Seronegative Spondyloarthropathy
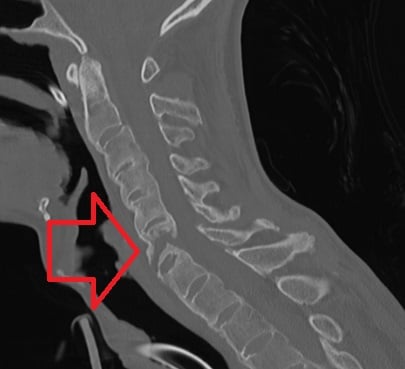
- The ankylosed 'bamboo' spine fractures dangerously after MINOR trauma - an unstable, usually extension/hyperextension (AO B3) three-column injury, easily missed on plain films, prone to displacement, epidural haematoma and cord injury. New spinal pain in an AS patient = unstable fracture until proven otherwise: CT the WHOLE spine, immobilise in the patient's HABITUAL posture (never force a fixed-kyphosis patient flat).
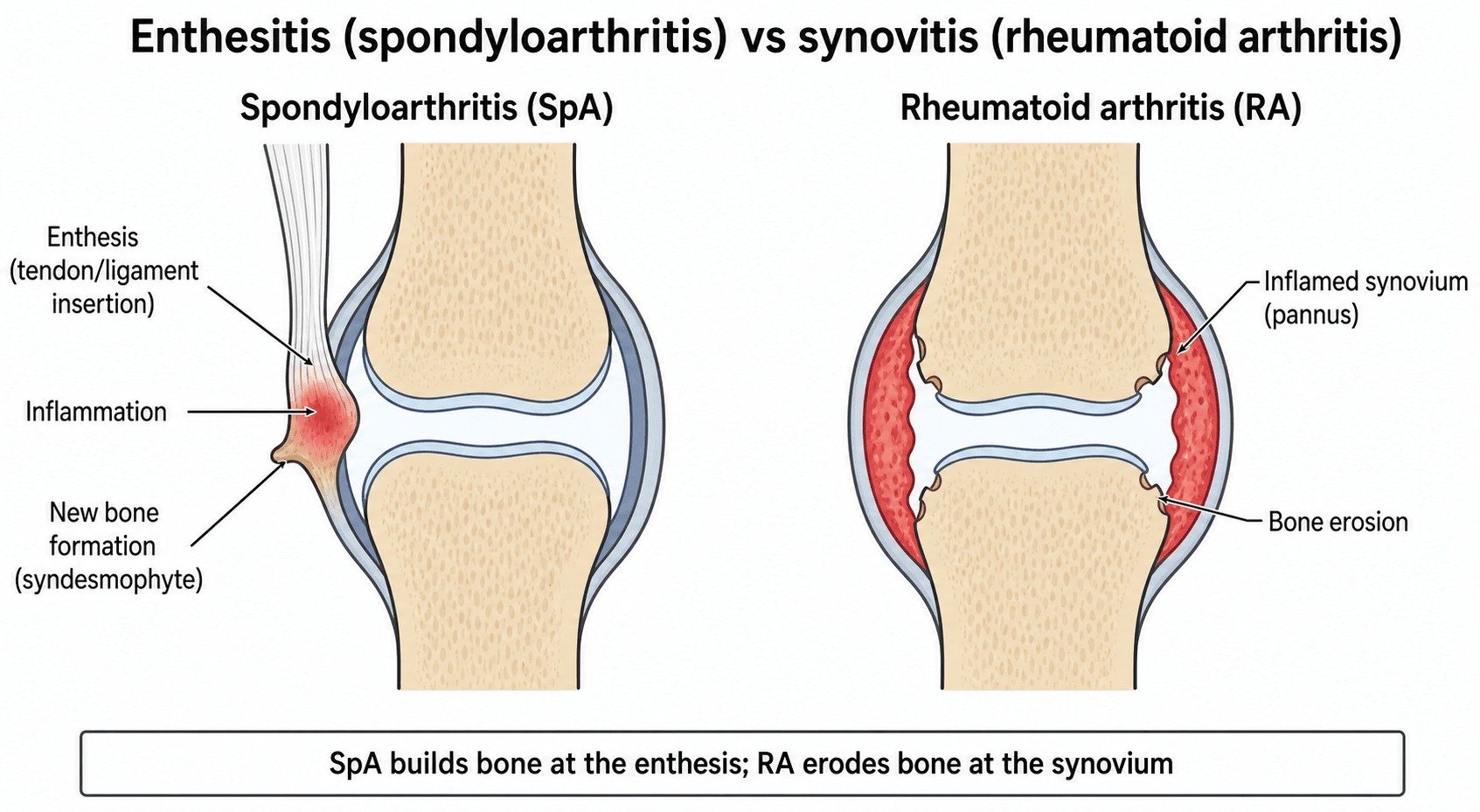
- SpA BUILDS bone (syndesmophytes/ankylosis); RA ERODES. SpA is seronegative, axial/asymmetric large-joint, enthesis-centred; RA is seropositive, symmetric small-joint, synovium-centred. Don't swap them.
- Enthesitis - not synovitis - is the defining lesion (it explains dactylitis, heel pain and the new-bone formation).
- HLA-B27 is neither necessary nor sufficient - most have it (strongest in AS) but it is a marker, not a diagnostic test.
- MRI sacroiliac bone-marrow oedema detects EARLY (non-radiographic) axial SpA before radiographs change - don't wait for the bamboo spine.
- Conventional DMARDs (sulfasalazine/methotrexate) do NOT work for AXIAL disease - they help peripheral arthritis only; axial refractory disease needs a biologic (anti-TNF/IL-17) or JAK inhibitor.
Overview & Epidemiology
The seronegative spondyloarthropathies are a unifying rheumatology framework the exam loves: one family, one shared biology, and a distinctive orthopaedic hazard (the fracture-prone ankylosed spine). Recognising the pattern - seronegative, HLA-B27, enthesis-centred, new-bone-forming - lets you place any individual subtype.
- Onset typically in the third decade; axial SpA has a male predominance for the radiographic (ankylosing spondylitis) form (~2:1) and roughly 1:1 for non-radiographic axial SpA.
- Strongly heritable - over 90% heritability for ankylosing spondylitis, with HLA-B27 the dominant genetic association.
- A spectrum, not silos: ankylosing spondylitis / axial SpA, psoriatic, reactive, enteropathic and juvenile/undifferentiated - linked by the gut-joint axis and the IL-23/IL-17 pathway.
- Why orthopaedics cares: the late ankylosed (bamboo) spine is biomechanically a long bone and fractures unstably after minor trauma, with high morbidity.
Pathophysiology: enthesitis, HLA-B27 & the IL-23/IL-17 axis
- The enthesis, not the synovium, is the primary site - inflammation begins where tendon/ligament/capsule inserts into bone, explaining dactylitis, Achilles/plantar heel pain and spinal disease.
- HLA-B27 is the dominant genetic association (its precise pathogenic role - misfolding, the 'arthritogenic peptide' and free heavy-chain hypotheses - remains debated); it is a marker, not necessary or sufficient.
- The IL-23/IL-17 axis (with TNF-α) drives the inflammation - the rationale for anti-TNF and anti-IL-17 therapy; the gut-joint axis links subclinical bowel inflammation to joint disease.
- Repair by OSSIFICATION: unlike the erosive synovitis of RA, SpA enthesitis heals with new-bone formation - syndesmophytes, ankylosis and the bamboo spine - so SpA characteristically builds bone while RA erodes it.
The family & what unites it
The seronegative spondyloarthropathies usually start in the third decade, are rheumatoid-factor (and anti-CCP) negative, carry the HLA-B27 marker, and share axial and peripheral arthritis, dactylitis, enthesitis and extra-articular manifestations. The family is ankylosing spondylitis (now within the axial spondyloarthritis concept), psoriatic arthritis, reactive arthritis, enteropathic (IBD-associated) arthritis, and juvenile-onset / undifferentiated SpA. Joint and gut inflammation are intimately linked (the gut-joint axis), with shared genetics and the IL-23/IL-17 pathway.
- Distinguishing features
- Inflammatory back pain, sacroiliitis, ascending ankylosis; strongest HLA-B27 link
- Distinguishing features
- Psoriasis, nail pitting/onycholysis, DIP involvement, dactylitis; axial or peripheral patterns
- Distinguishing features
- 1–4 weeks after GU (Chlamydia) or GI infection; arthritis + urethritis + conjunctivitis
- Distinguishing features
- Arthritis with Crohn's/ulcerative colitis; peripheral often mirrors gut activity, axial does not
- Distinguishing features
- Childhood onset; or SpA features not meeting a single subtype
Investigations
- Bloods: RF and anti-CCP NEGATIVE (hence 'seronegative'); HLA-B27 positive in most (strongest in AS) but neither necessary nor sufficient; raised CRP/ESR in active disease.
- Radiographs: sacroiliitis (erosion/sclerosis/fusion), syndesmophytes, vertebral 'squaring', and the fused 'bamboo spine' in advanced AS.
- MRI: detects early disease — bone-marrow oedema at the sacroiliac joints/spine — defining non-radiographic axial SpA before radiographic changes appear.
Classification (e.g. the ASAS criteria for axial and peripheral SpA) integrates clinical features, HLA-B27, CRP and imaging.

The other ankylosing spine that fractures dangerously is DISH (diffuse idiopathic skeletal hyperostosis / Forestier disease) — a non-inflammatory mimic the examiner sets against AS (and the comparator in the Tan evidence card):
- DISH: flowing, bulky, NON-marginal ossification ("dripping candle wax") along the anterolateral aspect of at least four contiguous vertebrae, with PRESERVED disc heights, NO erosive sacroiliitis and NO apophyseal (facet) joint fusion (Resnick criteria). Older patients (typically over 50), male, associated with type-2 diabetes / metabolic syndrome / obesity; HLA-B27 not associated.
- Ankylosing spondylitis: erosive bilateral symmetric SACROILIITIS (the hallmark), thin MARGINAL vertical syndesmophytes, vertebral squaring, facet ankylosis; inflammatory, younger (third decade), HLA-B27-associated.
- Both ankylose and both fracture dangerously as a long bone — but only AS shows sacroiliitis and erosion, and AS patients are more frail with higher fracture-fixation morbidity (Tan).
- Other sacroiliitis mimics: osteitis condensans ilii (triangular iliac-side sclerosis, parous women, no erosion), osteoarthritis (sclerosis/osteophytes, no erosion), and septic sacroiliitis (usually unilateral).
Management
- First line (axial disease): NSAIDs and a structured exercise/physiotherapy programme — the cornerstone for axial SpA.
- Conventional DMARDs (sulfasalazine, methotrexate): useful for PERIPHERAL arthritis but NOT effective for axial disease.
- Biologics/targeted therapy: anti-TNF, anti-IL-17 (secukinumab) and JAK inhibitors for active/refractory axial or peripheral disease; tailor to the EAMs (e.g. an anti-TNF monoclonal for coexisting IBD/uveitis).
- Treat-to-target, early diagnosis and managing comorbidities (osteoporosis, cardiovascular risk). Care is multidisciplinary (rheumatology + gastroenterology/dermatology/ophthalmology for the EAMs).
The fused 'bamboo' spine behaves biomechanically like a long bone: even low-energy trauma can cause a highly unstable, often extension-type, three-column fracture (frequently through the rigid disc/bone segment). These fractures are easily missed on plain films, are prone to displacement and epidural haematoma, and carry a high risk of spinal-cord injury. In any AS patient with new spinal pain after even trivial trauma, assume an unstable fracture, CT (and often MRI) the WHOLE spine, and immobilise in the patient's habitual posture (do not force a fixed-kyphosis patient flat).
First line: NSAIDs + a structured exercise/physiotherapy programme - the cornerstone for axial SpA. Conventional DMARDs do not work here. Active/refractory axial disease escalates to a biologic (anti-TNF or anti-IL-17) or a JAK inhibitor.
Complications
- Complication
- Unstable fracture of the ankylosed spine
- Note
- Long-bone behaviour; minor trauma → extension/B3 3-column fracture; high morbidity/complications
- Complication
- Spinal-cord injury, epidural haematoma, displacement
- Note
- Easily missed; cervical especially; CT the whole spine, immobilise in habitual posture
- Complication
- Progressive fixed kyphosis
- Note
- May need corrective osteotomy in selected patients
- Complication
- Acute anterior uveitis, IBD flares, psoriasis
- Note
- The gut-joint-eye axis; coordinate multidisciplinary care
- Complication
- Aortitis/conduction disease, apical lung fibrosis, IgA nephropathy, amyloidosis
- Note
- Less common but examinable extra-articular sequelae
- Complication
- Osteoporosis + cardiovascular risk
- Note
- Osteoporosis compounds the fracture risk; treat proactively
Never treat new spinal pain in an ankylosing-spine patient as 'mechanical'. Even a trivial mechanism can produce an unstable fracture with a high cord-injury and complication rate - CT the whole spine, involve spinal surgery early, and immobilise in the patient's habitual posture.
Mnemonics & Memory Aids
- Seronegative (RF/anti-CCP negative) + HLA-B27; the family = PAIR (Psoriatic, Ankylosing, IBD-associated, Reactive) + juvenile/undifferentiated.
- Enthesitis is the defining lesion (not synovitis); plus dactylitis, inflammatory back pain, EAMs (uveitis/psoriasis/IBD).
- SpA builds bone (syndesmophytes/ankylosis, bamboo spine); RA erodes; SpA is axial/asymmetric large-joint vs RA's symmetric small joints.
- MRI sacroiliac bone-marrow oedema detects early (non-radiographic) axial SpA.
- Ladder: NSAIDs + exercise (axial) → DMARDs (peripheral only) → biologics (anti-TNF/IL-17, JAK).
- The ankylosed spine fractures dangerously — unstable extension-type from minor trauma; CT the whole spine.
PAIRThe family
Hook:The seronegative SpA family is a PAIR: Psoriatic, Ankylosing, IBD-associated, Reactive (+ juvenile/undifferentiated).
SPINEACHEThe SpA features
Hook:SPINEACHE captures the spondyloarthritis features - the classic SpA screening checklist.
BAMBOOThe fractured ankylosed spine
Hook:A BAMBOO spine fracture: long-bone behaviour, image it all, easily missed, immobilise as-is, fix it long - high complications.
Viva practice
Viva practice
Practise clinical reasoning and management decisions out loud
“What unifies the seronegative spondyloarthropathies, what conditions are in the family, and how do they differ from rheumatoid arthritis?”
“An ankylosing spondylitis patient with a fused spine presents with new neck pain after a minor fall. Why does this worry you, and how do you investigate and manage it?”
Exam cheat sheet
The family & what unites it
- RF/anti-CCP negative; HLA-B27 associated
- AS/axial SpA, psoriatic, reactive (Reiter's), enteropathic (IBD), juvenile/undifferentiated
- Shared: inflammatory back pain/sacroiliitis, enthesitis, dactylitis, EAMs (uveitis/psoriasis/IBD)
vs RA
- SpA: seronegative, axial/asymmetric large-joint, enthesis-centred, NEW bone (syndesmophytes/ankylosis)
- RA: seropositive, symmetric small-joint, erosive
- Enthesitis is the defining lesion of SpA
Investigations
- RF/anti-CCP negative; HLA-B27 (not necessary/sufficient); CRP/ESR up
- X-ray: sacroiliitis, syndesmophytes, bamboo spine
- MRI: sacroiliac bone-marrow oedema (non-radiographic axial SpA); ASAS criteria
Management & ortho hazard
- NSAIDs + exercise first-line (axial); DMARDs for peripheral only; biologics (anti-TNF/IL-17, JAK)
- Treat-to-target; manage EAMs and comorbidities (osteoporosis, CV risk)
- Ankylosed (bamboo) spine: unstable extension fractures from minor trauma - CT whole spine, treat as unstable
Evidence Base
Axial spondyloarthritis
- Axial SpA spans non-radiographic and radiographic (ankylosing spondylitis) disease; onset in the third decade, M:F ~2:1 for radiographic and ~1:1 for non-radiographic.
- Over 90% heritability, with HLA-B27 the strongest genetic association (its pathogenic role still debated); TNF-α and IL-17 are central to pathogenesis.
- MRI is the most important imaging method for early diagnosis; NSAIDs and TNF blockers are effective, and IL-17 blockade is a relevant newer option.
Seronegative spondyloarthropathy-associated inflammatory bowel disease
- Seronegative SpA starts in the third decade with negative rheumatoid factor and the HLA-B27 marker, and features spinal and peripheral arthritis, dactylitis, enthesitis and extra-articular manifestations.
- It is classified as ankylosing spondylitis, psoriatic arthritis, reactive arthritis, enteropathic arthritis or juvenile-onset SpA, with joint and gut inflammation intricately linked (shared genetic/immunopathogenic mechanisms).
- NSAIDs first-line for peripheral and axial SpA; conventional DMARDs help peripheral but not axial disease or IBD; anti-TNF monoclonal antibodies are effective across SpA and IBD; JAK inhibitors are emerging.
Clinical management of psoriatic arthritis
- Psoriatic disease is a multi-organ inflammatory disorder (skin and joints) with extra-articular manifestations, comorbidities and a substantial clinical burden.
- Early identification, timely diagnosis and treatment are crucial to prevent long-term structural damage and disability.
- Biologic and targeted synthetic DMARDs have transformed treatment; strategies include treat-to-target, early remission-induction and tapering.
AS-related AO Type B3 thoracolumbar fractures: increased frailty and morbidity vs DISH
- AO Type B3 hyperextension fractures are the commonest fracture subtype in ankylosing spinal disorders; medical/surgical complications occurred in 10 of 14 (71.4%) surgically-managed patients.
- Compared with DISH, ankylosing spondylitis patients were far more likely to fracture from a LOW fall (OR 35.0), were more frail (higher modified frailty index), and had more postoperative complications per patient.
- Underscores that AS-related spinal fractures are low-energy, high-morbidity injuries requiring careful, individualised surgical management.
The axial-SpA concept, the HLA-B27/IL-23-17 biology and the MRI-led early diagnosis come from Sieper & Poddubnyy 2017 (DOI); the family classification, gut-joint axis and treatment ladder from Wang & Tsai 2023 (DOI); the treat-to-target/biologic strategy from Van den Bosch & Coates 2018 (DOI); and the ankylosed-spine fracture morbidity from Tan et al. 2019 (DOI). The ASAS classification, inflammatory-back-pain features and enthesitis biology are standard, well-established teaching. (See also our Ankylosing Spondylitis, Psoriatic Arthritis, Reactive Arthritis and Rheumatoid Arthritis topics.)