Perfusion | Reduction | ABI/API | CTA | Fixation sequence | Fasciotomy
- Vascular injury is diagnosed by limb behaviour, not by X-ray severity alone. A spontaneously reduced knee dislocation can still have popliteal artery injury.
- Hard signs need urgent vascular control. CTA is for patients stable enough for imaging and where imaging will change management.
- ABI/API is a screening tool, not a replacement for clinical judgement. An abnormal or unreliable result prompts vascular imaging or operative assessment.
- Reduction can be limb-saving. A gross dislocation with threatened perfusion should be reduced urgently, with neurovascular status documented before and after.
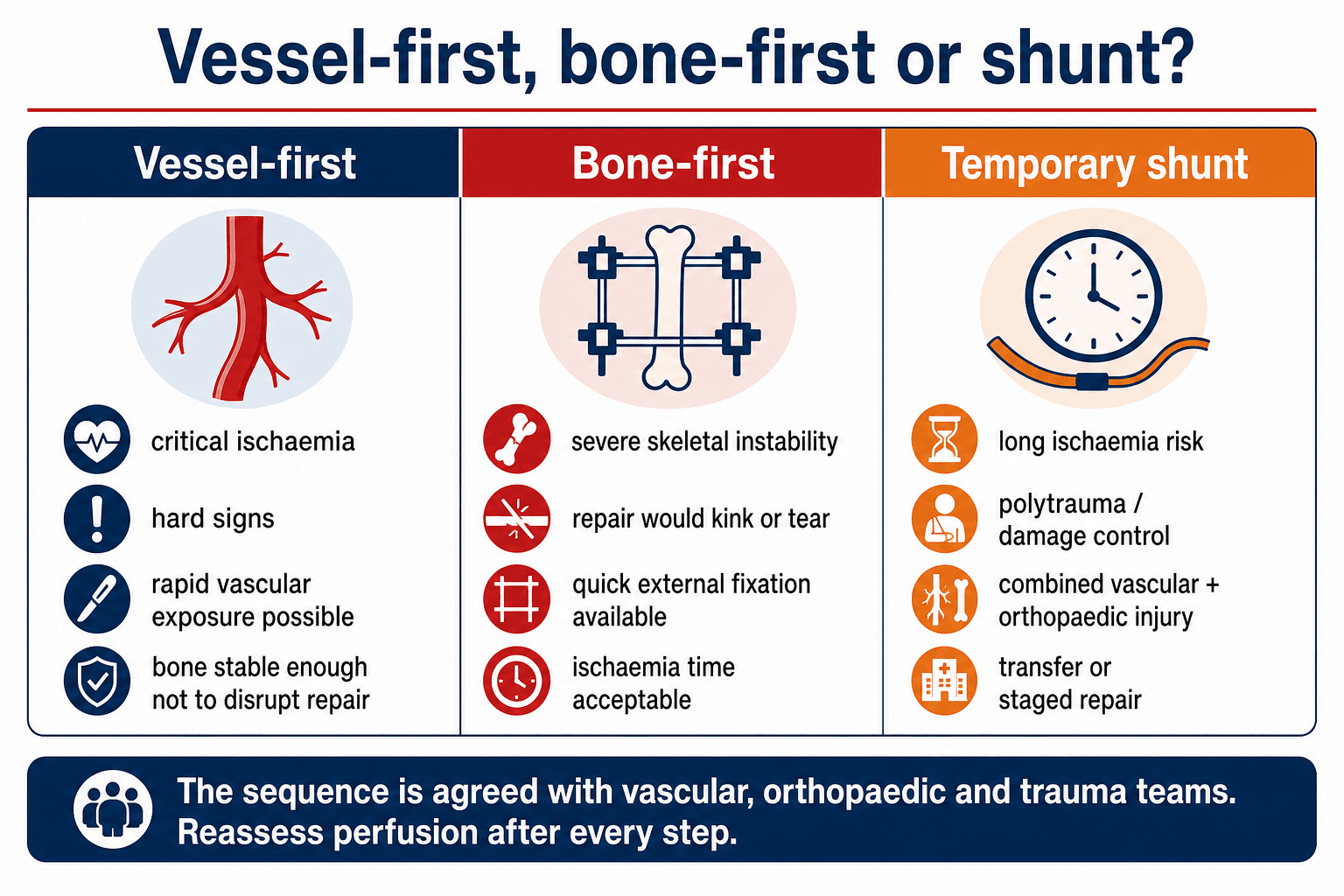
- The orthopaedic sequence protects the vascular repair. Use rapid external fixation, definitive fixation or a temporary shunt depending ischaemia time and skeletal instability.
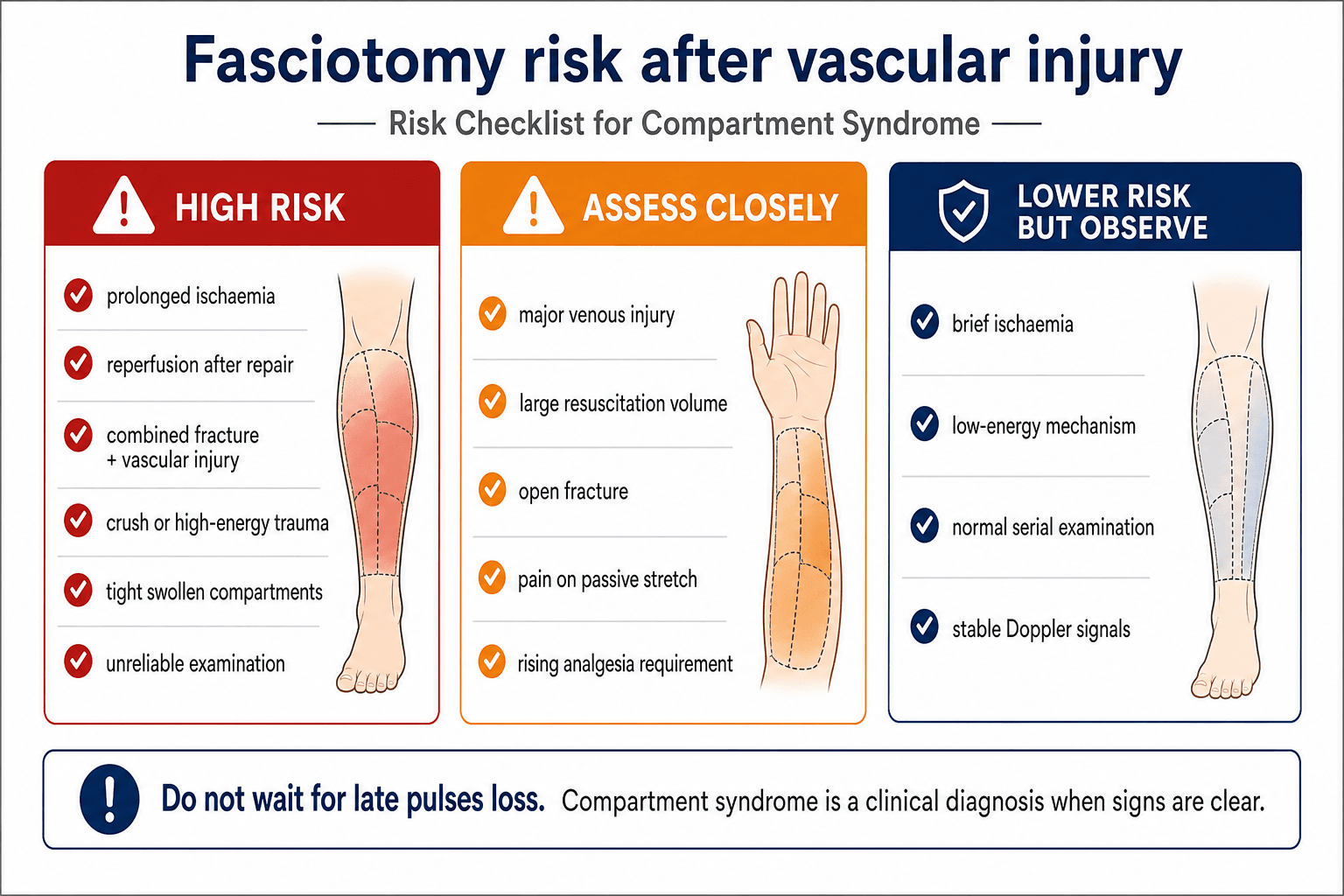
- Fasciotomy risk rises after ischaemia and reperfusion. Do not wait for late pulse loss before treating compartment syndrome.
- “The safe first sentence is: assess the patient, control bleeding, document neurovascular status, reduce gross dislocation if limb threatened, then screen with ABI/API or CTA as appropriate.
- “Normal palpable pulses do not end the assessment when mechanism and examination are concerning.
- “Temporary shunting is not definitive repair; it is damage-control perfusion while the patient, skeleton or transfer pathway is made safe.
- “A technically patent artery does not guarantee limb salvage if muscle, nerve, bone and soft tissue are not viable.
Do not send an ischaemic limb for routine imaging without a vascular plan. If there are hard signs or a cold pulseless limb after reduction, haemorrhage control and revascularisation take priority.
- Finding That Matters
- Shock, uncontrolled haemorrhage, multiple trauma or threatened airway.
- Action
- Primary survey, haemorrhage control and damage-control decision-making.
- Finding That Matters
- Cold, pale, pulseless, painful limb; absent Doppler; motor or sensory deterioration.
- Action
- Urgent vascular involvement and reperfusion pathway.
- Finding That Matters
- Knee, ankle, elbow or shoulder deformity with threatened perfusion.
- Action
- Reduce urgently, document neurovascular status before and after.
- Finding That Matters
- Active bleeding, expanding haematoma, bruit, thrill or absent pulse.
- Action
- Vascular team and theatre; imaging only if it will not delay needed control.
- Finding That Matters
- Soft signs, proximity wound, high-risk fracture pattern or pulse asymmetry.
- Action
- ABI/API, duplex or CTA depending reliability and local pathway.
- Finding That Matters
- Fracture-dislocation that will kink, stretch or disrupt repair.
- Action
- Rapid external fixation, definitive fixation if fast and safe, or temporary shunt.
FLOWInitial Priorities | ABIScreening Logic | SHUNTTemporary Shunt Use |
|---|---|---|
F Find hard signs Bleeding, expanding haematoma, bruit, thrill, absent pulse, ischaemia. | A Above 0.9 Serial examinations if the clinical picture is reliable. | S Severe combined injury Vessel and bone both need urgent attention. |
L Limb reduction Reduce gross dislocation if perfusion is threatened. | B Borderline or abnormal CTA or vascular imaging when stable. | H Haemodynamic damage control Shorten ischaemia while physiology is corrected. |
O Orthopaedic stability Stabilise bone when it protects vascular repair. | I Imaging not for hard signs Do not delay theatre for obvious limb-threatening arterial injury. | U Unstable skeleton Allows skeletal stabilisation before definitive repair. |
W Watch compartments Serial checks after injury, repair and reperfusion. | N Need transfer Restores flow while moving to definitive expertise. | |
T Time critical Use when definitive repair cannot be done immediately. | ||
The limb needs flow before finesse. | ABI/API is a gate, not the whole answer. | A shunt buys perfusion time. |
Overview and Epidemiology
Vascular injury associated with a fracture or dislocation is a limb-threatening trauma problem. The orthopaedic surgeon is often the first clinician to recognise the pattern because the vessel injury is hidden behind a dramatic fracture, a reduced dislocation, or an apparently normal pulse.
The common clinical settings are:
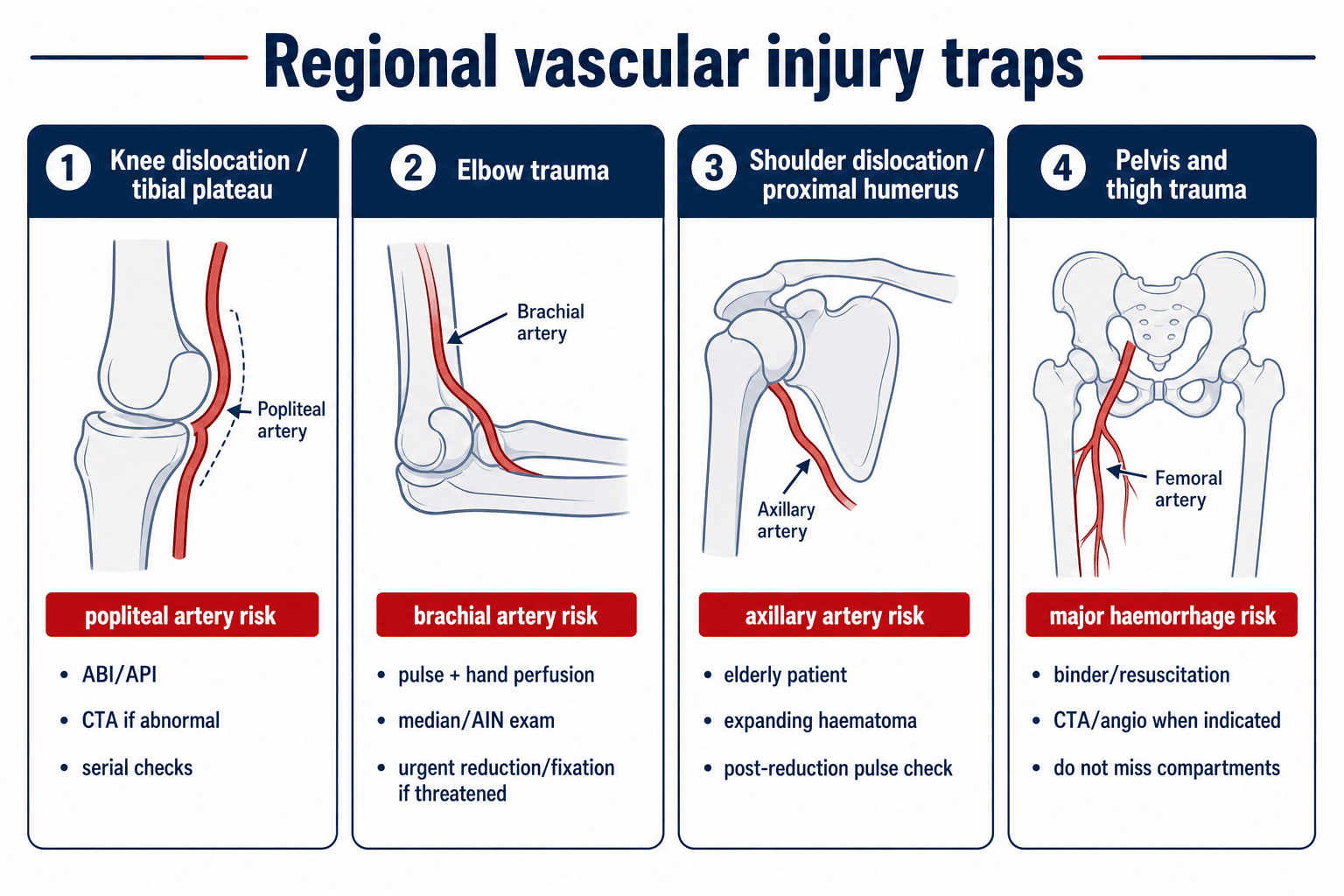
- knee dislocation and high-energy tibial plateau fracture with popliteal artery risk
- elbow fracture-dislocation or paediatric supracondylar fracture with brachial artery risk
- shoulder dislocation or proximal humeral fracture, especially in older patients, with axillary artery risk
- pelvic, acetabular, femoral and tibial trauma with major haemorrhage or limb ischaemia
- open fracture, crush injury, blast injury or ballistic trauma with arterial disruption
- iatrogenic injury during fixation, arthroplasty, deformity correction or revision surgery
Treat vascular injury as a sequence problem: resuscitate, control haemorrhage, restore or preserve perfusion, stabilise the skeleton when it protects the repair, and monitor for reperfusion and compartment complications.
Anatomy and Biomechanics
Why fracture-dislocations injure vessels
Vessels are injured by stretch, compression, transection, intimal disruption, thrombosis, spasm or entrapment. A dislocation can tear the artery during the injury, while a fracture spike can lacerate or tent the vessel. Reduction may restore flow, but it can also reveal an intimal injury that later thromboses.
Tethered vessels are vulnerable
- The popliteal artery is relatively tethered around the adductor hiatus and soleus arch, so knee dislocation and plateau fracture patterns can stretch or disrupt it.
- The brachial artery crosses the elbow anteriorly and is vulnerable in supracondylar fracture, elbow dislocation and distal humerus trauma.
- The axillary artery is at risk in shoulder dislocation, proximal humeral fracture and traction injuries around the shoulder girdle.
- The femoral and iliac vessels are at risk in pelvic, acetabular and proximal femoral trauma, especially when haemorrhage is the dominant problem.
Pulse physiology trap
Palpable pulses may persist because of collateral flow, partial injury, vasospasm resolution, or an intimal flap that has not yet thrombosed. A normal pulse is reassuring only when it fits with a normal examination, normal ABI/API and a low-risk mechanism.
Mechanism of Injury
Mechanism helps determine the probability and type of vascular injury.
- Likely Vessel Problem
- Stretch, intimal tear, thrombosis or complete rupture.
- Orthopaedic Implication
- Reduce urgently if perfusion is threatened; reassess pulse and Doppler after reduction.
- Likely Vessel Problem
- Laceration by spike, segmental vessel injury, crush or thrombosis.
- Orthopaedic Implication
- CTA or direct vascular assessment if abnormal examination or high-risk pattern.
- Likely Vessel Problem
- Transection, partial laceration, contamination and compartment risk.
- Orthopaedic Implication
- Control bleeding, antibiotics, debridement, fixation and vascular plan.
- Likely Vessel Problem
- Vascular disruption plus muscle necrosis and reperfusion injury.
- Orthopaedic Implication
- Low threshold for fasciotomy and metabolic monitoring.
- Likely Vessel Problem
- Axillary artery injury from atherosclerotic or fragile vessel stretch.
- Orthopaedic Implication
- Check pulse before and after reduction; consider CTA with haematoma or pulse change.
- Likely Vessel Problem
- Drill, screw, retractor, saw, osteotome or implant-related injury.
- Orthopaedic Implication
- Recognise immediately; control bleeding; call vascular help early.
Classification Systems
Classify vascular injury in terms that change treatment.
- Examples
- Active arterial bleeding, expanding or pulsatile haematoma, bruit, thrill, absent pulse, distal ischaemia.
- Action
- Urgent vascular control; image only if stable and imaging will not delay needed treatment.
- Examples
- History of bleeding, small stable haematoma, pulse asymmetry, neurological deficit, proximity injury.
- Action
- ABI/API and selective imaging; serial examination.
- Examples
- Warm limb, symmetric pulses, normal Doppler, normal ABI/API and reliable clinical setting.
- Action
- Observation with documented serial checks.
Clinical Presentation
Obvious presentation
The obvious case is a bleeding or pulseless limb after major fracture or dislocation. Features include:
- active external bleeding or rapidly expanding haematoma
- cold, pale or mottled distal limb
- absent or asymmetric pulses
- absent Doppler signal
- severe pain, paraesthesia or motor weakness
- major fracture-dislocation, open wound or crush mechanism
Subtle presentation
The subtle case is the dangerous one. Examples include:
- knee dislocation that has reduced before arrival
- tibial plateau fracture with symmetric pulses but high-risk mechanism
- shoulder dislocation in an older patient with a small pulse difference
- elbow fracture with a pink hand but abnormal Doppler or neurological deficit
- ballistic wound near a major vessel with no hard signs
- delayed thrombosis after an initially normal examination
Delayed presentation
Delayed vascular injury can present with:
- increasing pain or swelling
- pseudoaneurysm
- arteriovenous fistula
- delayed thrombosis
- compartment syndrome
- claudication or reduced exercise tolerance
- wound breakdown or failed fracture healing due to poor perfusion
Physical Examination
Examination must be repeated and timed. Document findings before reduction, after reduction, after splinting or fixation, after vascular repair, and during postoperative observation.
Look
- limb colour, temperature and capillary refill
- deformity or dislocation
- open wound and active bleeding
- expanding haematoma
- skin tension, blistering or threatened skin
- muscle swelling and compartment tension
- signs of polytrauma or shock
Feel
- radial, ulnar, brachial, dorsalis pedis and posterior tibial pulses as relevant
- compare both limbs
- palpate haematoma gently; do not provoke bleeding
- assess temperature gradient from proximal to distal limb
- assess compartment firmness, but do not rely on firmness alone
Move and neurological examination
- document motor function by named nerves
- document sensory territories
- look for deterioration after reduction or revascularisation
- remember that neurological deficit can be vascular, nerve, compartment or fracture-related
Bedside vascular tests
- How To Use It
- Check distal arterial signal and compare sides.
- Interpretation
- Absent or changing signal is concerning even if the limb looks warm.
- How To Use It
- Doppler systolic pressure injured limb divided by uninjured limb or brachial pressure.
- Interpretation
- Above 0.9 with normal examination supports serial observation; 0.9 or less prompts imaging or vascular assessment.
- How To Use It
- Adjunct in fingers or toes when available.
- Interpretation
- A waveform can support perfusion assessment but does not replace Doppler and ABI/API.
- How To Use It
- Pain, passive stretch pain, paraesthesia, analgesia requirement and tense compartments.
- Interpretation
- Treat clinically clear compartment syndrome urgently.
Imaging and Investigations
Plain radiographs
Order the radiographs needed to define and reduce the fracture or dislocation. Do not allow routine imaging to delay reduction of a limb-threatening dislocation.
Radiographs help identify:
- dislocation direction and reduction quality
- fracture-dislocation pattern
- tibial plateau, distal femoral, proximal tibial or elbow injuries that carry vascular risk
- open fracture contamination and bone loss
- fixation strategy if external fixation is needed
CT angiography
CTA is the usual first-line vascular imaging test when imaging is needed and the patient is stable enough. It defines:
- vessel occlusion, transection, active extravasation or pseudoaneurysm
- length and level of arterial injury
- relationship to fracture fragments
- distal runoff
- surgical approach and graft planning
CTA is not a delay tool. It is used when the limb is stable enough for imaging and the result will guide treatment. Hard signs with an obvious operative target can proceed directly to theatre.
Duplex ultrasound
Duplex can be useful for selected stable patients, postoperative surveillance or institutions where rapid expert scanning is available. It is less useful when wounds, dressings, splints, body habitus, pain or time pressure make the study unreliable.
Laboratory tests
Useful tests include:
- full blood count and coagulation profile
- group and crossmatch
- lactate, pH and base deficit in major trauma
- creatine kinase, potassium and renal function when crush, prolonged ischaemia or reperfusion risk exists
- serial haemoglobin when haemorrhage is suspected
Differential Diagnosis
Not every cold or painful limb has the same cause. Differentiate:
- Clue
- Hard signs, abnormal ABI/API, CTA lesion, absent Doppler.
- Management Implication
- Urgent vascular plan.
- Clue
- Often transient, especially in children or after manipulation.
- Management Implication
- Observe only after senior review and reliable perfusion.
- Clue
- Pain on passive stretch, rising analgesia, tense compartments, neurological symptoms.
- Management Implication
- Fasciotomy; pulses may remain present.
- Clue
- Motor or sensory deficit without perfusion abnormality.
- Management Implication
- Document and reassess; explore if associated open injury or transection suspected.
- Clue
- Bilateral cool limbs, systemic hypotension.
- Management Implication
- Resuscitate; still examine the injured limb separately.
- Clue
- Older patient, calcified vessels, baseline pulse difference.
- Management Implication
- Compare sides, use Doppler/CTA, avoid false reassurance.
Management Algorithm
Management is based on physiology, perfusion, fracture stability, time since ischaemia and team availability.
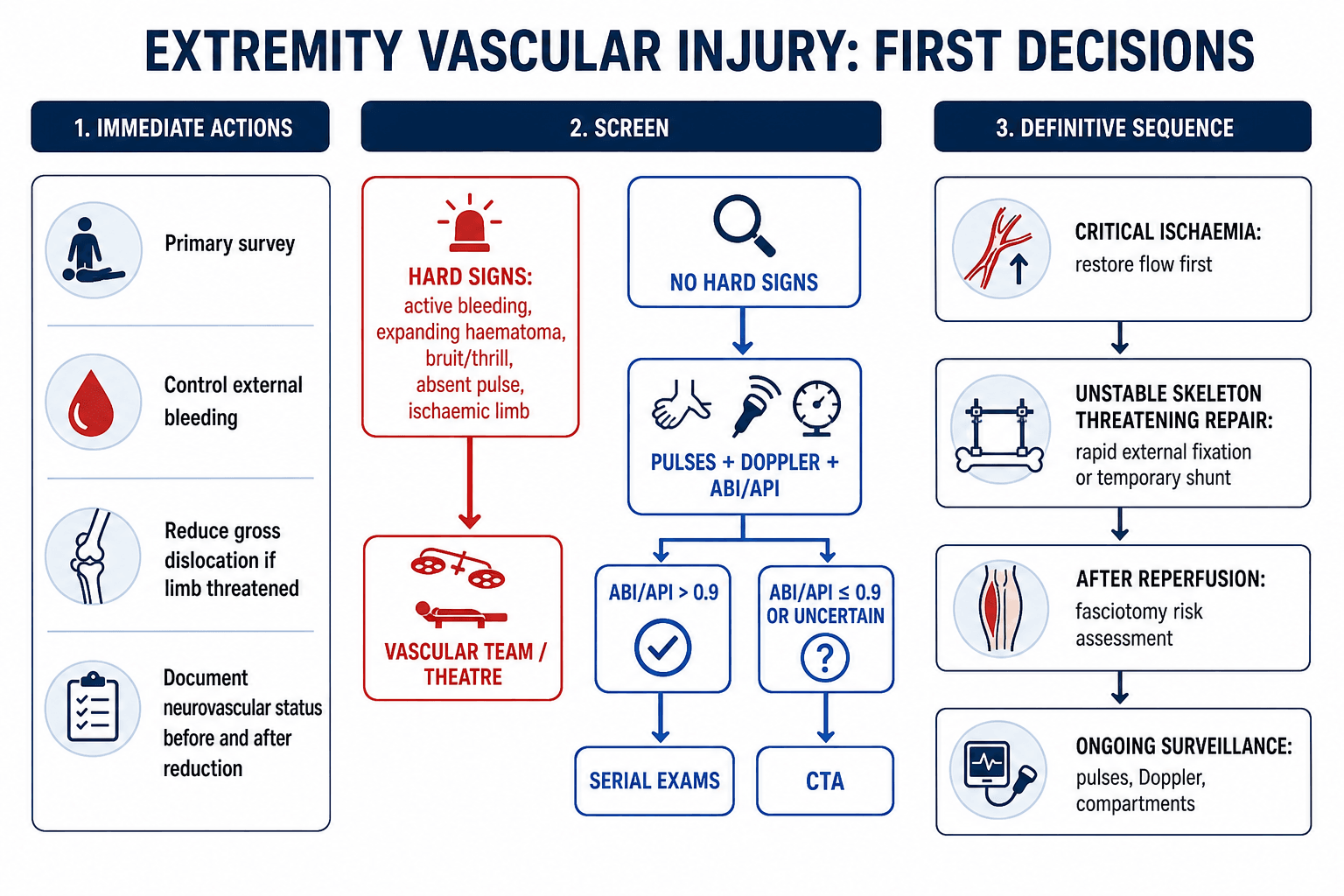
- Primary survey and haemorrhage control.
- Remove constrictive dressings or splints if compromising perfusion.
- Document neurovascular status.
- Reduce gross dislocation if the limb is threatened.
- Reassess and document neurovascular status.
- Identify hard signs.
- If hard signs are present, involve vascular surgery and proceed to control or repair.
- If no hard signs, use ABI/API and CTA pathway when indicated.
- Choose vessel-first, bone-first or temporary shunt sequence.
- Assess fasciotomy need after ischaemia, repair, shunting or reperfusion.
Surgical Technique
Principles:
- reduce dislocations urgently when perfusion is threatened
- splint in a stable position that does not compromise flow
- use external fixation when skeletal instability risks vascular repair or soft tissues
- keep fixation rapid and outside planned vascular or soft-tissue incisions where possible
- reassess Doppler and compartments after fixation
The artery gets the attention, but the concomitant major venous injury is a genuine decision point and a frequent omission:
- Why the vein matters: a divided major outflow vein (popliteal, femoral) causes venous hypertension and limb oedema, which worsens compartment syndrome and can compromise the arterial repair (poor outflow promotes arterial thrombosis).
- Repair when feasible: in the stable patient with a salvageable limb, repair a major vein (lateral suture or interposition graft) - it reduces oedema/compartment risk and supports arterial patency, particularly for the popliteal vein.
- Ligation is acceptable as damage control: in the unstable/polytrauma patient or a difficult exposure, ligating even a major vein is a legitimate life-saving shortcut - but expect marked limb swelling, so it mandates fasciotomy and leg elevation/compression afterwards. Small/expendable veins are simply ligated.
- Sequence note: when both are injured, many restore arterial inflow first (shunt or repair) to limit ischaemia, then address the vein.
Exam point: assess and address the vein as well as the artery - repair a major vein in the stable salvageable limb (less oedema, protects the arterial repair), but ligation is acceptable damage control provided you then perform a fasciotomy for the swelling it causes.
Regional Injury Patterns
- Vessel Concern
- Popliteal artery intimal tear, thrombosis or rupture.
- Practical Checks
- Reduce, document pulse/Doppler before and after, ABI/API, CTA when abnormal or uncertain.
- Vessel Concern
- Knee-dislocation equivalent mechanism can injure popliteal vessels.
- Practical Checks
- ABI/API screening even with symmetric pulses is used in many trauma pathways.
- Vessel Concern
- Brachial artery injury or entrapment.
- Practical Checks
- Check radial/ulnar pulses, hand perfusion, median/AIN function and post-reduction status.
- Vessel Concern
- Axillary artery injury, especially with haematoma or pulse change.
- Practical Checks
- Check pulse before and after reduction; CTA if abnormal or expanding haematoma.
- Vessel Concern
- Major haemorrhage from pelvic vessels more than isolated limb ischaemia.
- Practical Checks
- Binder, resuscitation, pelvic haemorrhage pathway, CTA/angio or packing as indicated.
- Vessel Concern
- Anterior tibial, posterior tibial or peroneal artery injury with compartment risk.
- Practical Checks
- Doppler, ABI/API, CTA if abnormal; low fasciotomy threshold.
Fasciotomy and Reperfusion
Compartment syndrome can occur before repair, after reduction, after vascular repair, after shunting, or during resuscitation. It can occur despite restored pulses.
Do not wait for late findings
Late findings include paralysis, pulselessness and pallor. These should not be used as the trigger for fasciotomy. The important early pattern is escalating pain, pain on passive stretch, increasing analgesic requirement, paraesthesia and tense compartments.
Prophylactic fasciotomy
Prophylactic fasciotomy is considered when the risk of missing compartment syndrome is higher than the morbidity of fasciotomy. This is common after prolonged ischaemia, reperfusion, combined fracture and vascular injury, crush injury or unreliable examination.
Documentation
Document:
- time of injury and estimated ischaemia duration
- time of reduction, shunt and repair
- pulse, Doppler and ABI/API findings
- compartment findings and analgesic requirement
- reason for fasciotomy or reason for observation
Restoring flow to a long-ischaemic limb is not purely good news - the systemic reperfusion load can be lethal, and recognising this changes both monitoring and the salvage decision:
- The warm-ischaemia clock: skeletal muscle tolerates roughly six hours of warm ischaemia before irreversible necrosis; beyond this, reperfusion washes the products of dead muscle into the circulation.
- The reperfusion syndrome (historically "myonephropathic-metabolic syndrome"): sudden release of potassium, myoglobin, hydrogen ions and lactate causes hyperkalaemia (arrhythmia/arrest), myoglobinuric acute kidney injury and metabolic acidosis - a physiological hit that can occur the moment the clamp/shunt is released.
- Management: anticipate it - aggressive IV fluids, monitor and treat hyperkalaemia, monitor creatine kinase and renal function, maintain a brisk urine output (with consideration of urinary alkalinisation), correct acidosis, and fasciotomy to relieve the muscle oedema; warn anaesthesia before reperfusion.
- The "life over limb" decision: reperfusing an unsalvageable, necrotic limb can kill the patient - in the moribund or severely physiologically deranged patient with a clearly non-viable limb (prolonged ischaemia, dead muscle), primary amputation is the safer choice than revascularisation. The whole-patient physiology, not just the artery, drives the decision.
Exam point: reperfusion after prolonged ischaemia causes hyperkalaemia, myoglobinuric AKI and acidosis - pre-empt it with fluids/electrolyte management and fasciotomy, and remember that reperfusing a dead limb can be fatal, so primary amputation may be the life-saving choice.
Complications
- Why It Occurs
- Normal pulses, spontaneous reduction, incomplete examination.
- Prevention or Response
- Repeat examination, ABI/API, CTA when abnormal or uncertain.
- Why It Occurs
- Intimal injury, poor runoff, kinking, compression by fracture or swelling.
- Prevention or Response
- Protect repair with alignment, monitor Doppler, urgent vascular reassessment if signal changes.
- Why It Occurs
- Ischaemia, reperfusion, crush, fracture bleeding and resuscitation swelling.
- Prevention or Response
- Early fasciotomy when clinical or high risk.
- Why It Occurs
- Open fracture, contamination, devitalised tissue.
- Prevention or Response
- Debridement, soft tissue cover, antibiotics and avoid synthetic graft when possible.
- Why It Occurs
- Muscle necrosis, infection, severe bone/soft tissue loss or failed repair.
- Prevention or Response
- Realistic counselling and serial viability assessment.
- Why It Occurs
- Nerve injury, compartment syndrome, stiffness, nonunion and scarring.
- Prevention or Response
- Early multidisciplinary rehabilitation and surveillance.
Postoperative Care
Postoperative care is active surveillance, not routine observation.
Monitoring
- hourly or protocol-based neurovascular checks initially
- Doppler signal documentation
- compartment examination and analgesic requirement
- wound and fasciotomy dressing checks
- graft or repair surveillance according to vascular plan
- renal and metabolic monitoring after crush or reperfusion
Immobilisation and fixation
- external fixator pin sites must not compromise vascular access or planned flaps
- splints should not compress the repair or compartments
- definitive fixation timing depends on physiology, perfusion, soft tissues and infection risk
- vascular graft location affects surgical approach and reoperation planning
Rehabilitation
Rehabilitation depends on nerve, muscle, bone and soft tissue recovery. A perfused limb may still be weak, painful or functionally limited. Early goals are protection of repair, oedema control, joint motion where safe, wound care and realistic patient counselling.
Outcomes and Prognosis
Outcomes depend less on the vessel alone and more on the whole limb.
Important prognostic factors:
- warm ischaemia time
- blunt versus penetrating mechanism
- popliteal or multi-level tibial vessel injury
- associated fracture-dislocation or open fracture
- nerve injury
- muscle viability
- need for fasciotomy
- infection and soft-tissue cover
- patient physiology and rehabilitation capacity
Successful revascularisation is necessary but not sufficient. Limb salvage still depends on viable muscle, stable bone, durable soft tissue, nerve function and absence of infection.
Guidelines, Registries & Global Practice
Extremity vascular injury complicates roughly 1 to 3 percent of major limb trauma in civilian series, rising sharply in penetrating and military cohorts. The popliteal and superficial femoral arteries dominate lower-limb injury, and the brachial artery dominates the upper limb. Outcomes are driven less by the artery and more by ischaemia time, mechanism (blunt worse than penetrating) and associated musculoskeletal and nerve injury.
Side-by-side guidance
- Core Position
- Hard signs go to operative control; selective imaging otherwise.
- Practical Emphasis
- Physical examination plus ABI for triage; CTA as imaging of choice; tourniquets and shunts as adjuncts.
- Core Position
- Damage-control and restoration of perfusion in the unstable patient.
- Practical Emphasis
- Shunting and external fixation as part of staged limb salvage.
- Core Position
- Skeletal stabilisation must protect the vascular repair.
- Practical Emphasis
- Rapid external fixation before or alongside revascularisation when the skeleton is unstable.
- Core Position
- Combined orthoplastic and vascular care in specialist centres.
- Practical Emphasis
- Early senior decision-making, fix-and-flap planning and timely transfer.
- Core Position
- Time-to-reperfusion is the key modifiable factor.
- Practical Emphasis
- Minimise warm ischaemia; low threshold for fasciotomy after reperfusion.
Registry and large-cohort data (multicentre civilian shunt series and the PROOVIT vascular-injury registry) consistently show that severely injured shunted limbs achieve salvage rates comparable to or better than non-shunted limbs despite greater injury severity, and that blunt mechanism, popliteal location and pulseless presentation predict eventual amputation.
High- versus limited-resource practice
In high-resource trauma networks, definitive CTA, vascular surgery, interventional radiology, intensive care and orthoplastic reconstruction are available in one centre, allowing single-stage vessel-and-bone management. In limited-resource or pre-transfer settings, the priorities are haemorrhage control, reduction of limb-threatening dislocations, documented serial neurovascular checks, early senior consultation and transfer planning. A temporary intravascular shunt plus a spanning external fixator is a powerful damage-control combination that restores perfusion and stabilises the skeleton while definitive vascular and orthopaedic reconstruction is arranged or the patient is transferred.
Controversies and Areas of Uncertainty
Several questions in this field have no single right answer and are common viva ground.
- The Debate
- Observe a well-perfused but pulseless hand after reduction versus explore.
- Pragmatic Position
- Reduce and stabilise first; a perfused hand may be observed closely, but persistent pulselessness with poor perfusion or median/AIN deficit favours exploration in many protocols.
- The Debate
- Whether to shunt routinely in combined orthopaedic-vascular injury.
- Pragmatic Position
- No randomised data; cohort evidence links shunting to less compartment syndrome. Shunt when bone fixation will delay flow or physiology is hostile.
- The Debate
- Routine fasciotomy after revascularisation versus close monitoring.
- Pragmatic Position
- Low threshold after prolonged ischaemia, combined arterial and venous injury or unreliable examination; selective monitoring when ischaemia time is short and examination reliable.
- The Debate
- Whether all Schatzker 4-6 fractures with symmetric pulses need ABI.
- Pragmatic Position
- Single-centre data show ABI screening misses no injuries; many trauma services now screen routinely.
- The Debate
- Stenting or embolisation versus open repair in extremity arterial injury.
- Pragmatic Position
- Endovascular is useful for selected proximal, pseudoaneurysm or AV-fistula lesions; open repair remains standard for most acute limb-threatening transection.
Common Pitfalls
- Calling the limb safe because a pulse is palpable once.
- Forgetting that a knee dislocation may reduce before presentation.
- Delaying reduction of a threatened limb for routine imaging.
- Sending a patient with hard signs for CTA without vascular agreement.
- Performing prolonged definitive fixation while the foot is ischaemic.
- Repairing the artery without stabilising a skeleton that will disrupt the repair.
- Failing to consider a temporary shunt in a damage-control situation.
- Waiting for pulselessness before diagnosing compartment syndrome.
- Forgetting to document serial neurovascular checks.
- Assuming limb salvage means useful function.
MCQ Practice Points
Q: What are hard signs of extremity vascular injury? A: Active arterial bleeding, expanding haematoma, bruit, thrill, absent pulse and distal ischaemia are hard signs. They require urgent vascular control rather than routine delayed imaging.
Q: What does an ABI/API above 0.9 mean after extremity trauma? A: If the examination is normal and reliable, it supports serial observation. An ABI/API of 0.9 or less, uncertainty or a discordant high-risk mechanism prompts CTA or vascular assessment.
Q: Why is a spontaneously reduced knee dislocation still dangerous? A: Popliteal artery injury can be occult initially, so the patient still needs vascular screening with documented pulses, Doppler, ABI/API and serial examination.
Q: What is the role of a temporary vascular shunt? A: It restores perfusion during damage control, transfer, skeletal stabilisation or staged repair. It is a bridge to definitive vascular reconstruction, not definitive treatment.
Q: Can compartment syndrome occur with pulses present after vascular repair? A: Yes. Reperfusion after vascular repair is a major risk setting, and compartment syndrome remains a clinical diagnosis when signs are clear.
Exam Cheat Sheet
First Actions
- Primary survey and haemorrhage control
- Document neurovascular status
- Reduce gross dislocation if limb threatened
- Repeat examination after reduction
- Hard signs go to urgent vascular pathway
Screening
- Pulses alone are not enough
- Use Doppler and ABI/API
- Above 0.9 plus normal reliable exam supports serial observation
- 0.9 or less, uncertainty or discordance prompts CTA or vascular review
- CTA is first-line imaging when stable enough
Sequence
- Critical ischaemia favours vessel-first
- Unstable skeleton threatening repair may need rapid external fixation
- Temporary shunt restores flow during staged care
- Definitive fixation follows physiology, perfusion and soft tissue readiness
- Reassess perfusion after every step
Fasciotomy
- Established compartment syndrome is an emergency
- High risk after prolonged ischaemia and reperfusion
- Combined fracture and vascular injury lowers threshold
- Do not wait for pulselessness
- Document timing and serial findings
Applied Scenarios
Practise clinical reasoning and management decisions out loud
“A patient reports a knee deformity that reduced before arrival. The limb is warm and pulses are palpable.”
“A patient has an ankle fracture-dislocation with a cool foot and absent Doppler signal.”
“A patient has a distal femur fracture, absent distal pulses and CTA shows popliteal artery occlusion. The fracture is very unstable.”
“An older patient has shoulder dislocation with axillary artery occlusion. Flow is restored after repair, but the arm becomes tense and analgesic requirement rises.”
Evidence Base
Penetrating Lower-Extremity Arterial Trauma: EAST Practice Management Guideline
- Forty-three articles screened; 20 used to construct the guideline updating the 2002 EAST recommendations.
- Physical examination and ankle-brachial index allow expedited triage of penetrating lower-limb arterial injury.
- CTA has become the diagnostic study of choice when imaging is required.
- Tourniquets and temporary intravascular shunts are recognised adjuncts in lower-extremity arterial trauma.
Imaging Vascular Trauma
- Systematic review of 58 articles (2000-2010); CTA was the dominant modern diagnostic modality across the vascular-trauma literature.
- CTA showed acceptable sensitivity and specificity for blunt and penetrating vascular injury within the neck and extremity.
- Duplex, MRA and transoesophageal echocardiography each had significant drawbacks as first-line tools.
CT Angiography Effectively Evaluates Extremity Vascular Trauma
- Single Level-I trauma centre series; 38 patients underwent CTA and 14 conventional arteriography for extremity vascular trauma.
- There were no false negatives or missed injuries with CTA.
- CTA supplanted catheter arteriography as the initial radiographic test, offering non-invasiveness and immediate availability.
Nonoperative Management of Occult Arterial Injuries and Physical Examination Alone
- Clinically occult arterial injuries without hard signs were safely managed nonoperatively; only 4 of 43 (9%) deteriorated and needed delayed surgery, all with good results.
- Of 287 patients managed by physical examination alone, only 4 (1.3%) required delayed surgery within the first week.
- No patient contacted at long-term follow-up reported vascular symptoms.
Reference Links
- PubMed: EAST lower-extremity arterial trauma guideline
- PubMed: CTA effectively evaluates extremity vascular trauma
- PubMed: imaging vascular trauma systematic review
- PubMed: physical examination and occult arterial injury follow-up
- PubMed: ABI and ultrasonography systematic review
- PubMed: temporary shunts systematic review
- PubMed: combined orthopaedic and vascular trauma shunting
- PubMed: civilian lower-extremity arterial trauma outcomes