Neuraxial and Peripheral Blocks | Ultrasound-Guided | LAST Prevention and Management
REGIONAL ANESTHESIA CLASSIFICATION
Critical Must-Knows
- Ultrasound guidance reduces complications and improves success rates
- LAST (Local Anesthetic Systemic Toxicity) - recognize CNS then cardiac signs
- Interscalene block for shoulder - expect phrenic nerve palsy
- Adductor canal block preserves quadriceps strength vs femoral block
- Lipid emulsion 20% is first-line treatment for LAST
Clinical Pearls
- "Regional anesthesia reduces opioid use, improves pain control, and enables early mobilization
- "Ultrasound has become standard of care for most peripheral nerve blocks
- "LAST presents with CNS symptoms first (perioral numbness, tinnitus) then cardiovascular collapse
- "Continuous catheter techniques provide prolonged analgesia (48-72 hours)
Critical Regional Anesthesia Exam Points
LAST Recognition and Management
CNS symptoms precede cardiac: perioral numbness, metallic taste, tinnitus, seizures, then arrhythmias and cardiac arrest. Treatment: stop LA injection, lipid emulsion 20% (1.5 mL/kg bolus), CPR if needed, avoid vasopressin.
Ultrasound Guidance Benefits
Ultrasound reduces block failure and vascular puncture (block failure RR 0.41, vascular puncture RR 0.16 vs nerve stimulation). Allows direct visualization of nerves, needle, and local anesthetic spread. Real-time adjustment prevents intravascular injection.
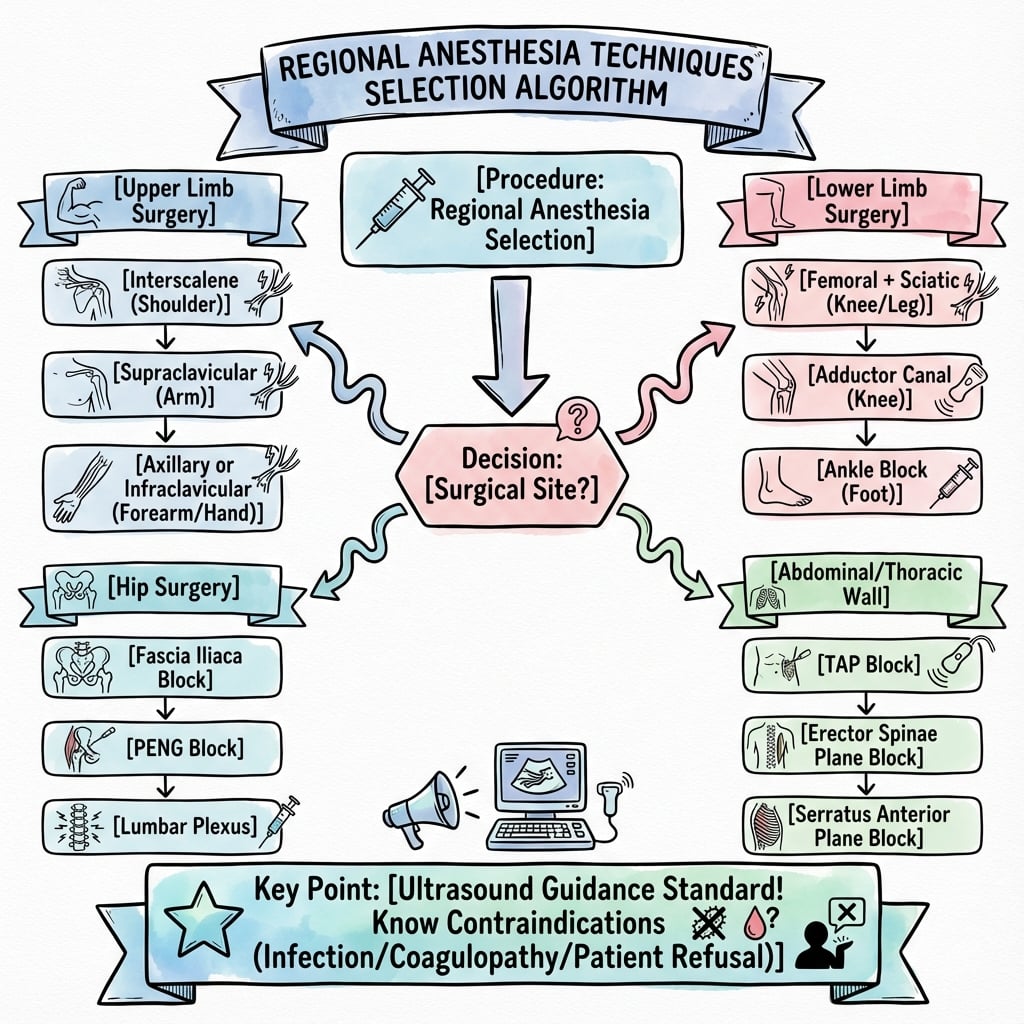
Block Selection for Surgery
Match block to procedure: shoulder (ISB), elbow/forearm (SCB or ICB), hand (axillary), TKA (ACB + sciatic or periarticular), THA (lumbar plexus or fascia iliaca), ankle (sciatic + saphenous).
Functional Implications
Motor vs sensory: femoral block causes quadriceps weakness (fall risk), adductor canal block preserves strength. Interscalene blocks the phrenic nerve (avoid bilateral, caution in respiratory disease).
At a Glance
Regional anesthesia in orthopaedics includes neuraxial (spinal/epidural) and peripheral nerve blocks for upper limb (interscalene for shoulder, supraclavicular/infraclavicular for elbow/forearm, axillary for hand) and lower limb (femoral, adductor canal, sciatic, popliteal). Ultrasound guidance is now standard, reducing block failure and vascular puncture compared with nerve stimulation. The critical complication is LAST (Local Anesthetic Systemic Toxicity), which presents with CNS symptoms first (perioral numbness, tinnitus, seizures) before cardiovascular collapse - treatment is 20% lipid emulsion (1.5 mL/kg bolus). Adductor canal block is preferred over femoral nerve block for TKA as it preserves quadriceps strength and enables early mobilisation.
LAST - LLAST - Local Anesthetic Systemic Toxicity Signs
| L | Lightheaded, tongue numbness Early CNS - perioral tingling, metallic taste |
| A | Auditory changes (tinnitus) Ringing in ears, visual disturbances |
| S | Seizures and confusion Severe CNS toxicity - agitation, seizures, coma |
| T | Tachycardia then bradycardia Cardiac - arrhythmias, hypotension, arrest |
| L | Lightheaded, tongue numbness Early CNS - perioral tingling, metallic taste | S | Seizures and confusion Severe CNS toxicity - agitation, seizures, coma |
| A | Auditory changes (tinnitus) Ringing in ears, visual disturbances | T | Tachycardia then bradycardia Cardiac - arrhythmias, hypotension, arrest |
Hook:LAST symptoms progress from CNS (first) to cardiac (late) - recognize early and give lipid emulsion
LASTLIPIDS - Treatment of LAST
| L | LIPID emulsion 20% 1.5 mL/kg bolus over 1 minute |
| I | Infusion 0.25 mL/kg/min Continue for at least 10 minutes after stability |
| P | Propofol is NOT a substitute Use intralipid or similar lipid emulsion |
| I | IV access and airway Secure airway, ventilate with 100% O2 |
| D | Don't use vasopressin Use adrenaline in small doses for cardiac arrest |
| S | Stop LA injection immediately Recognize early, stop injecting |
| L | LIPID emulsion 20% 1.5 mL/kg bolus over 1 minute | P | Propofol is NOT a substitute Use intralipid or similar lipid emulsion | D | Don't use vasopressin Use adrenaline in small doses for cardiac arrest |
| I | Infusion 0.25 mL/kg/min Continue for at least 10 minutes after stability | I | IV access and airway Secure airway, ventilate with 100% O2 | S | Stop LA injection immediately Recognize early, stop injecting |
Hook:LIPIDS saves lives in LAST - lipid emulsion is the antidote, not propofol
4 A4 As - Upper Limb Block Approaches
| A1 | Above clavicle (Interscalene) Shoulder surgery - C5, C6, C7 |
| A2 | Above clavicle (Supraclavicular) Elbow/forearm - entire brachial plexus |
| A3 | Axilla (Axillary) Hand/wrist - terminal branches |
| A4 | Around humerus (Infraclavicular) Elbow/forearm - cords of plexus |
| A1 | Above clavicle (Interscalene) Shoulder surgery - C5, C6, C7 | A3 | Axilla (Axillary) Hand/wrist - terminal branches |
| A2 | Above clavicle (Supraclavicular) Elbow/forearm - entire brachial plexus | A4 | Around humerus (Infraclavicular) Elbow/forearm - cords of plexus |
Hook:The 4 As go from proximal (shoulder) to distal (hand) as you move down the arm
FNB - QACB vs FNB - Quadriceps Strength
| A | Adductor Canal Block Preserves quadriceps strength |
| C | Canal contains sensory nerves Saphenous nerve + nerve to vastus medialis (mostly sensory) |
| B | Better for mobilization Early ambulation after TKA |
| F | Femoral Nerve Block Blocks quadriceps motor function |
| N | No quadriceps strength Fall risk, delayed mobilization |
| B | Better analgesia But motor block is a disadvantage |
| A | Adductor Canal Block Preserves quadriceps strength | B | Better for mobilization Early ambulation after TKA | N | No quadriceps strength Fall risk, delayed mobilization |
| C | Canal contains sensory nerves Saphenous nerve + nerve to vastus medialis (mostly sensory) | F | Femoral Nerve Block Blocks quadriceps motor function | B | Better analgesia But motor block is a disadvantage |
Hook:ACB for mobilization (motor-sparing), FNB for analgesia (motor block)
Overview and Role in Orthopaedics
Regional anesthesia encompasses neuraxial (spinal, epidural) and peripheral nerve block techniques that provide targeted anesthesia and analgesia for orthopaedic procedures. These techniques have become integral to Enhanced Recovery After Surgery (ERAS) protocols and multimodal analgesia.
Benefits in orthopaedic surgery:
- Superior analgesia compared to systemic opioids
- Reduced opioid consumption by 30-50%
- Earlier mobilization with motor-sparing blocks
- Reduced hospital length of stay
- Lower incidence of PONV (postoperative nausea and vomiting)
- Improved patient satisfaction
Evolution of practice:
- Landmark-based techniques (1970s-1990s): anatomical landmarks, nerve stimulator
- Ultrasound guidance (2000s-present): direct visualization, real-time needle placement
- Motor-sparing blocks (2010s-present): adductor canal, IPACK, PENG blocks
- Continuous catheter techniques: prolonged analgesia for complex surgery
Ultrasound Revolution
The introduction of ultrasound guidance has transformed regional anesthesia. In a meta-analysis of randomised trials, ultrasound reduced block failure (RR 0.41), reduced vascular puncture (RR 0.16), shortened onset and prolonged block duration compared with nerve stimulation. Ultrasound allows visualization of nerves, surrounding structures (vessels, pleura), needle trajectory, and local anesthetic spread.
Neuraxial Anesthesia
Spinal Anesthesia (Subarachnoid Block)
Technique:
- Level: L3-L4 or L4-L5 interspace (below conus medullaris at L1-L2)
- Position: Sitting or lateral decubitus
- Needle: 25G or 27G pencil-point (Whitacre, Sprotte) reduces PDPH
- Local anesthetic: Bupivacaine 0.5% heavy (10-15 mg for lower limb)
- Onset: 5-10 minutes
- Duration: 90-150 minutes (plain), 120-180 minutes (heavy with opioid)
Indications in orthopaedics:
- Total hip arthroplasty
- Total knee arthroplasty
- Lower limb fracture fixation
- Foot and ankle surgery
Advantages:
- Rapid onset
- Dense motor and sensory block
- Predictable duration
- Reduced blood loss (controlled hypotension)
Disadvantages:
- Fixed duration (single-shot)
- Hypotension (sympathetic blockade)
- Urinary retention
- Headache risk if dural puncture with large needle
Epidural Anesthesia
Technique:
- Level: Lumbar (L2-L3, L3-L4) for lower limb, thoracic for upper abdominal/thoracic
- Loss of resistance technique to identify epidural space
- Catheter placement: allows continuous infusion
- Local anesthetic: Bupivacaine 0.25-0.5%, ropivacaine 0.2-0.5%
- Onset: 15-30 minutes
- Duration: Continuous (with catheter)
Indications:
- Major lower limb surgery (bilateral TKA, complex trauma)
- Postoperative analgesia after spine surgery
- Rib fractures (thoracic epidural)
Advantages:
- Titratable anesthesia
- Continuous technique (catheter)
- Can be used for postoperative analgesia
- Cardiovascular stability (gradual onset)
Disadvantages:
- Slower onset than spinal
- More drug required
- Epidural hematoma risk (anticoagulation)
- Patchy block (5-10% failure rate)
Combined Spinal-Epidural (CSE)
Technique:
- Needle-through-needle or separate spaces
- Spinal component for rapid onset
- Epidural catheter for prolonged analgesia
Indications:
- Long or unpredictable duration surgery
- Postoperative analgesia required (THA, TKA)
Neuraxial Techniques Comparison
| Feature | Spinal | Epidural | CSE |
|---|---|---|---|
| Onset | 5-10 minutes | 15-30 minutes | 5-10 minutes |
| Duration | 90-180 minutes | Continuous | Continuous |
| Failure rate | Less than 5% | 5-10% | Less than 5% |
| Hypotension | High | Moderate | High initially |
| PDPH risk | Less than 1% | 1-2% | Less than 1% |
| Best use | Short procedures | Long procedures | Long with rapid onset |
Absolute contraindications to neuraxial anesthesia:
- Patient refusal
- Infection at injection site
- Therapeutic anticoagulation (see time intervals below)
- Hypovolemic shock
- Elevated intracranial pressure
Relative contraindications:
- Sepsis
- Thrombocytopenia (under 80,000)
- Pre-existing neurological disease
- Severe aortic stenosis
Upper Extremity Peripheral Nerve Blocks
Interscalene Block (ISB)
Anatomy:
- Target: Brachial plexus roots (C5, C6, C7) at the level of cricoid cartilage
- Location: Between anterior and middle scalene muscles
- Nerves blocked: C5, C6, C7 (superior trunk primarily)
- Nerves often missed: C8, T1 (ulnar nerve territory - hand)
Indications:
- Shoulder surgery (rotator cuff, arthroplasty, arthroscopy)
- Proximal humerus fractures
- Clavicle fractures
Technique:
- Position: Supine, head turned away
- Ultrasound: High-frequency linear probe at cricoid level
- Target: Between scalene muscles, roots appear as "traffic lights"
- Local anesthetic: 15-20 mL of 0.5% ropivacaine or bupivacaine
- Approach: In-plane or out-of-plane
Expected outcomes:
- Onset: 15-30 minutes
- Duration: 12-18 hours (single-shot), 48-72 hours (catheter)
- Coverage: Shoulder, proximal arm (incomplete hand coverage)
Complications:
- Phrenic nerve palsy: 100% temporary hemidiaphragm paralysis
- Horner syndrome: 25-75% (ptosis, miosis, anhidrosis)
- Recurrent laryngeal nerve block: 5-10% (hoarseness)
- Vertebral artery injection: rare but catastrophic
- Pneumothorax: under 1% with ultrasound
Special considerations:
- Avoid bilateral ISB: risk of bilateral phrenic palsy and respiratory compromise
- Caution in respiratory disease: COPD, obstructive sleep apnea
- Low-volume techniques (5-10 mL) reduce phrenic nerve involvement
This completes the interscalene block section.
Upper Extremity Block Selection by Surgery
| Surgery | First Choice | Alternative | Coverage Needed |
|---|---|---|---|
| Shoulder arthroscopy | Interscalene | Supraclavicular | C5, C6, C7 (superior trunk) |
| Proximal humerus ORIF | Interscalene | Supraclavicular | C5-C7, partial C8-T1 |
| Elbow arthroscopy | Supraclavicular | Infraclavicular | Complete C5-T1 |
| Radius/ulna ORIF | Supraclavicular | Infraclavicular or axillary | C6-T1 |
| Carpal tunnel release | Axillary | Wrist blocks | Median nerve only |
| Hand fracture ORIF | Axillary | Supraclavicular | C7-T1 |
Lower Extremity Peripheral Nerve Blocks
Femoral Nerve Block (FNB)
Anatomy:
- Target: Femoral nerve lateral to femoral artery
- Location: Below inguinal ligament in femoral triangle
- Innervation: Anterior thigh, knee joint, medial leg (saphenous branch)
Indications:
- Femur fracture (analgesia)
- Knee surgery (combined with sciatic or local infiltration)
- Quadriceps tendon repair
Technique:
- Position: Supine, leg slightly abducted
- Ultrasound: Linear probe at inguinal crease
- Target: Femoral nerve lateral to artery, deep to fascia iliaca
- Local anesthetic: 20-30 mL
- Approach: In-plane from lateral
Expected outcomes:
- Onset: 15-30 minutes
- Duration: 12-18 hours
- Coverage: Anterior thigh, knee joint, medial leg
Complications:
- Quadriceps weakness: 100% (major disadvantage)
- Fall risk: due to inability to weight-bear
- Vascular puncture: femoral artery adjacent
- Nerve injury: rare with ultrasound
Fascia Iliaca Block (FIB):
- Alternative approach: more lateral, below fascia iliaca
- Advantages: Easier landmark, lower nerve injury risk
- Disadvantages: Less consistent coverage, requires higher volume (40-50 mL)
This completes the femoral nerve block section.
Lower Extremity Block Selection by Surgery
| Surgery | Block Options | Motor Considerations | Advantage |
|---|---|---|---|
| TKA | ACB + IPACK or periarticular | Quadriceps preserved | Early mobilization |
| THA | PENG or fascia iliaca | Quadriceps preserved | Hip-specific analgesia |
| Femur fracture | Femoral or fascia iliaca | Quadriceps blocked (acceptable) | Superior analgesia |
| Ankle ORIF | Popliteal sciatic + saphenous | Foot drop (overnight) | Complete ankle coverage |
| Foot surgery | Ankle block (5 nerves) | No motor block needed | Avoid sciatic motor block |
| ACL reconstruction | ACB | Quadriceps preserved | Allows quad exercises |
Ultrasound Guidance in Regional Anesthesia
Benefits of Ultrasound
Improved outcomes (Abrahams meta-analysis, BJA 2009):
- Block failure: reduced (RR 0.41, 95% CI 0.26-0.66)
- Onset time: 29% faster
- Block duration: 25% longer
- Vascular puncture: reduced (RR 0.16, 95% CI 0.05-0.47)
- Block quality: improved density and coverage
Safety advantages:
- Direct visualization: nerves, vessels, pleura, peritoneum
- Real-time needle tracking: prevents vascular puncture
- Spread confirmation: ensures adequate distribution
- Avoidance of injection: if intravascular or intraneural
Ultrasound Techniques
Probe selection:
- High-frequency linear (8-15 MHz): Superficial structures (under 4 cm)
- Low-frequency curvilinear (2-5 MHz): Deep structures (over 4 cm)
Needle approaches:
- In-plane: Needle parallel to probe, entire shaft visible
- Out-of-plane: Needle perpendicular to probe, only cross-section visible
Nerve identification:
- Hyperechoic: Bright, fascicular structure
- Honeycomb appearance: Multiple hypoechoic fascicles
- Adjacent structures: Arteries (pulsatile, compressible), veins, muscles
Signs of successful injection:
- Circumferential spread: "donut sign" around nerve
- Nerve expansion: slight distension during injection
- Separation: nerve separates from adjacent structures
Signs of intraneural injection (STOP immediately):
- High resistance to injection (over 15 psi)
- Patient reports severe paresthesia or pain
- Nerve expansion without spread around nerve
- No visible spread despite injection
If intraneural injection suspected, STOP, withdraw needle slightly, and reassess position.
Training and Competency
Learning curve:
- Basic skills: 20-30 blocks
- Competency: 50-100 blocks
- Expert level: 200+ blocks
Recommended pathway:
- Didactic learning (anatomy, physics)
- Simulation and phantom practice
- Supervised clinical practice
- Independent practice with backup
Local Anesthetic Pharmacology
Common Agents
Local Anesthetic Properties
| Agent | Onset | Duration | Max Dose (mg/kg) | Use |
|---|---|---|---|---|
| Lidocaine | Fast (5-10 min) | 60-120 min | 3 (5 with epi) | Short procedures |
| Mepivacaine | Moderate (10-15 min) | 90-180 min | 5 (7 with epi) | Intermediate duration |
| Bupivacaine | Slow (15-30 min) | 240-480 min | 2 (3 with epi) | Long procedures |
| Ropivacaine | Slow (15-30 min) | 240-480 min | 3 | Motor-sparing, long duration |
| Levobupivacaine | Slow (15-30 min) | 240-480 min | 2.5 | Less cardiotoxic than bupivacaine |
Mechanism of Action
Sodium channel blockade:
- Local anesthetics bind to voltage-gated sodium channels
- Block propagation of action potentials
- Prevent depolarization of nerve fibers
Differential blockade:
- Small fibers blocked first: Pain (C fibers), temperature (A-delta)
- Large fibers blocked last: Motor (A-alpha), proprioception
- Explains sensory block before motor block
Adjuncts
Epinephrine (1:200,000 to 1:400,000):
- Vasoconstriction: prolongs duration by 30-50%
- Reduces systemic absorption: lowers LAST risk
- Marker of intravascular injection: tachycardia if IV
- Avoid: in digital blocks, ISB (phrenic palsy duration)
Dexamethasone (4-8 mg):
- Prolongs duration: 30-50% increase
- Anti-inflammatory: reduces postoperative pain
- Perineural or IV: both effective
Clonidine (1-2 mcg/kg):
- Alpha-2 agonist: prolongs sensory and motor block
- Side effects: hypotension, sedation
- Less commonly used with longer-acting agents
Local Anesthetic Systemic Toxicity (LAST)
Mechanism and Risk Factors
Pathophysiology:
- CNS toxicity: Inhibition of inhibitory neurons first (excitation), then all neurons (depression)
- Cardiac toxicity: Blockade of cardiac sodium and potassium channels, calcium dysregulation
- Lipid sink theory: Lipid emulsion creates a "sink" to sequester LA from tissues
Risk factors:
- High total dose: exceeding maximum recommended
- Accidental intravascular injection: especially into artery
- Highly vascular site: intercostal, paracervical blocks
- Patient factors: extremes of age, cardiac disease, hepatic dysfunction, low protein states
Relative toxicity (most to least):
- Bupivacaine: highest cardiotoxicity
- Ropivacaine: intermediate
- Lidocaine: least toxic
Clinical Presentation
Progression of LAST:
Stage 1 - CNS excitation:
- Perioral numbness
- Metallic taste
- Tinnitus
- Visual disturbances
- Agitation, confusion
- Muscle twitching
Stage 2 - CNS depression:
- Seizures
- Loss of consciousness
- Respiratory depression
- Coma
Stage 3 - Cardiovascular toxicity:
- Bradycardia
- Hypotension
- Arrhythmias (ventricular tachycardia, fibrillation)
- Cardiac arrest (often resistant to standard ACLS)
Recognize LAST early: The first sign is often perioral numbness or tinnitus in an awake patient. If patient reports these symptoms during injection, STOP IMMEDIATELY. Do not continue injecting.
Management of LAST
Immediate actions:
- STOP injecting local anesthetic immediately
- Call for help - LAST is a team emergency
- Airway management: 100% oxygen, ventilate if needed
- Suppress seizures: Benzodiazepines (NOT propofol initially)
Lipid emulsion therapy:
- First-line treatment for LAST
- Intralipid 20% or equivalent lipid emulsion
Dosing protocol:
- Bolus: 1.5 mL/kg over 1 minute (approximately 100 mL for 70 kg adult)
- Infusion: 0.25 mL/kg/min
- Repeat bolus: if cardiovascular instability persists after 5 minutes
- Continue infusion: for at least 10 minutes after cardiovascular stability
- Maximum dose: 10 mL/kg over first 30 minutes
Cardiac arrest management:
- Start CPR immediately with ACLS protocol
- Continue lipid emulsion throughout resuscitation
- Use epinephrine in small doses (under 1 mcg/kg)
- AVOID vasopressin (may worsen cardiac toxicity)
- AVOID propofol (is NOT lipid emulsion therapy)
- Prolonged resuscitation: may require over 60 minutes, do not give up early
Post-resuscitation:
- Observe 4-6 hours minimum (12-24 hours if severe)
- Monitor: ECG, cardiac enzymes, lipid levels
- Risk of recurrence: as LA redistributes from tissues
Why Not Propofol?
Propofol is NOT a substitute for lipid emulsion. While propofol contains lipid, the concentration is too low (10% vs 20% in Intralipid), and propofol itself is a myocardial depressant. Using propofol for LAST can worsen cardiovascular collapse. Always use 20% lipid emulsion (Intralipid).
Prevention Strategies
Reduce risk of LAST:
- Use ultrasound guidance: reduces accidental intravascular injection
- Aspirate before injection: check for blood
- Fractionated dosing: inject 3-5 mL aliquots with pauses
- Test dose: with epinephrine (will cause tachycardia if IV)
- Maximum dose limits: calculate and respect limits
- Avoid bupivacaine for IVRA: use lidocaine or prilocaine
- Communicate with patient: ask about symptoms during injection
Contraindications and Complications
Absolute Contraindications
All regional blocks:
- Patient refusal
- Infection at injection site
- Allergy to local anesthetic (rare - true allergy under 1%)
Neuraxial specific:
- Therapeutic anticoagulation (see timing guidelines)
- Coagulopathy or thrombocytopenia (under 80,000)
- Elevated intracranial pressure
- Hypovolemic shock
Relative Contraindications
Consider risks vs benefits:
- Pre-existing neurological deficit (medicolegal)
- Sepsis (bacteremia risk of seeding)
- Severe spinal deformity (difficult technique)
- Prior spine surgery at level (altered anatomy)
- Prophylactic anticoagulation (timing critical)
Anticoagulation Guidelines
Neuraxial anesthesia timing:
Anticoagulation and Neuraxial Blocks
| Medication | Time Before Block | Time After Block | Notes |
|---|---|---|---|
| Aspirin | No restriction | No restriction | Safe for neuraxial |
| NSAIDs | No restriction | No restriction | Safe for neuraxial |
| Prophylactic LMWH | 12 hours | 4 hours | Daily dosing |
| Therapeutic LMWH | 24 hours | 4 hours | Twice-daily dosing |
| Unfractionated heparin (prophylactic) | 4-6 hours | 1 hour | Check aPTT if over 4 days |
| Warfarin | 5 days, INR under 1.4 | After catheter removal | Check INR before block |
| Rivaroxaban | 72 hours | 6 hours | NOACs require longer intervals |
| Apixaban | 72 hours | 6 hours | NOACs require longer intervals |
Catheter removal timing:
- Remove catheter before restarting anticoagulation
- Wait same interval as for block placement after removal
- Observe for 4 hours after removal for signs of hematoma
Complications by Block Type
Neuraxial complications:
- Epidural hematoma: under 1 in 150,000 (higher with anticoagulation)
- Epidural abscess: under 1 in 50,000
- Post-dural puncture headache: 0.5-1% (lower with pencil-point needles)
- Total spinal: 1 in 1,000 (high epidural injection)
- Urinary retention: 10-30% (resolves as block wears off)
- Hypotension: 20-40% (treat with fluids, vasopressors)
Peripheral nerve block complications:
- Nerve injury: under 1 in 1,000 (lower with ultrasound)
- Vascular injury: under 1 in 500 (usually self-limiting hematoma)
- Pneumothorax: under 1% for SCB with ultrasound
- LAST: rare; ultrasound reduces vascular puncture (RR 0.16) but trials were not powered to prove a LAST reduction
- Phrenic nerve palsy: 100% with ISB (temporary)
- Horner syndrome: 25-75% with ISB (temporary)
Risk minimization:
- Use ultrasound guidance
- Avoid injection if high resistance
- Stop if patient reports severe pain
- Respect anatomy and avoid excessive force
- Use atraumatic needles
Anatomy
Neuraxial Anatomy
Spinal Cord Levels
- Cord termination: L1-L2 in adults (L3 in children)
- Dural sac: Ends at S2
- Ligamentum flavum: Key resistance in epidural
- Epidural space: 3-5mm in lumbar region
- CSF volume: 120-150mL total
Epidural Space Contents
- Fat: Provides cushioning
- Lymphatics: Venous plexus (Batson's)
- Nerve roots: Exiting at each level
- Dural cuff: Where LA spreads
- Blood vessels: Risk of hematoma
Brachial Plexus Anatomy
Brachial Plexus Organization
| Level | Structure | Approach | Clinical Relevance |
|---|---|---|---|
| Roots (C5-T1) | Exit interscalene groove | Interscalene block | Covers shoulder surgery; spares ulnar (C8-T1) |
| Trunks | Upper, middle, lower | Supraclavicular block | Most complete arm block; pneumothorax risk |
| Divisions | Anterior/posterior | N/A (not targeted) | Transition zone behind clavicle |
| Cords | Lateral, posterior, medial | Infraclavicular block | Complete arm anesthesia; deeper access |
| Branches | Terminal nerves | Axillary block | Elbow/hand surgery; multiple injections needed |
Lower Extremity Nerve Anatomy
Lumbar Plexus (L1-L4)
- Femoral nerve: L2-L4, anterior thigh and knee
- Lateral femoral cutaneous: L2-L3, lateral thigh
- Obturator: L2-L4, medial thigh and hip
- Lies within: Psoas major muscle
- Block level: Psoas compartment or fascia iliaca
Sacral Plexus (L4-S3)
- Sciatic nerve: L4-S3, posterior thigh, leg, foot
- Posterior femoral cutaneous: S1-S3, posterior thigh
- Pudendal: S2-S4, perineum
- Sciatic divides: Popliteal fossa (tibial + common peroneal)
- Block levels: Gluteal, subgluteal, popliteal
Key Landmark Anatomy
Ultrasound has transformed regional anesthesia - nerves appear as round/oval hypoechoic structures with hyperechoic fascicular pattern ("honeycomb"). Understanding sonoanatomy is now essential.
Classification
Types of Regional Anesthesia
Classification of Regional Techniques
| Category | Technique | Indications | Duration |
|---|---|---|---|
| Neuraxial | Spinal (subarachnoid) | Lower limb, perineal surgery | 2-4 hours (single shot) |
| Neuraxial | Epidural | Labor, post-op analgesia, surgery | Continuous (catheter) |
| Neuraxial | Combined spinal-epidural | Arthroplasty, prolonged procedures | Surgical + extended |
| Peripheral | Single-shot nerve block | Day surgery, post-op analgesia | 8-24 hours |
| Peripheral | Continuous catheter block | Prolonged analgesia | Days (catheter) |
| Local | Local infiltration | Minor procedures, wound edges | 2-6 hours |
| Local | Local infiltration analgesia (LIA) | Arthroplasty, multimodal | 12-24 hours |
Upper Extremity Blocks
Shoulder and Arm Blocks
- Interscalene: Shoulder, proximal humerus
- Supraclavicular: Complete arm block
- Infraclavicular: Arm, elbow, hand
- Suprascapular: Shoulder (limited motor block)
- Axillary: Elbow, forearm, hand
Forearm and Hand Blocks
- Median at wrist: Palmar thumb, index, middle
- Ulnar at wrist: Palmar/dorsal ulnar hand
- Radial at wrist: Dorsal radial hand
- Digital blocks: Individual finger anesthesia
- WALANT: Wide awake local anesthesia no tourniquet
Lower Extremity Blocks
Hip and Thigh Blocks
- Lumbar plexus (psoas): THA, femur fractures
- Fascia iliaca: Hip fractures, THA (anterior)
- Femoral nerve: Knee surgery, femur fractures
- PENG block: Hip (pericapsular)
- Lateral femoral cutaneous: Thigh graft harvest
Knee and Below Blocks
- Adductor canal: Motor-sparing knee block
- Sciatic (multiple approaches): Below-knee surgery
- Popliteal sciatic: Foot and ankle
- Saphenous: Medial leg and ankle
- Ankle block: Foot surgery (5 nerves)
Clinical Assessment
Pre-Block Patient Assessment
History Components
- Allergies: Local anesthetics, latex, antiseptics
- Anticoagulation: Type, dose, last dose timing
- Previous blocks: Success, complications, nerve injury
- Comorbidities: Cardiac, respiratory, neurological
- Consent issues: Language, comprehension, anxiety
Physical Examination
- Infection: At proposed block site
- Anatomy: Landmarks, deformity, body habitus
- Neurological: Pre-existing deficits (document!)
- Skin: Lesions, scarring, burns
- Vascular: Peripheral vascular disease
Contraindications
Absolute vs Relative Contraindications
| Contraindication | Type | Specific Blocks Affected | Management |
|---|---|---|---|
| Patient refusal | Absolute | All | Alternative anesthesia |
| Infection at site | Absolute | All | Alternative site or GA |
| True LA allergy | Absolute | All LA blocks | Amide/ester switch or GA |
| Coagulopathy (severe) | Absolute | Deep/neuraxial blocks | Peripheral or GA |
| Therapeutic anticoagulation | Relative | Deep blocks, neuraxial | Timing per guidelines |
| Pre-existing neuropathy | Relative | Block in affected territory | Document, discuss with patient |
| Respiratory compromise | Relative | Interscalene, high neuraxial | Motor-sparing alternatives |
Consent Process
Key Discussion Points
- Procedure description: What will be done
- Expected benefits: Pain relief, opioid sparing
- Common risks: Bruising, numbness, discomfort
- Serious risks: LAST, nerve injury, infection
- Alternatives: GA, IV analgesia, other blocks
- Block duration: When sensation returns
Documentation
- Risks discussed: Specific to block type
- Pre-existing deficits: Motor/sensory exam
- Patient understanding: Confirmed
- Questions answered: Note any concerns
- Consent signed: Before sedation
Investigations
Pre-Procedural Investigations
Investigations Before Regional Anesthesia
| Investigation | When Required | Target/Normal | Action if Abnormal |
|---|---|---|---|
| INR | Warfarin use, liver disease | Less than 1.5 for neuraxial | Hold warfarin or use peripheral block |
| aPTT | UFH use | Normal (less than 40 sec) | Wait 4-6 hours post-heparin |
| Platelet count | Suspected thrombocytopenia | Greater than 80,000 for neuraxial | Consider peripheral alternatives |
| Creatinine/eGFR | DOAC use | Calculate dose adjustments | Extend hold times for renal impairment |
| ECG | Not routine | Cardiac history only | Optimize before elective surgery |
Ultrasound Assessment
Pre-Scan Benefits
- Identify anatomy: Nerve location and depth
- Vessel mapping: Avoid vascular puncture
- Pathology detection: Cysts, tumors, anomalies
- Needle trajectory: Plan optimal approach
- Patient habitus: Probe and needle selection
Sonographic Findings
- Nerves: Hypoechoic with hyperechoic rim
- Arteries: Pulsatile, non-compressible
- Veins: Compressible, non-pulsatile
- Fascia: Hyperechoic linear structures
- Muscle: Striated pattern, contractile
Management Algorithm
Surgical Technique
General Principles of Block Technique
Preparation
- Monitoring: SpO2, ECG, BP before sedation
- IV access: Essential before any block
- Resuscitation equipment: Lipid emulsion available
- Sterile technique: Skin prep, sterile probe cover
- Positioning: Comfortable, access to block site
Equipment
- Ultrasound machine: High-frequency linear (most blocks)
- Nerve stimulator: Adjunct, not mandatory with US
- Block needles: 50-100mm, echogenic preferred
- Local anesthetic: Pre-drawn, labeled syringes
- Extension tubing: For aspiration and injection
Ultrasound-Guided Technique Steps
Step-by-Step Block Procedure
| Step | Action | Key Points |
|---|---|---|
| 1. Scan | Identify target nerve/structures | Optimize image depth, gain, frequency |
| 2. Plan trajectory | Determine needle path | In-plane preferred for visualization |
| 3. Skin prep | Antiseptic, sterile field | Allow to dry; probe in sterile sheath |
| 4. Local anesthetic (skin) | Subcutaneous LA at entry point | Small volume, reduce patient discomfort |
| 5. Needle insertion | Advance under real-time visualization | Keep needle tip in view at all times |
| 6. Hydrolocation | Small test injection (D5W or LA) | Confirms tip position; opens tissue planes |
| 7. Aspiration | Check for blood before main injection | Negative aspiration does not exclude IV placement |
| 8. Incremental injection | 5mL aliquots with aspiration | Watch for spread around nerve; reposition if needed |
Common Upper Extremity Blocks
Interscalene Block
- Position: Supine, head turned away
- Probe: Lateral neck, transverse
- Target: Roots between scalene muscles
- Volume: 15-20mL
- Coverage: Shoulder, upper arm
- Limitation: Ulnar (C8-T1) often spared
Supraclavicular Block
- Position: Supine, arm at side
- Probe: Supraclavicular fossa
- Target: "Cluster of grapes" at first rib
- Volume: 20-30mL
- Coverage: Complete arm (most reliable)
- Risk: Pneumothorax (1-2% landmark, rare with US)
Common Lower Extremity Blocks
Femoral/Adductor Canal
- Femoral: Below inguinal ligament, lateral to artery
- Adductor canal: Mid-thigh, under sartorius
- Volume: 15-20mL
- Adductor advantage: Preserves quadriceps strength
- Coverage: Anterior knee, medial leg
Popliteal Sciatic
- Position: Prone, lateral, or supine with leg elevated
- Probe: Popliteal crease, transverse
- Target: Sciatic before division (or both branches)
- Volume: 20-30mL
- Coverage: Posterior knee, leg, foot (except medial)
Complications
Local Anesthetic Systemic Toxicity (LAST)
LAST Recognition and Treatment
Recognize early: Perioral tingling, metallic taste, tinnitus, confusion → progresses to seizures and cardiac arrest.
Immediate actions:
- Stop injection - call for help
- Airway management - 100% oxygen, avoid hyperventilation
- Seizure control - Benzodiazepines (avoid propofol initially)
- Cardiac arrest - Reduce epinephrine doses (max 1mcg/kg), prolonged CPR
- Lipid emulsion - 20% Intralipid: 1.5mL/kg bolus, then 0.25mL/kg/min infusion
LAST Prevention Strategies
| Strategy | Rationale | Implementation |
|---|---|---|
| Dose calculation | Stay within maximum doses | Weight-based calculation before drawing up |
| Incremental injection | Allows detection of IV injection | 5mL aliquots with aspiration and pause |
| Ultrasound guidance | Visualize needle and spread | Reduces required LA volume |
| Epinephrine marker | 1:200,000 epinephrine in LA | HR increase suggests IV injection |
| Fractionated dosing | Multiple smaller blocks | Divide dose between blocks/sites |
Differential Diagnosis: Sudden Deterioration After a Block
Acute collapse or distress shortly after local anaesthetic injection has a focused differential. Distinguishing these rapidly drives very different management.
Differential Diagnosis of Acute Deterioration Following Regional Block
| Diagnosis | Typical timing/clues | Key discriminator | Immediate action |
|---|---|---|---|
| LAST | Seconds to minutes; perioral numbness, tinnitus, seizures then arrhythmia | CNS signs precede cardiac; recent large/vascular LA dose | Stop injection, lipid emulsion 20%, ACLS |
| High/total spinal | Minutes; rising sensory level, bradycardia, hypotension, apnoea | Ascending block after neuraxial or deep injection | Airway/ventilation, fluids, vasopressors, atropine |
| Anaphylaxis | Minutes; urticaria, bronchospasm, hypotension | Skin/airway features; often to antiseptic, latex or antibiotic, not LA | Adrenaline, fluids, remove trigger |
| Vasovagal syncope | During/just after block; bradycardia, pallor, nausea, rapid recovery supine | Self-limiting, responds to position and atropine | Lie flat, reassure, atropine if bradycardic |
| Phrenic nerve palsy (ISB/SCB) | 15-30 min; dyspnoea, reduced ipsilateral air entry | Isolated respiratory symptoms after interscalene block | Oxygen, upright posture, reassurance |
| Pneumothorax (SCB/ICB) | Delayed; pleuritic pain, dyspnoea, reduced breath sounds | Supraclavicular/infraclavicular approach; confirm on imaging | Oxygen, imaging, drain if tension/large |
| Pulmonary embolism | Often hours-days post-op; hypoxia, tachycardia, pleuritic pain | Not temporally linked to injection; VTE risk factors | Oxygen, anticoagulation, CTPA |
Nerve Injury
Types of Nerve Injury
| Type | Mechanism | Prognosis | Prevention |
|---|---|---|---|
| Neuropraxia | Pressure, ischemia, stretching | Complete recovery (weeks-months) | Ultrasound guidance, low pressure injection |
| Axonotmesis | More severe pressure/trauma | Recovery possible (months) | Avoid intraneural injection |
| Neurotmesis | Needle transection (rare) | Poor; may need surgery | Keep needle tip visible; stop if paresthesia |
Other Complications
Block-Site Specific
- Interscalene: Phrenic block (100%), Horner syndrome, hoarseness
- Supraclavicular: Pneumothorax (rare with US)
- Neuraxial: Epidural hematoma, infection, PDPH
- Lumbar plexus: Epidural spread, renal injury
- Femoral: Fall risk due to quadriceps weakness
General Complications
- Failed block: Incomplete anesthesia (5-10%)
- Vascular puncture: Hematoma formation
- Infection: Rare with single-shot; higher with catheters
- Allergic reaction: Rare (esters greater than amides)
- Retained catheter: May require imaging/extraction
Postoperative Care
Post-Block Monitoring
Monitoring Requirements After Regional Anesthesia
| Setting | Block Type | Monitoring Requirements | Discharge Criteria |
|---|---|---|---|
| Day surgery (ambulatory) | Peripheral block | 30-60 min observation | Stable vitals, protective sensation returning, escort home |
| Day surgery | Spinal/epidural | Full motor recovery required | Walking, voiding, stable BP |
| Inpatient | Peripheral block | Routine ward observations | Document block resolution on chart |
| Inpatient | Continuous catheter | Daily catheter checks, motor/sensory assessment | Remove if infection signs or no longer needed |
Limb Protection
Sensory Block Precautions
- Position awareness: Prevent nerve compression
- Thermal protection: Avoid hot/cold injury
- Sharp objects: Protect insensate limb
- Weight-bearing: Crutches/support if leg blocked
- Patient education: Written instructions provided
Motor Block Considerations
- Fall risk: Femoral block affects quadriceps
- Physiotherapy timing: After block resolves for gait training
- Sling/support: For arm blocks
- DVT prophylaxis: Continue despite immobility
- Documentation: Time of expected block resolution
Discharge Instructions
Key Discharge Information
- Block duration: Expected time for sensation/movement to return
- Limb protection: Keep insensate limb safe from injury
- Pain medication: Take before block wears off
- When to seek help: Numbness greater than 24 hours, increasing weakness, signs of infection
- Follow-up: Contact number for concerns
Outcomes
Efficacy of Regional Anesthesia
Pain Control Outcomes
Analgesia Outcomes by Block Type
| Block/Technique | Surgery | Pain Score Reduction | Duration of Effect |
|---|---|---|---|
| Interscalene block | Shoulder surgery | VAS reduced by 3-4 points | 12-18 hours |
| Adductor canal block | TKA | VAS reduced by 2-3 points | 12-24 hours |
| Popliteal sciatic + saphenous | Foot/ankle surgery | Excellent analgesia | 18-24 hours |
| Fascia iliaca | Hip fracture | Reduces opioid in ED and periop | 8-12 hours |
| Continuous catheter (any site) | Major surgery | Sustained analgesia | Days (while catheter in situ) |
Quality Improvement Metrics
Positive Outcomes
- Opioid sparing: Reduced PONV, faster recovery
- Early mobilization: Especially with motor-sparing blocks
- Shorter hospital stay: In enhanced recovery programs
- Patient satisfaction: Consistently higher scores
- Chronic pain prevention: Some evidence for reduced incidence
Complications to Track
- Block failure rate: Target less than 5%
- LAST incidence: Should be rare with proper technique
- Nerve injury: Document and track; most transient
- Falls: Monitor with femoral/motor blocks
- Catheter infections: Track if using continuous blocks
Evidence Base
Neuraxial vs General Anaesthesia for Hip/Knee Arthroplasty
- Large US cohort (382,236 primary hip/knee arthroplasties, 2006-2010)
- Neuraxial anaesthesia: lower 30-day mortality (0.10% vs 0.18% general)
- For TKA, general anaesthesia carried higher adjusted mortality (OR 1.83, 95% CI 1.08-3.1)
- Neuraxial associated with fewer in-hospital complications, shorter stay and lower cost
Adductor Canal Block vs Femoral Nerve Block and Quadriceps Strength
- Randomised, double-blind, placebo-controlled crossover study in healthy volunteers (n=11 analysed)
- Quadriceps strength fell only 8% from baseline with ACB vs 49% with FNB
- Ambulation test performance preserved with ACB compared with FNB
- Demonstrated the predominantly sensory nature of the adductor canal block
Ultrasound vs Nerve Stimulation for Peripheral Nerve Block
- Systematic review and meta-analysis of 13 randomised controlled trials
- Ultrasound reduced block failure (RR 0.41, 95% CI 0.26-0.66)
- Ultrasound reduced vascular puncture (RR 0.16, 95% CI 0.05-0.47)
- Faster onset (29% shorter) and longer block duration (25% longer) than nerve stimulation
Treatment of Local Anaesthetic Systemic Toxicity (LAST)
- Narrative review establishing the modern LAST treatment paradigm
- Airway, oxygenation and seizure suppression are the foundation of resuscitation
- Lipid emulsion should be considered early once LAST is suspected
- Recommends avoiding vasopressin and using only small doses of adrenaline
100% Incidence of Hemidiaphragmatic Paresis with Interscalene Block
- Ultrasonography showed ipsilateral hemidiaphragmatic paresis in all 13 patients after interscalene block
- Paresis developed within 5 minutes (most by 2 minutes) of injection
- Diaphragmatic motion returned to normal within 3-5 hours as the block resolved
- Established phrenic palsy as an essentially inevitable consequence of the classic interscalene block
ASRA Local Anaesthetic Systemic Toxicity Checklist (2020)
- Updated ASRA cognitive aid for managing LAST, revised from simulation studies and user feedback
- Reinforces lipid emulsion 20% as the cornerstone pharmacological therapy
- Recommends reduced adrenaline dosing and avoidance of vasopressin, calcium channel blockers and beta-blockers
- Endorses prolonged resuscitation and consideration of cardiopulmonary bypass in refractory arrest
Regional Anesthesia Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: LAST Recognition and Management
"You are performing an interscalene block for a shoulder arthroscopy. After injecting 15 mL of 0.5% ropivacaine, the patient suddenly reports perioral numbness and ringing in the ears. What is happening and how do you manage this?"
Scenario 2: Block Selection for Total Knee Arthroplasty
"You are planning anesthesia for a 68-year-old patient undergoing primary total knee arthroplasty as part of an ERAS protocol. The surgeon wants the patient ambulating on the day of surgery. What regional anesthesia options would you consider and why?"
Scenario 3: Interscalene Block Complications
"You have just performed an ultrasound-guided interscalene block for shoulder arthroscopy. Thirty minutes later, the patient reports difficulty breathing and feels short of breath. Oxygen saturation is 92% on room air. What are your differential diagnoses and management?"
MCQ Practice Points
Clinical Pearl
Q: What is Local Anesthetic Systemic Toxicity (LAST) and how is it treated?
A: LAST occurs when local anesthetic reaches toxic plasma levels, affecting CNS (tinnitus, circumoral numbness, seizures, coma) and cardiovascular system (arrhythmias, cardiovascular collapse). Treatment: Stop injection, call for help, manage airway, give Intralipid 20% (1.5 mL/kg bolus then infusion). Avoid propofol (lipid-soluble) and vasopressin. Bupivacaine is most cardiotoxic; ropivacaine and levobupivacaine are safer alternatives.
Clinical Pearl
Q: What are the maximum safe doses of commonly used local anesthetics?
A: Lidocaine: 4 mg/kg plain, 7 mg/kg with adrenaline. Bupivacaine: 2 mg/kg (150 mg max, regardless of adrenaline). Ropivacaine: 3 mg/kg (225 mg max). Prilocaine: 6 mg/kg (can cause methaemoglobinaemia). Levobupivacaine: 2 mg/kg. For regional blocks, total dose matters more than concentration. Always calculate dose before injection.
Clinical Pearl
Q: What nerve block provides anesthesia for knee arthroscopy and TKA?
A: Adductor canal block (saphenous nerve) combined with iPACK (interspace between popliteal artery and capsule of knee) provides excellent analgesia while preserving quadriceps strength. Alternative: femoral nerve block gives good analgesia but causes quadriceps weakness (fall risk). Sciatic block adds posterior knee coverage. For TKA, multimodal including periarticular infiltration is standard.
Clinical Pearl
Q: What blocks comprise the brachial plexus approaches and what are their indications?
A: Interscalene: Shoulder/proximal humerus (C5-6 predominant). Risks: phrenic nerve palsy (100%), Horner's, recurrent laryngeal. Supraclavicular: Arm/elbow ("spinal of the arm"). Risk: pneumothorax. Infraclavicular: Forearm/hand. Axillary: Hand/forearm - safest, no pneumothorax risk. Choose level based on surgical site and risk tolerance. Ultrasound guidance is now standard for all approaches.
Clinical Pearl
Q: What are the contraindications to neuraxial anesthesia (spinal/epidural)?
A: Absolute: Patient refusal, coagulopathy/anticoagulation (ASRA guidelines for timing), infection at injection site, severe hypovolemia, increased ICP. Relative: Pre-existing neurological disease, severe spinal stenosis, previous spinal surgery (relative for epidural). For anticoagulation: stop warfarin 5 days (INR less than 1.4), LMWH 12-24 hours, heparin 4-6 hours, DOACs 3-5 days depending on agent and renal function.
Guidelines, Registries & Global Practice
OrthoVellum is a worldwide resource: regional anaesthesia is practised on every continent, and the major society guidance is largely convergent. The differences a candidate is most likely to be examined on relate to anticoagulation timing, LAST rescue protocols, and the local availability of ultrasound and lipid emulsion.
Epidemiology and burden
- Local anaesthetic systemic toxicity (LAST) is the most feared complication of regional anaesthesia. Contemporary registry and audit data place clinically apparent LAST in the low single digits per 10,000 peripheral nerve blocks, with severe cardiac events rarer still.
- Permanent peripheral nerve injury after blockade is rare (of the order of 0.02-0.04% at long-term follow-up), with most postoperative neurological deficits being transient and multifactorial (surgery, tourniquet, positioning).
- Adoption of ultrasound guidance has risen to near-universal in high-resource settings; nerve stimulation and landmark techniques remain important where ultrasound is unavailable.
Major guidelines, side by side
Society Guidance on Regional Anaesthesia
| Body (region) | Focus | Key recommendation | Evidence basis |
|---|---|---|---|
| ASRA (USA) | Neuraxial + anticoagulation | Agent-specific hold/restart intervals (e.g. prophylactic LMWH 12 h before, therapeutic 24 h; DOACs typically 72 h) | Consensus, evidence-based (4th ed, Horlocker 2018) |
| ASRA (USA) | LAST | Lipid emulsion 20% first-line; reduced adrenaline dosing; avoid vasopressin; displayed checklist | Consensus advisory + checklist (2020) |
| ESAIC / ESRA (Europe) | Neuraxial + antithrombotics | Broadly aligned intervals; some European thresholds differ for specific agents and renal impairment | European consensus guidelines |
| AAGBI / RA-UK (UK & Ireland) | LAST management; Stop Before You Block | Quick reference LAST guideline; pre-block pause to prevent wrong-side block | Consensus / safety initiative |
| WHO (global) | Procedural safety | Surgical Safety Checklist and team time-out before invasive procedures | Global standard |
Where guidelines genuinely differ
The headline principles (ultrasound where available, lipid emulsion immediately available, respect maximum doses, document pre-block neurology) are universal. Anticoagulation intervals are the main area of divergence between ASRA and European bodies, particularly for DOACs and in renal impairment — always quote the local/most recent guideline and the principle that the risk is bleeding into a confined space for neuraxial and deep blocks.
LAST rescue: the global consensus
- 20% lipid emulsion is the agreed first-line therapy worldwide and should be stocked wherever local anaesthetic is injected in potentially toxic doses.
- Bolus 1.5 mL/kg then infusion 0.25 mL/kg/min, with repeat boluses for persistent instability and an approximate upper limit of 10-12 mL/kg.
- Reduce adrenaline dosing, avoid vasopressin, calcium channel blockers and beta-blockers, and anticipate prolonged resuscitation with consideration of cardiopulmonary bypass in refractory arrest.
Registry and practice variation
- Regional anaesthesia is not implant-based, so it is not tracked by the arthroplasty joint registries (NJR, AOANJRR, AJRR, SHAR); registry insight instead comes from national audit projects and adverse-event databases.
- High- vs limited-resource settings: where ultrasound machines, single-use block needles or lipid emulsion are scarce, nerve stimulation and landmark spinal anaesthesia remain mainstays, and drug selection favours cheaper agents (lidocaine, bupivacaine) over ropivacaine/levobupivacaine.
- ERAS integration is global: regional anaesthesia is a cornerstone of enhanced recovery for arthroplasty everywhere, with motor-sparing combinations (ACB + IPACK for TKA; PENG or fascia iliaca for hip; interscalene for shoulder) reducing opioid use and enabling early mobilisation.
REGIONAL ANESTHESIA TECHNIQUES
Clinical summary
LAST Management
- •Early signs: perioral numbness, metallic taste, tinnitus
- •Late signs: seizures, arrhythmias, cardiac arrest
- •STOP injecting immediately
- •Lipid emulsion 20%: 1.5 mL/kg bolus, then 0.25 mL/kg/min
- •Prolonged CPR may be needed (over 60 minutes)
- •Avoid vasopressin, propofol is NOT lipid therapy
Upper Extremity Blocks
- •Interscalene: shoulder (C5-C7, 100% phrenic palsy)
- •Supraclavicular: elbow/forearm (complete block, low pneumothorax risk with US)
- •Infraclavicular: elbow/hand (cords, good for catheters)
- •Axillary: hand/wrist (safe, no pneumothorax, multi-injection)
- •15-25 mL per block, 12-18 hour duration
Lower Extremity Blocks
- •Femoral: anterior thigh/knee (50% quadriceps weakness)
- •ACB: knee analgesia (motor-sparing, 8% quad weakness)
- •IPACK: posterior knee capsule (no motor block)
- •Sciatic: posterior thigh, leg/foot below knee
- •Popliteal: ankle/foot (foot drop expected)
- •PENG: hip joint (motor-sparing hip block)
Block Selection by Surgery
- •Shoulder arthroscopy: Interscalene
- •TKA: ACB + IPACK (motor-sparing for ERAS)
- •THA: PENG or fascia iliaca (motor-sparing)
- •Ankle ORIF: Popliteal sciatic + saphenous
- •Hand surgery: Axillary or supraclavicular
- •Femur fracture: Femoral or fascia iliaca
Ultrasound Benefits
- •Reduced block failure (RR 0.41 vs nerve stimulation)
- •Reduced vascular puncture (RR 0.16 vs nerve stimulation)
- •Faster onset (29%) and longer block duration (25%)
- •Direct visualization of nerves, needle, spread
- •Real-time adjustment prevents intravascular injection
- •Standard of care for peripheral nerve blocks
Anticoagulation Timing
- •Aspirin/NSAIDs: no restriction for neuraxial
- •Prophylactic LMWH: 12 hours before, 4 hours after
- •Therapeutic LMWH: 24 hours before, 4 hours after
- •Warfarin: 5 days before, INR under 1.4
- •NOACs (rivaroxaban, apixaban): 72 hours before, 6 hours after
- •Remove catheter before restarting anticoagulation
Summary
Regional anesthesia is a cornerstone of modern orthopaedic perioperative care, offering superior analgesia, reduced opioid consumption, and facilitation of early mobilization. The evolution from landmark-based techniques to ultrasound-guided approaches has dramatically improved safety and efficacy.
Key exam points:
- LAST is a life-threatening complication treated with lipid emulsion 20%
- Ultrasound guidance is now standard of care for peripheral nerve blocks
- Motor-sparing blocks (ACB, IPACK, PENG) enable ERAS protocols and same-day mobilization
- Block selection must match surgical site and patient goals
- Anticoagulation timing is critical for neuraxial safety
Future directions include development of novel motor-sparing blocks, longer-acting local anesthetics, and integration of continuous catheter techniques with ambulatory surgery protocols.