Massive Cuff Tear | Superior Migration | Acetabularization
Seebauer Classification
Critical Must-Knows
- Pathophysiology: Loss of 'The Spacer' (Supraspinatus) and 'The Fulcrum' (Force Couples).
- Acetabularization of the acromion is the hallmark radiographic sign.
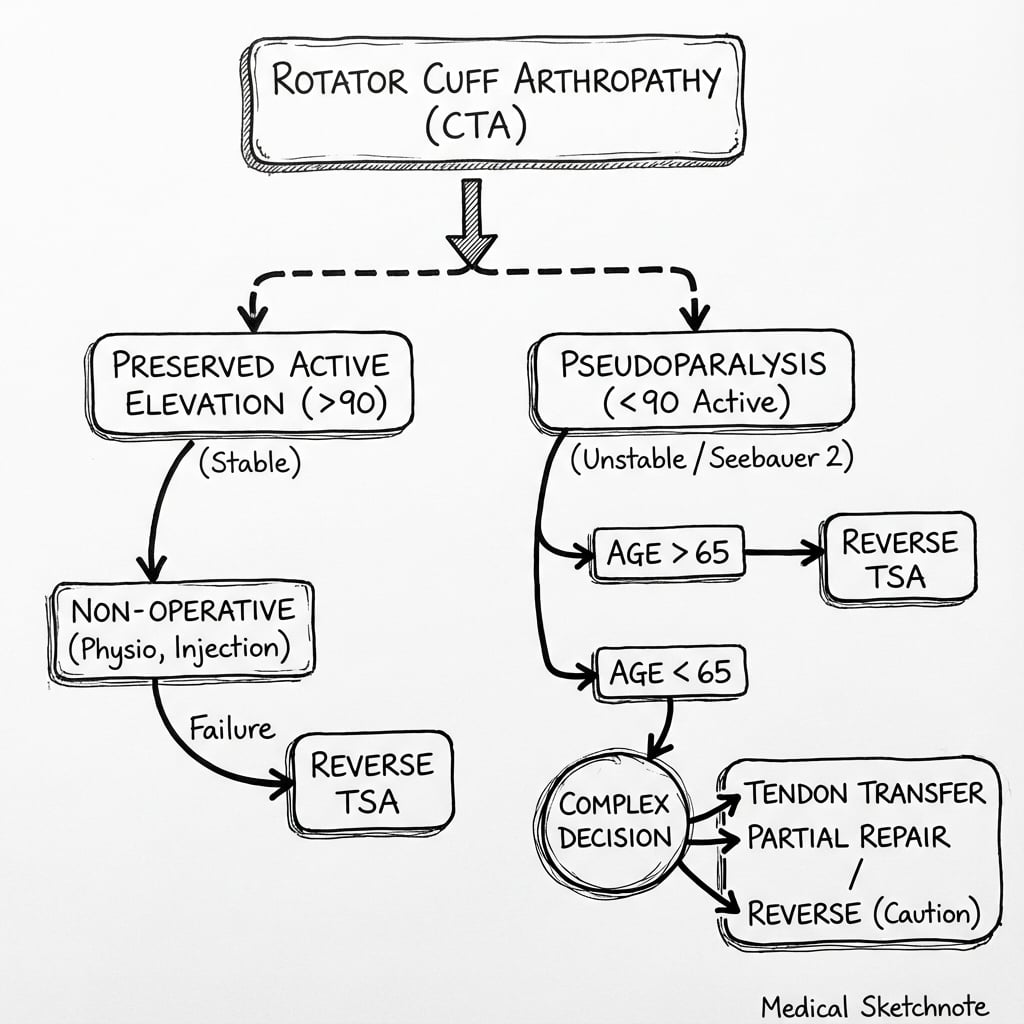
- Pseudoparalysis (less than 90 deg active elevation with full passive) is a key indication for Reverse TSA.
- Hemiarthroplasty is largely historical/salvage (CTA Head).
- Reverse TSA requires a functioning Deltoid and Axillary Nerve.
Clinical Pearls
- "Look for the 'Popeye' deformity (Biceps rupture is common precursor).
- "Anterior-Superior Escape: Head palpable subcutaneously.
- "Hornblower's Sign (Teres Minor) predicts External Rotation outcome.
- "Fluid sign (Geyser sign) on AC joint.
- "Subscapularis failure leads to Anterior Escape.
- "Teres Minor failure leads to External Rotation deficit.
Clinical Imaging
Imaging Gallery



Critical definition: Pseudoparalysis vs Pseudo-pseudoparalysis
At a Glance
Differential Diagnosis of the High-Riding Head
| Condition | History | Key Feature | Management |
|---|---|---|---|
| Cuff Tear Arthropathy | Chronic pain, weakness | Arthritis + Cuff Tear | Reverse TSA |
| Massive Cuff Tear (No OA) | Pain, preserved motion | Normal Joint Space | Repair / SCR / Balloon |
| Acute Cuff Tear | Trauma | No acromial wear | Urgent Repair |
| Rheumatoid Arthritis | Systemic disease | Central erosion | Medical Mx / Arthroplasty |
Mnemonics
FATCTA Pathophysiology
| F | Fulcrum Loss Loss of concavity compression |
| A | Acetabularization Acromion becomes a socket |
| T | Translation Superior migration of the head |
| F | Fulcrum Loss Loss of concavity compression |
| A | Acetabularization Acromion becomes a socket |
| T | Translation Superior migration of the head |
Hook:FAT shoulder: Fulcrum loss, Acetabularization, Translation.
BADRequirements for Reverse TSA
| B | Bone Stock Glenoid must support baseplate |
| A | Axillary Nerve Deltoid must be functioning |
| D | Deltoid Muscle quality must be adequate |
| B | Bone Stock Glenoid must support baseplate |
| A | Axillary Nerve Deltoid must be functioning |
| D | Deltoid Muscle quality must be adequate |
Hook:Don't use a Reverse if the scenario is BAD (No Bone, No Nerve, No Deltoid).
ASHContraindications to Hemi
| A | Anterior Escape Coracoacromial arch incompetence |
| S | Stability Lack of static constraints |
| H | High Demand Patient needs active elevation |
| A | Anterior Escape Coracoacromial arch incompetence |
| S | Stability Lack of static constraints |
| H | High Demand Patient needs active elevation |
Hook:Hemi turns to ASH in unstable shoulders.
TILTScapular Notching Prevention
| T | Tilt inferiorly Inferior baseplate tilt reduces impingement |
| I | Inferior placement Place glenosphere flush or below inferior rim |
| L | Lateralize Lateralized glenosphere or BIO-RSA |
| T | 135 neck-shaft angle Modern 135 degree stems reduce notching vs 155 degree |
| T | Tilt inferiorly Inferior baseplate tilt reduces impingement | L | Lateralize Lateralized glenosphere or BIO-RSA |
| I | Inferior placement Place glenosphere flush or below inferior rim | T | 135 neck-shaft angle Modern 135 degree stems reduce notching vs 155 degree |
Hook:TILT the baseplate to prevent notching!
Overview and Epidemiology
Definition. Cuff tear arthropathy (CTA) is the end-stage of a chronic massive rotator cuff tear: loss of the cuff force couples allows the humeral head to migrate superiorly, eroding the acromion (acetabularization), rounding the greater tuberosity (femoralization) and finally destroying the glenohumeral joint. First characterised by Neer in 1983; the rapidly destructive crystal-driven variant is "Milwaukee shoulder".
- Who: Typically elderly (over 70 years), with a female predominance.
- Frequency: A minority of massive cuff tears progress to true arthropathy; estimated prevalence around 4% in cohorts over 70. Most massive tears remain functional ("suspension-bridge" compensation) without ever developing arthritis.
- Mechanism (two-hit): (1) mechanical loss of the force couple and superior stabiliser, plus (2) a nutritional/inflammatory element (decreased synovial fluid, basic calcium phosphate crystal release) contributing to cartilage loss.
- Natural history: Slow progression over years; pain and pseudoparalysis, not the radiographic grade alone, drive the decision to operate.
Anatomy and Biomechanics
Relevant Anatomy
- Coracoacromial Arch: Becomes the new weight-bearing roof of the shoulder. Do NOT violate the CA ligament in CTA surgery (it is the only restraint against escape).
- Glenoid: Can become eroded superiorly ("E2 type wear").
- Subscapularis: Often intact in early stages but if torn, leads to anterior escape.
- Teres Minor: Critical for external rotation. If absent or fatty infiltrated (Hornblower's), a standard Reverse TSA will still result in an arm that cannot externally rotate (Latissimus Dorsi transfer may be added).
- Neurovascular Relations:
- Axillary Nerve: Runs 5cm distal to the acromion. Travels through the quadrangular space with the posterior circumflex humeral artery.
- Suprascapular Nerve: Travels through the suprascapular notch (under the transverse ligament) and spinoglenoid notch. Risk of injury during posterior glenoid retraction.
- Cephalic Vein: The primary landmark for the deltopectoral approach. Preserving it reduces venous congestion.
Classification Systems
Seebauer Classification
Functional classification based on the center of rotation and stability. Guides treatment.
| Type | Features | Stability | Treatment |
|---|---|---|---|
| Type 1A | Head Centered, Minimal migration | Stable | Hemi / Reverse |
| Type 1B | Head Centered, Medialized glenoid | Stable | Hemi / Reverse |
| Type 2A | Head Migrated Superiorly | Stable (under arch) | Reverse TSA |
| Type 2B | Anterior-Superior Escape | Unstable | Reverse TSA |
Clinical Assessment
History
- Pain: Night pain is prominent.
- Weakness: Inability to lift arm ("Pseudoparalysis").
- Duration: Often long history of shoulder trouble.
Examination
- Look: Supraspinatus/Infraspinatus wasting. "Popeye" muscle (biceps rupture).
- Move: Pseudoparalysis (Forward flexion less than 90). Anterolaterally escaped head (palpable bulge).
- Lag Signs: ER Lag sign (Infraspinatus), Hornblower's sign (Teres Minor), Lift-off lag (Subscap).
Neurological Exam
Always document Axillary Nerve function (deltoid contraction). A Reverse TSA relies entirely on the deltoid. If the deltoid is paralyzed, a Reverse TSA is contraindicated (Disaster).
Investigations
Diagnostic Workup
- AHI: Acromiohumeral interval less than 7mm suggests massive tear. Less than 5mm is diagnostic of extensive tear.
- Femoralization: Rounding of greater tuberosity.
- Acetabularization: Concavity of acromion undersurface.
The radiographic changes progress systematically from early superior migration to late acetabularization.
- Joint Space: Loss of GH space (superiorly first).
- Bone Stock: Assess glenoid for existing screws/anchors from prior surgeries.
- Erosion: Look for superior glenoid wear (Favard E-type).
MRI is the gold standard for assessing the "engine" of the shoulder - the muscles.
- Goutallier Classification: Defines fatty infiltration.
- Grade 0: No fat.
- Grade 1: Some fat streaks.
- Grade 2: More muscle than fat (less than 50%).
- Grade 3: Equal muscle and fat (50%).
- Grade 4: More fat than muscle (greater than 50%).
- Significance: Grade 3 and 4 changes are irreversible. Repairing a cuff with Grade 3/4 fat has a 90-100% failure rate.
- Teres Minor Integrity: This is the most critical structure to evaluate for a Reverse TSA. Look for it on the axial cuts. If Teres Minor is Grade 3/4, the patient will NOT have external rotation post-op. This is a specific indication for a Latissimus Dorsi Transfer.
Imaging Gallery
Management Algorithm
Conservative Management
- Indications: Elderly, low demand, stable joint (Seebauer 1).
- Physiotherapy: Deltoid re-education protocol. Anterior Deltoid strengthening. Avoid rotator cuff strengthening (it's gone).
- Injections: Corticosteroid for pain relief (temporary).
- Outcomes: Many patients (Type 1A/B) abide well with low demand adaptation.
Pearl: Always try a period of non-operative management first unless there is an anterior escape (Seebauer 2B) which is functionally debilitating.
Reverse TSA Principles
Reverse Total Shoulder Arthroplasty (rTSA) The workhorse for CTA.
Biomechanics of Grammont Style Reverse
- Medialization: Moves center of rotation medially. Increases the lever arm of the deltoid (recruits more fibers).
- Distalization: Moves center of rotation distally. Retensions the deltoid.
- Constraint: Semi-constrained design provides stability (replaces the cuff's function).
Indications
- CTA with pseudoparalysis.
- Massive unrepairable cuff tear.
- Failed Hemiarthroplasty/Total Arthroplasty.
- Proximal Humerus Malunion/Nonunion.
Contraindications
- Deltoid Paralysis (Axillary nerve injury).
- Active Infection.
- Glenoid Bone Deficiency (unable to hold baseplate screws).
Surgical Technique
Deltopectoral Approach
- Standard approach.
- Pearl: The Coracoacromial (CA) ligament is often preserved in CTA if doing a Hemi, but in Reverse, it is usually released.
- Subscapularis: Often contracted or torn. Released/Debrided.
Preserve the deltoid insertion distally. Protect the cephalic vein.
Complications
| Complication | Risk | Mechanism | Prevention |
|---|---|---|---|
| Scapular Notching | Common | Medial humeral cup hits scapula neck | Lateralized glenosphere / Inverse graft |
| Acromial Fracture | 1-3% | Overtensioning / Delt stress / Osteopenia | Avoid lengthening arm too much |
| Dislocation | 3% | Undertensioning / Impingement | Proper tensioning, larger glenosphere |
| Neuroapraxia | Common | Arm lengthening traction | Intra-op monitoring |
Scapular Notching (Sirveaux Classification) Notching is a unique complication of Reverse TSA where the humeral cup abrades the inferior scapular neck during adduction.
- Grade 1: Defect involving pillar only.
- Grade 2: Defect contacting lower screw.
- Grade 3: Defect extending over lower screw.
- Grade 4: Defect extending to central peg (Threatening fixation).
- Prevention:
- Lateralization: This is the most effective method.
- Glenoid Side: Bony-metallic (BIO-RSA) or Metallic lateralization.
- Humeral Side: Onlay stems or curved stems.
- Inferior Overhang: Placing the glenosphere inferiorly prevents impingement in adduction.
- Neck-Shaft Angle:
- 155 degrees (Grammont original): High rate of notching.
- 135 degrees (Modern): Reduces notching but increases shear force on the baseplate.
- Lateralization: This is the most effective method.
Acromial Stress Fracture
- Pathology: The deltoid is significantly tensioned. In elderly osteopenic patients, this stress can fracture the acromion or scapular spine.
- Diagnosis: Sudden onset pain after doing well for 3 months. X-ray might miss it (requires scapular views/CT).
- Consequence: Catastrophic. The deltoid origin becomes unstable. The "Reverse" stops working.
- Treatment: Conservative (High rate of non-union). ORIF has high failure rate.
Infection (Periprosthetic Joint Infection - PJI)
- Pathogen: Cutibacterium acnes (C. acnes) is the causative organism in over 60% of shoulder PJIs.
- Biology: Gram-positive, anaerobic, slow-growing bacillus. Commensal on skin, specifically in sebaceous glands (which are dense in the shoulder region).
- Risk Factors: Male gender (more hair/sebum), younger age, prior surgery, topical steroids.
- Presentation: rarely presents with acute sepsis (fever/redness). Typical presentation is aggressive "stiffness" or unexplained "pain" after a period of doing well.
- Diagnosis:
- Markers: ESR/CRP are often normal in C. acnes infection.
- Aspiration: Dry taps are common.
- Cultures: Must be held for minimum 14 days (up to 21 days).
- Frozen Section: Over 50 PMNs per HPF is suggestive.
- Management:
- DAIR (Debridement): Poor success rate for C. acnes. Only considered for acute hematogenous spread.
- Two-Stage Revision: The Gold Standard.
- Stage 1: Removal of all implants, thorough debridement, placement of antibiotic spacer (high dose Vancomycin/Gentamicin).
- Antibiotics: 6 weeks of targeted therapy (often includes Rifampin for biofilm).
- Stage 2: Reimplantation after antibiotic holiday and negative rescreen.
Neurological Injury
- Axillary Nerve: Most at risk during the inferior capsular release or from traction.
- Presentation: Deltid paralysis.
- Prognosis: Most are neurapraxias that resolve.
- Prevention: Identify the nerve. Keep the arm adducted while releasing inferiorly.
Postoperative Care
Rehab Protocol
- Sling: Worn for comfort and protection, usually for 4 weeks.
- Range of Motion:
- Passive Supine Elevation to 90 degrees allowed immediately.
- Passive External Rotation to neutral (0 degrees).
- Restrictions:
- No Extension: Extension coupled with adduction and internal rotation (reaching for back pocket) is the position of dislocation.
- No Active Elevation: Protect the deltoid and subscapularis repair (if done).
- Functional: Hand to mouth activities (eating, drinking) are encouraged to prevent stiffness.
- Wean Sling: Discontinue sling use during the day.
- Active Assisted Motion: Pulleys and stick exercises.
- Deltoid Recruitment:
- Begin supine active forward elevation (gravity eliminated).
- Progress to standing active forward elevation as deltoid control improves.
- Hydrotherapy: Excellent for deltoid activation without gravity.
- Deltoid Strengthening: Progressive resistance bands (Therabands).
- Scapular Stabilizers: Rhomboids and Trapezius strengthening.
- Functional Use: Return to full activities of daily living.
- Sports: Golf and swimming (breaststroke) are often tolerated. Overhead sports (tennis service) are generally discouraged.
- Weight Limit: Generally restrict lifting to under 5-10kg repetitive overhead.
- Function: Expect active elevation to ~140 degrees. Rapid fatigue with overhead activity is common due to deltoid fatigue.
- Proprioception: The joint position sense is altered (no cuff).
Outcomes and Prognosis
Across landmark series, RTSA reliably converts a painful pseudoparalytic shoulder into a functional, pain-free one, with Constant scores roughly doubling (Sirveaux 22.6 to 65.6; Wall 23 to 60).
- Elevation: Restore active elevation reliably (over 130 degrees).
- Rotation: External rotation is often not restored (0-10 degrees) unless Teres Minor is intact or Lat Dorsi transfer is done.
- Function: Patients can feed themselves and reach top of head, but reaching up back (IR) is limited.
Controversies and Areas of Uncertainty
Medialized vs Lateralized Design
Grammont medialization reduces notching but limits rotation; lateralization (bony BIO-RSA or metallic) improves rotation and contour at the cost of more baseplate torque. The optimal degree of global lateralization and distalization is still debated.
135 vs 155 degree Neck-Shaft Angle
155 degree (original Grammont) increases notching; 135 degree inlay/onlay designs reduce notching but raise shear at the baseplate. No design has proven clearly superior in revision rates.
Subscapularis Repair
Whether to repair the subscapularis in RTSA is unresolved. Some evidence links repair to lower dislocation rates, but with lateralized designs the benefit is less clear and repair may limit rotation.
RTSA in Younger / Active Patients
Reverse TSA for cuff-deficient shoulders under ~60 years remains contentious given finite implant longevity and higher demand; joint-preserving options (debridement, partial repair, superior capsular reconstruction, lower trapezius/lat dorsi transfer) are weighed first.
Pseudoparalysis vs Pseudoparesis
The literature inconsistently defines "pseudoparalysis" (truly less than 90 degrees) versus "pseudoparesis" (weak but greater than 90 degrees), which confounds comparison of joint-preserving vs replacement outcomes.
Navigation / PSI and Stemless Stems
Whether navigation/patient-specific instrumentation reduces glenoid-placement outliers enough to lower long-term loosening, and the durability of stemless reverse humeral components, await mature registry data.
Evidence Base
Grammont Reverse Principles
- Medializing the centre of rotation increases the deltoid lever arm and recruits more fibres.
- Distalizing the humerus tensions the deltoid.
- A fixed, semi-constrained fulcrum lets the deltoid substitute for the absent cuff.
Reverse TSA Results by Etiology
- Mean Constant score improved from 23 to 60 points; 173 of 186 patients satisfied or very satisfied.
- Best results in primary cuff tear arthropathy, OA with cuff tear, and massive cuff tear.
- Posttraumatic and revision cases had less improvement and higher complication rates.
Grammont Inverted Prosthesis for CTA (Landmark Series)
- Mean Constant score improved from 22.6 to 65.6; active forward elevation rose from 73 to 138 degrees.
- Integrity of teres minor was essential for recovery of external rotation and significantly influenced Constant score.
- Glenoid loosening/component dissociation noted; recommended for elderly low-demand patients.
BIO-RSA (Bony Increased-Offset Lateralization)
- Autologous humeral-head bone graft behind the baseplate incorporated in 98% of cases.
- Inferior scapular notching in only 19%; Constant score improved from 31 to 67.
- Bony lateralization keeps the centre of rotation at the bone interface, avoiding the added torque of metallic lateralization.
Hemiarthroplasty vs Reverse for CTA
- New Zealand Joint Registry pairs matched for age, sex and ASA.
- Mean 6-month Oxford Shoulder Score 37.5 (reverse) vs 31.1 (hemiarthroplasty).
- Fewer revisions in the reverse group (5 vs 9).
Goutallier Fatty Degeneration (CT vs MRI)
- Interobserver reproducibility of fatty-degeneration grading good-to-excellent on both CT and MRI.
- Degree of fatty degeneration correlated significantly with muscle atrophy.
- Proposed simplification to a 3-grade scale for MRI assessment.
Scapular/Acromial Fractures after RTSA
- Osteoporosis was a significant risk factor (odds ratio 1.97).
- Plain radiographs detected only 78.8% of fractures; advanced imaging often required.
- 14 of 16 scapular-spine fractures originated at a screw tip; the proposed (Crosby) classification had only moderate reliability.
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
The Failed Hemi
"A 75F had a Hemiarthroplasty for a fracture 2 years ago. Now has pain and cannot lift arm above 40 degrees. X-ray shows superior escape of the prosthesis."
No External Rotation
"You perform a Reverse TSA on a 70M. Post-op, he has 140 elevation but cannot externally rotate (ER is -10). He is unhappy (cannot eat with fork, comb hair). Why?"
The 'Pseudoparalytic' Shoulder
"Differentiate Pseudoparalysis from True Paralysis from Stiffness."
MCQ Practice Points
Pathophysiology
Q: What is the primary mechanical deficit in CTA? A: Loss of the Force Couple (Concavity Compression) and upward migration of the humeral head due to unopposed Deltoid pull.
Classification
Q: What distinguishes Seebauer 2A from 2B? A: Anterior instability. 2A is centered superiorly (stable under arch). 2B escapes antero-superiorly (unstable).
Biomechanics
Q: How does a Reverse TSA improve elevation? A: It Medializes the center of rotation (recruiting more deltoid fibers) & Distalizes the humerus (tensioning the deltoid).
Complications
Q: What is the most common complication of Grammont style Reverse TSA? A: Scapular Notching. (Though modern lateralized designs have reduced this).
Contraindications
Q: Which nerve must be functioning for a Reverse TSA? A: Axillary Nerve (Deltoid function). Without deltoid, the prosthesis won't work.
Guidelines, Registries & Global Practice
Global registry trends. National joint registries worldwide (AOANJRR in Australia, NJR in England/Wales, the New Zealand Joint Registry, and Nordic registries) document the same shift: reverse TSA has overtaken hemiarthroplasty and anatomic TSA for the cuff-deficient shoulder and now accounts for the majority of all shoulder replacements in most developed health systems. Hemiarthroplasty for cuff deficiency has been largely abandoned because of unreliable pain relief and superior migration.
Registry and Society Guidance, Side by Side
| Source | Position on CTA Management |
|---|---|
| AAOS (US) | Reverse TSA recommended for CTA with pseudoparalysis; cuff repair not indicated once arthropathy is established. |
| BOA / BESS (UK) | Reverse TSA is the procedure of choice for symptomatic CTA; emphasises deltoid/axillary nerve integrity. |
| Major registries (AOANJRR, NJR, NZJR) | Reverse TSA the dominant implant for CTA; lower revision than hemiarthroplasty for the same diagnosis. |
| EFORT / European consensus | Lateralized designs and inferior glenosphere placement to reduce notching; teres minor assessment before surgery. |
Revision and survivorship (registry-level).
- Primary reverse TSA shows roughly 90-95% survivorship at 10 years across large registries.
- Leading reasons for revision: infection (often the commonest early cause), instability/dislocation, and periprosthetic/acromial fracture.
- For an elderly primary CTA patient the lifetime risk of revision is low, so the implant typically outlasts the patient.
Implant and fixation notes.
- Metal-backed (screw-fixed) baseplates are standard for the reverse glenoid, in contrast to the cemented all-polyethylene glenoid used in anatomic TSA (where metal-backed designs failed early).
- Registries show no consistent difference between cemented and uncemented humeral stems for reverse TSA; modern uncemented HA-coated stems perform well.
Surgeon volume. A consistent volume-outcome relationship exists across registries: low-volume surgeons (broadly fewer than ~10 shoulder arthroplasties/year) have higher revision rates. Shoulder arthroplasty is increasingly a subspecialty procedure.
High- vs limited-resource practice variation.
- High-resource settings: ready access to reverse implants, CT-based planning, navigation/patient-specific instrumentation (used in a substantial minority of cases to reduce glenoid-placement outliers), and stemless/short-stem options (faster uptake in Europe).
- Limited-resource settings: reverse implants may be unavailable or unaffordable; arthroscopic debridement, biceps tenotomy, partial cuff repair, or even glenohumeral arthrodesis remain pragmatic salvage options for pain in the cuff-deficient arthritic shoulder.
CTA Summary
Clinical summary
Diagnosis
- •Pseudoparalysis
- •High riding head
- •Acetabularization
- •Fluid Sign
- •Hornblower's Sign
Classification
- •Hamada (X-ray severity)
- •Seebauer Type 1 (Stable)
- •Seebauer Type 2 (Unstable/Escape)
- •Favard (E-type glenoid)
Management
- •Non-op (Physio/Inject) for low demand
- •Reverse TSA (Gold Standard)
- •Hemi (Historical)
- •Arthrodesis (Salvage)
Reverse Biomechanics
- •Medialize COR
- •Lengthen Deltoid Lever
- •Distalize Humerus
- •Semi-constrained
- •Recruit ant/post deltoid
Complications
- •Scapular Notching
- •Acromial Fracture
- •Dislocation
- •Infection
- •Neuroapraxia