Low Back Pain Source | Provocative Tests | Injection
Causes
Critical Must-Knows
- 15-30% of low back pain may originate from SI joint
- Cluster of 3+ positive provocative tests supports diagnosis
- Fluoroscopic-guided injection (greater than 75% relief) confirms diagnosis
- Consider spondyloarthropathy in young patients (HLA-B27)
- SI joint fusion for refractory cases after failed conservative treatment
Clinical Pearls
- "FABER, Gaenslen's, thigh thrust, sacral compression, distraction tests
- "Pain typically over PSIS, may radiate to buttock/posterior thigh
- "MRI for inflammatory causes, plain film for degenerative
- "Injection both diagnostic and therapeutic
Clinical Imaging
Imaging Gallery


Critical SI Joint Exam Points
Diagnosis Challenge
SI joint pain is difficult to diagnose. No single test is diagnostic. Cluster of 3+ positive provocative tests increases likelihood. Injection is gold standard.
Red Flags
Consider spondyloarthropathy (ankylosing spondylitis, reactive arthritis) in young patients with inflammatory pattern pain (morning stiffness, improves with activity). Check HLA-B27, inflammatory markers.
Provocative Tests
FABER (Patrick's), Gaenslen's, Thigh Thrust, Sacral Compression, Distraction. 3+ positive = increased likelihood of SI joint origin.
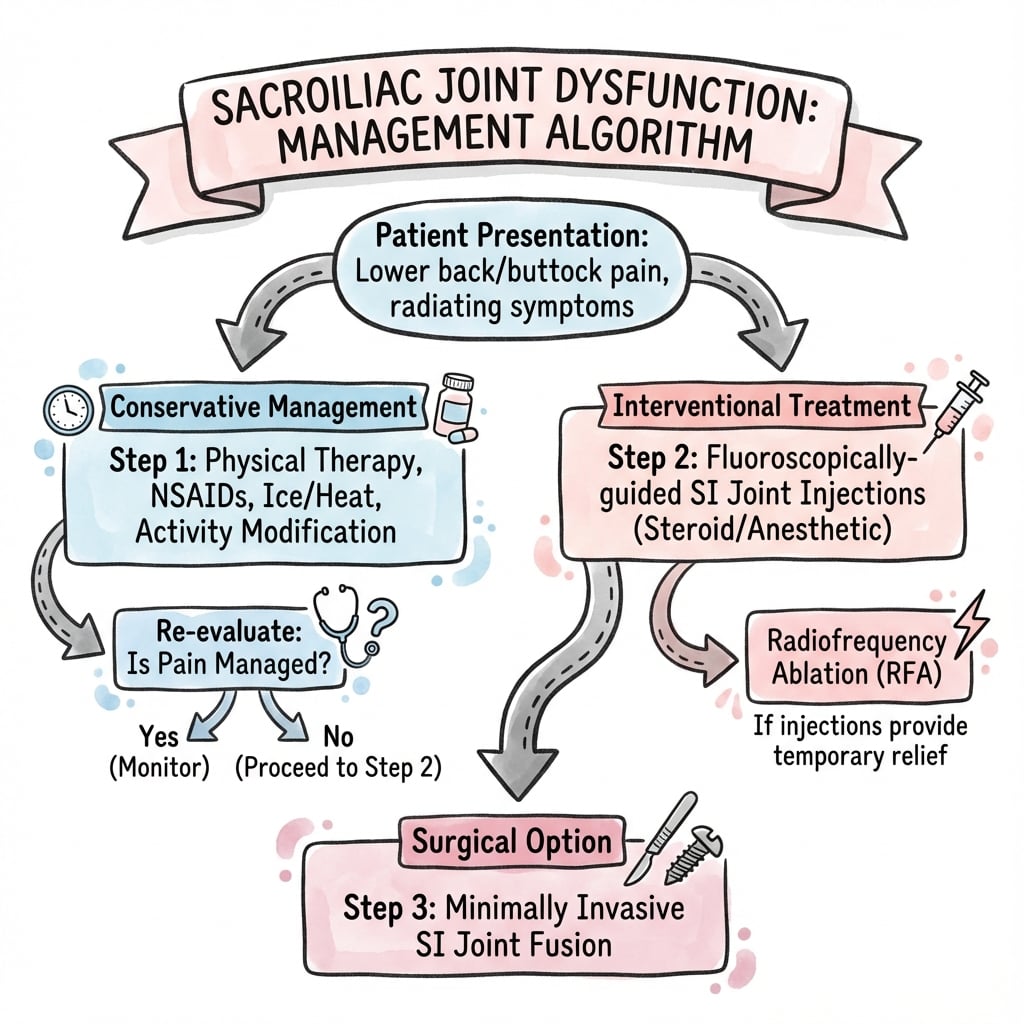
Treatment
Conservative: PT, injection, activity modification. Surgical: SI joint fusion for refractory cases. Minimally invasive techniques available.
At a Glance
Sacroiliac joint dysfunction is responsible for 15-30% of low back pain cases and is notoriously difficult to diagnose—no single test is definitive. A cluster of 3+ positive provocative tests (FABER, Gaenslen's, thigh thrust, sacral compression, distraction) increases diagnostic probability. Fluoroscopic-guided SI joint injection with over 75% pain relief is the gold standard for confirming the diagnosis. Pain typically localizes over the PSIS with radiation to the buttock or posterior thigh. In young patients with inflammatory pattern symptoms (morning stiffness, improvement with activity), consider spondyloarthropathy and check HLA-B27. Treatment progresses from conservative measures (physiotherapy, injection) to SI joint fusion for refractory cases.
FGTCDSI Joint Provocative Tests
| F | FABER (Patrick's) Flexion, Abduction, External Rotation |
| G | Gaenslen's Hip extended off table, other flexed |
| T | Thigh Thrust Axial load through flexed hip |
| C | Compression Lateral compression of pelvis |
| D | Distraction Press anterior pelvis apart |
| F | FABER (Patrick's) Flexion, Abduction, External Rotation | C | Compression Lateral compression of pelvis |
| G | Gaenslen's Hip extended off table, other flexed | D | Distraction Press anterior pelvis apart |
| T | Thigh Thrust Axial load through flexed hip |
Hook:FGTCD = FABER, Gaenslen's, Thigh thrust, Compression, Distraction!
IPAINInflammatory Back Pain Red Flags
| I | Insidious onset Gradual, not acute |
| P | Pain at night / second half Wakes patient, eases on rising |
| A | Age under 40 Young patient at onset |
| I | Improves with exercise Not relieved by rest |
| N | Nightly stiffness over 30 min Morning stiffness; check HLA-B27 |
| I | Insidious onset Gradual, not acute | I | Improves with exercise Not relieved by rest |
| P | Pain at night / second half Wakes patient, eases on rising | N | Nightly stiffness over 30 min Morning stiffness; check HLA-B27 |
| A | Age under 40 Young patient at onset |
Hook:IPAIN = think axial spondyloarthritis, not mechanical SI pain.
CMBDiagnostic Pathway
| C | Cluster of provocation tests 3+ of 6 positive raises suspicion |
| M | MRI for inflammation Bone-marrow oedema = sacroiliitis |
| B | Block confirms Image-guided injection, over 75% relief |
| C | Cluster of provocation tests 3+ of 6 positive raises suspicion |
| M | MRI for inflammation Bone-marrow oedema = sacroiliitis |
| B | Block confirms Image-guided injection, over 75% relief |
Hook:CMB = Cluster, MRI, Block - the three steps to a secure diagnosis.
Overview and Epidemiology
The sacroiliac (SI) joint is a diarthrodial synovial joint between the sacrum and ilium. It is a significant source of low back and buttock pain, estimated to cause 15-30% of non-radicular low back pain.
Anatomy
The SI joint has both synovial and ligamentous components. The posterior ligamentous complex is the primary stabilizer. Innervation is complex, with contributions from L4-S3 (posterior primarily S1-3). This makes diagnosis challenging.
Etiology
Mechanical: Hypermobility, asymmetric loading, leg length discrepancy.
Inflammatory: Ankylosing spondylitis and other spondyloarthropathies.
Traumatic: Post-pelvic fracture instability.
Degenerative: Osteoarthritis of SI joint.
Peripartum: Hormonal relaxation (relaxin), usually self-limiting.
Pathophysiology
Pain arises when load transfer across the joint becomes abnormal. Stability normally depends on form closure (interlocking auricular surfaces) and force closure (compression from the posterior ligamentous complex, gluteal, latissimus and abdominal muscle slings). Disruption of either, through ligament laxity (relaxin in pregnancy), trauma, asymmetric loading, adjacent-segment stress after lumbar fusion, or degenerative cartilage loss, generates nociception via the richly innervated posterior capsule and ligaments (L5 dorsal ramus and S1-S3 lateral branches). In inflammatory disease, synovitis and subchondral bone-marrow oedema drive an erosive then ankylosing process distinct from this mechanical pathway.
Anatomy
SI Joint Anatomy
Joint Structure
- Diarthrodial synovial joint between sacrum and ilium
- Auricular (ear-shaped) surfaces interlock for stability
- Irregular surface topography increases friction and stability
- Small range of motion (1-4° rotation, 1-2mm translation)
Ligamentous Stabilizers
- Anterior sacroiliac ligament: Thin, covers anterior joint
- Posterior sacroiliac ligaments: Short and long posterior ligaments, primary stabilizers
- Interosseous sacroiliac ligament: Strongest, fills posterior joint space
- Sacrotuberous and sacrospinous ligaments: Contribute to pelvic stability
Innervation
- Complex and variable
- Posterior innervation: L5 dorsal ramus, S1-S4 lateral branches
- Anterior innervation: L2-S2 contributions
- Explains referred pain patterns to buttock, posterior thigh, groin
Classification
Classification by Etiology
Mechanical SI Joint Dysfunction
- Hypermobility or hypomobility
- Leg length discrepancy
- Asymmetric loading patterns
- Post-trauma (falls, motor vehicle accidents)
Inflammatory SI Joint Disease
- Ankylosing spondylitis
- Reactive arthritis
- Psoriatic arthritis
- Inflammatory bowel disease-associated arthritis
- Characterized by sacroiliitis on imaging
Degenerative SI Joint Arthritis
- Osteoarthritis of SI joint
- More common in older patients
- Sclerosis and osteophyte formation
Peripartum-Related
- Hormonal effects (relaxin) causing ligament laxity
- Usually self-limiting postpartum
- May require treatment if persistent
Clinical Presentation
History
Pain typically located over the posterior superior iliac spine (PSIS) or "Fortin's area." May radiate to buttock, posterior thigh, or groin. Rarely below the knee. Worse with sitting, transitional movements, or prolonged standing. May note stiffness.
Inflammatory Pattern (consider spondyloarthropathy): Young patient (less than 40 years), insidious onset, morning stiffness greater than 30 minutes, improves with activity, not relieved by rest.
Examination
Provocative Tests: 3 or more positive tests increase likelihood of SI joint origin.
FABER (Patrick's Test): Flexion, Abduction, External Rotation of hip. Pain at SI joint suggests SI pathology (also stresses hip).
Gaenslen's Test: Patient supine. One hip flexed to chest, other hip extended off table edge. Stresses SI joint.
Thigh Thrust (Posterior Shear Test): Supine, hip flexed 90°. Axial load through femur toward SI joint.
Sacral Compression Test: Side-lying. Downward pressure on ilium.
Distraction Test: Supine. Posterior force on ASISs to distract anterior pelvis.
Differential Diagnosis
SI joint pain overlaps heavily with other axial and gluteal pain generators. Multiple sources frequently coexist, so the table below is a guide to dominant features rather than mutually exclusive diagnoses.
Differential Diagnosis of SI Joint Pain
| Condition | Pain Location | Discriminating Features | Confirmatory Test |
|---|---|---|---|
| SI joint dysfunction | Below L5 over PSIS (Fortin area), buttock, posterior thigh, rarely below knee | Worse sitting and sit-to-stand transitions, 3+ provocation tests positive | Image-guided intra-articular block (over 75% relief) |
| Lumbar facet arthropathy | Paraspinal low back, buttock | Worse with extension and rotation, less PSIS-focal | Medial branch blocks L4-L5/L5-S1 |
| Lumbar radiculopathy / disc | Radiating below knee in dermatomal pattern | Positive SLR, neurological deficit, dermatomal sensory loss | MRI lumbar spine plus selective nerve root block |
| Hip / FAI / labral pathology | Groin, anterior thigh, C-sign grip | Positive FADIR, pain-limited hip ROM, groin pain | Intra-articular hip block, hip MRI/MR arthrogram |
| Greater trochanteric pain syndrome / gluteal tendinopathy | Lateral hip, point tenderness over trochanter | Pain on single-leg stance and side-lying, no PSIS focus | Ultrasound/MRI, peritrochanteric injection |
| Inflammatory sacroiliitis (axial SpA) | Bilateral buttock, alternating | Age under 40, inflammatory back pain, morning stiffness over 30 min, HLA-B27 | MRI bone marrow oedema, raised CRP |
| Piriformis / deep gluteal syndrome | Deep buttock, sciatic distribution | Pain on resisted external rotation, sitting intolerance | Diagnostic piriformis/peri-sciatic block |
Diagnosis
Gold Standard: Fluoroscopic or CT-guided injection of local anesthetic into the SI joint.
Diagnostic Criteria: Greater than 75% pain relief following injection confirms SI joint as pain source.
Therapeutic: Corticosteroid can be included for therapeutic effect.
This is the most reliable method to confirm SI joint origin given the limitations of clinical testing.
Investigations
Imaging
Plain Radiographs
- AP pelvis: Assess joint margins, sclerosis, osteophytes
- Ferguson view: Angled for better SI joint visualization
- May show degenerative changes or advanced sacroiliitis
MRI
- Gold standard for detecting sacroiliitis
- Shows bone marrow edema (active inflammation)
- Detects erosions, sclerosis, fatty replacement
- STIR or fat-saturated T2 sequences best for edema
CT Scan
- Better bony detail than MRI
- Shows erosions, sclerosis, ankylosis
- Useful for surgical planning
Laboratory
- Inflammatory markers: ESR, CRP (elevated in sacroiliitis)
- HLA-B27: Positive in most ankylosing spondylitis patients
- Rheumatoid factor: Usually negative in spondyloarthropathy
Management
Physiotherapy: Core strengthening, pelvic stabilization, stretching.
Activity Modification: Avoid aggravating activities.
SI Belt: External support for hypermobility.
Injection: Intra-articular corticosteroid. May provide lasting relief. Can repeat.
Pharmacotherapy: NSAIDs (especially for inflammatory pain). DMARDs/biologics for spondyloarthropathy.
Surgical Technique
SI Joint Fusion Techniques
Minimally Invasive Lateral Transiliac Approach
- Most common modern technique
- Small lateral incision over ilium
- Fluoroscopic guidance essential
- Triangular titanium implants placed across joint
- Typically 3 implants in triangular configuration
Key Steps
- Patient positioning: Prone or lateral
- Fluoroscopic setup: AP and lateral views
- Small incision over lateral ilium
- Guidewire placement across SI joint
- Sequential drilling and implant placement
- Confirm position on multiple views
Open SI Joint Fusion
- Indicated for traumatic instability
- Anterior or posterior approach
- Cartilage debridement and bone grafting
- Screw or plate fixation
Complications
Complications
Nerve Injury
- L5 nerve root: Lateral approach risk
- S1 nerve root: If implants too superior
- Sciatic nerve: Rare, from malpositioning
- Prevention: Fluoroscopic guidance, stay below S1 foramen
Hardware-Related
- Implant malposition
- Implant prominence (buttock pain)
- Implant loosening or migration
- Pseudarthrosis (failed fusion)
Persistent Pain
- Most common "complication"
- May indicate incorrect diagnosis or adjacent pathology
- Rate: 15-30% of patients
Other Complications
- Wound infection
- Hematoma
- DVT/PE
- Adjacent segment degeneration
Postoperative Care
Postoperative Protocol
Immediate Postoperative
- Pain control: Multimodal analgesia
- Wound care: Keep dry, monitor for infection
- DVT prophylaxis: Mechanical and pharmacological
Weight-Bearing
- Variable protocols depending on technique
- MIS with triangular implants: Often weight-bearing as tolerated
- Open fusion: May require protected weight-bearing 6-8 weeks
Activity Restrictions
- Limit twisting and bending initially
- Avoid prolonged sitting (aggravates SI joint)
- Gradual return to normal activities over 6-12 weeks
Physiotherapy
- Begin after initial healing phase (2-4 weeks)
- Core strengthening and pelvic stabilization
- Gait training if needed
Outcomes
Treatment Outcomes
Conservative Treatment
- Physiotherapy: Variable success, better for mild cases
- SI joint injection: 50-70% get temporary relief
- Repeat injections: May provide ongoing benefit
Radiofrequency Ablation
- 60-70% significant pain reduction
- Duration: 6-12 months typically
- Can be repeated if symptoms recur
Surgical Fusion
- Success rate: 70-85% significant improvement
- Fusion rate: 85-95% radiographic fusion
- Time to maximum improvement: 6-12 months
Factors Affecting Outcomes
- Positive diagnostic injection response (most important)
- Patient selection and realistic expectations
- Technique and implant choice
- Presence of other pain generators
Evidence Base
- 48 patients examined with provocation tests then intra-articular anaesthetic block as reference standard
- Three or more of six positive tests: sensitivity 94%, specificity 78%
- If none of the six tests reproduce familiar pain, the SI joint can be ruled out as the source
- No single test alone is diagnostic
- 54 patients with unilateral LBP and SI-pattern pain assessed with double diagnostic blocks
- Confirmed SI joint pain prevalence of 18.5% (10/54) on confirmatory block
- No individual provocation test reached statistical significance against the block standard
- Establishes the SI joint as a real but over-diagnosed pain source
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Buttock Pain
"A 45-year-old woman has low back and right buttock pain for 6 months. MRI spine is unremarkable. How do you assess for SI joint dysfunction?"
Scenario 2: Equivocal Provocative Tests - Diagnostic Dilemma
"A 52-year-old male office worker presents with 12 months of right-sided low back and buttock pain. He describes the pain as localized over the right PSIS with occasional radiation to the posterior thigh, never below the knee. The pain is worse with sitting for prolonged periods and with transitional movements from sitting to standing. He has tried physiotherapy for 6 months with minimal benefit. MRI lumbar spine shows mild L4-5 and L5-S1 facet arthropathy bilaterally, but no significant disc pathology, stenosis, or nerve root compression. On examination, FABER test is positive on the right (reproduces his typical pain), Gaenslen's test is equivocal (some discomfort but not clearly positive), thigh thrust is negative, sacral compression is positive, and distraction is negative. So you have 2 clearly positive tests, 1 equivocal, and 2 negative. Hip examination shows full range of motion with no pain. There is no neurological deficit. The patient is frustrated and asks for a definitive diagnosis and treatment plan. How do you approach this diagnostic dilemma, and what is your management strategy?"
Scenario 3: Failed SI Joint Fusion - Persistent Pain After Surgery
"A 48-year-old woman underwent minimally invasive SI joint fusion 9 months ago for chronic right SI joint pain that had been refractory to 18 months of conservative treatment including physiotherapy, SI belt, and multiple corticosteroid injections. Pre-operatively, she had a cluster of 4 positive provocative tests and 85% pain relief with diagnostic SI joint injection, confirming the SI joint as the pain source. She underwent lateral transiliac approach with placement of three triangular titanium implants across the right SI joint. Initial post-operative X-rays showed good implant position. However, she now presents to your clinic complaining that her pain has never improved after surgery - she rates it as 7/10 (same as pre-operative). The pain remains localized over the right PSIS and buttock. She is frustrated, has been off work for 9 months, and is demanding answers. On examination, she has tenderness over the right SI joint, 3 positive provocative tests on the right (same as pre-op), and no neurological deficit. CT scan shows the three implants in good position crossing the SI joint with some bridging bone formation around the implants, but no complete fusion visible. There is no implant loosening, fracture, or migration. Inflammatory markers are normal (CRP less than 5, ESR 12). What is your differential diagnosis for persistent pain after SI joint fusion, how do you investigate this patient, and what are your management options?"
MCQ Practice Points
Diagnosis
Q: What is the gold standard for diagnosing SI joint as pain source? A: Fluoroscopic-guided injection of local anesthetic. Greater than 75% pain relief confirms SI joint origin.
Clinical Tests
Q: How many positive provocative tests support SI joint dysfunction? A: 3 or more positive tests (from FABER, Gaenslen's, thigh thrust, compression, distraction) increases likelihood of SI joint origin (Laslett: sensitivity 94%, specificity 78%).
Surgical Evidence
Q: What is the evidence for minimally invasive SI joint fusion? A: Two Level I RCTs (INSITE, iMIA) show MIS triangular-implant fusion is superior to conservative care at 6-12 months (INSITE 6-month success 81% vs 26%). Caveats: unblinded, single device, industry-sponsored; outcome depends on an injection-confirmed diagnosis.
Controversies & Areas of Uncertainty
The SI joint remains one of the most debated pain generators in spine practice. Examiners reward a candidate who can articulate where the evidence is genuinely soft.
- Does the diagnosis even exist as a discrete entity? Provocation tests have no validated reference standard beyond the response to anaesthetic block, and the block itself has imperfect reliability (single vs double/comparative blocks give very different prevalence figures). Maigne reported only 18.5% confirmed on double block, while clinical series quote 15-30%.
- Block threshold is arbitrary. The widely used "over 75% relief" cut-off is convention, not a validated criterion; placebo response and anaesthetic spread to adjacent structures (dorsal rami, L5, posterior ligaments) confound the result. Comparative or placebo-controlled blocks reduce false positives but are rarely performed.
- Surgical evidence is industry-linked. The pivotal RCTs (INSITE, iMIA) and the pooled analysis were sponsored by the device manufacturer, were unblinded, used a single implant system, and compared against conservative care that itself was not standardised. Effect sizes are large but the risk of bias is real. There is no head-to-head RCT of fusion vs sham surgery.
- Patient selection drives outcome more than technique. A secure injection-confirmed diagnosis, exclusion of concurrent hip/lumbar pathology, and avoidance of central sensitisation matter more than the specific construct. Smoking and opioid use predict worse results.
- Lateral-branch RFA is intermediate at best. Variable lateral-branch anatomy limits reliable denervation; benefit typically lasts 6-12 months and trials are small.
- Imaging does not diagnose mechanical SI pain. MRI/CT confirm inflammatory sacroiliitis but degenerative changes correlate poorly with symptoms, so the diagnosis stays clinical plus block-based.
Guidelines, Registries & Global Practice
Global Epidemiology
- The SI joint accounts for an estimated 15-30% of chronic non-radicular low back pain, with double-block studies giving more conservative figures (~18%).
- Higher risk in peripartum women (relaxin-mediated laxity), patients with prior lumbar fusion (adjacent-segment loading), manual workers, and after pelvic trauma.
- Inflammatory sacroiliitis (axial spondyloarthritis) is a distinct entity with population prevalence of ankylosing spondylitis around 0.1-0.5%, strongly HLA-B27 associated.
Guidelines Side by Side
How Major Bodies Frame SI Joint Pain
| Body / Region | Diagnostic Stance | Surgical Fusion Position |
|---|---|---|
| NICE / BOA (UK) | Treat non-specific LBP conservatively; image-guided block to localise | Cautious; MIS fusion via interventional/registry pathways with strict selection |
| NASS (US) | Coverage criteria require positive history/exam plus 75%+ relief on dual diagnostic blocks | MIS fusion appropriate only after documented failed conservative care and confirmatory blocks |
| ISASS / spine-device guidance | Cluster of provocation tests plus image-guided intra-articular block | Supports MIS triangular-implant fusion in selected, injection-confirmed patients |
| ASAS / EULAR (rheumatology) | MRI bone-marrow oedema plus clinical criteria for axial SpA | Not surgical; biologic DMARDs (TNF/IL-17 inhibitors) for inflammatory disease |
Registry & Outcome Notes
- There is no dedicated international SI joint fusion registry comparable to arthroplasty registries; long-term data derive mainly from manufacturer-sponsored trials and device databases.
- Reported revision rates are roughly 5-10% at 2-5 years in the RCT cohorts; longer real-world durability is uncertain.
- Adverse-event surveillance (e.g. device-malfunction reporting databases) has flagged implant malposition and neural irritation as the principal device-related harms.
High- vs Limited-Resource Practice
- High-resource settings: ready access to fluoroscopy/CT for confirmatory blocks, MRI for sacroiliitis, RFA, and MIS fusion with image guidance and navigation.
- Limited-resource settings: diagnosis rests on a careful provocation-test cluster and a clinically guided or single fluoroscopic block; management is predominantly physiotherapy, NSAIDs, an SI belt and intermittent steroid injection, with fusion reserved for the few centres with implants and fluoroscopy.
- For inflammatory disease, access to biologics is the main global divide; where unavailable, NSAIDs and physiotherapy remain the backbone.
Exam Viva Point
Global framing for the viva: the diagnosis is clinical plus a confirmatory image-guided block; rheumatology guidelines (ASAS/EULAR) own the inflammatory pathway (MRI oedema, HLA-B27, biologics) while spine/device guidance (NASS/ISASS) owns the mechanical pathway. Surgical evidence is Level I but unblinded and industry-sponsored, so quote the trials and their limitations together.
SI JOINT DYSFUNCTION
Clinical summary
Key Facts
- •15-30% of low back pain
- •Pain over PSIS (Fortin's area)
- •Radiates to buttock, posterior thigh
- •Cluster of 3+ tests positive
Provocative Tests (FGTCD)
- •FABER (Patrick's)
- •Gaenslen's
- •Thigh Thrust
- •Compression
- •Distraction
Diagnosis
- •Injection is gold standard
- •Greater than 75% relief confirms
- •MRI for inflammatory causes
- •XR for degenerative
Red Flags
- •Young patient (less than 40)
- •Morning stiffness greater than 30 min
- •Improves with activity
- •Consider spondyloarthropathy