Rockwood Classification of AC Joint Injuries
Examiners expect you to classify the injury on imaging, describe the ligament disruption pattern, and justify your management based on the type. The two high-yield pressure points are: (1) why type III is controversial — name the factors that push you toward surgery (overhead sport, dominant arm, manual occupation, acute injury less than three weeks, high cosmetic concern, and bilateral comparison for asymmetry), and (2) why types IV to VI are operative — the posterior or inferior displacement represents structural failure that will not remodel and risks skin breakdown, neurovascular compromise, or painful non-union if left unreduced. Always mention the axillary lateral view — an AP film alone misses type IV and VI injuries.
The Rockwood Classification System

The patient typically presents after a direct fall onto the point of the shoulder — common in cycling, rugby, skiing, and contact sports. Pain is localised to the AC joint; the arm is held adducted close to the body to relieve strain on the injured ligaments.
Examination sequence:
- Look: Inspect both shoulders from behind. Compare the clavicle contour — a type III or V injury shows a prominent superior step at the AC joint. Type IV may show a posterior bulge. Type VI shows the shoulder sitting inferiorly with a shortened clavicular profile. Check for skin tenting, abrasions, and swelling over the AC joint.
- Feel: Palpate directly over the AC joint — point tenderness is present in all types. Palpate along the clavicle for tenderness extending to the CC ligament interval. In type IV, the posterior edge of the clavicle may be palpable behind the acromion.
- Move: Active forward flexion and abduction are painful, particularly in the mid-range. Cross-body adduction compresses the AC joint and reproduces pain in all types. Assess scapular dyskinesis — early fatigue and abnormal scapulohumeral rhythm may indicate trapezius dysfunction in higher-grade injuries.
- Special tests: Cross-body adduction test — forward flex the arm to 90 degrees then forcibly adduct across the chest. Pain over the AC joint is positive and highly sensitive for AC joint pathology. AC joint compression (Paxinos) test — downward force on the proximal humerus with the arm adducted. Active compression (O'Brien) test — sensitive but less specific for AC joint disorders.
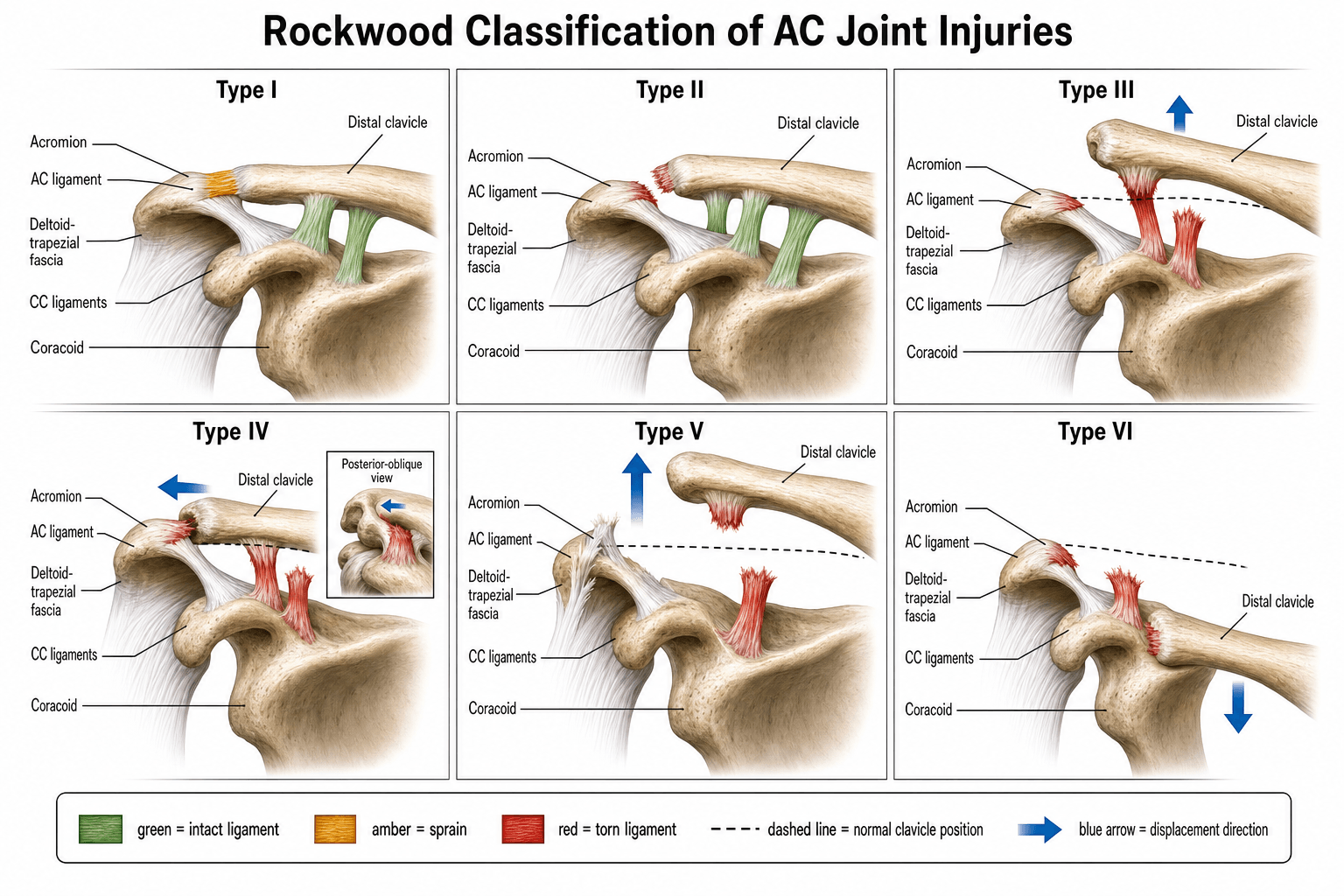
The classification describes six grades of acromioclavicular separation based on the structures disrupted and the magnitude and direction of clavicular displacement.
- AC Ligaments
- Sprained
- CC Ligaments
- Intact
- Clavicle Displacement
- None
- Key Clinical Feature
- Point tenderness over AC joint; normal radiographs; no instability on stress views
- AC Ligaments
- Torn
- CC Ligaments
- Sprained (partial)
- Clavicle Displacement
- Slight superior (less than 50 per cent of clavicle width)
- Key Clinical Feature
- Palpable step-off; mild upward subluxation on Zanca view; mild instability
- AC Ligaments
- Torn
- CC Ligaments
- Torn
- Clavicle Displacement
- Superior, 25–100 per cent of clavicle width above acromion
- Key Clinical Feature
- Prominent deformity; CC distance increased; deltoid-trapezius fascia detached from distal clavicle
- AC Ligaments
- Torn
- CC Ligaments
- Torn
- Clavicle Displacement
- Posterior — clavicle displaced behind acromion into trapezius
- Key Clinical Feature
- Posterior prominence; pain on cross-body adduction; may have skin tenting; visible on axillary view only
- AC Ligaments
- Torn
- CC Ligaments
- Torn
- Clavicle Displacement
- Severe superior, 100–300 per cent of clavicle width
- Key Clinical Feature
- Gross deformity; deltoid and trapezius completely detached from distal clavicle; high-energy mechanism
- AC Ligaments
- Torn
- CC Ligaments
- Torn
- Clavicle Displacement
- Inferior — clavicle displaced under coracoid process
- Key Clinical Feature
- Rare; very high-energy; associated neurovascular injury and rib or scapula fractures; shoulder looks shortened and inferior
UBVD — Up · Behind · Very high · DownDirection defines the high-grade types
Hook:From type III onward both AC and CC ligaments are torn — only the DIRECTION of clavicle displacement separates III/IV/V/VI.
The axillary lateral view is non-negotiable for AC joint injuries. An anteroposterior radiograph alone cannot detect posterior (type IV) or inferior subcoracoid (type VI) displacement. In the viva, if you describe the classification without mentioning the axillary view, the examiner will ask you what you are missing.
The Rockwood patterns only make sense once you know what each ligament does. The AC joint has a dual restraint system, and the two groups stabilise in different planes:
- AC capsular ligaments (superior, inferior, anterior, posterior thickenings of the joint capsule, with a variable intra-articular fibrocartilaginous meniscoid disc) are the primary HORIZONTAL (anteroposterior) stabilisers — the superior and posterior capsular ligaments are the strongest and resist posterior translation of the clavicle. This is why posterior buttonholing (type IV) reflects capsular failure.
- Coracoclavicular (CC) ligaments are the primary VERTICAL (superior–inferior) stabilisers, tethering the clavicle down to the coracoid. They have two distinct components: the conoid (more medial and posterior, fan-shaped, the main restraint to superior displacement) and the trapezoid (more lateral and anterior, resisting axial compression and posterior axial loading). This is why progressive superior displacement (types III and V) requires CC failure.
Putting it together: an isolated AC capsular sprain with intact CC ligaments allows little displacement (type I–II); once both the AC capsule and the CC ligaments fail, the direction of displacement is then determined by which restraint and which surrounding fascia gives way (superior in III/V, posterior in IV, inferior in VI). Normal distances to quote: the AC joint space is roughly 1 to 3 mm, and the normal CC distance is 1.1 to 1.3 cm — a CC distance more than 25 to 50 per cent greater than the uninjured side indicates complete CC disruption. Restoring the conoid and trapezoid footprints is the rationale behind anatomical CC reconstruction for the high grades.
Treatment by Classification Grade

- Recommended Management
- Non-operative
- Key Indication
- Sling for comfort (1 to 2 weeks), ice, analgesia; early active-assisted ROM
- Expected Outcome
- Excellent; full return to sport at 2 to 6 weeks
- Recommended Management
- Non-operative
- Key Indication
- Sling 2 to 3 weeks, gradual ROM then strengthening; return to sport at 6 to 8 weeks
- Expected Outcome
- Good; mild residual step-off common but pain-free in most
- Recommended Management
- Controversial — non-operative first line
- Key Indication
- Non-operative: sling, rehab, activity modification. Surgery for select patients — overhead athletes, manual labourers, dominant arm, acute presentation less than three weeks
- Expected Outcome
- Non-operative: satisfactory in 85 to 90 per cent of patients at medium-term follow-up. Surgical: better cosmesis and strength but higher complication rate; no clear superiority in outcome scores
- Recommended Management
- Operative
- Key Indication
- Open or arthroscopic CC ligament reconstruction (modified Weaver-Dunn, anatomical CC reconstruction with allograft or autograft, hook plate)
- Expected Outcome
- Restored anatomy and stability; address posterior buttonholing
- Recommended Management
- Operative
- Key Indication
- CC ligament reconstruction with deltoid-trapezius repair; fixation options include hook plate, double-button (TightRope), or coracoclavicular screw (temporary)
- Expected Outcome
- Functional restoration; risk of loss of reduction if deltoid repair fails
- Recommended Management
- Operative — urgent
- Key Indication
- Open reduction, CC ligament reconstruction, repair of surrounding soft tissues; assess for neurovascular injury
- Expected Outcome
- Satisfactory outcome with prompt reduction; delay risks neurovascular compromise
Type VI injuries can compromise the brachial plexus and subclavian vessels because the clavicle is driven inferiorly beneath the coracoid and into the thoracic outlet. Examine distal pulses, radial nerve function, and upper limb neurology urgently. These are high-energy injuries — screen for associated pneumothorax, scapular fracture, and sternoclavicular disruption. Operative reduction and stabilisation is urgent.
The tables list "Weaver-Dunn", "TightRope" and "hook plate" — examiners expect you to actually explain what each is and, crucially, that timing dictates the technique.
The acute-versus-chronic principle (the single decision that drives reconstruction):
- Acute (within about three weeks): the native AC and CC ligaments still have healing potential. The goal is reduce and stabilise so they heal in place — CC fixation with a double-button / suspensory device (TightRope/Dog Bone: a button on the clavicle and a button under the coracoid joined by high-strength suture, reducing and holding the CC distance), a hook plate, or a temporary CC screw, with repair of the deltotrapezial fascia. A biological graft is often not needed.
- Chronic (beyond roughly three to six weeks): the torn ligaments will not heal, so reduction alone fails. You must add biological reconstruction — the construct needs new ligamentous tissue, not just a suture tether.
- Weaver-Dunn: excise the distal clavicle and transfer the coracoacromial (CA) ligament (detached from the acromion) into the medullary canal of the distal clavicle to act as a new CC restraint. Historically the classic chronic reconstruction but biomechanically weaker than the intact CC ligaments, so prone to loss of reduction.
- Modified Weaver-Dunn: the CA transfer augmented with a suture/suspensory or tape construct to protect it while it heals.
- Anatomical CC reconstruction: a free tendon graft (e.g. semitendinosus allograft/autograft) passed around or through tunnels in the coracoid and clavicle to recreate the conoid and trapezoid footprints — the current preference for chronic and high-grade injuries because it restores anatomy and is stronger than a CA transfer.
- Hook plate: a plate hooked under the acromion holding the reduction; reliable but causes subacromial erosion and rotator-cuff irritation and must be removed (typically at three to six months).
loss of reduction (the commonest failure, especially after isolated CA transfer or if the deltotrapezial repair fails), coracoid or clavicle fracture through drill tunnels, hardware migration, and over-tunnelling weakening the bone.
Non · Non · Discuss · Operate · Operate · OperateTreatment decision by type
Hook:The dividing line is structural: I–II heal, III is a judgement call, IV–VI will not remodel and need surgery.
Controversies and Limitations
- The type III debate is the single biggest exam topic. The evidence does not support routine operative fixation for acute type III injuries. Multiple level-1 and level-2 trials and systematic reviews show that non-operative treatment produces comparable functional outcome scores, return-to-work rates, and patient satisfaction at two to five years. Surgery offers better cosmetic appearance and marginally stronger isometric strength, but carries a complication rate of 20 to 40 per cent including hardware failure, wound infection, loss of reduction, and the need for re-operation. Most guidelines recommend non-operative treatment as first line with surgery reserved for specific patient factors (overhead athletes, manual labourers, dominant arm, acute injury less than three weeks, high cosmetic demands).
- Inter-observer reliability is only moderate. Studies using both plain radiographs and CT show fair to moderate agreement between surgeons when classifying the same injury, particularly distinguishing between type III and V injuries and between III and IV when the axillary view is suboptimal. The CC distance measurement threshold between types varies between institutions.
- Weighted stress views are debated. Some centres use bilateral weighted views (5 to 10 kg per hand) to demonstrate dynamic CC instability and help differentiate type II from III. Critics argue that the test is painful, non-standardised, and that all patients with complete CC disruption show widening under stress regardless of treatment implications.
- The classification does not capture chronicity. A type III injury treated non-operatively that remains painful and unstable at six months is a chronic type III — this is functionally a different clinical entity from an acute type III, and the treatment algorithm shifts toward late reconstruction.
- Rockwood type VI is rare and poorly studied. Most published series have fewer than five cases. The classification was described before widespread adoption of CT, and the true incidence and optimal surgical technique are not well established.
- Imaging limitations. Plain radiographs underestimate CC distance compared with CT or MRI. The Zanca view is technically dependent on beam angulation (10 to 15 degree cephalic tilt). MRI can directly visualise the ligaments but is not routine in acute injury management. Normal CC distance is 1.1 to 1.3 cm; a difference greater than 50 per cent compared with the contralateral side suggests complete CC disruption.
- The classification does not account for associated injuries. Concomitant rotator cuff tears, superior labral anterior-posterior (SLAP) lesions, and coracoid fractures can occur with any type and change the treatment plan independently of the Rockwood grade.
ZAW — Zanca · Axillary · WeightedImaging views for AC joint injury
Hook:Normal CC distance ~1.1–1.3 cm; a difference over 50% versus the contralateral side suggests complete CC disruption.
Viva practice
Exam Viva
Practise clinical reasoning and management decisions out loud
“A 28-year-old professional cricketer presents with a painful left shoulder after a diving catch two days ago. Examination reveals a prominent AC joint step-off with tenderness. Radiographs show the clavicle displaced about 75 per cent of its width above the acromion on the Zanca view, with an increased CC distance. How would you classify and manage this?”
“A 45-year-old construction worker fell from scaffolding onto his right shoulder. He has a grossly deformed shoulder with the clavicle sitting very high — radiographs show it displaced more than twice the clavicle width above the acromion with an empty CC space. The axillary view confirms the clavicle is superiorly displaced, not posterior. How do you classify this, what is your surgical plan, and what are the key steps?”
Exam cheat sheet
Classification — ligament disruption and displacement
- I: AC sprained, CC intact, no displacement
- II: AC torn, CC sprained, slight superior displacement (less than 50 per cent of clavicle width)
- III: AC and CC torn, superior displacement 25 to 100 per cent of clavicle width, deltoid-trapezius detached
- IV: AC and CC torn, posterior displacement into trapezius — detect on axillary view
- V: AC and CC torn, severe superior displacement (100 to 300 per cent), deltoid-trapezius stripped
- VI: AC and CC torn, inferior subcoracoid displacement — rare, high-energy, screen neurovascular status
Imaging essentials
- Zanca view (10 to 15 degree cephalic tilt AP centred on AC joint) — primary grading view
- Axillary lateral — essential to detect type IV (posterior) and type VI (inferior) displacement
- Weighted stress views — 5 to 10 kg per hand; distinguishes type II from III by unmasking CC instability
- Normal CC distance is 1.1 to 1.3 cm; a difference greater than 50 per cent compared with the contralateral side suggests complete CC disruption
Treatment rules
- I and II: non-operative — sling, ice, analgesia, early ROM; expect excellent outcome
- III: controversial — non-operative first line (85 to 90 per cent satisfactory); surgery for overhead athletes, manual labourers, dominant arm, acute less than three weeks
- IV, V, VI: operative — CC ligament reconstruction, deltoid-trapezius repair; type VI is urgent
- Type III surgery factors: sport, occupation, dominance, timing, cosmetic concern, and bilateral comparison
Exam traps
- Forgetting the axillary view — you cannot classify without it
- Classifying a type V as type III — the displacement and soft-tissue stripping are different
- Saying all type III injuries are non-operative without mentioning the controversy or patient factors
- Not mentioning complications of surgery (20 to 40 per cent rate: hardware failure, infection, loss of reduction, re-operation)
Evidence
Surgical versus conservative management of Type III acromioclavicular dislocation: a systematic review
- Systematic review of 14 studies (646 shoulders) comparing operative versus non-operative Rockwood type III AC dislocation; recurrence in the surgical group was 14%.
- No statistically significant difference in post-treatment osteoarthritis or persistence of pain (pain trended lower with surgery).
- There was insufficient evidence to establish a difference in functional outcome — high-quality RCTs are needed.
Multicenter Randomized Clinical Trial of Nonoperative Versus Operative Treatment of Acute Acromio-Clavicular Joint Dislocation
- Multicentre RCT of 83 patients with acute complete (grade III/IV/V) AC dislocations: hook-plate fixation versus non-operative treatment.
- DASH scores were significantly BETTER in the non-operative group at 6 weeks and 3 months, with no difference at 6 months, 1 year or 2 years; Constant scores followed the same pattern.
- Radiographic alignment was better after surgery, but the reoperation rate was significantly higher in the operative group; both groups reached a good/excellent result by 2 years.
According to PubMed, the type III controversy (no clear functional benefit of surgery; 14% surgical recurrence in 646 shoulders) is from Longo et al. 2017 (DOI 10.1093/bmb/ldx003), the key RCT showing hook-plate surgery gives better radiographs but no clinical superiority (faster early recovery and fewer reoperations non-operatively) from the Canadian Orthopaedic Trauma Society 2015 (DOI 10.1097/BOT.0000000000000437); and the high-grade (III–V) meta-analysis favouring operative treatment for functional/radiological outcomes (Constant MD 2.38; complications 18.3% vs 15.9%) is from Adra et al. 2024 (DOI 10.7759/cureus.76682).