Posterior Interosseous Nerve Compression | Pain Without Weakness | Controversial Diagnosis
FIVE POTENTIAL COMPRESSION SITES
Critical Must-Knows
- Pain without weakness - distinguishes from PIN syndrome (motor palsy)
- Arcade of Frohse - fibrous arch at proximal supinator edge (70% of cases)
- Rule of 9s test - pain with resisted long finger extension at 9cm distal to lateral epicondyle
- Conservative management first - 3-6 months trial before considering surgery
- Electrodiagnostics usually normal - clinical diagnosis, not confirmed by EMG/NCS
Clinical Pearls
- "Radial tunnel syndrome = pain only; PIN syndrome = motor palsy
- "Differential diagnosis includes lateral epicondylitis (tennis elbow)
- "Arcade of Frohse is present in 30% of population (fibrous in 50% of those)
- "Surgical decompression has variable outcomes (50-90% success)
Clinical Imaging
Imaging Gallery




Critical Radial Tunnel Syndrome Exam Points
No Motor Weakness
RTS is a pain syndrome WITHOUT motor weakness. If extensor weakness is present, this is Posterior Interosseous Nerve (PIN) syndrome, not radial tunnel syndrome. Pure sensory pain in the proximal forearm is the hallmark.
Five Compression Sites
FACES mnemonic: Fibrous bands, Arcade of Frohse (most common 70%), ECRB edge, Supinator distal edge, Leash of Henry. The arcade is a fibrous arch at the proximal supinator in 30% of population.
Rule of 9s Test
Pain with resisted long finger MCP extension at 9cm distal to lateral epicondyle is the specific test. This localizes the PIN at the radial tunnel and differentiates from lateral epicondylitis (pain at epicondyle).
Controversial Diagnosis
RTS is controversial - some surgeons question its existence. Electrodiagnostics are usually normal. Diagnosis is clinical. Conservative management for 3-6 months is mandatory before considering surgery.
Differential Diagnosis - RTS vs Lateral Epicondylitis vs PIN Syndrome
| Feature | Radial Tunnel Syndrome | Lateral Epicondylitis | PIN Syndrome |
|---|---|---|---|
| Pain location | Mobile mass 4-5cm distal to lateral epicondyle | Lateral epicondyle (fixed) | Proximal forearm (with weakness) |
| Motor weakness | None (key feature) | None | Extensor weakness (thumb, fingers) |
| Resisted wrist extension | Pain distal to epicondyle | Pain at epicondyle | Weakness with pain |
| Rule of 9s test | Positive (pain at 9cm) | Negative | May be positive with weakness |
| Electrodiagnostics | Normal | Normal | Abnormal (denervation of PIN-innervated muscles) |
At a Glance
Radial tunnel syndrome is a controversial pain syndrome without motor weakness, distinguishing it from PIN syndrome which causes extensor paralysis. The posterior interosseous nerve is compressed at one of five sites (FACES mnemonic), with the Arcade of Frohse (fibrous proximal supinator edge) being most common (70%). Diagnosis is clinical using the Rule of 9s test - pain with resisted long finger MCP extension at 9cm distal to the lateral epicondyle - as electrodiagnostics are typically normal. Conservative management (activity modification, NSAIDs, splinting) should be trialled for 3-6 months before considering surgical decompression, which has variable outcomes (50-90% success).
FACESFACES - The Five Compression Sites
| F | Fibrous bands Anterior to radial head (proximal-most site) |
| A | Arcade of Frohse Proximal supinator edge (most common - 70%) |
| C | ECRB edge Tendinous margin of extensor carpi radialis brevis |
| E | Exit from supinator Distal edge of supinator muscle |
| S | Leash (vessels) Recurrent radial vessels (leash of Henry) |
| F | Fibrous bands Anterior to radial head (proximal-most site) | E | Exit from supinator Distal edge of supinator muscle |
| A | Arcade of Frohse Proximal supinator edge (most common - 70%) | S | Leash (vessels) Recurrent radial vessels (leash of Henry) |
| C | ECRB edge Tendinous margin of extensor carpi radialis brevis |
Hook:The PIN FACES five obstacles as it passes through the radial tunnel
NINENINE - Rule of 9s Test Components
| N | Nine centimeters Distance distal to lateral epicondyle |
| I | Index or long finger Resist MCP extension (long finger most specific) |
| N | No motor weakness Pain only, no extensor palsy |
| E | Elbow extension Test with elbow extended, forearm pronated |
| N | Nine centimeters Distance distal to lateral epicondyle | N | No motor weakness Pain only, no extensor palsy |
| I | Index or long finger Resist MCP extension (long finger most specific) | E | Elbow extension Test with elbow extended, forearm pronated |
Hook:NINE helps remember the rule of 9s test - 9cm distal, long finger resistance, no weakness
SPRINTSPRINT - Conservative Management Protocol
| S | Splint Forearm supination splint to reduce compression |
| P | Physical therapy Stretching and strengthening exercises |
| R | Rest from aggravating activities Activity modification |
| I | Injection Steroid injection into radial tunnel (diagnostic and therapeutic) |
| N | NSAIDs Anti-inflammatory medication |
| T | Time 3-6 months trial before surgery |
| S | Splint Forearm supination splint to reduce compression | R | Rest from aggravating activities Activity modification | N | NSAIDs Anti-inflammatory medication |
| P | Physical therapy Stretching and strengthening exercises | I | Injection Steroid injection into radial tunnel (diagnostic and therapeutic) | T | Time 3-6 months trial before surgery |
Hook:SPRINT through conservative treatment before considering surgical decompression
Overview and Epidemiology
Radial Tunnel Syndrome (RTS) is a controversial clinical entity characterized by pain in the proximal lateral forearm attributed to compression of the posterior interosseous nerve (PIN) within the radial tunnel, without motor weakness.
The radial tunnel:
- Extends from the radial head to the distal edge of the supinator muscle
- Approximately 4-5cm in length
- Contains the posterior interosseous nerve (deep branch of radial nerve)
- Has five potential compression sites along its course
Why Controversial?
RTS is controversial because: (1) electrodiagnostic studies are usually normal, (2) there is significant overlap with lateral epicondylitis, (3) surgical outcomes are variable (50-90% success), and (4) some authors question whether it is a distinct entity. Conservative management is always tried first.
Key distinguishing feature:
- RTS = pain WITHOUT motor weakness
- PIN syndrome = motor weakness (extensor palsy)
Clinical presentation:
- Aching pain in the proximal dorsal forearm
- Pain described as a mobile tender mass 4-5cm distal to lateral epicondyle
- Exacerbated by repetitive pronation-supination and gripping
- No weakness of thumb or finger extension (if weakness present = PIN syndrome)
Pathophysiology and Anatomy
Radial Nerve Anatomy
The radial nerve divides into superficial radial nerve (sensory) and posterior interosseous nerve (motor) at the level of the radiocapitellar joint. The PIN enters the radial tunnel and passes through the supinator muscle to innervate all finger and thumb extensors (except ECRL, which is innervated before the split).
Radial nerve course:
- Proximal forearm: Radial nerve lies between brachialis and brachioradialis
- Radiocapitellar joint level: Divides into superficial branch (sensory) and deep branch (PIN - motor)
- Radial tunnel entry: PIN enters tunnel anterior to radial head
- Supinator passage: PIN passes through supinator muscle via arcade of Frohse
- Tunnel exit: Emerges at distal supinator edge to innervate extensors
The five potential compression sites (FACES):
Arcade of Frohse (Most Common - 70%)
Anatomy:
- Fibrous arch at the proximal edge of the supinator muscle
- Present in approximately 30% of the population
- When present, it is fibrous (non-yielding) in 50% of cases
- Formed by the tendinous margin of the superficial head of supinator
Mechanism of compression:
- PIN passes beneath the arcade as it enters the supinator
- Pronation increases tension on the arcade
- Repetitive pronation-supination causes chronic irritation
- Fibrous arcade does not yield during forearm rotation
Clinical significance:
- Most common site of compression in radial tunnel syndrome
- Target of surgical decompression (release the arcade)
- Variable anatomy explains inconsistent surgical outcomes
This is the most important compression site to know for exams.
Pathophysiology:
Repetitive pronation-supination activities cause mechanical compression of PIN at one or more sites in the radial tunnel. Most commonly at the arcade of Frohse during pronation.
Chronic compression leads to perineural inflammation and nerve irritation. The nerve does not develop significant demyelination or axonal injury (hence normal electrodiagnostics).
Patients develop chronic pain in the proximal forearm without motor dysfunction. The pain is thought to be from nociceptive C-fibers in the nerve sheath, not from nerve dysfunction.
Clinical Presentation and Diagnosis
Classic History
Patient presents with aching pain in the proximal dorsal forearm, 4-5cm distal to the lateral epicondyle. Pain is worse with repetitive pronation-supination (turning a screwdriver, doorknob) and gripping. No motor weakness. Often misdiagnosed as lateral epicondylitis (tennis elbow).
History:
Symptoms
- Pain location: Proximal dorsal forearm
- Quality: Deep, aching, burning
- Radiation: May extend to dorsal forearm
- Aggravating factors: Pronation, supination, gripping
- Relieving factors: Rest, forearm supination
- Duration: Usually insidious onset over weeks to months
- No paresthesias or numbness (purely motor nerve)
Risk Factors
- Occupational: Repetitive pronation-supination activities
- Sports: Racquet sports, golf, weightlifting
- Previous trauma: Radial head fracture, elbow dislocation
- Anatomic: Fibrous arcade of Frohse
- Coexisting conditions: Lateral epicondylitis (5% overlap)
- Space-occupying lesions: Lipoma, ganglion (rare)
Physical Examination:
Inspection
- No visible deformity in most cases
- No muscle wasting (differentiates from PIN syndrome)
- Compare both forearms for symmetry
Palpation
- Tenderness at 4-5cm distal to lateral epicondyle (over radial tunnel)
- Patient describes tender area as a mobile mass
- Tenderness moves with pronation and supination
- No tenderness directly at lateral epicondyle (if present, consider lateral epicondylitis)
Mobile mass sign:
- PIN and radial tunnel move during forearm rotation
- Tender point moves distally with pronation, proximally with supination
- Differentiates RTS from lateral epicondylitis (fixed tenderness at epicondyle)
Palpation is the most important examination finding.
Investigations
Electrodiagnostics in RTS
EMG and nerve conduction studies are USUALLY NORMAL in radial tunnel syndrome. This is because the compression causes pain but not significant demyelination or axonal injury. Normal electrodiagnostics do NOT rule out RTS. Diagnosis is clinical.
Electromyography (EMG) and Nerve Conduction Studies (NCS)
Typical findings in RTS:
- Normal motor latencies (radial nerve and PIN)
- Normal sensory latencies (superficial radial nerve)
- No denervation on needle EMG
- Normal recruitment in PIN-innervated muscles
Role:
- Rule out PIN syndrome (which shows denervation)
- Rule out radial nerve palsy (proximal lesion)
- Rule out C7 radiculopathy (cervical spine)
- Confirm clinical diagnosis is not due to nerve pathology
If EMG shows denervation of PIN muscles: This is PIN syndrome, not RTS
Findings in PIN Syndrome (for comparison)
- Denervation in PIN-innervated muscles (supinator, ECU, EDC, EPL, APL)
- Fibrillation potentials and positive sharp waves on needle EMG
- Reduced recruitment in affected muscles
- Indicates axonal injury requiring surgical decompression
Electrodiagnostics differentiate RTS (normal) from PIN syndrome (abnormal).
Management
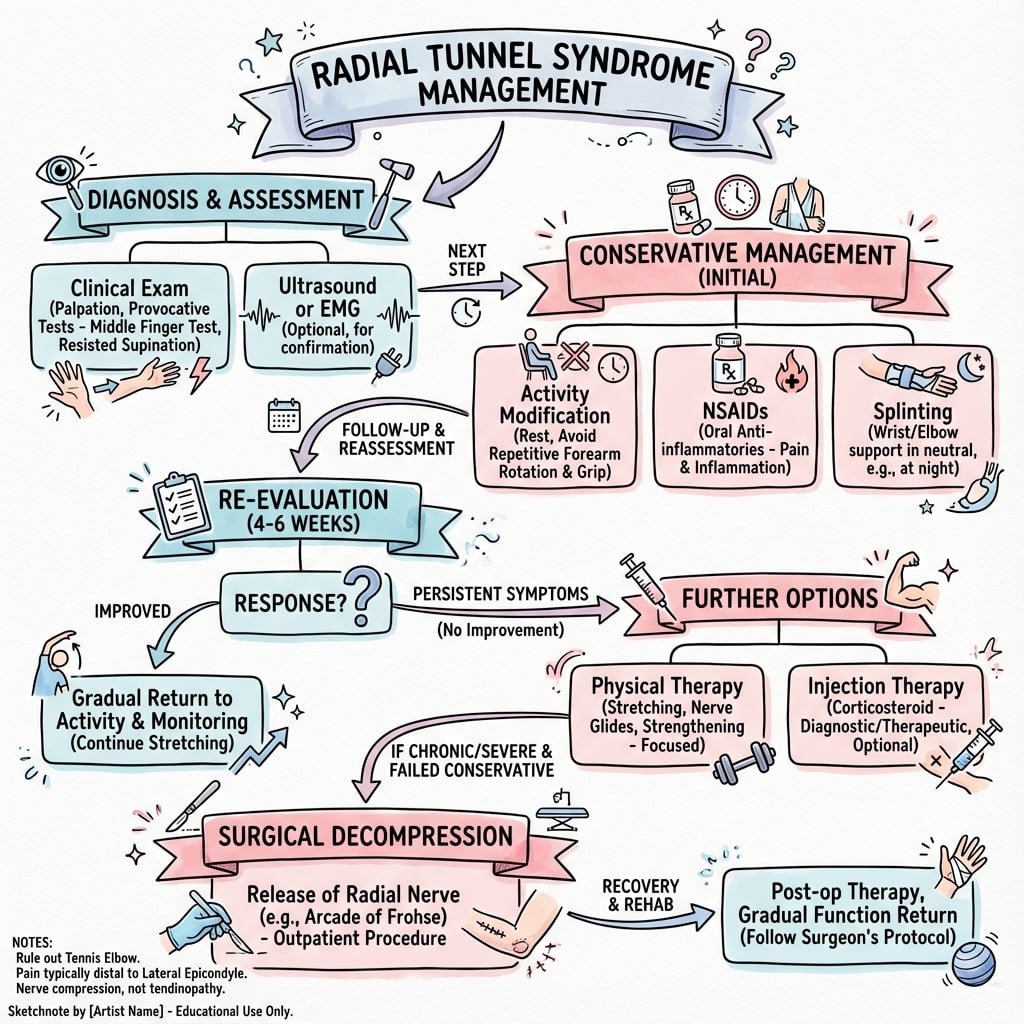
Treatment Hierarchy
Conservative management for 3-6 months is MANDATORY before considering surgical decompression. Surgery has variable outcomes (50-90% success) and should be reserved for patients who fail comprehensive non-operative treatment. Diagnostic injection can help select surgical candidates.
Conservative Management (First-Line - 60-80% Success)
Duration: Minimum 3-6 months trial before surgery
1. Activity Modification
- Avoid repetitive pronation-supination activities
- Avoid forceful gripping with forearm pronated
- Ergonomic workplace modifications
- Limit aggravating sports activities
2. Splinting
- Forearm supination splint to reduce compression
- Wear during activities and at night
- 6-8 weeks trial
- Keeps forearm in neutral to supination (opens arcade of Frohse)
3. NSAIDs
- Ibuprofen 400-600mg three times daily with food
- Naproxen 500mg twice daily
- Duration: 2-4 weeks
- Watch for GI side effects
4. Physical Therapy
- Stretching: Forearm flexor and extensor stretches
- Strengthening: Progressive resistance exercises
- Nerve gliding: Radial nerve glides to reduce adhesions
- Modalities: Ice, ultrasound (limited evidence)
5. Corticosteroid Injection
- Indication: Failure of conservative measures at 6 weeks
- Technique: 2-3mL of triamcinolone 40mg/mL + 1% lidocaine
- Injection site: 4-5cm distal to lateral epicondyle, deep to brachioradialis
- Expected: Immediate relief if diagnosis correct
- Repeat: Can repeat once if partial response at 6 weeks
- Value: Diagnostic AND therapeutic
6. Observation
- Regular follow-up every 4-6 weeks
- Reassess symptoms and examination
- Reassess differential diagnosis if not improving
Most patients (60-80%) improve with conservative management.
Complications
Intra-operative Complications
Posterior interosseous nerve injury (Most serious - 1-5%):
- Mechanism: Direct injury during dissection, stretch injury, thermal injury
- Presentation: Post-operative finger and thumb extensor weakness
- Prevention: Careful identification and protection of PIN throughout decompression
- Management: Observation for 3-6 months (most recover), nerve exploration/repair if no recovery
Vascular injury:
- Leash of Henry (recurrent radial vessels) can be injured
- Prevention: Careful dissection, no tourniquet (see vessels)
- Management: Direct pressure, ligation if necessary
Early Post-operative Complications (less than 6 weeks)
Wound complications:
- Infection: Less than 1%, treat with antibiotics +/- washout
- Hematoma: Rare without tourniquet, may require evacuation
- Dehiscence: Rare, secondary closure
Persistent pain:
- Incomplete decompression: May need revision
- Wrong diagnosis: Consider alternative diagnosis
- Nerve injury: Neuropathic pain
Late Complications (more than 6 weeks)
Recurrent symptoms (10-30%):
- Incomplete decompression: Most common cause
- Scar formation: Nerve re-compression
- Adhesions: Nerve tethering
- Management: Revision decompression in selected cases
Loss of supination strength (10-20%):
- Supinator muscle partially released
- Usually minimal functional impact
- Improves with strengthening exercises
Lateral antebrachial cutaneous nerve injury:
- Numbness/dysesthesia in lateral forearm
- Prevention: Identify and protect during superficial dissection
- Usually resolves over 6-12 months
Chronic regional pain syndrome (CRPS):
- Rare (less than 1%)
- Disproportionate pain, autonomic changes
- Management: Early PT, desensitization, pain clinic
PIN injury is the most serious complication - prevention is key.
Controversies and Areas of Uncertainty
RTS is one of the most contested diagnoses in upper-limb surgery. Examiners use it to probe how you handle weak evidence and diagnostic uncertainty.
Does RTS exist as a distinct entity?
Rosenbaum argued the term should be reserved for truly neurogenic (motor) cases, viewing the pain-only variant as a flawed analogy to carpal tunnel syndrome. Others accept RTS as a real compressive pain syndrome. There is no resolution; the safe exam line is that it is a clinical diagnosis of exclusion.
RTS vs lateral epicondylitis - separable?
The two overlap clinically and anatomically (ECRB edge), can coexist, and some surgeons treat them as a spectrum. Distinguishing point of maximal tenderness (at the epicondyle versus 4-5 cm distal) is the practical, if imperfect, separator.
Value of diagnostic injection
A positive local-anaesthetic injection is widely used to confirm the diagnosis and predict surgical success, but it is not validated against a true reference standard and a positive result may simply reflect non-specific local anaesthesia.
How much to decompress
Whether to release all five sites versus selective release is debated. Wilhelm's large series found that adding direct PIN decompression did not improve results over simpler procedures, questioning aggressive multi-site release.
The Balanced Exam Answer
State up front that RTS is a controversial, clinically diagnosed pain syndrome with normal electrodiagnostics; emphasise excluding PIN syndrome (weakness) and lateral epicondylitis; commit to a prolonged conservative trial; and reserve surgery for well-selected patients with a positive diagnostic injection after failed non-operative care, with honest counselling about variable outcomes.
Evidence Base
Original Description - Resistant Tennis Elbow as Nerve Entrapment
- Introduced the concept of radial tunnel syndrome as a distinct entity
- Proposed that a subset of 'resistant tennis elbow' is radial nerve/PIN entrapment in the radial tunnel rather than epicondylar tendinopathy
- Reported symptom relief after surgical decompression, establishing the Roles and Maudsley outcome grade still used today
Anatomical Basis - The Arcade of Frohse
- Classic anatomical study of the arcade of Frohse, the fibrous proximal margin of the supinator
- Identified the arcade as the key structure related to posterior interosseous nerve compression in the proximal forearm
- Demonstrated variability of the arcade between fibrous and membranous forms
Diagnosis and Management Review
- RTS is a pain syndrome from PIN compression with no specific radiologic or electrodiagnostic findings
- Recommends conservative treatment first, with surgical release of all potential entrapment sites if it fails
- Outcomes are generally good but poorer with coexisting lateral epicondylitis or workers' compensation claims
Large Surgical Series - Decompression for Resistant Tennis Elbow
- Series of 166 patients (172 cases) of resistant tennis elbow treated by radial nerve denervation/decompression, scored by Roles and Maudsley
- Denervation achieved roughly 90% good-to-excellent results
- Adding direct PIN decompression by resecting the supinator arcade (Group C) did NOT improve outcomes (only 65% good/excellent) and prolonged time off work
The Disputed Entity - Electrodiagnostic Perspective
- Argues the term 'radial tunnel syndrome' is best reserved for truly neurogenic cases with focal PIN motor weakness
- In the painful, weakness-free variant, electrodiagnostic studies are typically normal
- Decompression for forearm pain rests on a flawed analogy to carpal tunnel syndrome and should be assessed in controlled studies
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Differentiating RTS from Lateral Epicondylitis
"A 42-year-old office worker presents with 4 months of lateral elbow pain. She describes the pain as being 'a few centimeters below the bony point' on the outside of the elbow. Pain is worse with typing and turning doorknobs. No history of trauma. She has tried rest and ibuprofen with minimal improvement. How would you assess and manage this patient?"
Scenario 2: PIN Syndrome versus RTS
"A 35-year-old carpenter presents with 6 weeks of progressive difficulty extending his fingers. He reports no pain, but noticed his wrist deviates to the radial side when he extends it. No history of trauma. On examination, he has weak finger and thumb extension but normal wrist extension strength. What is your diagnosis and management?"
Scenario 3: Failed Surgical Decompression
"A 48-year-old patient underwent radial tunnel decompression 4 months ago for chronic lateral forearm pain. Post-operatively, he had mild improvement for 6 weeks but now reports pain has returned to pre-operative levels. He is frustrated and asks what went wrong. How would you manage this patient?"
MCQ Practice Points
Clinical Pearl
Q: What is the key clinical difference between radial tunnel syndrome and posterior interosseous nerve (PIN) syndrome?
A: Radial tunnel syndrome: Pain only, NO motor weakness. PIN syndrome: Motor weakness (finger/thumb extension), NO pain or sensory loss. Both involve PIN compression in the radial tunnel, but radial tunnel syndrome affects sensory afferents in nerve sheath while PIN syndrome causes axonal damage to motor fibers. Treatment also differs: RTS often conservative, PIN syndrome often requires surgery.
Clinical Pearl
Q: What are the five sites of compression in the radial tunnel (FACES mnemonic)?
A: Fibrous bands anterior to radiocapitellar joint, Arcade of Frohse (most common, 70%), C (ECRB medial edge), Exit of PIN from supinator, S (leash of Henry - recurrent radial vessels). The Arcade of Frohse is a fibrous arch at the proximal edge of supinator, present in 30% of people, fibrous in 50% of those. Most surgical releases focus on this structure.
Clinical Pearl
Q: What examination findings help differentiate radial tunnel syndrome from lateral epicondylitis?
A: Both cause lateral forearm pain. Radial tunnel syndrome: Tender 4-5 cm distal to lateral epicondyle (over radial tunnel), pain with resisted middle finger extension (ECRB edge stretches over PIN), pain with resisted supination. Lateral epicondylitis: Tender at lateral epicondyle itself, pain with resisted wrist extension. Can coexist in up to 5% of cases.
Clinical Pearl
Q: What muscles does the posterior interosseous nerve supply?
A: Supinator (first branch), then ECU, EDC, EDM, APL, EPL, EPB, EIP. Notably does NOT supply ECRL or ECRB (these are supplied by radial nerve proper before division). This explains why PIN palsy causes finger and thumb drop but preserved wrist extension (radially deviated due to intact ECRL/ECRB without ECU balance).
Clinical Pearl
Q: What is the role of EMG/NCS in radial tunnel syndrome diagnosis?
A: EMG/NCS are typically NORMAL in radial tunnel syndrome (this is a pain syndrome without denervation). This differentiates from PIN syndrome where EMG shows denervation of PIN-innervated muscles. Diagnosis of radial tunnel syndrome is clinical. Diagnostic injection of local anesthetic into the radial tunnel with pain relief supports diagnosis. MRI may show muscle edema but is often normal.
Guidelines, Registries & Global Practice
Global epidemiology: RTS is rare compared with lateral epicondylitis and has no dedicated implant registry (it is a soft-tissue decompression, not arthroplasty). Reported series are small and retrospective. It is most often seen in adults aged 30-50 in occupations or sports involving repetitive forearm pronation-supination and forceful gripping (manual trades, racquet sports, musicians). Coexisting lateral epicondylitis is reported in a minority of cases and worsens outcomes.
No formal society guidelines exist for RTS specifically; practice is guided by hand-surgery consensus and is broadly consistent worldwide. There is, however, an important difference in emphasis between schools of thought rather than between countries.
How Different Bodies of Practice Approach RTS
| Source / School | Position on RTS | Practical Emphasis |
|---|---|---|
| ASSH / IFSSH (hand surgery consensus) | Accepted as a pain syndrome from PIN compression; clinical diagnosis | Conservative trial first; complete multi-site release if surgery |
| BSSH / BOA (UK hand practice) | Recognised but emphasises excluding lateral epicondylitis and PIN palsy | Diagnostic injection to confirm before considering decompression |
| Electrodiagnostic / neurology view (Rosenbaum) | Term should be reserved for truly neurogenic (weakness) cases | Caution about operating on pain-only presentations |
| Resource-limited settings | Diagnosis remains clinical; advanced imaging/EMG often unavailable | Greater reliance on examination and diagnostic injection response |
Practice variation by resource setting:
- High-resource settings: MRI and ultrasound are used to exclude space-occupying lesions; EMG/NCS routinely performed to exclude PIN syndrome; structured hand therapy available.
- Limited-resource settings: Diagnosis is clinical, anchored on the mobile point of tenderness, the rule of 9s test, and response to a diagnostic local-anaesthetic injection; surgery is reserved for clear failures with a positive injection.
Registry note: Because RTS involves no implant, it is not captured by arthroplasty registries (NJR, AJRR, AOANJRR). Evidence is therefore limited to case series, and outcome reporting commonly uses the Roles and Maudsley grading introduced in the original 1972 description.
RADIAL TUNNEL SYNDROME
Clinical summary
One-Liner
- •Compression of PIN in radial tunnel causing pain WITHOUT weakness (differentiates from PIN syndrome)
- •Controversial, clinically diagnosed entity with normal electrodiagnostics; a key differential for resistant tennis elbow
Key Anatomy
- •Radial tunnel: 4-5cm from radial head to distal supinator
- •Five compression sites (FACES): Fibrous bands, Arcade (70%), ECRB, Exit, Leash
- •PIN innervates: supinator, ECU, EDC, EDM, APL, EPL, EPB, EIP (NOT ECRL/ECRB)
- •Arcade of Frohse: present 30%, fibrous 50% of those
Presentation
- •Aching pain 4-5cm distal to lateral epicondyle (mobile mass)
- •Worse with pronation-supination and gripping
- •NO motor weakness (if weakness = PIN syndrome)
- •NO paresthesias (PIN is purely motor)
Diagnosis
- •Rule of 9s: pain with resisted long finger extension at 9cm distal to epicondyle
- •Mobile mass sign: tenderness moves with pronation/supination
- •EMG/NCS: NORMAL (abnormal = PIN syndrome)
- •Diagnostic injection: pain relief confirms diagnosis
Differential
- •Lateral epicondylitis: pain AT epicondyle (fixed), resisted wrist extension
- •PIN syndrome: motor weakness with abnormal EMG
- •C7 radiculopathy: neck pain, triceps weakness, multiple myotomes on EMG
Management
- •Conservative 3-6 months: splint (supination), NSAIDs, PT, injection
- •Surgery: Thompson approach, release all five sites (FACES)
- •Success: 50-90% (variable), full benefit 3-6 months
- •Complications: PIN injury (1-5%), recurrence (10-30%)
Viva Pearls
- •RTS = pain only; PIN syndrome = weakness; radial nerve palsy = wrist drop
- •Always try conservative 3-6 months first
- •Positive diagnostic injection predicts surgical success
- •Arcade of Frohse is most common site (70%)
What Gets You Failed
- •Not differentiating RTS from PIN syndrome (check motor strength!)
- •Operating without 3-6 month conservative trial
- •Not releasing all five compression sites during surgery
- •Missing coexisting lateral epicondylitis