Clinical diagnosis | Pressure support | Complete release | Regional traps | Wound care
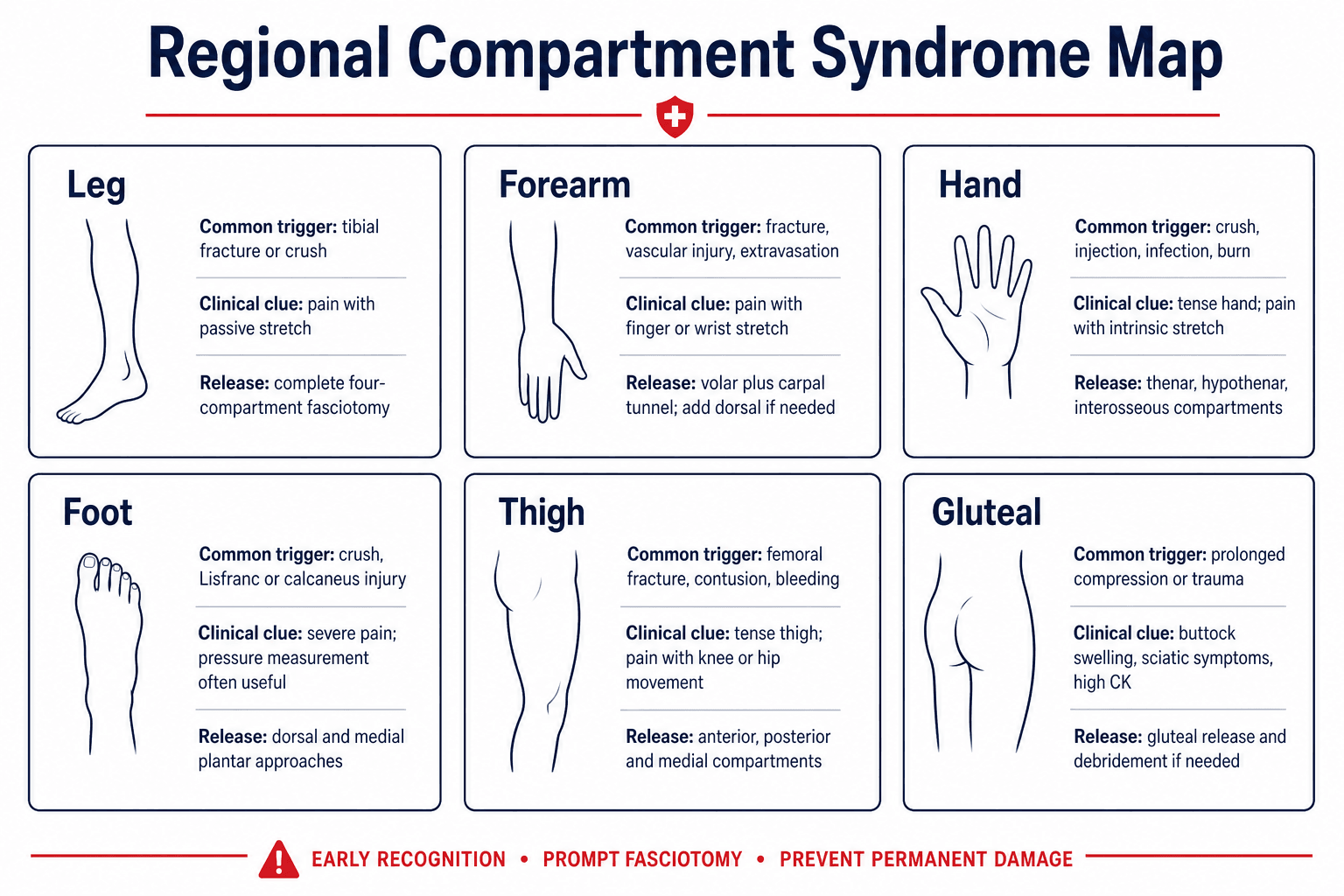
- Compartment syndrome is a regional diagnosis. Each region has different compartments, nerves, passive-stretch manoeuvres and release strategies.
- Pain out of proportion and pain with passive stretch are early clues. Pallor, paralysis and pulselessness are late and unreliable.
- Pressure measurement helps when the examination is unreliable or equivocal. It does not replace urgent fasciotomy when the clinical picture is clear.
- Complete release matters more than the incision count. The failure is leaving an involved compartment closed.
- Reperfusion, crush and vascular repair lower the threshold. The limb can deteriorate after flow returns.
- Post-fasciotomy care is active treatment. Second look, debridement, closure planning, renal monitoring and rehabilitation determine outcome.
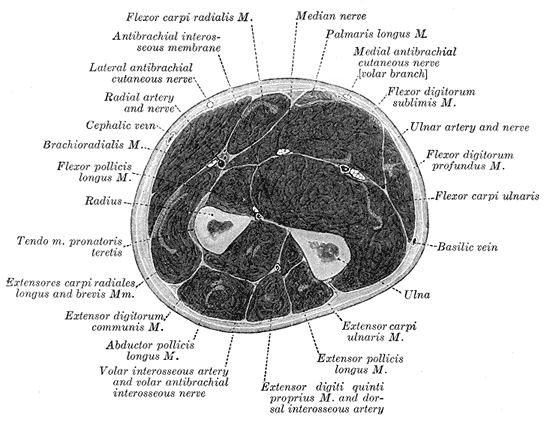
- “Forearm volar fasciotomy usually includes carpal tunnel release because swelling extends distally and median nerve compression can coexist.
- “Foot compartment syndrome is uncommon, but high-energy midfoot and calcaneal trauma can produce severe long-term morbidity if missed.
- “Gluteal compartment syndrome commonly presents with buttock swelling, sciatic symptoms, high creatine kinase and rhabdomyolysis rather than an obvious fracture.
- “A single normal pressure or one-time pressure reading is weak evidence if the patient keeps getting worse.
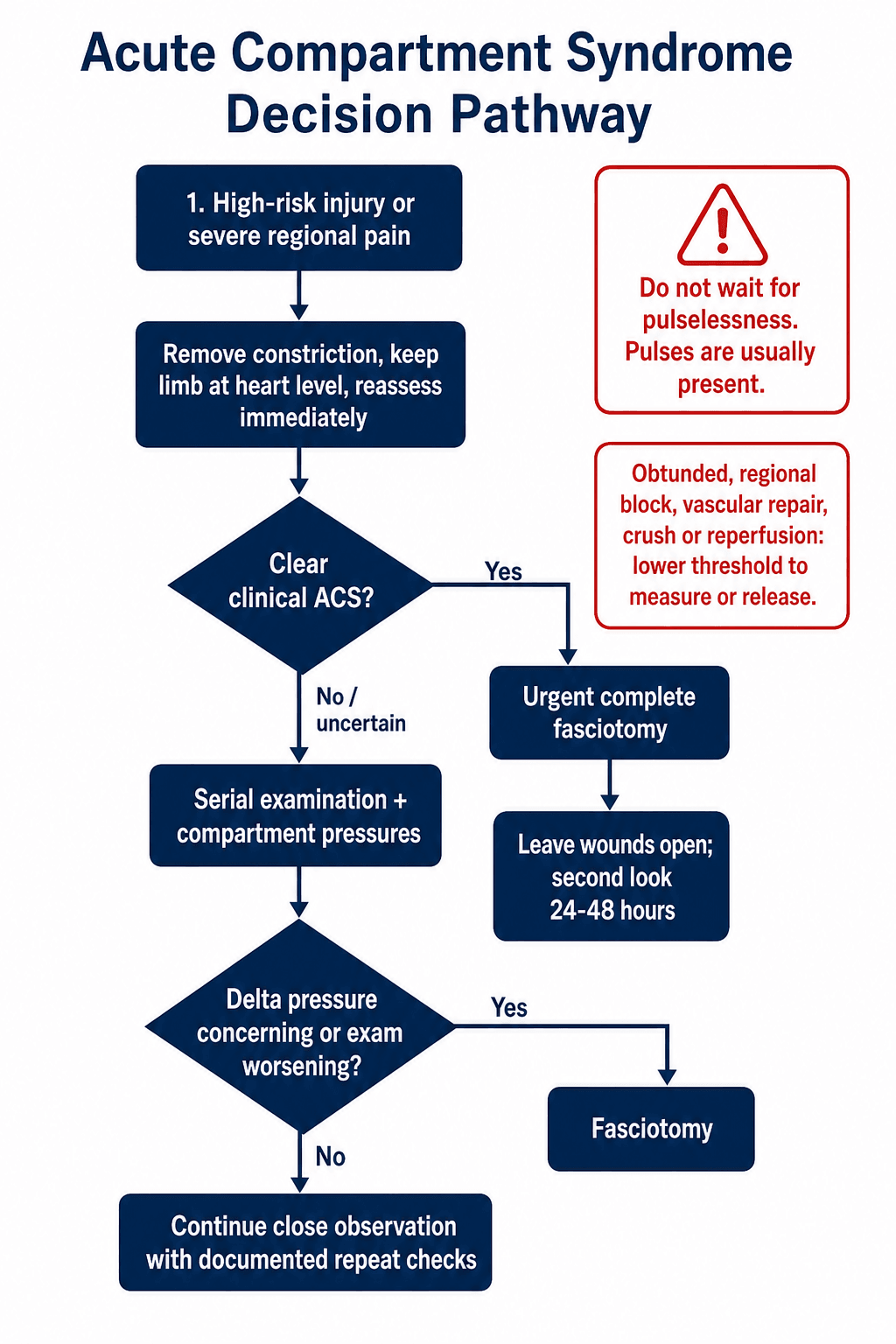
If the patient has a high-risk injury with escalating regional pain, remove constriction, keep the limb at heart level, document the neurovascular examination and call for senior review. Do not wait for pulselessness.
- Common Trigger
- Tibial fracture, crush, reperfusion, vascular repair
- Clinical Clue
- Pain with passive stretch; first web space symptoms may suggest anterior compartment involvement
- Release Principle
- Release anterior, lateral, superficial posterior and deep posterior compartments
- Common Trigger
- Distal radius fracture, both-bone fracture, supracondylar fracture, vascular injury, extravasation
- Clinical Clue
- Pain with passive finger extension or wrist movement; median or ulnar symptoms
- Release Principle
- Volar release plus carpal tunnel; add dorsal and mobile wad release if involved
- Common Trigger
- Crush, injection, infection, burn, prolonged compression
- Clinical Clue
- Tense intrinsic compartments, pain with intrinsic stretch, swelling between metacarpals
- Release Principle
- Thenar, hypothenar, adductor and interosseous release as required
- Common Trigger
- Crush, calcaneus fracture, Lisfranc or Chopart injury
- Clinical Clue
- Severe foot pain, tense plantar swelling, less reliable passive stretch signs
- Release Principle
- Pressure measurement often useful; dorsal and medial plantar approaches when indicated
- Common Trigger
- Femoral fracture, blunt contusion, haematoma, anticoagulation, vascular injury
- Clinical Clue
- Tense thigh, pain with knee or hip movement, femoral or sciatic symptoms
- Release Principle
- Release anterior, posterior and medial compartments if involved
- Common Trigger
- Prolonged immobilisation, substance-related compression, trauma, vascular surgery, obesity
- Clinical Clue
- Buttock swelling, severe pain, sciatic neuropathy, high CK
- Release Principle
- Urgent gluteal release, debridement, renal and rhabdomyolysis care
PAINRecognition | MAPPressure Logic | OPENOperative Rule |
|---|---|---|
P Passive stretch Pain with stretching the involved muscles is a key early clue. | M Measure if uncertain Equivocal, obtunded, regional block or sedated patient. | O Open complete compartments The named involved compartments must be decompressed fully. |
A Analgesia escalation Increasing opioid need after fracture, casting or fixation is suspicious. | A Assess trend Serial examination matters more than one isolated reading. | P Protect nerves Median, ulnar, peroneal, tibial and sciatic nerves define regional risk. |
I Injury pattern Tibial fracture, forearm fracture, crush, vascular repair and compression raise risk. | P Perfusion pressure Delta pressure is diastolic pressure minus compartment pressure. | E Evaluate muscle Colour, contractility, consistency and capacity to bleed guide debridement. |
N Nerves Paresthesia and weakness indicate threatened nerve perfusion. | N Never close under tension Leave fasciotomy wounds open and plan staged closure. | |
Pain is the early warning. | Measure when the examination cannot answer the question. | Open everything that is threatened. |
Overview and Epidemiology
Acute compartment syndrome is a time-critical failure of tissue perfusion inside a closed fascial space. The diagnosis is usually clinical, but the practical problem is regional. A leg, forearm, hand, foot, thigh and buttock do not fail in the same way, and they are not decompressed in the same way.
The common teaching phrase is "pain out of proportion". That is useful, but incomplete. A treating surgeon also needs to know which compartment is at risk, which nerve is threatened, which passive movement stretches the involved muscles, when pressure measurement adds value, and whether the planned fasciotomy actually releases the threatened compartment.
High-risk settings include:
- tibial shaft, tibial plateau, distal tibia and high-energy ankle trauma
- forearm fractures, paediatric supracondylar fracture, floating elbow and vascular injury
- hand crush, injection, burn, infection or prolonged compression
- calcaneus fracture, Lisfranc injury, Chopart injury and foot crush
- femoral fracture, thigh contusion, anticoagulation-related bleeding and vascular injury
- gluteal compression after loss of consciousness, prolonged surgery, trauma or vascular procedures
A generic fasciotomy answer can still fail the patient if the wrong compartment is left closed. The deep posterior leg compartment, carpal tunnel, intrinsic hand compartments, calcaneal foot compartment and gluteal compartments are common places where incomplete thinking leads to poor outcome.
Anatomy and Pathophysiology by Region
The underlying pathophysiology is the same in every region: swelling, bleeding, external compression or reperfusion raises compartment pressure, venous outflow fails first, capillary perfusion falls, tissue oedema increases, and muscle and nerve ischaemia accelerates. The regional anatomy determines what fails first and how it must be released.
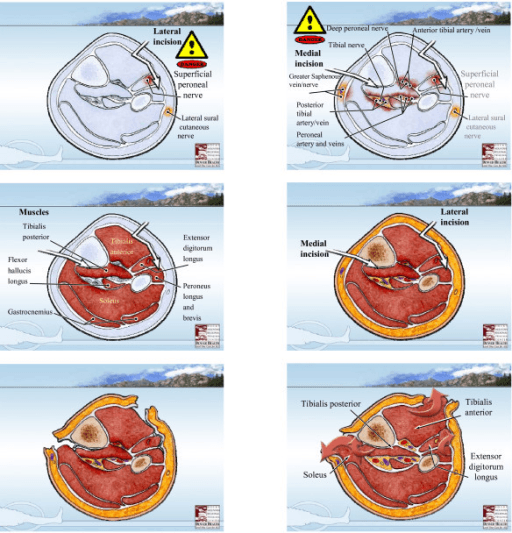
The leg has four clinically important compartments:
- Anterior: tibialis anterior, extensor hallucis longus, extensor digitorum longus, deep peroneal nerve and anterior tibial vessels.
- Lateral: peroneus longus and brevis with the superficial peroneal nerve.
- Superficial posterior: gastrocnemius, soleus and plantaris.
- Deep posterior: tibialis posterior, flexor hallucis longus, flexor digitorum longus, tibial nerve and posterior tibial vessels.
Anterior compartment syndrome may produce first web space paraesthesia and pain with passive plantarflexion of the ankle or toes. Posterior compartment involvement may produce pain with passive dorsiflexion and tibial nerve symptoms. The deep posterior compartment is a classic missed release.
Classification Systems and Regional Patterns
Classification in compartment syndrome is less about named eponyms and more about risk stratification. The useful classifications are clinical:
- Features
- High-risk mechanism, escalating pain, pain with passive stretch, tense compartment, evolving nerve symptoms
- Action
- Proceed to urgent fasciotomy without delaying for pressure measurement
- Features
- Pain or swelling present but examination inconsistent or early
- Action
- Serial examination plus pressure measurement; escalate if trend worsens
- Features
- Obtunded, sedated, intoxicated, paediatric distress, regional anaesthesia, ventilated patient
- Action
- Lower threshold for pressure monitoring or fasciotomy depending mechanism
- Features
- Vascular repair, prolonged ischaemia, crush, high CK, major swelling
- Action
- Low threshold for prophylactic or therapeutic fasciotomy and metabolic monitoring
Everything above is acute compartment syndrome (a surgical emergency); its examinable counterpart is chronic exertional compartment syndrome (CECS) - a reversible, exercise-induced rise in compartment pressure, classically the anterior or deep posterior leg in young runners and military trainees. The story is the opposite of ACS: cramping, aching or tightness that comes on at a predictable point in exercise, sometimes with transient foot drop or paraesthesia, and resolves within minutes of stopping - the patient is normal at rest. Diagnosis is by dynamic intracompartmental pressure testing using the Pedowitz criteria (resting pressure 15 mmHg or more, 1-minute post-exercise 30 mmHg or more, or 5-minute post-exercise 20 mmHg or more). The key differentials are medial tibial stress syndrome, a tibial stress fracture, and popliteal artery entrapment for exertional calf symptoms. Management is activity modification, gait retraining and relative rest first, then elective fasciotomy for refractory cases - never the emergency two-incision release of ACS. Confusing the two is a classic trap.
Clinical Assessment
The examination is structured, repeated and documented. The question is not "does the patient have all six Ps?" The question is "is this region behaving like a threatened closed compartment?"
- Injury time, mechanism and energy
- Fracture, dislocation, crush, burn, injection, extravasation or vascular injury
- Pain trajectory and analgesia escalation
- Cast, splint, dressing, tourniquet or positioning history
- Anticoagulation, bleeding disorder or reperfusion risk
- Time since vascular repair or reduction
- Inspect swelling, skin tension, blisters and wounds
- Palpate the specific region, but do not rely on palpation alone
- Test passive stretch of the muscles in the suspected compartment
- Document sensory and motor function by nerve distribution
- Check pulses and Doppler, but remember pulses can remain present
- Repeat the examination with times recorded
- Passive Stretch or Nerve Clue
- Pain with passive plantarflexion of ankle or toes; first web space paraesthesia
- Do Not Miss
- Deep peroneal nerve symptoms may be early
- Passive Stretch or Nerve Clue
- Pain with passive dorsiflexion; tibial nerve symptoms
- Do Not Miss
- Deep posterior compartment can be incompletely released
- Passive Stretch or Nerve Clue
- Pain with passive finger extension; median, ulnar or AIN symptoms
- Do Not Miss
- Carpal tunnel compression may coexist
- Passive Stretch or Nerve Clue
- Tense intrinsic spaces, pain between metacarpals, painful intrinsic stretch
- Do Not Miss
- Normal pulses do not reassure in intrinsic compartment disease
- Passive Stretch or Nerve Clue
- Severe pain and plantar swelling; toe motion pain may be subtle
- Do Not Miss
- Clinical signs are less reliable; pressure measurement often helps
- Passive Stretch or Nerve Clue
- Buttock swelling, sciatic pain or weakness, high CK
- Do Not Miss
- Can present as rhabdomyolysis or sciatic neuropathy rather than fracture pain
The differential matters because several conditions mimic compartment syndrome, and missing the real diagnosis in either direction is dangerous: an unnecessary fasciotomy is a large open wound, while a missed compartment syndrome costs the limb.
- Discriminating Features
- Pain out of proportion, pain with passive stretch, tense compartment, escalating analgesia, rising delta pressure
- Why It Is Confused with ACS
- The reference diagnosis; treat when the picture fits
- Discriminating Features
- Absent pulses, cool pale limb, abnormal ankle-brachial index, hard signs of vascular injury
- Why It Is Confused with ACS
- Both cause severe pain; but ACS usually has present pulses and arterial injury can also trigger reperfusion ACS
- Discriminating Features
- Diffuse swelling, calf tenderness, risk factors, raised D-dimer, confirmatory ultrasound
- Why It Is Confused with ACS
- Painful swollen calf, but no pain with passive stretch and no compartment tension
- Discriminating Features
- Fever, erythema, systemic sepsis, crepitus or skin changes, raised inflammatory markers
- Why It Is Confused with ACS
- Necrotising fasciitis is also a surgical emergency and may coexist
- Discriminating Features
- Pain proportionate to injury, settles with analgesia, no passive-stretch pain
- Why It Is Confused with ACS
- Postoperative or fracture pain can mask early ACS; the trend is the key
- Discriminating Features
- Sensory or motor deficit without compartment tension or escalating pain
- Why It Is Confused with ACS
- Overlapping neurological signs, but no rising pressure or stretch pain
Investigations and Pressure Measurement
Compartment syndrome is not diagnosed by X-ray, CT or MRI. Imaging is used to define fractures, dislocations and vascular injury, but it should not delay decompression when clinical ACS is clear.
Pressure measurement is most useful when:
- the patient is obtunded, ventilated, intoxicated, sedated or unreliable
- pain assessment is difficult because of paediatric age, communication problems or regional anaesthesia
- the examination is equivocal but the injury is high risk
- there is vascular repair, reperfusion, crush injury or prolonged compression
- small compartments of the foot or hand are suspected and clinical signs are subtle
Commonly used thresholds include:
- How to Interpret
- A high pressure is concerning, but the exact critical number is imperfect
- Clinical Meaning
- Use with clinical picture and blood pressure
- How to Interpret
- Diastolic blood pressure minus compartment pressure
- Clinical Meaning
- A delta pressure around 30 mmHg or lower is commonly used as a fasciotomy threshold
- How to Interpret
- Worsening pain, rising pressure, falling delta pressure or new nerve signs
- Clinical Meaning
- More important than a single isolated reading
- How to Interpret
- Can create false positives or false reassurance
- Clinical Meaning
- Do not let one number overrule a deteriorating patient
The most dangerous use of pressure monitoring is to create false reassurance. If the examination is worsening, the limb is high risk and the clinical story fits, treat the patient rather than the number.
Management Algorithm
- Assess the patient and mechanism.
- Remove splints, casts, circumferential dressings and constriction.
- Keep the limb at heart level.
- Give analgesia, but do not let pain relief hide serial deterioration.
- Document regional examination: swelling, passive stretch, sensory, motor, pulses, Doppler.
- Reduce dislocations and stabilise grossly unstable fractures when needed.
- If clear ACS is present, proceed to urgent fasciotomy.
- If uncertain, measure pressures and repeat the examination frequently.
Surgical Technique and Regional Fasciotomy Principles
The operative principle is simple: release every involved compartment completely, assess muscle viability and leave the wounds open. The technique varies by region.
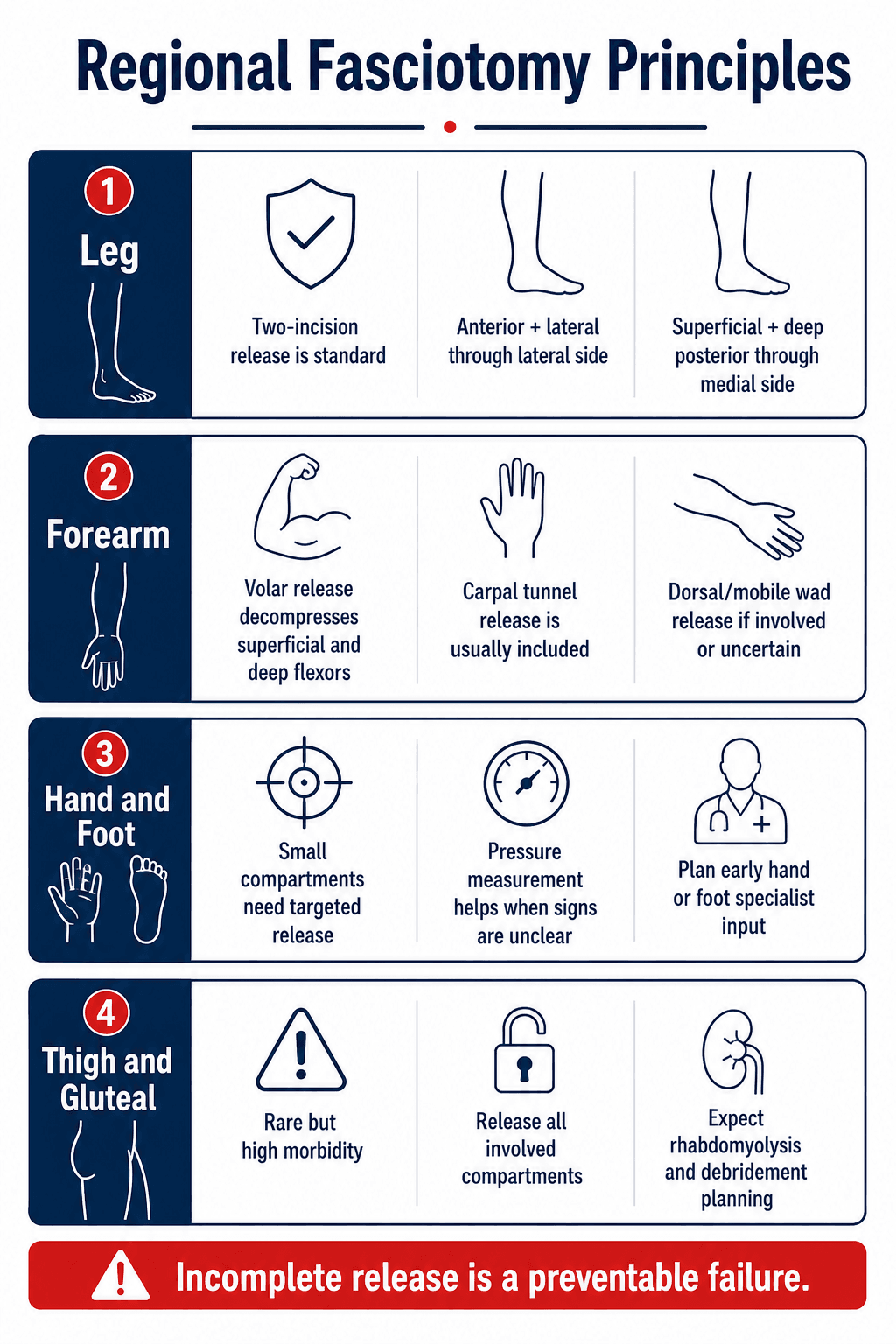
Standard teaching is two-incision four-compartment fasciotomy:
- lateral incision releases anterior and lateral compartments
- medial incision releases superficial and deep posterior compartments
- identify and protect superficial peroneal nerve laterally
- avoid missing deep posterior fascia medially
- extend releases enough to decompress the full compartment length
Complications
The worst complication is missed or incomplete decompression. After that, morbidity comes from muscle necrosis, nerve injury, wound problems and systemic effects.
- Complication
- Persistent compartment syndrome after incomplete release
- Practical Meaning
- Recurrent pain, rising pressure or CK after fasciotomy needs urgent reassessment
- Complication
- Rhabdomyolysis, hyperkalaemia, renal injury
- Practical Meaning
- Especially thigh, gluteal, crush and reperfusion injuries
- Complication
- Wound infection, skin necrosis, bleeding
- Practical Meaning
- Fasciotomy wounds are open injuries requiring active wound planning
- Complication
- Nerve deficit, stiffness, contracture
- Practical Meaning
- Hand, forearm and foot morbidity can be function-limiting even with limb survival
- Complication
- Volkmann contracture, claw toes, chronic pain, amputation
- Practical Meaning
- Usually reflects delayed diagnosis, severe injury or incomplete release
Compartment syndrome compromises microvascular perfusion before major arterial inflow is lost. A warm foot or palpable pulse can coexist with threatened muscle and nerve.
The chronic sequela of a missed or incompletely released forearm ACS is Volkmann ischaemic contracture - ischaemic necrosis and fibrosis of the deep flexor mass (FDP and FPL first, as they lie deepest and furthest from inflow) producing the classic flexed, pronated claw hand that worsens on wrist extension (a positive wrist-extension/Volkmann test). It is graded by the Tsuge classification: mild (a few digits, little or no sensory loss), moderate (all fingers and thumb, with intrinsic and sensory involvement), and severe (all flexors and extensors, fixed deformity, severe sensory and intrinsic loss). Reconstruction is staged by severity: splinting and dynamic therapy with excision of the fibrotic infarct, flexor slide or tendon lengthening for mild-to-moderate disease, and tendon transfers, neurolysis or free functioning muscle transfer (e.g. gracilis) for severe established contracture. The exam point is that it is preventable - it represents a failure to recognise and completely decompress acute forearm compartment syndrome (including the carpal tunnel) in time.
Postoperative Care and Rehabilitation
Fasciotomy is the start of treatment, not the end. After release, the goals are to confirm decompression, prevent systemic complications, keep viable tissue alive and close the wound safely.
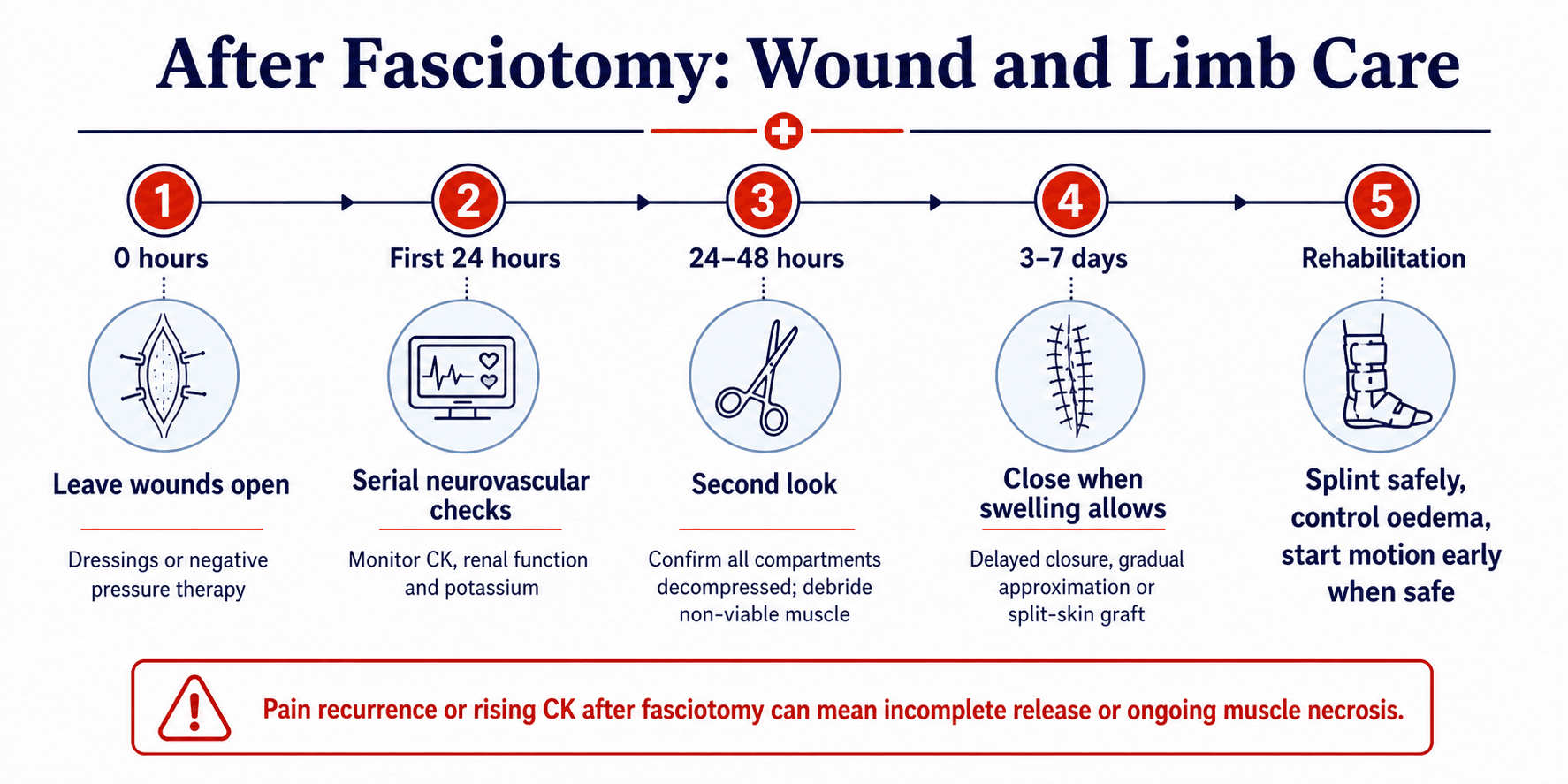
Immediate care includes:
- leave fasciotomy wounds open
- use non-adherent dressings or negative pressure therapy according to local practice
- repeat neurovascular and compartment examination
- monitor CK, potassium, creatinine, urine output and acidosis in large muscle injuries
- return to theatre around 24 to 48 hours for second look when indicated
- debride clearly non-viable muscle
- close only when swelling allows, using delayed primary closure, gradual approximation or split-skin grafting
- splint safely and involve therapy early, especially for hand and forearm
Outcomes and Prognosis
Outcome depends on time to diagnosis, mechanism, region, completeness of release, muscle viability, nerve injury and wound management. Limb survival is not the same as functional recovery.
Better outcomes are associated with:
- early recognition and decompression
- reliable serial examinations in high-risk patients
- complete release of all involved compartments
- coordinated vascular and orthopaedic management in reperfusion injuries
- early second look and debridement when muscle viability is uncertain
- early oedema control and rehabilitation
Poor prognostic patterns include:
- delayed presentation with neurological deficit
- thigh or gluteal syndrome with very high CK and renal injury
- compartment syndrome after prolonged compression or substance-related immobilisation
- missed foot or hand syndrome leading to chronic pain, stiffness and deformity
- incomplete fasciotomy requiring delayed revision
Controversies and Areas of Uncertainty
Several questions remain genuinely unresolved, and examiners reward candidates who can discuss them without overstating the evidence:
- The exact pressure threshold. Delta pressure under 30 mmHg is the most validated trigger, but the optimal cut-off and duration are debated, and one-time readings overcall the diagnosis. Some advocate continuous monitoring or higher delta thresholds to reduce unnecessary fasciotomy.
- Continuous monitoring versus serial clinical examination. Continuous monitoring helps in unreliable patients but is not universally available and can generate false positives; serial examination remains central where the patient is alert.
- Foot compartment release. The number of foot compartments, whether to decompress, and the surgical approach are all contested; some surgeons favour non-operative management given uncertain functional benefit and high wound morbidity.
- Gluteal compartment syndrome management. Recent evidence suggests neurologically intact patients may be managed medically with close surveillance, whereas those with an established deficit benefit from fasciotomy.
- Emerging diagnostics. Near-infrared spectroscopy, biomarkers and ultrasound elastography are investigational and not yet a substitute for clinical judgement and pressure measurement.
Guidelines, Registries & Global Practice
Acute compartment syndrome is a worldwide emergency, and the core principles are consistent across examination systems: early senior review, repeat documented examination, rapid theatre access, multidisciplinary coordination with vascular, plastic, hand and foot-and-ankle and critical-care teams, and local antimicrobial and perioperative protocols for open wounds. Reported incidence is heavily skewed toward young men with tibial diaphyseal fractures (around 2 to 3 percent of tibial shaft fractures, much higher in high-energy or multiply-injured patients).
- Diagnostic Emphasis
- Serial clinical examination is primary; continuous pressure monitoring for unreliable or obtunded patients
- Decompression Trigger
- Clear clinical ACS or sustained delta pressure under 30 mmHg
- Diagnostic Emphasis
- Documented serial neurovascular checks; escalating analgesia is a red flag; theatre within target timeframe
- Decompression Trigger
- Clinical diagnosis prompts immediate fasciotomy; do not await all six Ps
- Diagnostic Emphasis
- Combine clinical signs with intracompartmental pressure when examination is unreliable
- Decompression Trigger
- Delta pressure under 30 mmHg or convincing clinical picture
- Diagnostic Emphasis
- Highlights limited evidence base; favours serial assessment plus monitoring in high-risk groups
- Decompression Trigger
- Low threshold for fasciotomy in reperfusion, crush and sedated patients
There is no dedicated international registry for acute compartment syndrome; trauma registries (for example TARN in the UK and the German DGU TraumaRegister) capture it as a complication of fractures and crush injury rather than as a standalone dataset. The validated postfasciotomy classification (Bouklouch and Duckworth) is an emerging tool for standardised outcome reporting and audit.
High- versus limited-resource practice variation: where continuous pressure monitoring and rapid theatre access are available, equivocal cases can be monitored safely; where they are not, the threshold for clinical fasciotomy is appropriately lower, and delayed presentation after prolonged transport or compression is more common. The principle of releasing every threatened compartment completely does not change with resource setting.
Practical documentation should include:
- time of injury and time of first concern
- analgesia escalation and serial examination findings
- passive-stretch findings by region
- sensory and motor status by nerve distribution
- pressure readings if measured, with blood pressure and time recorded
- timing of fasciotomy, compartments released and muscle viability
- plan for second look, renal monitoring, closure and rehabilitation
Compartment syndrome is dynamic. A single note saying "neurovascularly intact" is weak documentation. Timed repeat findings are safer for the patient and clearer for the treating team.
MCQ Practice Points
Q: Do palpable pulses exclude compartment syndrome? A: No. Pulses are often present because the problem is microvascular perfusion inside the compartment, not necessarily large-vessel occlusion.
Q: What pressure finding commonly supports fasciotomy? A: A delta pressure around 30 mmHg or lower supports fasciotomy, but clear clinical compartment syndrome should not wait for measurement.
Q: What is usually included with volar forearm fasciotomy? A: Carpal tunnel release is usually included; dorsal or mobile-wad release is added when those compartments are involved or uncertain.
Q: Why is foot compartment syndrome easy to miss? A: It can follow calcaneus, Lisfranc or crush injury, and clinical signs may be less reliable than in the leg.
Q: What clues suggest gluteal compartment syndrome? A: Prolonged compression, buttock swelling, rhabdomyolysis and sciatic neuropathy. It may not present with an obvious fracture.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 26-year-old man is six hours after tibial nailing. He has increasing analgesic requirement, severe pain with passive toe movement and first web space paraesthesia. Pulses are present.”
“A 68-year-old anticoagulated patient has a displaced distal radius fracture reduced in a tight splint. Pain worsens despite opioids. Passive finger extension is very painful.”
“A 42-year-old man is found after prolonged immobilisation. He has buttock swelling, sciatic distribution paraesthesia, creatine kinase over 50,000 and rising creatinine.”
Recognise
- High-risk injury plus escalating regional pain.
- Pain with passive stretch of the involved muscles.
- Paresthesia or motor change is a danger sign.
- Pulses are often present.
- Remove constriction and reassess immediately.
Measure
- Measure when the examination is equivocal or unreliable.
- Use delta pressure with the clinical picture.
- One-time readings can mislead.
- Obtunded, sedated, regional anaesthesia and vascular repair lower the threshold.
- Trend matters more than a single number.
Release
- Release every involved compartment completely.
- Leg: anterior, lateral, superficial posterior and deep posterior.
- Forearm: volar plus carpal tunnel; add dorsal or mobile wad if involved.
- Hand and foot: targeted small-compartment release.
- Thigh and gluteal: expect large muscle injury and debridement planning.
Aftercare
- Leave wounds open.
- Second look around 24 to 48 hours when indicated.
- Monitor CK, potassium, creatinine and urine output in crush, thigh, gluteal or reperfusion injuries.
- Delayed closure, gradual approximation or split-skin graft when swelling permits.
- Start region-specific rehabilitation early when safe.
Evidence Base
The Diagnosis of Acute Compartment Syndrome: A Review
- Clinical findings alone have poor sensitivity (13 to 64 percent) for acute compartment syndrome compared with continuous intracompartmental pressure monitoring (94 percent).
- A differential (delta) pressure of under 30 mmHg for more than 2 hours is the recommended trigger for decompression.
- Delayed diagnosis is a primary cause of poor outcome, and high-risk patients should undergo pressure monitoring.
Postfasciotomy Classification System for Acute Compartment Syndrome of the Leg
- An international expert panel developed and validated a grading system describing the consequences of leg acute compartment syndrome found at fasciotomy.
- Interrater agreement was strong (Fleiss kappa 0.711) and intrarater consistency was high across 32 clinical cases.
- The system standardises communication about muscle damage severity and the need for further surgery after fasciotomy.