected ROM (Hinge brace).
- Avoid heavy lifting for 3 months.
Detailed Rehab Phases (Adult Monteggia):
- Phase 1 (Week 0-2):
- Long arm splint.
- Edema control (Elevation).
- Finger/Shoulder ROM.
- Phase 2 (Week 2-6):
- Removal of splint/sutures.
- Hinged Elbow Brace (0-100 degrees).
- Active Assist ROM: Flexion/Extension.
- Forearm Rotation: Done with elbow at 90 degrees (protects LCL).
- Avoid: Varus stress (shoulder abduction).
- Phase 3 (Week 6-12):
- Wean brace.
- Static progressive splinting if stiff (Turnbuckle).
- Begin strengthening (Theraband).
- Phase 4 (Month 3+):
- Work hardening.
- Return to sport (if contact, wait for solid union 4-6 months).
Outcomes/Prognosis
- Nursemaid's: Excellent. 100% recovery. High recurrence rate until age 5.
- Acute Monteggia:
- Type I (Kids): Excellent if reduced. 90% good/excellent outcomes.
- Type II (Adults): Variable. High risk of stiffness and heterotopic ossification. MEPS (Mayo Elbow Performance Score) averages 85.
- Chronic Missed:
- Poor prognosis without surgery (progressive Valgus, PIN palsy).
- Surgery (Osteotomy) has 70% success rate but high complication rate (stiffness, nerve injury).
- Congenital:
- Generally functional adaptation.
- Often pain-free until adulthood.
- Excision in adulthood gives unpredictable pain relief.
Complications Detail:
- Stiffness: The most common complication. Extension loss of 10-15 degrees is common and functional. Flexion loss is poorly tolerated. Pronation/Supination loss is common if IOM injured.
- Heterotopic Ossification (HO): Common in adults with head injury or prolonged intubation. Indomethacin prophylaxis indicated for high risk.
- Synostosis: Cross-union between radius and ulna. Risk factors: Single incision for both bones, delayed fixation, head injury. Treatment: Excision after bone scan is "cold" (12-18 months).
- Implant Removal: Plates on the proximal ulna are prominent and often require removal. 40% removal rate.
Mayo Elbow Performance Score (MEPS):
- Pain (45 points): None = 45, Moderate = 30, Severe = 0.
- Motion (20 points): Greater than 100 deg arc = 20, 50-100 = 15, Less than 50 = 5.
- Stability (10 points): Stable = 10, Unstable = 0.
- Function (25 points): Combing hair, Feeding, etc.
- Greater than 90 = Excellent, 75-89 = Good.
| Approach | Interval | Pros | Cons/Risks |
|---|---|---|---|
| Kocher | Anconeus / ECU | Safer for PIN (if not extended too far) | Less anterior exposure. Hard to see coronoid. |
| Kaplan | EDC / ECRB | Excellent anterior exposure (Coronoid access) | High risk of PIN injury (Nerve crosses field). |
Evidence
Hyperpronation vs Supination/Flexion (RCT)
- Prospective randomised trial, 90 children under 6 with nursemaid's elbow (84 analysed).
- First-attempt success 95% (39/41) with hyperpronation vs 77% (34/44) with supination/flexion.
- Hyperpronation required fewer attempts and often succeeded after supination had failed (5/6 cross-over successes).
- Overall reduction 97.5% hyperpronation vs 86% supination.
Chronic Monteggia: Open Reduction, Annular Reconstruction and Ulnar Osteotomy
- 15 children with chronic Monteggia lesions (mean age 8 years; chronicity 6 weeks to 2 years).
- Treated with open reduction, annular ligament reconstruction using forearm fascia, and ulnar osteotomy via a single incision.
- Functional result excellent in 11, good in 3, poor in 1; flexion arc improved in all (mean 27.7 degrees).
- Modest loss of pronation (mean 16 degrees in 6 cases).
The Ulnar Bow Sign — 'Isolated' Traumatic Radial Head Dislocation
- Retrospective review identified a definable ulnar injury in EVERY case of so-called isolated radial head dislocation.
- Described the 'ulnar bow sign': deviation of the posterior ulnar border from a straight line on a true lateral.
- Truly isolated radial head dislocation is essentially a myth — look for plastic deformation of the ulna.
PIN Course Relative to the Proximal Radius (Forearm Rotation)
- Cadaveric 3D study (6 specimens) mapping the PIN against the proximal radius in rotation.
- Laterally the PIN crossed the radial neck a mean of 33mm below the radial head surface in pronation versus 17mm in supination.
- Pronation moves the PIN distally and away from the lateral surgical field, increasing its safety margin to roughly 3cm.
- The radial tuberosity is a reliable intraoperative landmark for the nerve.
Radial Head Shape, Overstuffing and Radiocapitellar Load
- Cadaveric study of 6 upper extremities altering radial head orientation.
- Ulnohumeral kinematics were unaffected by changing radial head shape (differences not significant).
- Radiocapitellar joint force rose markedly with an altered/non-anatomic head, predisposing to degenerative change.
- Underlines the consequences of a poorly contoured or oversized (overstuffed) radial head prosthesis.
Plastic Monteggia — Action on the Ulna is Central
- Case series of chronic radial head dislocation with plastic deformation of the ulna in children.
- Reaffirms that most 'isolated' dislocations are associated with ulnar plastic deformation (after Lincoln & Mubarak and Dubuc).
- Treatment combined open reduction, annular ligament reconstruction and ulnar osteotomy where needed (3 of 4 cases).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 6-year-old child presents with a radial head dislocation. There is no obvious fracture on X-ray.”
Evaluation:
- Suspicion: This is a Monteggia Variant until proven otherwise.
- Look for: Plastic deformation of the ulna (bowing). Is the ulna straight?
- Congenital: Check the other elbow! Is it bilateral? Is the head dome-shaped?
- Management: If traumatic, attempt reduction. If unstable, the ulna is plastically deformed and needs straightening (Osteoclasis).
“You see an adult with a chronic, asymptomatic radial head dislocation. They are worried about appearance.”
Counseling:
- Risk vs Benefit: Surgery for chronic dislocation in adults is unpredictable and high risk for stiffness and pain.
- Recommendation: Benign neglect. Do NOT operate for cosmesis.
- Option: If painful, excision is the only reliable option (if DRUJ stable).
“You perform an open reduction of a radial head dislocation in a child using a Kocher approach. Post-operatively, the child cannot extend their thumb.”
Diagnosis: Iatrogenic PIN Palsy.
Mechanism: The PIN was likely retracted too vigorously or the dissection went too far anteriorly/distally without identifying the nerve. The PIN rests on the anterior aspect of the radial neck.
Management:
- Immediate: Remove splint, extend wrist.
- Wait: Observation for 3 months (Neuropraxia is most common).
- Investigations: Ultrasound or Nerve conduction studies at 6 weeks if no recovery.
- Surgery: Exploration if nerve was seen to be cut (unlikely in Kocher, more likely in Kaplan). Tendon transfers if permanent.
MCQ Practice Points
Q: Which X-ray sign is pathognomonic for congenital dislocation? A: Convex (Dome-shaped) Radial Head and Hypoplastic Capitellum.
Q: Which nerve is most at risk in a Type I Monteggia fracture? A: Posterior Interosseous Nerve (PIN).
Q: What is the most successful maneuver for reducing a pulled elbow? A: Hyperpronation.
Q: What structure prevents proximal migration of the radius? A: The Central Band of the Interosseous Membrane.
Q: A posterior dislocation of the radial head with a posterior angulated ulna fracture is which Bado type? A: Type II.
Controversies & Areas of Uncertainty
- Is truly isolated radial head dislocation real? Lincoln and Mubarak found a definable ulnar injury in every "isolated" case, yet rare genuinely isolated traumatic dislocations are reported. Practically, treat every paediatric "isolated" dislocation as a plastic Monteggia and scrutinise the ulna.
- Acute vs delayed osteotomy in missed Monteggia: No consensus on the upper time limit for attempting reduction. Many achieve good results up to 1-3 years from injury, challenging older teaching that reconstruction beyond a few months is futile. Outcome depends more on chronicity and ulnar remodelling than a fixed cut-off age.
- Annular ligament reconstruction — necessary or not? Some series (e.g. single-incision techniques) report stable reductions from ulnar osteotomy alone without formal annular reconstruction, questioning routine Bell-Tawse-type reconstruction and its stiffness/synostosis risk.
- Imaging before reduction of pulled elbow: Routine radiographs are not required in a classic presentation; films are reserved for atypical history or failed reduction, where occult fracture prevalence remains low.
- Stable Monteggia radial head — fix, replace or leave: In adult Bado II with comminuted radial head, the threshold for replacement vs excision vs fixation after restoring ulnar length is debated; excision is avoided where longitudinal/DRUJ instability coexists.
- PIN palsy — when to explore: Most resolve with observation after reduction, but persistent palsy beyond 3 months with nerve entrapment in the radiocapitellar joint may warrant exploration; the exact timing for surgery is not standardised.
Guidelines, Registries & Global Practice
Global epidemiology:
- Pulled elbow (nursemaid's) is among the most common upper-limb presentations in children under 5 worldwide, peaking at 1-4 years with a female and left-arm predominance; recurrence is frequent until ligamentous maturity around age 5.
- Monteggia lesions are uncommon (about 1-2% of forearm fractures); Bado type I predominates in children and type II in adults.
- Missed/chronic Monteggia is a recognised global source of avoidable disability and medicolegal claims, driven by failure to apply the radiocapitellar line on every paediatric elbow/forearm film.
Side-by-side guidance (where emphasis differs):
| Source | Key Position | Practical Point |
|---|---|---|
| AAOS / OTA (US) | Anatomic restoration of ulnar length and alignment is the primary determinant of radial head reduction in Monteggia. | Fix the ulna first; reassess radiocapitellar congruity intra-operatively. |
| BOA / BSCOS (UK) | Every forearm/elbow injury in a child must have the radiocapitellar line checked to avoid the missed Monteggia. | Document the line on AP and lateral views. |
| AO Foundation | Proximal ulnar fixation must reproduce the dorsal angulation/bow; long plates and length restoration are stressed. | Beware the 'shotgun' comminuted proximal ulna — restore length via the shaft first. |
| EFORT / European consensus | Low threshold to image the contralateral elbow and to differentiate congenital from traumatic dislocation. | Bilateral, dome-shaped head = congenital; do not reduce. |
Registry / outcome notes: There is no dedicated radial head dislocation registry; radial head arthroplasty data are captured indirectly within elbow arthroplasty and implant series rather than national joint registries (NJR, AOANJRR, AJRR), which focus on hip/knee/shoulder. Most evidence is therefore Level IV case series.
High- vs limited-resource practice:
- Well-resourced: CT/3D planning for comminuted proximal ulna, modular radial head implants, hinged external fixators, and intra-operative imaging are routinely available.
- Limited-resource: Reliance on plain radiographs and the radiocapitellar line, plate or even K-wire/ex-fix ulnar fixation, and biological annular reconstruction (triceps/forearm fascia) rather than implants. Early recognition of the plastic Monteggia is the single highest-yield, low-cost intervention.
Radiocapitellar Line
- Line through center of radial neck
- Must bisect capitellum in ALL views
- Check AP, lateral, and oblique views
- Disruption indicates dislocation
Bado Classification
- I: Anterior (Extension) - Most common in children
- II: Posterior (Flexion) - Most common in adults
- III: Lateral
- IV: Both bones (radius and ulna)
Paediatric vs Adult
- Paeds: Closed Reduction (Cast)
- Adult: ORIF (Plate)
- Paeds: Anterior (Type I) most common
- Adult: Posterior (Type II) most common
Red Flags
- Plastic Ulnar Bowing in children
- PIN Palsy (finger extension weakness)
- Bilateral = likely Congenital
- Dome-shaped radial head = Congenital
Nursemaid's Elbow
- Hyperpronation technique preferred
- Audible click = successful reduction
- Immediate use of arm post-reduction
- No imaging needed if classical presentation