Sacral Insufficiency Fracture
- Normal radiographs do NOT exclude it - plain films are insensitive (bowel gas, osteopenia, sacral curve hide it). It is the "great mimicker": image with MRI (most sensitive, ~99%) or CT, not X-ray alone.
- EXCLUDE malignancy - metastasis and myeloma present identically in this age group. CT/MRI distinguish a fracture from a destructive lytic lesion before you accept an insufficiency fracture.
- The full Honda 'H' is the MINORITY (~4% on scintigraphy) - unilateral, vertical-only or horizontal-only variants are common, so the absence of an H does NOT exclude the diagnosis.
- The fracture is a SENTINEL event for under-treated bone disease - ~71% never get secondary fracture prevention. Treating the osteoporosis (and a falls/bone-health work-up) is as important as treating the fracture.
- Avoid prolonged bed rest - it is harmful in the elderly (deconditioning, VTE, pressure sores). Mobilise early with analgesia.
- Insufficiency vs fatigue: insufficiency = abnormal (weak) bone + normal load; fatigue = normal bone + abnormal repetitive load. Don't swap them.
Overview & Epidemiology
The sacral insufficiency fracture is an increasingly common fragility fracture - part of the fragility fracture of the pelvis (FFP) spectrum - and a frequently missed cause of disabling pain in older people. It is high-yield because it is easy to miss, easy to mistake for cancer, and a sentinel marker of untreated bone fragility.
- Demographics: elderly, predominantly postmenopausal osteoporotic women; also patients after pelvic radiotherapy, on chronic steroids, or with rheumatoid/renal/metabolic bone disease.
- Rising incidence with an ageing population; commonly under-diagnosed because radiographs look normal.
- High morbidity: loss of independence in ~64-89% and reported mortality of ~13-27% - comparable to other major fragility fractures.
- A care-gap condition: ~71% of patients are NOT started on secondary fracture prevention - the examiner's governance angle.
Pathophysiology: insufficiency vs fatigue & risk factors
A stress fracture is a fracture from repetitive sub-maximal load, and it has two types:
- Insufficiency fracture — abnormal (weakened) bone fails under normal physiological load. The sacral insufficiency fracture is the classic example: an osteoporotic sacrum in an elderly patient, often after minimal or no trauma.
- Fatigue fracture — normal bone fails under abnormal, repetitive load (runner, dancer, military recruit).
Beyond osteoporosis, weakened-bone causes include pelvic radiotherapy, chronic glucocorticoids, rheumatoid arthritis, renal osteodystrophy, Paget disease, hyperparathyroidism and osteomalacia. The sacral insufficiency fracture sits within the fragility fracture of the pelvis (FFP) spectrum and signals under-treated bone fragility.
Classification — fragility fractures of the pelvis
The fragility fracture of the pelvis (FFP) classification of Rommens and Hofmann grades by anterior and posterior pelvic ring involvement and stability, and the grade guides treatment (conservative for stable; fixation for unstable/progressive). Progression from a stable to an unstable pattern is common (influenced by bone density, pelvic morphology and sarcopenia) - so follow-up and treating the bone matter.
Anterior pelvic ring only (e.g. pubic rami) with an intact posterior ring - stable. Managed conservatively.

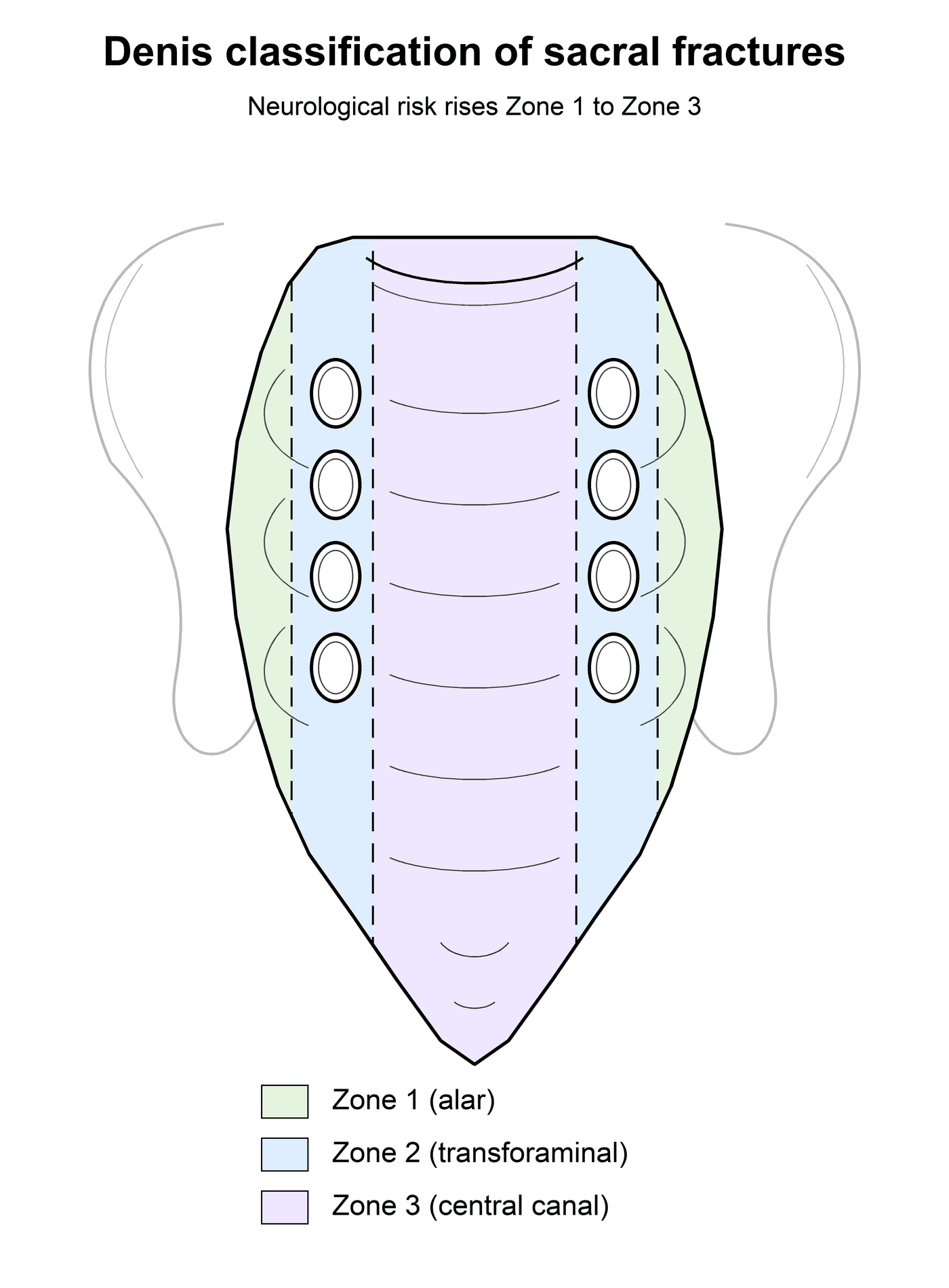
The FFP system grades the pelvic ring/stability; the Denis classification grades the sacral fracture itself by its medial–lateral position and predicts the neurological risk — and a sacral fracture topic that skips the nerve-root exam loses marks.
- Zone 1 (alar): lateral to the neural foramina, through the ala (the usual site of the insufficiency fracture's vertical limbs). Lowest neurological risk; if any, the L5 root (it runs over the ala).
- Zone 2 (transforaminal): through the foramina. Intermediate risk — unilateral L5/S1/S2 radiculopathy; a vertical-shear zone-2 pattern can be unstable.
- Zone 3 (central): medial to the foramina, into the central sacral canal. Highest neurological risk — bilateral deficits and bowel/bladder/sexual dysfunction (cauda equina). The transverse component of the H/U pattern, i.e. spinopelvic dissociation, is a zone-3 injury.
- Neurological injury rises with the zone (roughly 6%, 28% and 57% across zones 1–3 in the original Denis series).
- So examine the sacral roots in every case: L5 (dorsiflexion/EHL), S1 (plantarflexion, ankle jerk), and the S2–S4 sphincteric roots (perianal sensation, anal tone, urinary function) — a low-energy insufficiency fracture with a transverse/H (zone-3) pattern can still cause cauda equina and is a surgical red flag.
Clinical Presentation: the 'great mimicker'
- Low back, buttock or groin pain, sometimes radiating to the hip/thigh
- Difficulty weight-bearing / mobilising; pain worse with standing/walking
- Often insidious with no recalled injury (or trivial trauma)
- An elderly, often osteoporotic patient (or prior pelvic radiotherapy)
- Mimics mechanical low back pain, hip pathology, or metastatic disease
- Examination is often non-specific (sacral tenderness, pain on stressing the pelvis)
- Plain films are commonly normal — the diagnosis needs cross-sectional imaging
Investigations
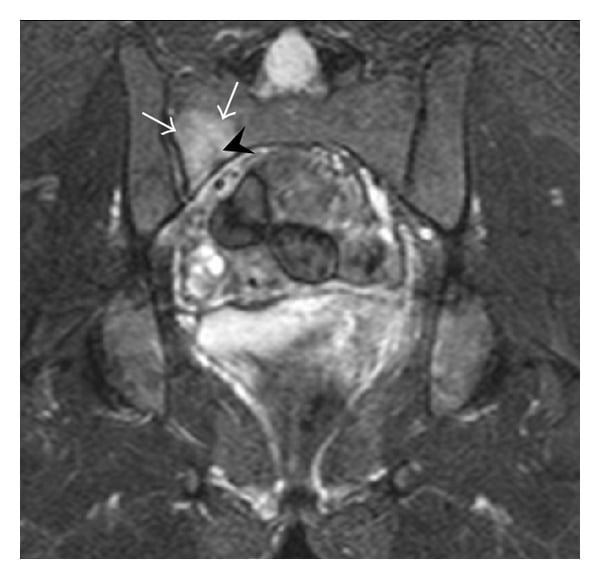
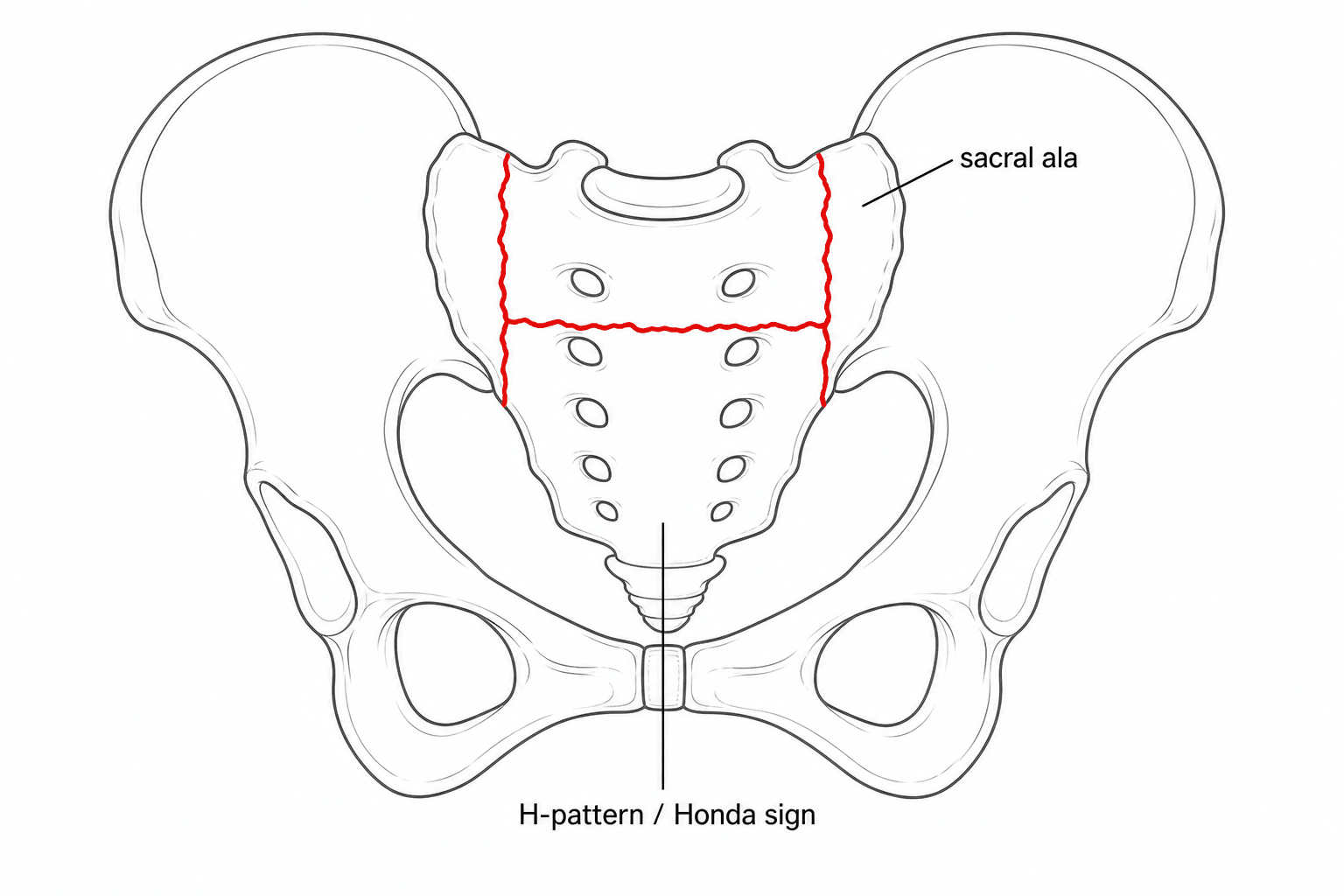
Plain radiographs are insensitive and frequently normal (overlying bowel gas, osteopenia and the sacral curvature obscure the fracture). CT is excellent for fracture morphology (a sclerotic fracture line/cortical break) and helps exclude a lytic/destructive lesion. MRI is the most sensitive test (around 99%), showing bone-marrow oedema in the sacral ala and the fracture line even when other imaging is normal — and it best distinguishes fracture from tumour. A bone scan classically shows the 'Honda sign' (an H-shaped pattern of increased uptake), though the full H is actually uncommon (~4% in one scintigraphy series) — so a missing H does not exclude the diagnosis.
"Exclude malignancy" is the refrain — but the examiner wants the discriminating features of a benign insufficiency fracture versus a metastasis/myeloma in the same elderly sacrum:
- Benign insufficiency fracture: a linear fracture line (often vertical in the ala, parallel to the SI joint); marrow signal change that is band-like and tracks ALONG the fracture line; the cortex is preserved; no soft-tissue mass; sclerosis along the line on CT (healing); a bilateral-symmetric H pattern is essentially diagnostic of benign disease.
- Malignant lesion: a focal, rounded/geographic destructive lytic lesion with cortical destruction/breakthrough; mass-like marrow replacement (a nodular low-T1 focus, not a thin band along a line); an associated soft-tissue / epidural mass; often multiple lesions elsewhere.
- When it is genuinely uncertain (atypical/asymmetric pattern, a focal mass, marrow change that does NOT track a fracture line, or a known primary): CT-guided biopsy, with myeloma/metastasis bloods (serum/urine electrophoresis and free light chains, calcium, PSA, the relevant tumour work-up). The bilateral-H morphology and oedema-along-the-line are what let you accept a benign fracture with confidence.
Management
The majority of sacral insufficiency fractures are managed conservatively: analgesia, early mobilisation (prolonged bed rest is harmful in the elderly), physiotherapy and fall prevention. Two things are non-negotiable: exclude malignancy, and investigate and treat the underlying osteoporosis (calcium/vitamin D, bone-protective therapy) — secondary fracture prevention is widely neglected (about 71% of patients do not receive it), yet the fracture is a sentinel event for further fragility fractures.
- 1Diagnose and exclude cancerMRI (most sensitive) or CT (morphology, excludes a lytic lesion) in an elderly patient with back/buttock pain and normal radiographs. Exclude metastasis/myeloma before accepting an insufficiency fracture, especially with an atypical pattern or known primary.
- 2Grade and treat conservatively firstGrade with the Rommens-Hofmann FFP system. Most (stable FFP I-II) are managed with analgesia, early mobilisation, physiotherapy and falls prevention — avoid prolonged bed rest.
- 3Treat the bone and the patientInvestigate and treat the osteoporosis (calcium/vitamin D + bone-protective therapy), arrange secondary fracture prevention, and involve orthogeriatrics — high morbidity and mortality in this group.
- 4Escalate for refractory pain or instabilitySacroplasty for refractory pain; percutaneous iliosacral/transsacral screws (often cement-augmented) for unstable/progressive posterior fractures; triangular lumbopelvic fixation or a transsacral bar for highly unstable patterns (FFP IV / spinopelvic dissociation).
- Indication / note
- Most fractures: analgesia, early mobilisation, fall prevention — plus osteoporosis treatment
- Indication / note
- Refractory pain: significant, often rapid PAIN relief and reduced analgesic use; limited stabilising capacity
- Indication / note
- Unstable or progressive posterior fractures (often cement-augmented in osteoporotic bone)
- Indication / note
- Highly unstable patterns (e.g. spinopelvic dissociation), bilateral/displaced fractures
- Indication / note
- Calcium/vitamin D + bone-protective therapy; secondary fracture prevention
A fragility fracture of the sacrum carries substantial morbidity in the elderly — loss of independence in 64–89% and mortality of 13–27% in reported series — and most patients are not on adequate bone-protective treatment. Treat it as a sentinel event: arrange bone-health assessment and secondary fracture prevention, orthogeriatric input, and a falls assessment, not just symptomatic relief.
The default for the stable majority (FFP I-II): analgesia, early mobilisation (avoid prolonged bed rest), physiotherapy and falls prevention - alongside, in every patient, osteoporosis treatment and orthogeriatric input.
Complications
- Complication
- Prolonged pain, immobility, deconditioning
- Note
- The 'great mimicker' is often missed on radiographs - delays mobilisation and care
- Complication
- Loss of independence (~64-89%) and mortality (~13-27%)
- Note
- Comparable to other major fragility fractures; mandates orthogeriatric care
- Complication
- Further fragility fractures
- Note
- A sentinel event - ~71% are not started on secondary fracture prevention
- Complication
- Progression to an unstable pattern
- Note
- Stable FFP can progress; influenced by bone density, pelvic morphology, sarcopenia - hence follow-up
- Complication
- VTE, pneumonia, pressure sores, decline
- Note
- Why early mobilisation (not bed rest) is the rule in the elderly
- Complication
- Cement leakage (sacroplasty); screw loosening/malposition
- Note
- Cement augmentation mitigates screw loosening in osteoporotic bone; sacral nerve roots at risk
The biggest 'complication' is treating the fracture and ignoring the bone. A sacral fragility fracture is a sentinel event: arrange bone-health assessment, secondary fracture prevention, a falls work-up and orthogeriatric input - and exclude malignancy - in every case.
Mnemonics & Memory Aids
- Insufficiency = weak (osteoporotic) bone + normal load; fatigue = normal bone + abnormal load.
- The 'great mimicker' — elderly, insidious back/buttock pain, often no injury, normal radiographs.
- MRI is most sensitive (~99%, marrow oedema); CT for morphology / exclude a lytic lesion.
- Honda sign = H-shaped bone-scan uptake — but the full H is the minority (~4%), so its absence doesn't exclude it.
- Always exclude malignancy and treat the osteoporosis (secondary prevention; ~71% currently miss it).
- Most conservative; sacroplasty for refractory pain, fixation (iliosacral/transsacral, triangular lumbopelvic) for unstable/progressive (Rommens-Hofmann FFP grade guides it).
SACRUMApproach
Hook:SACRUM: insufficiency stress fracture in the aged - exclude cancer, MRI it, mind the Honda sign, manage the bone.
HONDAThe Honda sign
Hook:The HONDA sign: H-pattern, osteoporotic, not always complete, diagnose on MRI/CT, augment/fix if needed.
POROUSCauses of weak bone
Hook:A POROUS sacrum: osteoporosis, radiotherapy, steroids/RA, osteomalacia/renal, hyperparathyroidism, Paget - the weak-bone causes.
Viva practice
Viva practice
Practise clinical reasoning and management decisions out loud
“An 78-year-old woman has 3 weeks of low back and buttock pain and difficulty walking, with no injury. Radiographs of the pelvis are normal. What is your differential and how do you investigate?”
“MRI confirms a sacral insufficiency fracture. How would you manage her, and when would you consider intervention or surgery?”
Exam cheat sheet
Definition
- Insufficiency stress fracture: weak (osteoporotic) bone, normal load
- vs fatigue fracture: normal bone, abnormal load
- Risk: osteoporosis, pelvic radiotherapy, steroids, RA, renal osteodystrophy
Presentation & imaging
- Elderly, insidious back/buttock/groin pain, hard to weight-bear, often no injury - the 'great mimicker'
- Radiographs usually normal; MRI most sensitive (~99%, marrow oedema); CT morphology / exclude lytic lesion
- Bone scan Honda/H sign (full H ~4%, uncommon); EXCLUDE malignancy
Classification
- Pattern: bilateral vertical alar + transverse = H (Honda); variants common
- Rommens-Hofmann FFP (I anterior → IV bilateral/unstable) guides treatment
- Progression to instability is common
Management
- Most conservative: analgesia, early mobilisation, falls prevention
- ALWAYS: exclude malignancy + treat osteoporosis (secondary prevention) + orthogeriatrics
- Sacroplasty for refractory pain; iliosacral/transsacral screws or triangular lumbopelvic fixation for unstable/progressive
Evidence Base
Comprehensive classification of fragility fractures of the pelvic ring: recommendations for surgical treatment
- Based on 245 consecutive patients, proposes the FFP classification graded by morphology and degree of instability (FFP I anterior only to FFP IV bilateral/displaced posterior).
- Most FFPs are minimally displaced and do NOT need surgery, but insidious progression to displacement, nonunion and instability occurs in some.
- The grade corresponds to instability and guides treatment, from minimally invasive techniques to complex reconstruction.
Chronic pelvic insufficiency fractures and their treatment
- Fragility/insufficiency fractures of the pelvis and sacrum are increasingly prevalent with high morbidity (loss of independence 64-89%, mortality 13-27%); 71% of patients do not receive adequate secondary fracture prevention.
- Radiography often misses sacral fractures; CT is the gold standard for morphology and MRI has the highest sensitivity (~99%) for bone oedema; the Rommens-Hofmann FFP classification guides treatment.
- Conservative treatment is possible; unstable/progressive fractures are treated surgically (sacroplasty, iliosacral screws, triangular lumbopelvic fixation, transsacral bars; cement augmentation improves osteoporotic fixation) within a multidisciplinary approach.
Inter- and intraobserver reliability and critical analysis of the FFP classification of osteoporotic pelvic ring injuries
- 100 pelvic CTs classified by 4 observers: overall interobserver reliability was MODERATE (kappa 0.42-0.59) and intraobserver reliability SUBSTANTIAL (kappa 0.68-0.72).
- Reliability was poorest for the subtypes involving a complete non-displaced or displaced sacral fracture (FFP IIc/IIIc/IVb).
- The acceptable-but-imperfect reliability, especially for the complex sacral subtypes, limits the FFP system's precision for clinical and research use.
Clinical and scintigraphic evaluation of insufficiency fractures in the elderly
- Of 194 elderly patients with scintigraphic insufficiency fractures, the typical H-shaped (Honda) sacral pattern was present in only 17 (4%) - its absence should not exclude the diagnosis; fractures were often at multiple sites (commonest the vertebrae).
- Of those with bone-density measured, 38 of 48 had osteoporosis/osteopenia.
- These patients had markedly poorer survival than the age-matched population, underscoring that making the diagnosis (and treating the bone) matters.
The FFP classification and its conservative-vs-operative logic come from Rommens & Hofmann 2013 (DOI); the imaging hierarchy, morbidity/under-treatment figures and treatment ladder from Gewiess et al. 2024 (DOI); the FFP reliability caveat from Krappinger et al. 2018 (DOI); and the point that the full Honda 'H' is uncommon (~4%) plus the poor-survival association from Wat et al. 2007 (DOI). The insufficiency-vs-fatigue definition is standard teaching. (See also our Osteoporosis and Fragility/Geriatric pelvic-fracture material.)