Posterior Capsulodesis and Infraspinatus Tenodesis | Engaging Hill-Sachs Lesion | Anterior Instability
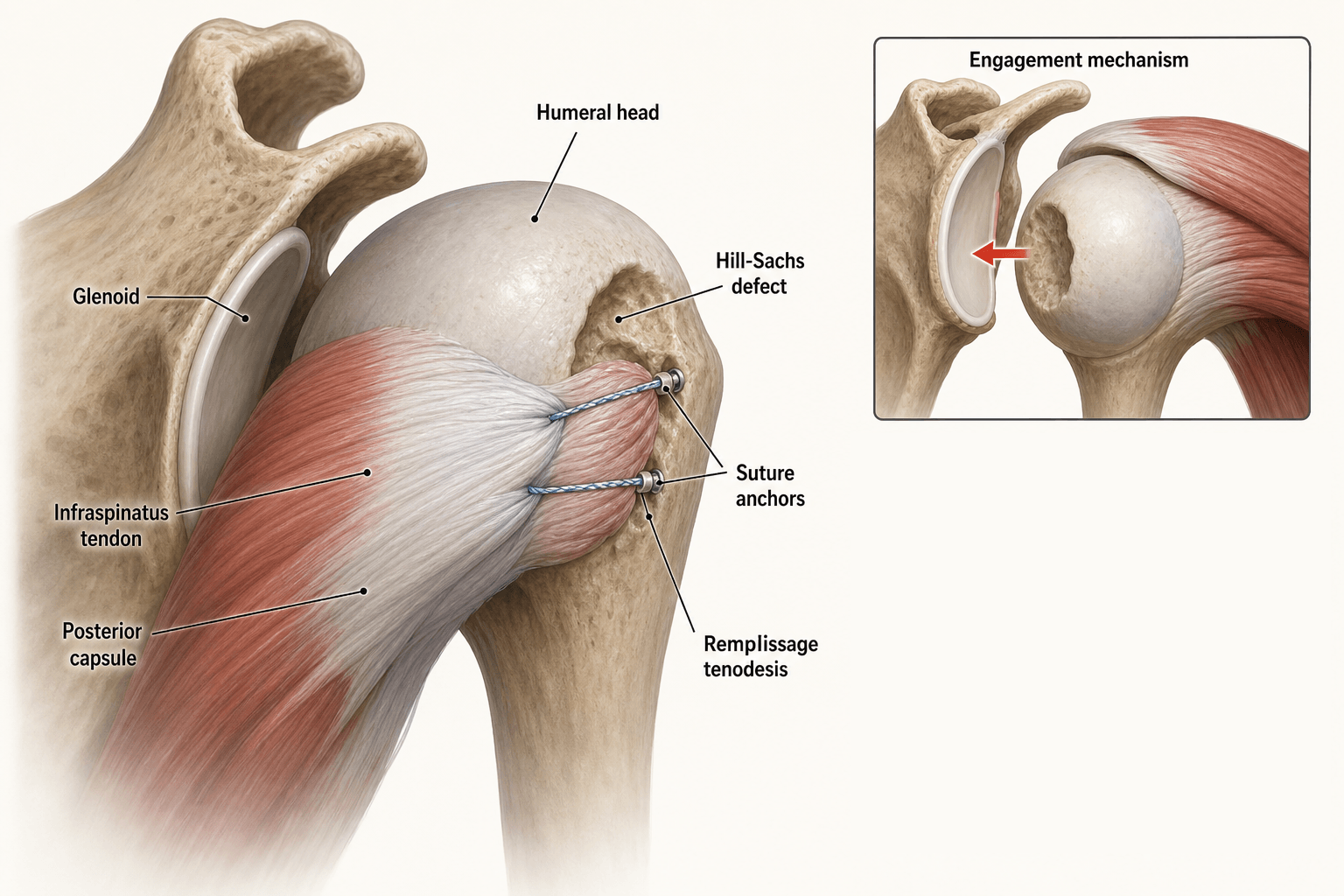
- Remplissage = arthroscopic posterior capsulodesis and infraspinatus tenodesis into Hill-Sachs defect
- Converts engaging intra-articular Hill-Sachs into non-engaging extra-articular lesion
- Indicated when glenoid track width is less than Hill-Sachs interval (off-track lesion)
- Combined with anterior Bankart repair in the same procedure
- Main trade-off: postoperative loss of external rotation (typically 8-14 degrees)
- “Glenoid track = glenoid width minus anterior rim bone loss minus posterior humeral offset
- “An engaging Hill-Sachs lesion is one that contacts the anterior glenoid rim in arm abduction and external rotation
- “Remplissage is contraindicated as a stand-alone procedure without Bankart repair
- “Stiffness is the primary complication; counsel patients preoperatively about external rotation loss
Glenoid track = 84 percent of glenoid width minus anterior glenoid bone loss. If the Hill-Sachs interval (width of Hill-Sachs plus bony bridge) exceeds the glenoid track, the lesion is off-track (engaging). Remplissage addresses the Hill-Sachs side; it does not correct glenoid bone loss.
Posterior capsule and infraspinatus tendon are tenodesed into the Hill-Sachs defect. This extra-articularises the lesion so the humeral head articular surface no longer engages the glenoid rim. The infraspinatus acts as a biological bumper.
Off-track bipolar bone loss with glenoid loss under 20-25 percent. If glenoid bone loss exceeds 25 percent of glenoid width, remplissage is insufficient and a Latarjet or glenoid bone graft is required instead.
Mean external rotation loss is 8-14 degrees. Most patients compensate and return to sport, but overhead athletes and those requiring full ER should be counselled carefully. Stiffness is the accepted cost of stability.
- Glenoid Track Status
- On-track (glenoid track greater than Hill-Sachs interval)
- Procedure
- Bankart repair alone
- Key Decision
- No remplissage needed
- Glenoid Track Status
- Off-track (glenoid track less than Hill-Sachs interval)
- Procedure
- Bankart + remplissage
- Key Decision
- Remplissage addresses Hill-Sachs; Bankart addresses labrum
- Glenoid Track Status
- Off-track with borderline glenoid loss
- Procedure
- Bankart + remplissage (marginally suitable)
- Key Decision
- Latarjet may be safer if glenoid loss approaching 25 percent
- Glenoid Track Status
- Glenoid track cannot be calculated reliably
- Procedure
- Latarjet or glenoid bone graft
- Key Decision
- Remplissage contraindicated as primary solution
TRACKGlenoid Track Calculation
Hook:TRACK the glenoid width, subtract rim loss, apply 84 percent, compare to Hill-Sachs, and decide!
FILLRemplissage Surgical Steps
Hook:FILL the defect with capsule and infraspinatus to prevent engagement!
Overview and Epidemiology
The remplissage procedure is one of the most significant advances in arthroscopic shoulder instability surgery over the past two decades. Before the glenoid track concept, surgeons struggled to decide when a Hill-Sachs lesion was clinically significant. Off-track engaging Hill-Sachs lesions are a major cause of recurrent instability after isolated Bankart repair. Remplissage converts these intra-articular lesions into extra-articular defects, dramatically reducing recurrence without requiring open bone grafting.
- Present in 40-90 percent of anterior shoulder dislocations
- First-time dislocation: Hill-Sachs visible on plain AP in 40-70 percent, on CT in up to 90 percent
- Recurrent instability: larger and more engaging lesions, approaching 100 percent prevalence
- Bipolar bone loss (combined Hill-Sachs and glenoid defect) present in up to 50 percent of revision cases
- Small non-engaging Hill-Sachs: typically irrelevant, Bankart repair alone sufficient
- Large engaging Hill-Sachs: drives recurrence risk despite labral repair
- Critical-size lesions: the defect engages the anterior glenoid rim in abduction/external rotation, creating a bony block to reduction
- Remplissage: addresses the humeral side of bipolar bone loss arthroscopically
Pathophysiology
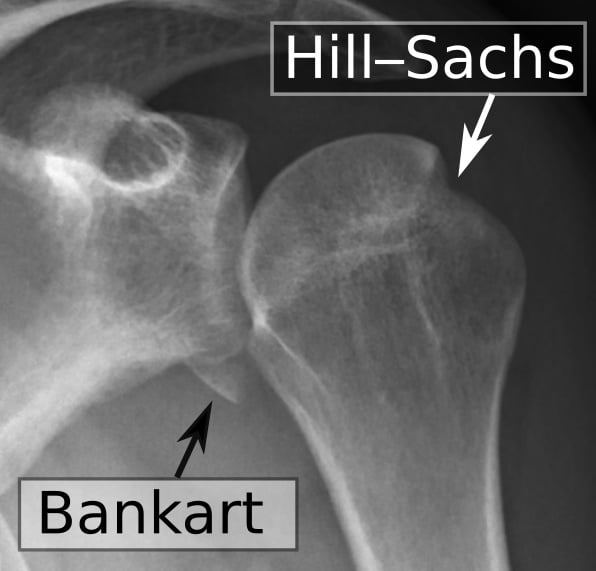
When the shoulder dislocates anteriorly, the posterosuperior humeral head impacts the anterior glenoid rim, producing a compression fracture (Hill-Sachs lesion). The position of the arm at the moment of impact (typically abduction and external rotation) determines the orientation of the defect. A lesion is engaging when, during arm abduction and external rotation, the Hill-Sachs defect aligns with the anterior glenoid rim such that the rim falls within the defect, creating a bony barrier to concentric reduction and predisposing to recurrent dislocation. The glenoid track concept quantifies this risk geometrically.
- Characteristics
- Small impression fracture, far from articular margin
- Engagement
- Non-engaging
- Clinical Significance
- No impact on surgical decision; Bankart repair alone
- Characteristics
- Larger defect, may approach articular margin
- Engagement
- May engage depending on glenoid track
- Clinical Significance
- Assess with glenoid track; remplissage if off-track
- Characteristics
- Extensive defect, occupies significant humeral head arc
- Engagement
- Engaging (off-track)
- Clinical Significance
- Requires remplissage, Latarjet, or humeral head allograft
Normal glenoid track: 84 percent of glenoid width (approximately 23-25 mm for a 28-30 mm glenoid)
Anterior glenoid bone loss narrows the track: Each millimetre of anterior rim loss reduces the glenoid track by the same amount
Hill-Sachs interval: measured as Hill-Sachs width plus the bony bridge posterior to it
Off-track: Hill-Sachs interval greater than glenoid track width
Extra-articularisation: Capsule and infraspinatus fill the defect, so the articular surface bypasses the anterior rim
Humeral head shifts medially: The effective radius of the humeral head in the remplissage zone decreases, widening the functional glenoid track
Infraspinatus tenodesis effect: The tethered infraspinatus creates a posterior soft tissue buttress resisting anterior translation
Combined with Bankart: Bankart restores the anterior bumper; remplissage prevents humeral engagement
The exact mirror image of the remplissage problem occurs in posterior instability, and examiners love the parallel:
- The lesion: a reverse Hill-Sachs (McLaughlin lesion) is an impaction fracture of the anteromedial humeral head, produced when the head locks against the posterior glenoid rim in a posterior dislocation (classic causes: seizure, electric shock, or major trauma - the "3 E's"). An engaging reverse Hill-Sachs causes recurrent/locked posterior instability.
- The classic trap: a locked posterior dislocation is the most commonly missed major joint dislocation; the AP looks deceptively normal ("light-bulb" sign, loss of the half-moon overlap) - get an axillary or CT view.
- The "posterior remplissage" - the McLaughlin procedure: for a moderate (roughly 20-40 percent) reverse Hill-Sachs, the subscapularis tendon is transferred into the defect (original McLaughlin); the modified McLaughlin (Neer) transfers the lesser tuberosity with the attached subscapularis into the defect. This fills/extra-articularises the anteromedial defect exactly as the infraspinatus/capsule fills the (anterior-instability) Hill-Sachs in a remplissage.
- Bigger defects: as with the anterior side, very large (over ~40 percent) reverse Hill-Sachs or chronic locked dislocations need structural reconstruction (allograft, rotational osteotomy) or arthroplasty.
Exam point: remplissage (infraspinatus into posterosuperior Hill-Sachs, anterior instability) and the McLaughlin/modified McLaughlin (subscapularis/lesser tuberosity into anteromedial reverse Hill-Sachs, posterior instability) are mirror-image defect-filling operations.
Classification and Types
Glenoid Track Classification (Itoi, 2012)
- Glenoid Track vs Hill-Sachs Interval
- Glenoid track greater than Hill-Sachs interval
- Engagement Risk
- Non-engaging
- Management Implication
- Bankart repair alone; no remplissage needed
- Glenoid Track vs Hill-Sachs Interval
- Glenoid track less than Hill-Sachs interval
- Engagement Risk
- Engaging
- Management Implication
- Remplissage + Bankart; or Latarjet if glenoid loss large
The on-track/off-track system replaced older percentage-based Hill-Sachs size classifications because it accounts for the interaction between humeral and glenoid bone loss rather than measuring the Hill-Sachs in isolation.
Clinical Assessment
- Dislocation events: Number, mechanism, direction, reduction method (self vs hospital)
- Instability pattern: position of arm at dislocation (typically abduction + external rotation)
- Apprehension: Does the patient avoid specific arm positions (e.g. overhead throwing, reaching back)
- Prior surgery: Bankart repair alone that failed suggests significant bone loss
- Sport and functional demands: Overhead athletes, manual workers, contact athletes
- Apprehension test: Anterior apprehension in abduction/external rotation
- Relocation test: Posterior force on humeral head relieves apprehension
- Sulcus sign: Inferior laxity (associated with multidirectional instability)
- Range of motion: Document external rotation and internal rotation preoperatively (baseline for postoperative comparison)
- Rotator cuff: Infraspinatus strength (remplissage affects this muscle)
Do not plan surgery for recurrent instability without quantifying bone loss on both sides. At minimum, obtain an axillary lateral X-ray and a CT scan with 3D reconstruction. Measure glenoid bone loss using the best-fit circle method on the en face glenoid view. Measure Hill-Sachs width and orientation. Calculate the glenoid track. Operating without bone loss assessment risks performing an isolated Bankart repair that fails in the presence of an off-track lesion.
- What It Shows
- Hill-Sachs (AP), glenoid morphology (axillary)
- Accuracy
- Moderate; underestimates bone loss
- Role in Remplissage Planning
- Initial screening; axillary view essential
- What It Shows
- Anterior glenoid rim detail
- Accuracy
- Good for anterior glenoid fractures
- Role in Remplissage Planning
- Acute bony Bankart assessment
- What It Shows
- Precise glenoid width, bone loss, Hill-Sachs size and orientation
- Accuracy
- Gold standard for bone loss quantification
- Role in Remplissage Planning
- Mandatory preoperative planning; glenoid track calculation
- What It Shows
- Labral integrity, capsular status, rotator cuff
- Accuracy
- Good for soft tissue; inferior for bone
- Role in Remplissage Planning
- Assess labral tear pattern; complement CT for bone
On the en face 3D CT reconstruction of the glenoid, fit a circle to the inferior glenoid. Measure the width of the missing anterior rim. Glenoid bone loss (percentage) equals (defect width divided by glenoid diameter) multiplied by 100. The same scan allows measurement of Hill-Sachs width and calculation of the glenoid track. A normal inferior glenoid AP diameter is approximately 28-30 mm.
The glenoid track decides whether the Hill-Sachs needs addressing; the Instability Severity Index Score (ISIS, Balg and Boileau) is the complementary preoperative tool that predicts failure of an arthroscopic (Bankart +/- remplissage) repair and flags patients who should go to a Latarjet/bone procedure instead:
- It is a 10-point score from six preoperative factors (history + examination + plain radiographs): age under 20 at surgery; participation in competitive sport; contact or overhead/forced-overhead sport; shoulder hyperlaxity; a Hill-Sachs visible on an external-rotation AP radiograph; and loss of the normal glenoid contour (sclerotic line/bone loss) on AP.
- The threshold: a score of more than 6 points predicts an unacceptably high recurrence after arthroscopic Bankart repair, and such patients are better served by an open bone-block (Latarjet) procedure; 6 or below supports an arthroscopic approach.
- How it complements the glenoid track: the track tells you the lesion is off-track and the Hill-Sachs needs filling; the ISIS tells you whether the overall patient/risk profile is still safe for arthroscopic surgery at all. Use them together - an off-track lesion with a high ISIS pushes toward Latarjet rather than Bankart + remplissage.
Exam point: quote the ISIS as a 10-point preoperative score with a cut-off of over 6 favouring Latarjet over arthroscopic repair - it is the classic answer to "how do you decide arthroscopic versus open for recurrent anterior instability?"
Investigations
Preoperative Imaging Protocol
Views: True AP (Grashey), axillary lateral, scapular lateral, Stryker notch
Look for: Hill-Sachs lesion on AP and Stryker notch, glenoid morphology on axillary, bony Bankart fragment, reverse Hill-Sachs (posterior dislocation)
Limitation: Underestimates bone loss by 20-50 percent compared to CT
Technique: Thin-slice CT (1 mm slices) of both shoulders; 3D surface reconstruction en face and rotated views
Glenoid bone loss: Best-fit circle method on inferior glenoid en face view
Hill-Sachs: Measure width, depth, and orientation; calculate Hill-Sachs interval
Glenoid track: 0.84 multiplied by (glenoid width minus anterior rim bone loss); compare to Hill-Sachs interval
Threshold for remplissage: Off-track lesion with Hill-Sachs interval greater than glenoid track
Indication: Assess labral tear pattern, capsular laxity, rotator cuff integrity
Use when: Planning combined procedures; concerns about SLAP, posterior labral tears, or rotator cuff pathology
Note: MRI underestimates bone loss; do not use MRI alone for remplissage decision-making
CT with 3D reconstruction is the mandatory investigation before deciding on remplissage. The entire remplissage decision rests on the glenoid track calculation, which requires precise measurements of both glenoid and humeral bone loss that are unreliable on plain radiographs alone. Always compare both shoulders on the same CT to account for individual glenoid size variation.
Management Algorithm
On-Track Lesion: Bankart Repair Alone
Criteria: Glenoid track width is greater than or equal to Hill-Sachs interval (on-track)
Procedure: Arthroscopic anterior Bankart repair with suture anchors
Rationale: The Hill-Sachs lesion is non-engaging. Restoring the anterior labral bumper prevents the humeral head from translating far enough anteriorly for the Hill-Sachs to contact the glenoid rim. No additional humeral-side procedure is needed.
Surgical Protocol: Isolated Bankart Repair
Setup: Lateral decubitus or beach chair; lateral decubitus preferred for remplissage access
Traction: Lateral traction with 10 degrees abduction and 20 degrees forward flexion
Portals: Standard posterior viewing portal, anterior working portal, anterosuperior (Wilmington) portal for anchor placement, posterolateral portal for remplissage access
Inspection: Labral tear pattern (Bankart, ALPSA, Perthes), capsular laxity, Hill-Sachs size
Dynamic assessment: Engage the Hill-Sachs against anterior glenoid in abduction/external rotation under arthroscopic visualisation
Probe measurements: Estimate Hill-Sachs width; correlate with CT measurements
Preparation: Debride labral edge to bleeding bone on glenoid neck
Anchors: 3-4 suture anchors along anterior glenoid rim from inferior to 4-5 o'clock position
Suture passage: Pass sutures through labrum using suture shuttles; shift labrum medially to restore bumper effect
Capsular plication: Address capsular laxity with side-to-side capsular stitches if needed
Immobilisation: Sling for 4-6 weeks; no passive external rotation beyond neutral for 3 weeks
Active assisted ROM: Start at week 3, avoid ER beyond 30 degrees for 6 weeks
Strengthening: Start at 6-8 weeks; return to contact sport at 6-9 months
Complications
- Incidence
- 8-14 degrees mean; up to 20-30 degrees in some series
- Risk Factors
- Large remplissage surface area, aggressive capsular plication
- Management
- Physiotherapy; MUA if refractory at 6-12 months; counsel preoperatively
- Incidence
- 4-17 percent at 2-10 years
- Risk Factors
- Large glenoid bone loss, inadequate remplissage, hyperlaxity, early return to sport
- Management
- Revision with Latarjet or glenoid bone graft; assess bone loss again on CT
- Incidence
- Rare
- Risk Factors
- Malpositioned anchors outside Hill-Sachs defect, anchor loosening
- Management
- Arthroscopic removal if symptomatic; careful anchor placement prevents
- Incidence
- Low incidence but reported
- Risk Factors
- Over-tensioning of infraspinatus tenodesis, aggressive postoperative ER
- Management
- Repair if tendon rupture; rehabilitation for weakness
- Incidence
- Up to 10-20 percent in early recovery
- Risk Factors
- Posterior capsule irritation, remplissage inflammation
- Management
- NSAIDs, physiotherapy; usually resolves by 3-6 months
Loss of external rotation is the expected trade-off of remplissage. Most patients lose 8-14 degrees and compensate functionally, but overhead athletes (throwers, volleyball, racquet sports) may be unable to return to their pre-injury performance level. A thorough preoperative discussion about the stiffness-stability trade-off is mandatory. For patients who cannot accept ER loss, Latarjet may be the better procedure.
SEALRemplissage Outcomes and Complications
Hook:SEAL the joint with remplissage: Stability gained, External rotation lost, Arthritis uncertain, Latarjet when glenoid loss is large!
Outcomes and Prognosis
- Procedure
- Isolated Bankart repair
- Recurrence Rate
- 5-10 percent at 2-5 years
- Functional Outcome
- Good to excellent (Rowe 85-95)
- External Rotation Loss
- Minimal (less than 5 degrees)
- Procedure
- Bankart + remplissage
- Recurrence Rate
- 4-8 percent at 2-5 years
- Functional Outcome
- Good to excellent (Rowe 80-90)
- External Rotation Loss
- 8-14 degrees mean
- Procedure
- Bankart + remplissage or Latarjet
- Recurrence Rate
- 8-17 percent (remplissage); 2-5 percent (Latarjet)
- Functional Outcome
- Moderate to good
- External Rotation Loss
- 8-14 degrees (remplissage); variable (Latarjet)
- Procedure
- Latarjet or glenoid bone graft
- Recurrence Rate
- 2-10 percent at 5-10 years
- Functional Outcome
- Good (Latarjet)
- External Rotation Loss
- Variable; subscapularis function key
Best prognosis: Off-track Hill-Sachs with minimal glenoid bone loss (less than 10 percent), first or second dislocation, compliant rehabilitation, contact sport avoidance during recovery
Poorer prognosis: Multiple recurrences, glenoid bone loss over 15-20 percent treated with remplissage alone, hyperlaxity, early return to contact sport, inadequate remplissage coverage
Key thresholds: Glenoid bone loss over 20-25 percent (consider Latarjet); external rotation loss over 20 degrees (may be functionally limiting for overhead athletes)
Guidelines, Registries and Global Practice
- Anterior shoulder instability affects 1-2 percent of the general population
- Hill-Sachs lesions are present in 40-90 percent of first-time dislocations (higher with imaging sensitivity)
- Engaging Hill-Sachs requiring remplissage is estimated in 10-20 percent of operative instability cases
- Bipolar bone loss (combined Hill-Sachs and glenoid defect) is a significant predictor of recurrence after isolated Bankart repair
- High-resource centres: Routine 3D CT for bone loss quantification; arthroscopic remplissage as standard for off-track lesions with small glenoid loss
- Limited-resource settings: CT may not be available; clinical judgement and plain radiographs used; decision to use remplissage may be intraoperative based on arthroscopic engagement testing
- Global trend: Arthroscopic remplissage has largely replaced open humeral plasty or partial humeral head resurfacing for engaging Hill-Sachs
- Remplissage Indication
- Off-track Hill-Sachs with glenoid loss less than 20-25 percent; combined with Bankart
- Bone Loss Assessment
- 3D CT recommended; glenoid track method preferred
- Alternative when Remplissage Insufficient
- Latarjet for glenoid loss over 20-25 percent or large engaging Hill-Sachs with failed remplissage
- Remplissage Indication
- Remplissage is an accepted arthroscopic option for off-track lesions
- Bone Loss Assessment
- CT with 3D reconstruction standard; proportion method or glenoid track method
- Alternative when Remplissage Insufficient
- Latarjet or Eden-Hybinette bone block for significant glenoid deficiency
- Remplissage Indication
- Part of the algorithm for bipolar bone loss; humeral-side bone loss addressed with remplissage when glenoid loss is small
- Bone Loss Assessment
- Precise CT measurement of both sides; 25 percent glenoid loss as key threshold
- Alternative when Remplissage Insufficient
- Coracoid transfer (Latarjet) or iliac crest bone graft for glenoid deficiency
- Remplissage Indication
- Remplissage included in instability guidelines for engaging Hill-Sachs; counsel on stiffness trade-off
- Bone Loss Assessment
- 3D CT where available; proportion method accepted
- Alternative when Remplissage Insufficient
- Latarjet as primary option for large glenoid defects or contact athletes
Shoulder instability registries (such as the Norwegian Shoulder Instability Registry and the Danish Shoulder Arthroscopy Registry) track Bankart and Latarjet procedures but do not yet consistently separate remplissage cases as a distinct category. The evidence base for remplissage is predominantly level 4 (retrospective case series) with no published randomised controlled trials comparing Bankart plus remplissage versus Latarjet for off-track bipolar bone loss. This is a recognised evidence gap.
Controversies and Areas of Uncertainty
No head-to-head randomised trial exists. Latarjet provides a bony block and may have lower recurrence in the setting of significant glenoid loss, but carries higher complication rates (nerve injury, graft problems, subscapularis dysfunction). Remplissage is arthroscopic, lower morbidity, but trades stiffness for stability. Surgeon preference and patient demands often dictate the choice.
Theoretical concern exists that the tenodesed infraspinatus rubbing against the posterior glenoid may accelerate degenerative change. Mid-term series (up to 10 years) have not shown significant arthritis progression, but truly long-term data (over 15-20 years) are not yet available.
Remplissage is almost always combined with Bankart repair. Performing isolated remplissage without restoring the anterior labral bumper is generally considered insufficient for anterior instability. However, rare case reports describe isolated remplissage in revision settings where the anterior labrum is scarred but competent. This is not standard practice.
The external rotation loss (8-14 degrees mean) is functionally significant for throwers and overhead sport athletes. Some authors recommend avoiding remplissage in competitive overhead athletes and favouring Latarjet or humeral osteoplasty instead. Other authors report acceptable return to overhead sport after remplissage with targeted rehabilitation. This remains a clinical judgement call.
MCQ Practice Points
Q: What structures are tenodesed into the Hill-Sachs defect during a remplissage procedure? A: The posterior capsule and the infraspinatus tendon. Suture anchors are placed in the floor of the Hill-Sachs defect, and sutures are passed through the posterior capsule and the infraspinatus footprint. The tendon is pulled into the defect without being detached from its insertion on the greater tuberosity. This creates an extra-articular buttress that prevents the defect from engaging the anterior glenoid rim.
Q: When is remplissage indicated in anterior shoulder instability? A: When the Hill-Sachs lesion is off-track (Hill-Sachs interval greater than glenoid track) and anterior glenoid bone loss is less than 20-25 percent. Remplissage is combined with Bankart repair. It is not indicated for on-track (non-engaging) lesions, which are managed with Bankart repair alone, or for glenoid bone loss exceeding 25 percent, where Latarjet or bone grafting is required.
Q: How is the glenoid track calculated and what does an off-track result mean? A: Glenoid track = 0.84 multiplied by (glenoid width minus anterior rim bone loss width). This is measured on 3D CT. Off-track means the Hill-Sachs interval (Hill-Sachs width plus the bony bridge posterior to it) is greater than the glenoid track width. An off-track lesion engages the anterior glenoid rim during arm abduction and external rotation, predisposing to recurrent dislocation despite labral repair.
Q: What is the most common complication of the remplissage procedure? A: Loss of external rotation (stiffness), with a mean loss of 8-14 degrees. This is the accepted trade-off for achieving stability. Most patients compensate functionally, but overhead athletes may notice the limitation. Patients must be counselled preoperatively about this expected outcome.
Q: When is remplissage contraindicated in the management of anterior shoulder instability? A: When anterior glenoid bone loss exceeds 20-25 percent of the glenoid width. In this setting, the Latarjet procedure or glenoid bone grafting is required because the glenoid deficiency, not the Hill-Sachs, is the dominant driver of instability. Remplissage addresses only the humeral side. Isolated remplissage without Bankart repair is also contraindicated as it does not restore the anterior labral bumper.
Q: Why should the Bankart repair be performed before the remplissage? A: The Bankart is the primary stabiliser and should be completed first. If remplissage is performed first, tethering the posterior humeral head may alter the arthroscopic view and make anterior labral repair technically more difficult. Additionally, the Bankart restores the anterior bumper, and the remplissage is an adjunct to prevent Hill-Sachs engagement. The sequence follows a logical priority: restore the primary stabiliser first, then augment for the secondary pathology.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 24-year-old rugby player presents with his fourth anterior shoulder dislocation. He has had one previous arthroscopic Bankart repair 18 months ago that has failed. CT scan with 3D reconstruction shows an off-track Hill-Sachs lesion (Hill-Sachs interval 22 mm, glenoid track 18 mm) and 12 percent anterior glenoid bone loss. How would you manage him?”
“A 19-year-old competitive volleyball player has had three anterior dislocations. CT shows an off-track Hill-Sachs lesion with a Hill-Sachs interval of 20 mm and a glenoid track of 16 mm. Anterior glenoid bone loss is 8 percent. He is desperate to return to competitive volleyball at the highest level. What are the management options and how would you counsel him?”
Key Anatomy and Concept
- Hill-Sachs = posterosuperior humeral head compression fracture from anterior dislocation
- Engaging Hill-Sachs = defect contacts anterior glenoid rim in abduction/external rotation
- Glenoid track = 0.84 multiplied by (glenoid width minus anterior rim bone loss)
- Off-track = Hill-Sachs interval greater than glenoid track width
Indications and Contra-indications
- Indicated: off-track Hill-Sachs with glenoid bone loss less than 20-25 percent, combined with Bankart repair
- Not indicated: on-track (non-engaging) Hill-Sachs (Bankart alone sufficient)
- Contraindicated: glenoid bone loss greater than 25 percent (Latarjet required)
- Contraindicated: isolated remplissage without Bankart (insufficient stability)
Surgical Technique
- Lateral decubitus position preferred; posterior viewing, posterolateral accessory portal for remplissage
- Complete Bankart repair first, then address Hill-Sachs
- Debride Hill-Sachs floor to bleeding bone; insert 2-3 anchors in defect
- Pass sutures through posterior capsule and infraspinatus; tie knots to fill defect
Outcomes
- Recurrence rate: 4-8 percent at 2-5 years when combined with Bankart
- External rotation loss: mean 8-14 degrees (accepted trade-off)
- Rowe scores: 80-90 percent good to excellent results
- No significant arthritis progression reported at mid-term (up to 10 years)
Complications and Pearls
- Stiffness (ER loss) is primary complication; counsel preoperatively
- Recurrent instability 4-17 percent; consider Latarjet if glenoid loss large
- Overhead athletes: Latarjet may be preferred over remplissage to preserve ER
- Always document bone loss measurements and glenoid track calculation
Evidence Base and Key Trials
Hill-Sachs 'remplissage': an arthroscopic solution for the engaging Hill-Sachs lesion
- First clinical description of arthroscopic remplissage technique combined with Bankart repair for engaging Hill-Sachs lesions
- Low recurrence and acceptable external rotation loss in early series of patients with anterior instability
- Demonstrated feasibility of converting engaging lesions to non-engaging via posterior capsulodesis
Arthroscopic double-pulley remplissage technique for engaging Hill-Sachs lesions in anterior shoulder instability repairs
- Described the double-pulley suture anchor technique for remplissage to achieve secure fixation of infraspinatus and capsule into the defect
- Provided step-by-step technical pearls for anchor placement and suture management in the Hill-Sachs lesion
- Highlighted the importance of addressing both the Hill-Sachs and Bankart components in bipolar bone loss
Midterm outcomes of arthroscopic remplissage for the management of recurrent anterior shoulder instability
- Midterm follow-up of arthroscopic remplissage showed good stability and low recurrence in patients with engaging Hill-Sachs lesions
- Significant improvement in shoulder scores with manageable loss of external rotation
- Confirmed the role of remplissage in converting off-track lesions and reducing revision rates
Bankart repair versus Bankart repair plus remplissage: an in vitro biomechanical comparative study
- Biomechanical study demonstrating that adding remplissage to Bankart repair significantly reduces anterior translation in engaging Hill-Sachs models
- Remplissage provides additional stability by limiting the engaging arc of the humeral head defect
- Quantified the contribution of remplissage to overall joint stability beyond labral repair alone
The biomechanical effect of shoulder remplissage combined with Bankart repair for the treatment of engaging Hill-Sachs lesions
- Demonstrated that remplissage plus Bankart repair restores glenohumeral stability more effectively than Bankart repair alone in engaging Hill-Sachs lesions
- Remplissage reduces the engaging potential by filling the defect and altering humeral head kinematics
- Supports use of remplissage when glenoid track assessment indicates off-track pathology