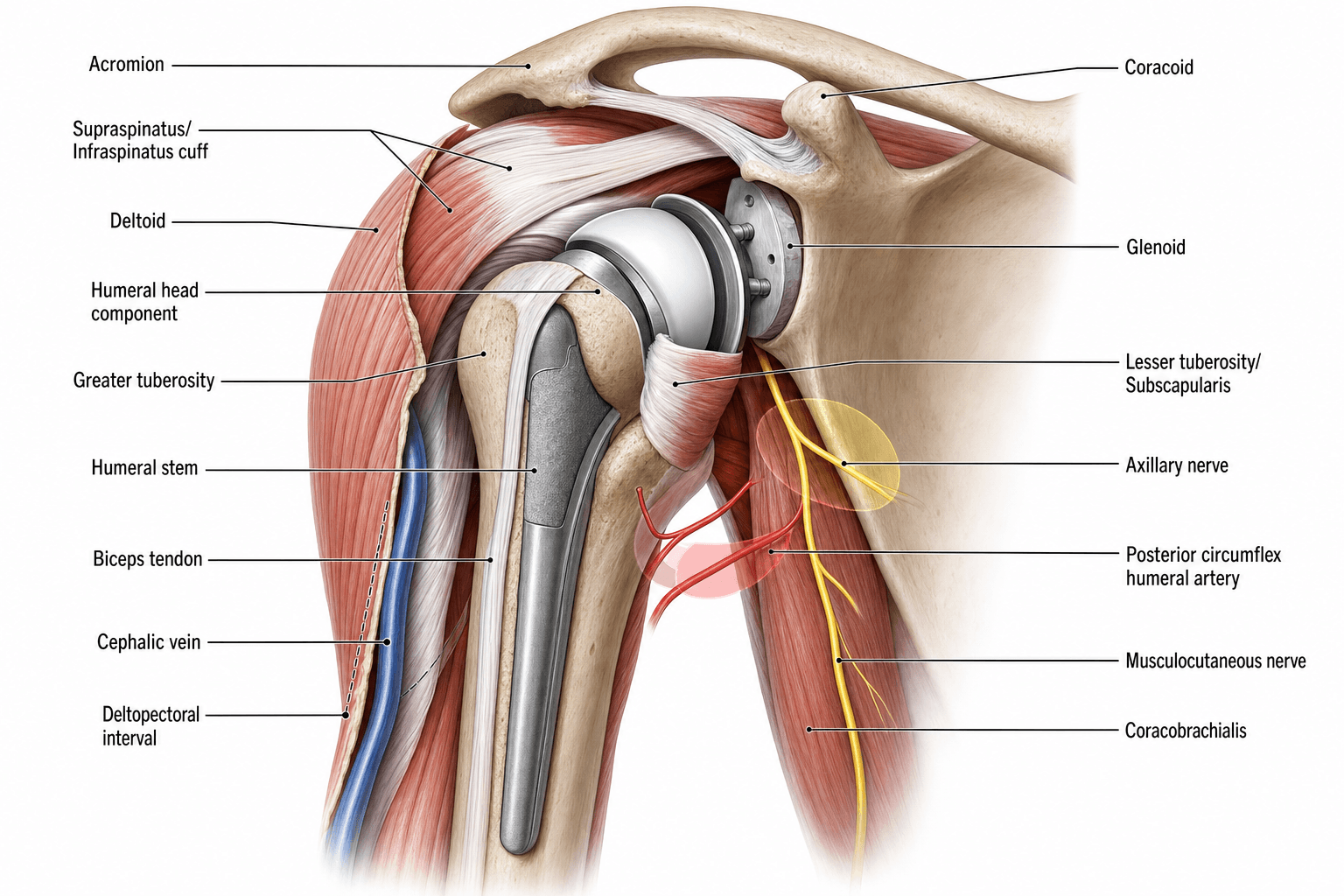
Deltopectoral Approach | Neurovascular Structures at Risk | Rotator Cuff Relationships | Glenoid Exposure
- Axillary nerve lies 5-7 cm inferior to acromion, vulnerable during inferior capsule release
- Musculocutaneous nerve enters coracobrachialis 3-8 cm from coracoid tip
- Cephalic vein runs in deltopectoral groove - ligate laterally or retract medially
- Subscapularis can be released via tenotomy, peel, or lesser tuberosity osteotomy
- Posterior glenoid exposure requires complete anterior capsule release and careful retraction
- “Three critical nerves: axillary (inferior), musculocutaneous (medial), suprascapular (posterior)
- “Deltopectoral interval is internervous and intermuscular - theoretically atraumatic
- “Ascending branch of anterior humeral circumflex artery requires ligation during approach
- “Humeral version averages 30 degrees retroversion relative to transepicondylar axis
Axillary nerve is most at risk during inferior capsule release and glenoid retraction. Lies 5-7 cm from acromion, travels with posterior humeral circumflex artery through quadrangular space. Test deltoid function postoperatively.
Internervous plane between deltoid (axillary nerve) and pectoralis major (medial and lateral pectoral nerves). Cephalic vein marks the interval - can ligate lateral branches or retract medially with pectoralis.
Three release techniques: subscapularis tenotomy (1 cm medial to insertion), subscapularis peel (partial thickness from tuberosity), or lesser tuberosity osteotomy (preserves tendon-bone healing). Each has specific repair requirements.
Normal glenoid retroversion 0-5 degrees. Excessive retroversion (over 10 degrees) requires reaming strategy to restore neutral version or component augmentation. Critical for implant stability and avoiding posterior instability.
- Key Structure
- Cephalic vein
- Clinical Significance
- Marks surgical plane
- Protection Strategy
- Ligate lateral branches or retract medially
- Key Structure
- Musculocutaneous nerve
- Clinical Significance
- Enters coracobrachialis 3-8 cm from coracoid
- Protection Strategy
- Avoid excessive medial retraction, stay above inferior border conjoint tendon
- Key Structure
- Axillary nerve
- Clinical Significance
- Travels through quadrangular space 5-7 cm from acromion
- Protection Strategy
- Release capsule under direct vision, use blunt dissection inferior to subscapularis
- Key Structure
- Suprascapular nerve
- Clinical Significance
- At spinoglenoid notch posterior to glenoid
- Protection Strategy
- Limit posterior retraction, avoid superior-posterior retractor placement
Overview and Clinical Significance
Shoulder arthroplasty demands precise anatomical knowledge due to the concentration of critical neurovascular structures within a limited surgical field. Unlike hip arthroplasty where the sciatic nerve is the primary concern, shoulder replacement requires awareness of four major nerves (axillary, musculocutaneous, suprascapular, and radial) and complex rotator cuff anatomy that must be preserved or repaired. The deltopectoral approach provides excellent exposure but requires careful dissection through multiple tissue planes. Understanding native glenoid and humeral version is essential for component positioning and preventing instability. Mastery of this anatomy reduces neurological complications (reported at 1-4 percent in most series) and improves functional outcomes.
- Safe extensile exposure through internervous plane
- Protection of axillary nerve during capsule release
- Subscapularis preservation or secure repair
- Glenoid visualization without nerve traction injury
- Humeral canal preparation without radial nerve injury
- Restoration of anatomic version relationships
Understanding these principles guides decision-making during complex arthroplasty cases.
- Nerve injuries occur in 1-4 percent of cases
- Axillary nerve most common (0.6-4 percent)
- Musculocutaneous injury from medial retraction (0.3-1 percent)
- Subscapularis failure causes anterior instability (2-10 percent)
- Excessive glenoid retroversion leads to posterior instability
- Version restoration critical for implant longevity
Poor anatomical understanding increases complication risk significantly.
Mnemonics for Shoulder Arthroplasty Anatomy
AMUSNerves at Risk During Shoulder Arthroplasty
Hook:AMUS - All Must be Understood and Safe before arthroplasty proceeds!
SCARFDeltopectoral Approach Layers
Hook:SCARF - Surgical Craft Achieves Reliable Function through proper layered dissection!
TOPSubscapularis Release Options
Hook:TOP - Three Options for Protection and repair of subscapularis!
TILTQuadrangular Space Boundaries
Hook:TILT - The space TILTs posteriorly, containing axillary nerve and posterior humeral circumflex artery!
Bony Anatomy and Landmarks
Scapular Anatomy
- Shape: Pear-shaped, wider inferiorly
- Version: 0-5 degrees retroversion normal
- Inclination: 5 degrees superior tilt
- Depth: Shallow socket, 25-30 mm diameter
- Articular arc: 75 percent of humeral head
- Bone density: Subchondral bone critical for fixation
Glenoid morphology varies with pathology - erosion patterns guide component selection.
- Projection: Anterolateral from superior scapula
- Attachments: Conjoint tendon (short head biceps and coracobrachialis)
- Landmark: Musculocutaneous nerve enters coracobrachialis 3-8 cm from tip
- Ligaments: Coracoacromial, coracoclavicular, coracohumeral
- Importance: Reference for nerve protection, retractor placement
The coracoid is the key medial landmark during deltopectoral approach.
Humeral Anatomy
- Key Feature
- Articular surface
- Measurement
- 130-150 degree neck-shaft angle
- Clinical Significance
- Component position affects ROM and stability
- Key Feature
- Head relative to epicondyles
- Measurement
- 20-40 degrees (average 30)
- Clinical Significance
- Restore native version to prevent instability
- Key Feature
- Supraspinatus, infraspinatus, teres minor insertion
- Measurement
- 5-8 mm superior to articular margin
- Clinical Significance
- Tuberosity malposition causes impingement
- Key Feature
- Subscapularis insertion
- Measurement
- 1 cm medial width
- Clinical Significance
- Osteotomy site preserves tendon-bone healing
- Key Feature
- Long head biceps
- Measurement
- Between tuberosities
- Clinical Significance
- Landmark for version, protect during exposure
Measuring glenoid version is critical for component positioning. Use CT with Friedman or scapular body method. Normal version is 0-5 degrees retroversion. Pathologic retroversion (over 10 degrees) occurs with posterior glenoid wear from cuff tear arthropathy or longstanding posterior instability. Options to correct version: eccentric reaming (limited to 10 degrees correction), augmented components, or bone grafting. Failure to restore version leads to component failure and instability.
Glenoid Inclination — The Coronal-Plane Partner of Version
Version (the axial-plane tilt) is only half of glenoid orientation; inclination is its coronal-plane partner, and the topic relies on it repeatedly (the normal "5 degrees superior tilt", "ream to neutral, avoid superior tilt" in anatomic TSA, and "inferior tilt to reduce notching" in reverse TSA), yet how it is measured is easily forgotten.
- Definition: Inclination is the superior-to-inferior tilt of the glenoid articular surface in the scapular (coronal) plane, whereas version is the anterior-to-posterior tilt in the axial plane. The native glenoid sits in a few degrees of superior tilt.
- Measurement (the beta angle, Maurer): On a true coronal CT reconstruction (or a Grashey AP), draw a line along the floor of the supraspinatus fossa (a reproducible bony reference along the scapular spine) and a second line across the glenoid fossa; the angle between them is the beta angle. A beta angle near 90 degrees is neutral inclination, a smaller angle indicates superior tilt, and a larger angle indicates inferior tilt. The reverse shoulder angle is a related measure used specifically for reverse-arthroplasty planning.
- Why it matters: In anatomic TSA, a glenoid component left in superior inclination promotes superior migration and a rocking-horse loosening pattern with eccentric loading, so the aim is to ream toward neutral and not retain superior tilt. In reverse TSA, baseplate superior tilt is a leading risk for inferior scapular notching and instability, so the baseplate is placed in neutral-to-slight inferior tilt with inferior glenosphere overhang.
Glenoid component planning needs two CT angles, not one: version in the axial plane (Friedman or scapular-body method, normal 0-5 degrees retroversion) and inclination in the coronal plane (the beta angle off the supraspinatus-fossa line, normally slight superior tilt). Superior tilt is poorly tolerated by both implants - ream toward neutral in anatomic TSA, and place the reverse baseplate with neutral-to-inferior tilt and inferior overhang to limit scapular notching.
Rotator Cuff Anatomy
Rotator Cuff Cable System
- Origin: Subscapular fossa of scapula
- Insertion: Lesser tuberosity of humerus
- Function: Internal rotation, anterior stability
- Nerve: Upper and lower subscapular nerves (C5-C6)
- Layers: Upper third superior, middle third horizontal, lower third inferior fibers
- Release: Must be released or osteotomized for humeral exposure
The subscapularis is the most important muscle for anterior stability and internal rotation.
- Origin: Supraspinatus fossa
- Insertion: Superior facet greater tuberosity
- Function: Abduction initiation (first 15 degrees), humeral head depression
- Nerve: Suprascapular nerve (C5-C6)
- Tendon: Courses under coracoacromial arch
- Exposure: Rotator interval between subscapularis and supraspinatus
Rarely released during arthroplasty but critical for reverse shoulder function.
- Infraspinatus: Infraspinatus fossa to middle/superior greater tuberosity
- Teres minor: Lateral scapular border to inferior greater tuberosity
- Function: External rotation, posterior stability
- Nerves: Suprascapular (infraspinatus), axillary (teres minor)
- Quadrangular space: Between teres minor and major (axillary nerve)
Posterior cuff rarely requires release but can be split for posterior approach.
- Boundaries: Superior border subscapularis, anterior edge supraspinatus
- Contents: Coracohumeral ligament, superior glenohumeral ligament, long head biceps
- Floor: Anterior superior capsule
- Importance: Opened first during deltopectoral approach to access joint
- Release: Improves external rotation in stiff shoulders
The rotator interval is the key to safe joint access during anterior approach.
- Method
- Release 1 cm medial to insertion, preserve cuff on bone
- Advantages
- Easier exposure, faster, allows repair to bone
- Disadvantages
- Potential weakness, 5-10 percent failure rate
- Method
- Osteotomize tuberosity with subscapularis attached
- Advantages
- Bone-bone healing, strongest repair, lower failure
- Disadvantages
- Technical demand, tuberosity malunion/nonunion risk
- Method
- Partial thickness peel from tuberosity, leave capsule
- Advantages
- Preserves some insertion, middle ground
- Disadvantages
- Unclear biomechanics, healing variable
Neurovascular Anatomy - Critical Structures
Nerves at Risk
Axillary Nerve - Highest Risk During Arthroplasty
- Origin: Posterior cord of brachial plexus (C5-C6)
- Course: Exits axilla through quadrangular space with posterior humeral circumflex artery
- Quadrangular space boundaries: Teres minor (superior), teres major (inferior), long head triceps (medial), surgical neck humerus (lateral)
- Branches: Anterior (to anterior/middle deltoid), posterior (to posterior deltoid and teres minor), superior lateral cutaneous nerve of arm
- 5-7 cm inferior to acromion along lateral shoulder
- Wraps around surgical neck of humerus posteriorly
- At risk during inferior capsule release and glenoid retraction
- Release inferior capsule under direct vision
- Use blunt dissection inferior to subscapularis
- Avoid inferior retractors placed blindly
- Limit inferior translation during glenoid exposure
- Test deltoid function immediately postoperatively
- Deltoid paralysis (loss of abduction beyond 15 degrees)
- Teres minor weakness (external rotation)
- Sensory loss over lateral shoulder (regimental badge area)
- Usually neurapraxia, recovers in 3-6 months
Understanding axillary nerve anatomy is mandatory for safe shoulder arthroplasty.
Four golden rules to prevent nerve injury during shoulder arthroplasty:
- Axillary nerve: Release inferior capsule under direct vision, avoid blind inferior retractors, stay greater than 5 cm from acromion inferiorly
- Musculocutaneous nerve: Limit medial retraction, stay above inferior subscapularis border, avoid dissection greater than 5 cm from coracoid
- Suprascapular nerve: Minimize posterior retraction duration and force, avoid superior-posterior retractor at glenoid rim, release posterior capsule fully
- Radial nerve: Stay centered in humeral canal, protect anterior cortex, use gentle technique in osteoporotic bone
Testing nerve function immediately postoperatively identifies injury early and guides management.
Vascular Anatomy
- Course
- Medial to surgical field, behind pectoralis minor
- Significance
- Main blood supply to arm, rarely at risk
- Management
- Avoid excessive medial dissection deep to conjoint tendon
- Course
- Ascends in bicipital groove, gives ascending branch
- Significance
- Requires ligation during deltopectoral approach
- Management
- Ligate ascending branch at superior border pectoralis major
- Course
- Travels with axillary nerve through quadrangular space
- Significance
- At risk during inferior capsule release
- Management
- Protected by protecting axillary nerve
- Course
- Runs in deltopectoral groove
- Significance
- Marks surgical interval
- Management
- Ligate lateral branches and retract medially, or ligate vein and retract laterally
Deltopectoral Approach - Step by Step
Surface Anatomy and Incision Planning
- Coracoid process: Palpable anteromedial, 2-3 cm medial and inferior to AC joint
- Acromion: Lateral shoulder prominence
- Clavicle: Superior reference
- Deltopectoral groove: Visible as depression, runs from clavicle toward deltoid insertion
- Axillary fold: Inferior limit of exposure
- Start: Coracoid process
- Direction: Oblique toward lateral edge of acromion, then distally along deltopectoral groove
- Extend: To deltoid insertion if needed (10-15 cm total length for standard arthroplasty)
- Curve: Gentle curve following natural skin lines for better scar
- Incise skin and subcutaneous fat to deltopectoral fascia
- Identify cephalic vein in groove (60-70 percent of cases visible)
- Mobilize vein: Ligate lateral branches and retract medially with pectoralis OR ligate vein and retract laterally with deltoid
The deltopectoral approach is internervous and provides excellent extensile exposure.
Two schools of thought on cephalic vein:
Retract medially with pectoralis (preferred by most):
- Ligate only lateral branches entering deltoid
- Preserves main vein drainage
- Reduces postoperative swelling
- Requires careful dissection
Ligate vein and retract laterally with deltoid:
- Faster, simpler dissection
- Ensures hemostasis
- Collateral drainage adequate
- Risk of increased swelling
Evidence: No significant difference in outcomes between techniques. Choose based on surgical preference and vein quality. If vein damaged during dissection, ligate completely.
Alternative Approaches
- Indication
- Most shoulder arthroplasty cases
- Advantages
- Extensile, internervous, familiar anatomy, lower infection
- Disadvantages
- Subscapularis must be released/repaired
- Indication
- Subscapularis deficiency or reverse arthroplasty
- Advantages
- Preserves subscapularis, good superior exposure
- Disadvantages
- Risk to axillary nerve, limited inferior exposure
- Indication
- Selected reverse arthroplasty cases
- Advantages
- Preserves anterior and posterior cuff
- Disadvantages
- Limited exposure, supraspinatus release required, steep learning curve
- Indication
- Posterior instability repair or revision
- Advantages
- Direct posterior access
- Disadvantages
- Requires prone position, limited anterior exposure
Indications for non-deltopectoral approach:
- Anterosuperior: Irreparable subscapularis deficiency, revision arthroplasty with subscapularis failure, reverse arthroplasty where subscapularis function less critical
- Superior: Primary reverse arthroplasty in hands of experienced surgeon, desire to preserve anterior structures
- Posterior: Posterior bone block for instability, posterior glenoid bone grafting, revision with posterior component removal
The deltopectoral approach remains gold standard for most cases due to extensile nature, internervous plane, familiar anatomy, and ability to extend proximally or distally as needed.
Deltoid-Splitting Approaches and the Axillary Nerve Safe Zone
The table above notes that the anterosuperior (Mackenzie) and superior (Neviaser) approaches "risk the axillary nerve" - but the reason deserves explanation, because it is a different axillary-nerve risk from the one met during the deltopectoral approach. The deltopectoral interval passes between deltoid and pectoralis and spares the deltoid muscle, so its axillary-nerve danger is deep and inferior (the main trunk at the inferior surgical neck during inferior capsule release). The anterosuperior and superior approaches instead split the deltoid fibres, and a deltoid split that is carried too far distally divides the nerve's anterior (deltoid) branch.
- The anatomy: After leaving the quadrangular space, the axillary nerve sends its anterior branch running transversely across the deep (undersurface) of the deltoid to supply the anterior and middle heads. This branch crosses roughly 5-7 cm distal to the lateral acromion. The Yildirim study cited above measured the nerve at a mean of 6.0 cm (range 5.5-6.6 cm) from the anterolateral acromion and proposed about 5.5 cm as a practical limit for the deltoid-splitting approach.
- The rule: Limit any deltoid split to within about 5 cm of the acromion, and place a stay (anchoring) suture at the distal apex of the split so that retraction cannot propagate it inadvertently into the nerve.
- The caveat: Nerve position is individually variable (Yildirim found it predictable in only about 18 percent of patients) and the nerve migrates closer to the acromion with abduction, so the safe zone is a guide, not a guarantee - palpate for the nerve on the deep deltoid surface when a split is used.
Name the axillary-nerve risk to the approach: in the deltopectoral approach the nerve is endangered deep and inferior (the main trunk at the inferior capsule/surgical neck, ~5-7 cm below the acromion); in deltoid-splitting approaches (anterosuperior, superior) it is the transverse anterior branch crossing the undersurface of the deltoid ~5 cm distal to the acromion. Keep a deltoid split within ~5 cm of the acromion and stay-suture its distal apex.
Subscapularis Repair
Subscapularis Tenotomy Repair
- Mobilize subscapularis tendon medially to ensure tendon reaches lesser tuberosity without tension
- Prepare bony bed on lesser tuberosity (remove soft tissue, create bleeding bone)
- Place trial components and reduce joint to assess tension
-
Suture anchors (most common):
- Place 3-4 anchors in lesser tuberosity footprint
- Use knotless or traditional anchors
- Pass sutures through tendon using modified Mason-Allen or simple sutures
- Secure with arm in neutral rotation (not external rotation - creates excessive tension)
-
Transosseous tunnels (alternative):
- Drill tunnels from lesser tuberosity to lateral cortex
- Pass nonabsorbable sutures through tendon and tunnels
- Tie over bone bridge laterally
- Consider pectoralis major transfer if poor tissue quality
- Use dermal allograft or synthetic patch for large defects (uncommon)
- Belly press test: Should have resistance at 20-30 degrees external rotation
- Lag sign: Should be negative with intact repair
Tenotomy repair strength depends on bone quality and suture anchor fixation.
Anatomy
Key Anatomical Considerations for Shoulder Arthroplasty
Osseous Anatomy
- Humeral head: 40-50mm diameter, 130-145° neck-shaft angle, 20-40° retroversion
- Glenoid: Pear-shaped, 35mm height, 25mm width, 5-10° retroversion, 5° superior tilt
- Glenoid vault: Central bone stock critical for baseplate fixation (depth 15-25mm)
- Coracoid process: Reference landmark, 25mm medial to glenoid rim
Rotator Cuff Footprints
- Supraspinatus: Superior facet of greater tuberosity
- Infraspinatus: Middle facet of greater tuberosity
- Teres minor: Inferior facet of greater tuberosity
- Subscapularis: Lesser tuberosity (critical for TSA stability)
Neurovascular Structures at Risk
- Axillary nerve: 5-7cm inferior to acromion, crosses anterior to subscapularis
- Musculocutaneous nerve: Enters coracobrachialis 5-8cm distal to coracoid
- Suprascapular nerve: At spinoglenoid notch, risk with posterior glenoid exposure
Clinical Correlations - Anatomical Injury Complications
- Incidence
- 0.6-4%
- Cause
- Inferior capsule release, retraction, traction
- Prevention
- Careful inferior release, avoid blind retractors, limit traction
- Management
- Observation 3-6 months (most recover), EMG at 6 weeks, consider exploration if no recovery
- Incidence
- 0.3-1%
- Cause
- Excessive medial retraction of conjoint tendon
- Prevention
- Limit medial retraction, stay above inferior subscapularis
- Management
- Usually recovers spontaneously, splint elbow in flexion initially
- Incidence
- Less than 1%
- Cause
- Posterior glenoid retraction, superior retractor
- Prevention
- Limit posterior retraction force and duration, avoid superior-posterior retractors
- Management
- Observation, consider decompression at notch if no recovery 6-12 months
- Incidence
- 2-10%
- Cause
- Poor tissue quality, inadequate repair, excessive tension, noncompliance
- Prevention
- Secure repair technique, protect postoperatively, patient education
- Management
- Revision repair if symptomatic instability, consider pectoralis major transfer
- Incidence
- Less than 0.1%
- Cause
- Excessive medial dissection, fracture, cerclage wires
- Prevention
- Stay lateral, careful medial dissection, avoid cerclage
- Management
- Immediate vascular surgery consultation, repair or graft
Test nerve function in recovery room before regional anesthesia wears off:
- Axillary nerve: Deltoid contraction (palpate muscle with abduction attempt), sensation over lateral shoulder
- Musculocutaneous nerve: Biceps contraction with elbow flexion
- Radial nerve: Wrist/finger extension
- Suprascapular nerve: Cannot test acutely (motor only)
Document findings and compare to preoperative examination. If new deficit detected, determine if complete or partial. Most neurapraxias recover with observation, but early recognition guides patient counseling and follow-up planning.
Classification
Glenoid Morphology Classifications
Walch Classification (Glenoid Wear Patterns)
- Description
- Minor central erosion, concentric humeral head
- Implications
- Standard glenoid component, no augment needed
- Description
- Major central erosion, concentric humeral head
- Implications
- May need bone graft for central defect
- Description
- Posterior subluxation, no erosion
- Implications
- Asymmetric reaming, consider RSA
- Description
- Posterior subluxation + biconcave posterior erosion
- Implications
- Posterior augment or asymmetric reaming, RSA preferred
- Description
- Monoconcave posterior erosion (retroversion greater than 15°)
- Implications
- Posterior augment mandatory, bone graft, or RSA
- Description
- Dysplastic glenoid (retroversion greater than 25°)
- Implications
- RSA with augment or custom implant
- Description
- Anterior subluxation/erosion
- Implications
- Rare, anterior augment or RSA
Investigations
Preoperative Imaging for Anatomical Assessment
Plain Radiographs (Essential)
- True AP (Grashey view): Joint space, humeral head position, glenoid wear
- Axillary lateral: Glenoid version, posterior wear, subluxation
- Scapular Y: Acromion morphology, os acromiale
- Full-length humerus: For stem sizing in revision
CT Scan with 3D Reconstruction
- Glenoid version and inclination measurement
- Walch classification determination
- Bone stock assessment for baseplate fixation
- Glenoid vault depth and screw trajectory planning
- 3D planning software for templating
MRI
- Rotator cuff integrity (determines TSA vs RSA)
- Fatty infiltration (Goutallier classification)
- Muscle atrophy assessment
Management
Management Based on Anatomical Findings
Prosthesis Selection Based on Anatomy
- Recommended Approach
- Anatomic TSA
- Rationale
- Restores normal biomechanics, best ROM
- Recommended Approach
- Reverse TSA (RSA)
- Rationale
- Deltoid-powered elevation, bypasses cuff
- Recommended Approach
- RSA preferred over TSA
- Rationale
- Lower glenoid loosening with baseplate vs pegged glenoid
- Recommended Approach
- RSA preferred
- Rationale
- No tuberosity healing required, reliable outcomes
Glenoid Version Correction
- Retroversion less than 15°: Asymmetric reaming alone
- Retroversion 15-25°: Posterior augmented glenoid or bone graft
- Retroversion greater than 25°: Custom implant or RSA with augment
Surgical Technique
Anatomical Landmarks in Surgical Technique
Deltopectoral Approach - Key Landmarks
- Coracoid process: Central reference point
- Cephalic vein: Lateral retraction (protects vein, maintains venous drainage)
- Conjoint tendon: Medial border of exposure
- Subscapularis: Must be addressed for exposure
Subscapularis Management Options
- Lesser tuberosity osteotomy: Best healing rates, bone-to-bone healing
- Subscapularis peel: Tendon from bone, higher failure rate
- Subscapularis tenotomy: Tendon cut, poorest healing (avoid in TSA)
Glenoid Exposure Sequence
- Position arm in extension, external rotation, adduction
- Place Fukuda retractor posteriorly
- Release anterior capsule off glenoid rim
- Release inferior capsule (protect axillary nerve)
- Place blunt retractors inferiorly and superiorly


Complications
Anatomically-Related Complications
Neurovascular Injuries
- Axillary nerve: Most common (0.6-4%), from inferior capsule release or retraction
- Musculocutaneous nerve: Excessive medial retraction on conjoint tendon
- Suprascapular nerve: Posterior glenoid retraction or long superior screws
Osseous Complications
- Intraoperative fracture: Greater tuberosity (3-5%), shaft (1-2%)
- Glenoid fracture: From aggressive reaming or malpositioning
- Periprosthetic fracture: Postoperative trauma or stress risers
Soft Tissue Complications
- Subscapularis failure: 2-10% for TSA, leads to instability
- Rotator cuff tear progression: 5-10% by 10 years
- Deltoid detachment: Rare but catastrophic for RSA

Postoperative Care
Postoperative Protocols
Immobilization
- Sling immobilization: 2-4 weeks (TSA), 4-6 weeks (RSA)
- Position: Internal rotation, slight abduction on pillow
- Remove for elbow, wrist, hand exercises and hygiene
Rehabilitation Phases
- Timeframe
- 0-4 weeks
- Goals
- Protect repair, control inflammation
- Exercises
- Pendulums, elbow/wrist ROM, isometrics
- Timeframe
- 4-8 weeks
- Goals
- Restore passive ROM
- Exercises
- Passive forward flexion, external rotation
- Timeframe
- 8-12 weeks
- Goals
- Active ROM, light function
- Exercises
- Active assisted to active ROM
- Timeframe
- 12-16 weeks
- Goals
- Progressive strength
- Exercises
- Rotator cuff, deltoid, scapular
Outcomes
Outcomes Related to Anatomical Factors
Functional Outcomes by Prosthesis Type
- TSA
- 140-160°
- RSA
- 120-140°
- TSA
- 40-60°
- RSA
- 20-40°
- TSA
- L1-T12
- RSA
- Sacrum-L3
- TSA
- 85-95%
- RSA
- 85-90%
- TSA
- 90-95%
- RSA
- 85-90%
Factors Affecting Outcomes
- Glenoid morphology: B2/B3 glenoids have higher loosening rates
- Rotator cuff integrity: Intact cuff improves TSA outcomes
- Bone quality: Osteoporosis increases fracture and loosening risk
Guidelines, Registries & Global Practice
Shoulder arthroplasty is one of the fastest-growing joint replacements worldwide, driven mainly by reverse TSA. Wherever it is performed, the deltopectoral approach and its neurovascular relationships are identical, so the surgical anatomy is genuinely a global, exam-universal core. National registries and society guidelines converge on the same anatomical safety principles, differing mainly in implant case-mix and perioperative protocols.
Global Epidemiology
According to PubMed, US nationwide data on more than 508,000 primary procedures (Best et al., J Shoulder Elbow Surg 2021, DOI) showed reverse TSA incidence rising from 7.3 to 19.3 per 100,000 persons and anatomic TSA from 9.5 to 12.5 per 100,000 between 2012 and 2017, while hemiarthroplasty fell from 3.7 to 1.5 per 100,000. The largest growth was reverse TSA in men and in patients aged 50-64 years. This rising, increasingly reverse-dominant case-mix means more patients are exposed to the deltopectoral neurovascular risks discussed above, even though reverse TSA may use the same or an anterosuperior approach.
Guidelines Side by Side
- Relevant recommendation
- Glenohumeral OA CPG and the 2009/2010 VTE consensus underpin routine chemoprophylaxis after TSA, associated with falling VTE rates over the following decade
- Evidence basis
- Clinical practice guideline / consensus; registry-linked observational support
- Relevant recommendation
- Joint-replacement standards emphasise consent for nerve injury, infection and revision, surgical-site infection bundles and PROMs capture; no UK guideline mandates a specific shoulder approach
- Evidence basis
- National standards / BOAST principles
- Relevant recommendation
- Teaching materials standardise the deltopectoral internervous interval, axillary-nerve protection during inferior release and structured subscapularis repair
- Evidence basis
- Expert consensus / educational standard
- Relevant recommendation
- Track implant survival, revision rate and the anatomic-versus-reverse case-mix; nerve injury is generally not a discrete registry endpoint
- Evidence basis
- Prospective registry / Level II-III
Registry Evidence and Practice Variation
Joint registries (the National Joint Registry for England, Wales, Northern Ireland and the Isle of Man; the American Joint Replacement Registry; the Australian AOANJRR; the New Zealand Joint Registry; and the Nordic registries) consistently document the global shift from anatomic TSA and hemiarthroplasty toward reverse TSA, and they benchmark implant survival and revision. Neurological injury is rarely a discrete registry field, so its incidence is best taken from clinical series rather than registries. Practice variation is mostly in case-mix and perioperative care rather than in the surgical anatomy: high-resource systems increasingly favour reverse TSA with CT-based planning, whereas in limited-resource settings hemiarthroplasty and standard instrumentation remain more common, and a sound understanding of the deltopectoral approach and axillary-nerve safe zone matters more where navigation and patient-specific guides are unavailable.
Across guidelines and health systems, the same anatomy-driven safety principles recur:
- Surgical-site infection bundle: weight-based intravenous antibiotic prophylaxis within 60 minutes of incision (a first-generation cephalosporin, with a glycopeptide alternative for severe beta-lactam allergy), skin antisepsis and normothermia. Follow the local/national antimicrobial formulary for exact agent and dose.
- VTE prophylaxis for joint-replacement patients, individualised to bleeding and thrombotic risk (AAOS consensus, DOI).
- Documented pre- and immediate post-operative neurological examination to detect axillary, musculocutaneous and radial nerve deficits early, given that injury is rarely captured by registries.
- Shared decision-making and PROMs capture for quality improvement and benchmarking against registry data.
MCQ Practice Points
Q: What is the average distance from the tip of the coracoid process to the point where the musculocutaneous nerve enters the coracobrachialis muscle?
A: In the classic cadaveric study by Flatow et al. (Clin Orthop Relat Res, 1989), the main musculocutaneous nerve trunk entered coracobrachialis at a mean of 56 mm (range 31-82 mm) below the coracoid, and small proximal twigs entered as close as 17 mm. Importantly, the often-quoted "5-8 cm safe zone" is unreliable, because 29 percent of main trunks entered proximal to 5 cm (74 percent when proximal twigs are counted). This anatomic relationship is critical during the deltopectoral approach: excessive medial retraction of the conjoint tendon risks musculocutaneous nerve injury by traction or direct trauma. Protection strategies include limiting medial retraction and staying superior to the inferior border of the subscapularis and conjoint tendon during deep dissection.
Q: What are the boundaries of the quadrangular space, and what structures pass through it?
A: Boundaries: Superior = teres minor, Inferior = teres major, Medial = long head of triceps, Lateral = surgical neck of humerus. Structures: Axillary nerve and posterior humeral circumflex artery. The quadrangular space is clinically important as the axillary nerve is vulnerable during inferior capsule release and humeral retraction for glenoid exposure. The nerve lies approximately 5-7 cm inferior to the acromion. Injury causes deltoid paralysis (loss of active abduction beyond 15 degrees), teres minor weakness, and sensory loss over the lateral shoulder (regimental badge area).
Q: What is the internervous plane for the deltopectoral approach to the shoulder?
A: Deltoid (innervated by axillary nerve from C5-C6) and pectoralis major (innervated by medial and lateral pectoral nerves from C5-T1). This is a true internervous and intermuscular plane, making it theoretically atraumatic to muscles. The interval is marked by the cephalic vein running in the deltopectoral groove. The deep layer requires release of the clavipectoral fascia and ligation of the ascending branch of the anterior humeral circumflex artery. The internervous nature is advantageous but does NOT protect deeper structures like the axillary nerve, musculocutaneous nerve, and suprascapular nerve which remain at risk during capsule release and glenoid retraction.
Q: Compare the biomechanical strength and clinical outcomes of subscapularis tenotomy versus lesser tuberosity osteotomy repair after shoulder arthroplasty.
A: Lesser tuberosity osteotomy provides stronger healing with bone-to-bone healing interface and lower failure rates (2-3 percent) compared to subscapularis tenotomy (5-10 percent failure rate). Osteotomy can be repaired with cortical screws (biomechanically strongest), suture anchors, or heavy sutures. Tenotomy repair uses suture anchors securing tendon to bone at the lesser tuberosity footprint. However, osteotomy carries risks of tuberosity malposition (causing impingement or weakness), nonunion (2-5 percent), and increased surgical complexity. In clinical practice, both techniques can achieve good outcomes with proper technique and postoperative protection. The choice depends on tissue quality, patient factors (younger patients may benefit from osteotomy), revision versus primary surgery, and surgeon experience and preference.
Q: What is normal glenoid version, how is it measured, and what are the implications of pathologic retroversion for shoulder arthroplasty component positioning?
A: Normal glenoid version is 0-5 degrees retroversion (slight posterior tilt of glenoid face). It is measured on axial CT using either the Friedman method (line perpendicular to glenoid face compared to scapular body line) or the scapular body method. Pathologic retroversion (over 10 degrees) occurs with posterior glenoid wear from rotator cuff tear arthropathy, chronic posterior instability, or osteoarthritis. Excessive retroversion leads to posterior humeral subluxation, glenoid component edge loading, loosening, and instability. Correction strategies include: eccentric reaming (can correct up to 10 degrees but limited by bone stock), augmented glenoid components (metal or polyethylene wedge on posterior), posterior bone grafting (for severe defects), or accepting retroversion and using posterior augmented component. Failure to address pathologic version results in high rates of posterior instability and glenoid component failure. Preoperative CT planning is mandatory to identify and plan for version abnormalities.
Q: A patient develops weakness in elbow flexion and sensory loss over the lateral forearm after shoulder arthroplasty. What nerve is likely injured, what is the mechanism, and how should this be managed?
A: This presentation suggests musculocutaneous nerve injury. The musculocutaneous nerve (C5-C7 from lateral cord) innervates coracobrachialis, biceps brachii, and brachialis (elbow flexion and forearm supination) and provides sensory innervation as the lateral antebrachial cutaneous nerve (lateral forearm sensation). During shoulder arthroplasty via deltopectoral approach, the nerve is at risk from excessive medial retraction of the conjoint tendon (short head biceps and coracobrachialis). The nerve enters the coracobrachialis a mean of 56 mm (range 31-82 mm) from the coracoid tip, with proximal twigs entering closer, so no fixed safe distance can be relied upon and aggressive medial retraction causes traction injury or direct trauma. Management: Most musculocutaneous nerve injuries are neurapraxias that recover spontaneously in 3-6 months. Initial management includes documentation of deficit, EMG/NCS at 6 weeks for baseline and prognosis, elbow splinting in flexion initially to reduce tension, and range of motion exercises to prevent stiffness. Patient counseling about expected recovery timeline is important. If no recovery by 6 months, consider nerve exploration, although outcomes of late exploration are poor. Prevention is critical: limit medial retraction, stay superior to the inferior border of subscapularis, and avoid dissection greater than 5 cm medial to coracoid tip.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“You are performing shoulder arthroplasty via deltopectoral approach. Describe the key anatomical landmarks, the surgical intervals you will develop, and the nerves at risk during your dissection.”
“Walk me through your subscapularis management during shoulder arthroplasty. What are the different release techniques, how do you decide which to use, and what are the repair principles for each?”
“During shoulder arthroplasty glenoid exposure, you are concerned you may have injured the axillary nerve. Describe the anatomy of the axillary nerve, how you would assess for injury intraoperatively and postoperatively, and your management if injury is confirmed.”
Key Anatomical Relationships
- Axillary nerve: 5-7 cm inferior to acromion, quadrangular space, at risk during inferior capsule release
- Musculocutaneous nerve: Enters coracobrachialis a mean of 56 mm (range 31-82 mm) from coracoid, twigs closer; no fixed safe zone, at risk with medial retraction
- Suprascapular nerve: Spinoglenoid notch posteriorly, at risk during posterior glenoid retraction
- Radial nerve: Spiral groove at mid-humerus (20 cm from acromion), at risk during humeral canal preparation
- Cephalic vein: Marks deltopectoral interval, ligate laterally or retract medially
- Ascending branch anterior humeral circumflex: Requires ligation at superior border pectoralis major
Deltopectoral Approach Steps
- Internervous plane: Deltoid (axillary nerve) and pectoralis major (pectoral nerves)
- Incision: Coracoid to lateral acromion, along deltopectoral groove distally
- Identify cephalic vein (marks interval), ligate lateral branches and retract medially
- Release clavipectoral fascia, ligate ascending branch anterior humeral circumflex
- Open rotator interval (between supraspinatus and subscapularis)
- Release subscapularis: Tenotomy (1 cm medial to insertion) OR lesser tuberosity osteotomy
Nerve Protection Strategies
- Axillary: Release inferior capsule under direct vision, avoid blind inferior retractors, limit inferior humeral translation
- Musculocutaneous: Limit medial retraction, stay above inferior border subscapularis/conjoint tendon, avoid dissection greater than 5 cm from coracoid
- Suprascapular: Minimize posterior retraction force and duration, avoid superior-posterior retractor placement
- Radial: Stay centered in humeral canal during reaming/broaching, protect anterior cortex, gentle technique in osteoporotic bone
Subscapularis Management
- Tenotomy: Release 1-2 cm medial to insertion, repair with 3-4 suture anchors, 5-10 percent failure rate
- Osteotomy: 1 cm bone wafer with subscapularis attached, repair with screws or anchors, 2-3 percent failure, stronger healing
- Repair: Arm in neutral rotation (not external rotation), secure fixation, avoid excessive tension
- Postoperative: Sling 4-6 weeks, no external rotation, gradual ROM progression, belly press test at 12 weeks
Glenoid and Humeral Anatomy
- Normal glenoid version: 0-5 degrees retroversion, measured on CT, pathologic if over 10 degrees
- Humeral retroversion: 20-40 degrees (average 30 degrees) relative to transepicondylar axis
- Glenoid: Pear-shaped, 25-30 mm diameter, shallow socket (25-30 percent of sphere)
- Quadrangular space: Teres minor (superior), teres major (inferior), triceps long head (medial), surgical neck (lateral)
- Contains: Axillary nerve and posterior humeral circumflex artery
Key Evidence and Complications
- Overall neurologic complication rate: 1-4 percent in shoulder arthroplasty
- Axillary nerve most common (0.6-4 percent), most are neurapraxias recovering in 3-6 months
- Subscapularis failure: 2-10 percent, causes anterior instability and internal rotation weakness
- Immediate postoperative nerve exam before regional anesthesia wears off - document findings
- EMG/NCS at 6 weeks if nerve injury suspected, observation for 3-6 months (most recover)
- Registries (NJR, AJRR, AOANJRR, NZJR, Nordic) track revision and the rising reverse-TSA case-mix; nerve injury is not a discrete registry endpoint, so use clinical series for its incidence
Evidence Base and Key Studies
Neurologic Complications After Total Shoulder Arthroplasty
- 417 total shoulder arthroplasties in 368 patients (1975-1989); 18 shoulders (17 patients) developed a postoperative neurologic deficit
- Most deficits localised to the brachial plexus, with the upper and middle trunks most commonly affected (13 shoulders)
- Presumed mechanism in most cases was intraoperative traction on the plexus rather than direct nerve laceration
- The long deltopectoral approach (deltoid left attached to clavicle/acromion) and methotrexate use were significant risk factors
- Prognosis for recovery was generally good (good in 11 shoulders, fair in 5 at one year), and injury did not compromise long-term arthroplasty outcome
Loss of Subscapularis Function After Total Shoulder Replacement
- Retrospective review of 41 patients after total shoulder replacement with the subscapularis repaired anatomically (9) or through bone tunnels (32)
- Despite meticulous repair, the lift-off test was abnormal in 25 of 37 shoulders (67.5 percent) and the belly-press test abnormal in 24 of 36 (66.6 percent)
- Of patients with an abnormal lift-off finding, 92 percent reported reduced subscapularis function
- Suboptimal return of internal rotation and subscapularis function was a frequent, under-recognised problem
- Subscapularis dysfunction limited activities of daily living such as tucking in a shirt
An Anatomic Study of the Musculocutaneous Nerve and Its Relationship to the Coracoid Process
- The distance from the coracoid to where the main musculocutaneous nerve trunk entered coracobrachialis ranged from 31 to 82 mm (mean 56 mm)
- Small nerve twigs entered the muscle as close as 17 mm below the coracoid (mean 31 mm)
- The frequently quoted 5-8 cm safe zone is unreliable: 29 percent of main trunks entered proximal to 5 cm below the coracoid (74 percent if proximal twigs are counted)
- Excessive medial retraction or coracoid mobilisation is the principal mechanism of injury
- If coracoid mobilisation is needed the nerve and its twigs should be identified and protected directly