Tscherne Classification of Closed Soft-Tissue Injury
Tscherne C2 and C3 injuries require staged management — never rush definitive internal fixation through compromised soft tissues. For C3 with compartment syndrome, fasciotomy is the immediate priority, followed by temporary spanning external fixation, and definitive fixation only after soft-tissue recovery (typically 10 to 21 days). For C2, a temporary external fixator or definitive fixation within 24 hours is acceptable only if the soft-tissue envelope is carefully assessed and the surgical approach does not further violate the injured zone.
The Tscherne Grades
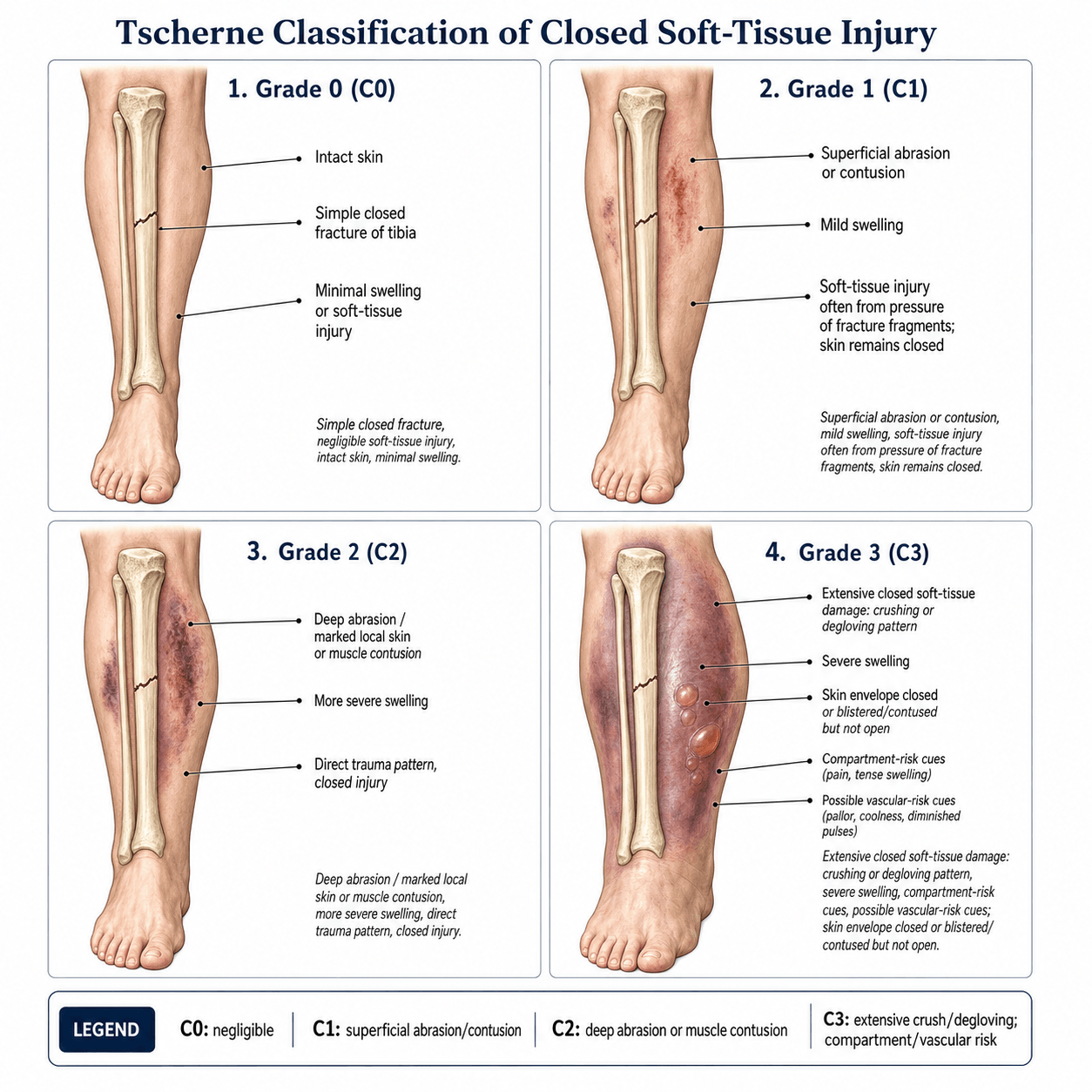

Each grade describes the severity of the closed soft-tissue injury. The fracture geometry is classified separately (AO/OTA).
- Soft-Tissue Injury
- None or minimal
- Fracture Mechanism
- Indirect / low energy
- Clinical Features
- Intact skin, no swelling or contusion
- Management
- Immediate definitive fixation
- Soft-Tissue Injury
- Superficial abrasion or contusion
- Fracture Mechanism
- Indirect violence
- Clinical Features
- Skin abrasion, mild swelling, no fracture blisters
- Management
- Definitive fixation; may stage if approach crosses contused skin
- Soft-Tissue Injury
- Deep contusion, muscle involvement
- Fracture Mechanism
- Direct / high energy
- Clinical Features
- Significant swelling, impending compartment syndrome, fracture blisters
- Management
- Staged: temporary external fixator, definitive fixation after soft-tissue recovery (7 to 21 days)
- Soft-Tissue Injury
- Compartment syndrome, vascular injury, crush, degloving
- Fracture Mechanism
- Severe direct / crush
- Clinical Features
- Established compartment syndrome, ischaemia, extensive degloving, or crush
- Management
- Emergency fasciotomy plus temporary external fixator; definitive fixation delayed 10 to 21 days
Clean · Skin · Deep · CrisisThe four Tscherne grades
Hook:Severity climbs from clean skin to crisis — and the grade, not the fracture pattern, drives the timing of fixation.
Tscherne is for CLOSED fractures only. If the fracture is open, use Gustilo-Anderson. If you are presented with a closed fracture and asked about soft-tissue severity, reach for Tscherne. A common exam trap is to grade an open fracture with Tscherne — the correct answer is Gustilo-Anderson.
Clinical Decision-Making: Timing of Fixation

The Tscherne grade directly determines the urgency and staging of fracture fixation.
- Fixation Strategy
- Definitive internal fixation (IM nail, plate)
- Timing
- Immediate or next operating list
- Key Principle
- Soft tissues are not a constraint
- Fixation Strategy
- Definitive fixation (plan approach around skin injury)
- Timing
- Within 24 to 48 hours
- Key Principle
- Avoid incisions through abrasions or contusions
- Fixation Strategy
- Staged: spanning external fixator then definitive fixation
- Timing
- Spanning ex-fix immediately; definitive at 7 to 21 days when soft tissues settle (wrinkle sign positive)
- Key Principle
- Never plate or nail through a swollen, blistered soft-tissue envelope
- Fixation Strategy
- Emergency fasciotomy and spanning external fixator; definitive fixation delayed
- Timing
- Fasciotomy immediately; ex-fix at same setting; definitive at 10 to 21 days
- Key Principle
- Limb salvage first — fasciotomy and revascularisation before fracture fixation
A Tscherne C3 limb with compartment syndrome is a surgical emergency. Time is tissue: irreversible muscle necrosis begins within 6 to 8 hours of raised compartment pressure. Fasciotomy must not be delayed for imaging, transfer, or fracture planning. Open all four compartments of the leg (or the relevant compartments at other sites). Decompress first, fix later.
Wrinkle sign = window openWhen to stage vs fix immediately
Hook:No wrinkles, no window — never plate or nail through a swollen, blistered soft-tissue envelope.
Tscherne vs Gustilo-Anderson: When to Use Which
Both systems grade soft-tissue injury associated with fractures, but they apply to different scenarios.
- Tscherne Classification
- Closed fractures only
- Gustilo-Anderson Classification
- Open fractures only
- Tscherne Classification
- C0, C1, C2, C3
- Gustilo-Anderson Classification
- I, II, IIIA, IIIB, IIIC
- Tscherne Classification
- Soft-tissue contusion, compartment status
- Gustilo-Anderson Classification
- Wound size, contamination, vascular injury
- Tscherne Classification
- Tscherne and Gotzen (Hannover, Germany)
- Gustilo-Anderson Classification
- Gustilo and Anderson (Minneapolis, USA)
- Tscherne Classification
- Timing of fixation (immediate vs staged)
- Gustilo-Anderson Classification
- Prognosis, antibiotic protocol, wound management
- Tscherne Classification
- Applying to open fractures (wrong)
- Gustilo-Anderson Classification
- Applying to closed fractures (wrong)
Some exam questions describe a closed fracture with significant swelling and blisters, then ask you to classify the soft-tissue injury. The answer is Tscherne C2 (closed, deep contusion, fracture blisters). If the same vignette mentioned an open wound, you would switch to Gustilo-Anderson. Always confirm the fracture is closed before applying Tscherne.
Specific Clinical Scenarios
Fracture Blisters
Fracture blisters indicate significant soft-tissue injury and appear when Tscherne grade is C2 or higher.
- Serous (clear) blisters: less severe dermal injury; incisions may be made through healed serous blister sites
- Haemorrhagic (blood-filled) blisters: indicate deeper dermal disruption; do not incise through haemorrhagic blister beds
- Management: leave intact, protect from shear, wait for re-epithelialisation before surgery
Degloving Injuries (Closed)
Closed degloving (Morel-Lavallee lesion) represents a Tscherne C3 pattern even without an open wound.
- Separation of subcutaneous tissue from underlying fascia
- Can accumulate significant haemorrhagic fluid
- High risk of infection if internal fixation is placed through the degloved zone
- Management: percutaneous drainage or open debridement, staged fixation
Compartment Syndrome
The hallmark of Tscherne C3 is established compartment syndrome.
- Five Ps: Pain out of proportion (early and most reliable), Pressure (tense compartment), Paraesthesia, Paralysis (late), Pulselessness (very late — do not wait for this)
- Pain with passive stretch of the muscles in the compartment is the most sensitive clinical sign
- Measure compartment pressure if clinical suspicion exists: delta pressure less than 30 mmHg (diastolic BP minus compartment pressure) is an indication for fasciotomy
- Open all compartments: leg requires four-compartment fasciotomy (anterior, lateral, superficial posterior, deep posterior)
The 5 Ps — Pain · Pressure · Paraesthesia · Paralysis · PulselessnessCompartment syndrome warning signs
Hook:Act on the early Ps (pain, pain on passive stretch) — never wait for pulselessness.
The topic quotes the threshold; examiners want the method and the reasoning behind it.
- The diagnosis is clinical in the awake patient. Pain out of proportion and pain on passive stretch decide it — do not delay an obvious case to obtain a number.
- Measurement is an ADJUNCT, most valuable when the patient cannot report pain — the obtunded, unconscious, intubated, or regionally-anaesthetised patient, or a genuinely equivocal awake case. In these, continuous monitoring (an indwelling catheter transducing pressure) is advocated.
- Technique: use a calibrated manometer — a handheld Stryker device, or a needle/slit catheter connected to an arterial-line transducer. Measure within 5 cm of the fracture (pressure is highest there), in each compartment (in the leg the deep posterior is the one most often missed), with the limb at heart level and the transducer zeroed.
- The threshold is perfusion-based — the delta pressure (ΔP). ΔP = diastolic blood pressure minus the measured compartment pressure; a ΔP of 30 mmHg or less is the indication for fasciotomy (McQueen and Court-Brown). ΔP is preferred over any absolute cut-off because it accounts for the patient's perfusion: a hypotensive, shocked patient tolerates a far lower absolute compartment pressure, so an absolute value alone under-calls compartment syndrome in exactly the patient most at risk.
- A single normal reading does not exclude an evolving compartment syndrome — repeat the clinical assessment and the measurement; beware a regional block or epidural masking the cardinal pain.
"Four-compartment fasciotomy" is the answer; the marks are in the technique, the aftercare, and the one situation where you should NOT decompress.
- Two-incision technique (the workhorse for the leg). An anterolateral incision releases the anterior and lateral compartments — identify and protect the superficial peroneal nerve as it pierces the fascia at the anterolateral intermuscular septum. A posteromedial incision a finger-breadth behind the posteromedial tibial border releases the superficial and deep posterior compartments — protect the saphenous vein and nerve. The deep posterior compartment is the one most often inadequately released — confirm you have opened it (tibialis posterior). A single perifibular incision is an alternative but less forgiving.
- Release must be complete and the skin generous — a short skin incision over a fully divided fascia still constricts ("dermotomy" matters). Excise only frankly necrotic muscle; preserve anything contractile/bleeding.
- Aftercare: leave the wounds OPEN. Apply a negative-pressure (VAC) dressing or vessel-loop dermatotraction ("shoelace") to keep the edges approximated, and return at 48–72 hours for a second-look debridement. Achieve delayed primary closure once swelling settles, or split-skin graft if the skin will not close.
- When NOT to decompress — the late/missed compartment syndrome. If presentation is late with an established, complete syndrome and clinically non-viable muscle (classically beyond roughly 24–36 hours, with dense paralysis and anaesthesia), opening dead muscle invites overwhelming infection and sepsis, and reperfusion drives rhabdomyolysis and acute kidney injury — fasciotomy is then contraindicated; manage expectantly (and consider delayed reconstruction or amputation).
- The end-stage of untreated compartment ischaemia is Volkmann's ischaemic contracture — fibrosis and fixed contracture of the infarcted muscle (the classic forearm deformity, with a leg equivalent) and the reason the early Ps must never be ignored.
Limitations and Modern Context
- Inter-observer reliability is moderate. As with Gustilo-Anderson, the final Tscherne grade may only be apparent at surgical exploration or after 48 hours of observation when the full extent of soft-tissue injury declares itself. Early grading tends to underestimate severity.
- MRI and compartment pressure monitoring improve accuracy but Tscherne remains primarily a clinical classification. MRI can reveal occult muscle contusion and oedema that upgrades a C1 to a C2 assessment.
- The AO/OTA system incorporates soft-tissue qualifiers that overlap with Tscherne. In practice, many surgeons document both the AO/OTA fracture code and the Tscherne soft-tissue grade to fully describe the injury.
- Damage-control orthopaedics (DCO) has become standard for C2 and C3 injuries: a spanning external fixator applied within hours, then conversion to definitive fixation at 7 to 21 days once the soft-tissue envelope recovers. This approach reduces complications (infection, wound breakdown, non-union) compared with early definitive fixation through compromised tissues.
- Tscherne was developed for tibial and femoral fractures. Application to other anatomical sites (forearm, humerus, pelvis) is extrapolation — the principles hold but the grading was originally described for lower-limb long-bone injuries.
Guidelines, Registries and Global Practice
International Guideline Consensus
- Key Recommendations
- Fasciotomy for suspected compartment syndrome; staged fixation for high-energy closed fractures with soft-tissue compromise; document soft-tissue grade
- Notes
- Emphasises clinical diagnosis; compartment pressure monitoring adjunctive only
- Key Recommendations
- Tscherne classification taught alongside AO/OTA fracture coding; C2 and C3 managed with damage-control protocol
- Notes
- Global training standard; integrates Tscherne into decision algorithms
- Key Recommendations
- Compartment syndrome is a surgical emergency; fasciotomy within 6 hours of diagnosis; staged fixation for severe soft-tissue injuries
- Notes
- Focus on medicolegal implications of delayed fasciotomy
- Key Recommendations
- Damage-control orthopaedics recommended for polytrauma with C2/C3 extremity injuries; temporary external fixation with early conversion
- Notes
- European trauma centres widely adopt DCO protocols
Registry Evidence and Global Practice Variation
- The Swedish Fracture Register (SFR) documents soft-tissue grading at index admission and captures complication data including infection, wound breakdown, and re-operation; analysis shows that Tscherne C2 and C3 injuries have significantly higher 12-month complication rates than C0/C1.
- Practice variation exists between regions: some European trauma centres have standardised DCO protocols with predefined conversion windows, while some US centres favour early total care with careful soft-tissue assessment. Both approaches are acceptable if the soft-tissue envelope is respected.
- In resource-limited settings, external fixation may be the definitive treatment for C3 injuries where theatre access and implants are scarce — the Tscherne grade still guides decision-making but the hardware available determines the final construct.
Viva practice
Exam Viva
Practise clinical reasoning and management decisions out loud
“A 28-year-old man is brought to the emergency department after a high-speed motorcycle collision. His right tibia has a closed diaphyseal fracture. The leg is markedly swollen, tense, and tender. There are haemorrhagic fracture blisters over the anteromedial shin. He has severe pain on passive toe extension. Distal pulses are present. How do you classify this injury and what is your management plan?”
“A 42-year-old woman sustains a closed bicondylar tibial plateau fracture (Schatzker VI) in a fall from a horse. Her leg is swollen with a large haemorrhagic fracture blister over the lateral proximal tibia and a tense anterior compartment. She has reduced sensation in the first web space. Distal pulses are present. Discuss your classification, assessment, and staged management plan.”
Exam cheat sheet
The four grades
- C0: no soft-tissue injury — simple fracture, intact skin, no swelling
- C1: superficial abrasion or contusion — indirect mechanism, mild swelling
- C2: deep contusion — direct/high-energy, significant swelling, fracture blisters, impending compartment syndrome
- C3: severe — established compartment syndrome, vascular injury, crush, or closed degloving
Management by grade
- C0 and C1: immediate or early definitive fixation (within 24 to 48 hours)
- C2: staged — spanning external fixator, then definitive fixation at 7 to 21 days
- C3: emergency fasciotomy plus spanning external fixator; definitive fixation at 10 to 21 days
- Wrinkle sign = soft tissues ready for definitive fixation
Key principles and traps
- Tscherne is for CLOSED fractures only — open fractures use Gustilo-Anderson
- Soft-tissue grade determines outcome more than fracture pattern
- Pain out of proportion and pain on passive stretch are the earliest compartment syndrome signs
- Do not wait for pulselessness — by then the limb may be unsalvageable
- Haemorrhagic blisters indicate deeper injury than serous blisters
- Fasciotomy wounds are left open — delayed primary closure or skin grafting
Evidence
Changes in the management of femoral shaft fractures in polytrauma patients: from early total care to damage control orthopedic surgery
- Cohort study across three eras (early total care 1981–89; intermediate; damage control 1993–2000) for femoral shaft fractures in blunt polytrauma.
- Systemic complications — multiple organ failure and ARDS — fell significantly from the early-total-care to the damage-control era, regardless of the type of femoral fixation.
- Primary external fixation was used more in the damage-control era; intramedullary nailing still carried a higher ARDS rate than external fixation even then.
Compartmental syndromes
- Foundational review establishing the relationship between raised intracompartmental pressure and muscle/nerve ischaemia.
- Emphasised that early diagnosis is vital and that simple clinical tests permit diagnosis in most cases.
- Prompt, complete decompression (fasciotomy) of the affected compartments preserves function and minimises complications.
According to PubMed, damage-control orthopaedics (fewer systemic complications than early total care) is supported by Pape et al. 2002 (DOI 10.1097/00005373-200209000-00010); the compartment-syndrome principles by Matsen & Krugmire 1978 (PMID 362581); fracture-blister management (avoid incisions through haemorrhagic blisters) by Giordano & Koval 1995 (DOI 10.1097/00005131-199504000-00014); and staged spanning-ex-fix-then-definitive fixation (5% deep infection) by Egol et al. 2005 (DOI 10.1097/01.bot.0000171881.11205.80).