Anterior vs Posterior | Locked Dislocations | Reverse Hill-Sachs | Tuberosity Integration
CLASSIFICATION
Critical Must-Knows
- Posterior Dislocation Trap: Often missed on AP X-ray. Look for 'Lightbulb Sign', 'Rim Sign', and 'Trough Line'.
- Reverse Hill-Sachs: Impression fracture of anteromedial head. Size determines stability (less than 20% stable, greater than 40% unstable).
- Reduction Risk: Reducing a fracture-dislocation can cause iatrogenic anatomical neck fracture (completing the fracture). Do it gently or in OT.
- Terrible Triad of Shoulder: Anterior Dislocation + Rotator Cuff Tear + Brachial Plexus Injury (check axillary nerve!).
Clinical Pearls
- "Anterior Fx-Dislocation in Elderly = High risk of cuff tear leads to RTSA often preferred
- "Axillary view (or Velpeau) is non-negotiable for diagnosis
- "Seizure / Electric Shock = Posterior Dislocation until proven otherwise
- "First time dislocation greater than 40y has 30% risk of cuff tear. Greater than 60y has greater than 80% risk.
Clinical Imaging
Imaging Gallery


Critical Exam Points
The Missed Posterior
Visual Trap: On AP X-ray, the head looks symmetric (Lightbulb). The overlap is misleading. ALWAYS get an orthogonal view (Axillary/Scapular Y).
Iatrogenic Injury
Reduction Danger: Forceful reduction of a proximal humerus fracture-dislocation can displace a non-displaced surgical neck fracture or shear the head, causing devastating devascularization.
Neurovascular
Axillary Nerve: Rate of injury is high. Document status pre- and post-reduction.
Bone Defect
Impression Fractures: The size of the head defect dictates treatment. A large Reverse Hill-Sachs (greater than 40%) will re-dislocate if not addressed (Transfer/Arthroplasty).
At a Glance - Management Decision
| Pattern | Defect Size | Time from Injury | Treatment |
|---|---|---|---|
| Posterior Locked | Small (less than 20%) | Acute (less than 3 weeks) | Closed Reduction + Immobilization (ER) |
| Posterior Locked | Medium (20-45%) | Acute | Modified McLaughlin (Lesser Tuberosity Transfer) |
| Posterior Locked | Large (greater than 45%) | Chronic (greater than 3 weeks) | Hemi (Young) or RTSA (Elderly) |
| Anterior Fx-Disloc | Comminuted | Elderly | Reverse Total Shoulder Arthroplasty |
LIGHTPosterior Dislocation Signs
| L | Lightbulb sign Head looks round due to internal rotation |
| I | Internal Rotation fixed Patient cannot externally rotate |
| G | Glenoid rim vacant Vacant glenoid sign (Rim sign) |
| H | History Seizure, Shock, Alcohol |
| T | Through Line Vertical line of trough (Reverse Hill Sachs) |
| L | Lightbulb sign Head looks round due to internal rotation | H | History Seizure, Shock, Alcohol |
| I | Internal Rotation fixed Patient cannot externally rotate | T | Through Line Vertical line of trough (Reverse Hill Sachs) |
| G | Glenoid rim vacant Vacant glenoid sign (Rim sign) |
Hook:Shed some LIGHT on the diagnosis with an Axillary view.
S-M-LImpression Fracture Sizing
| S | Small (less than 20%) Stable. Reduction only. |
| M | Medium (20-45%) Unstable. Transfer (McLaughlin) or Graft. |
| L | Large (greater than 45%) Arthroplasty. |
| S | Small (less than 20%) Stable. Reduction only. |
| M | Medium (20-45%) Unstable. Transfer (McLaughlin) or Graft. |
| L | Large (greater than 45%) Arthroplasty. |
Hook:Small, Medium, or Large defect determines the surgery.
RAPIDComplications
| R | Redislocation If defect not addressed |
| A | AVN High risk in anatomical neck fx |
| P | Palsy Axillary nerve injury |
| I | Infection Surgical risk |
| D | Devascularization Iatrogenic during reduction |
| R | Redislocation If defect not addressed | I | Infection Surgical risk |
| A | AVN High risk in anatomical neck fx | D | Devascularization Iatrogenic during reduction |
| P | Palsy Axillary nerve injury |
Hook:Action must be RAPID but careful to avoid complications.
Overview
Fracture-dislocations of the shoulder represent a severe subset of proximal humerus injuries. The combination of instability and fracture significantly complicates management. The priority is to achieve stable reduction while preserving blood supply to the humeral head.
Epidemiology
Incidence:
- Anterior: Common in trauma.
- Posterior: 2-4% of shoulder dislocations (rare), but 50% are missed initially.
- Bimodal: Young (High energy) vs Elderly (Low energy/Osteoporotic).
Pathology
Mechanism:
- Anterior: Abduction/External Rotation force. Greater tuberosity shears off, allowing head to escape anteriorly.
- Posterior: Adduction/Internal Rotation force (Seizure/Shock). Head impacts posterior glenoid, causing anterior impression (Reverse Hill-Sachs).
Anatomy and Pathophysiology
Structural Considerations
Anterior Fracture-Dislocation:
- The GT is often fractured/avulsed.
- If the GT fragment remains posterior, it can block reduction.
- Reducing the head often reduces the GT (via Periosteal sleeve/Rotator Cuff).
- If GT is widely displaced, cuff function is compromised.
Healed GT in malposition = Impingement and loss of abduction.
Classification
Fracture Patterns
Anterior Fracture-Dislocation:
- 2-Part: Head Dislocated + GT Fracture (Head/Shaft intact).
- 3-Part: Head Dislocated + GT Fracture + Surgical Neck Fracture.
- 4-Part: Head Dislocated + GT + LT + Surgical Neck (High AVN risk, Head matches glenoid, Tuberosities separated).
Often termed "Valgus Impacted" vs "Displaced".
Clinical Assessment
Diagnosis
History
Clues:
- Seizure: Unwitnessed fall, tongue biting, urinary incontinence.
- Electric Shock: Industrial accident.
- Electroconvulsive Therapy (ECT).
- Alcohol intoxication: Fall + unconscious.
High index of suspicion for Posterior Dislocation in these patients.
Examination
Anterior:
- Arm held in slight abduction/ER.
- Prominent acromion (squared off).
- Palpable head anteriorly.
Posterior:
- Arm LOCKED in internal rotation and adduction.
- Cannot externally rotate (Pathognomonic).
- Posterior fullness (head).
- Anterior flattening (coracoid prominent).
Neurovascular check (Axillary N, Radial pulse) is mandatory.
Investigations
Imaging Protocols
Trauma Series:
- AP: Lightbulb sign (Posterior), Overlap sign.
- Scapular Y: Head position relative to Y center.
- Axillary: GOLD STANDARD. Defines direction and tuberosity status.
- Velpeau View: If patient cannot abduct for axillary.
Never accept just an AP.
Differential Diagnosis
Distinguishing the Stiff or Deformed Post-Traumatic Shoulder
| Diagnosis | Key Clinical Clue | Best Discriminating Test |
|---|---|---|
| Locked posterior fracture-dislocation | Fixed internal rotation, cannot externally rotate | Axillary view / CT (reverse Hill-Sachs, head behind glenoid) |
| Anterior fracture-dislocation | Arm in slight abduction/ER, squared-off acromion | Axillary view (head anteroinferior, greater tuberosity status) |
| Isolated proximal humeral fracture (no dislocation) | Head congruent with glenoid on orthogonal view | Scapular Y / axillary view confirms reduction |
| Adhesive capsulitis / frozen shoulder | Global passive restriction, no acute trauma, normal bony alignment | Normal orthogonal radiographs |
| Posterior dislocation without fracture | Fixed IR but no impression defect or neck fracture | CT shows congruent head, no reverse Hill-Sachs |
| Luxatio erecta (inferior dislocation) | Arm fixed in abduction/elevation, high neurovascular risk | AP radiograph (head inferior to glenoid) |
Controversies and Areas of Uncertainty
Defect-size thresholds
Cut-offs for transfer versus arthroplasty (often quoted as 20-25% and 40-50%) are derived from small series, not prospective trials. Engagement in functional rotation, bone quality and chronicity matter as much as the percentage.
Fix versus replace in the elderly
PROFHER showed no benefit of surgery over nonoperative care for displaced surgical-neck fractures, but it largely excluded true fracture-dislocations and head-splits, so it cannot be extrapolated to lock the door on surgery here.
Hemiarthroplasty vs reverse
RCT and registry data favour reverse arthroplasty in older patients with unreconstructable heads because outcomes are less dependent on tuberosity healing, but reverse implants carry notching, long-term loosening and revision concerns in younger patients.
Biological reconstruction in the young
Osteochondral allograft, autograft, disimpaction-grafting and rotational osteotomy aim to preserve the native joint in large defects, but comparative evidence is limited to case series with no consensus on the optimal technique.
Management Algorithm
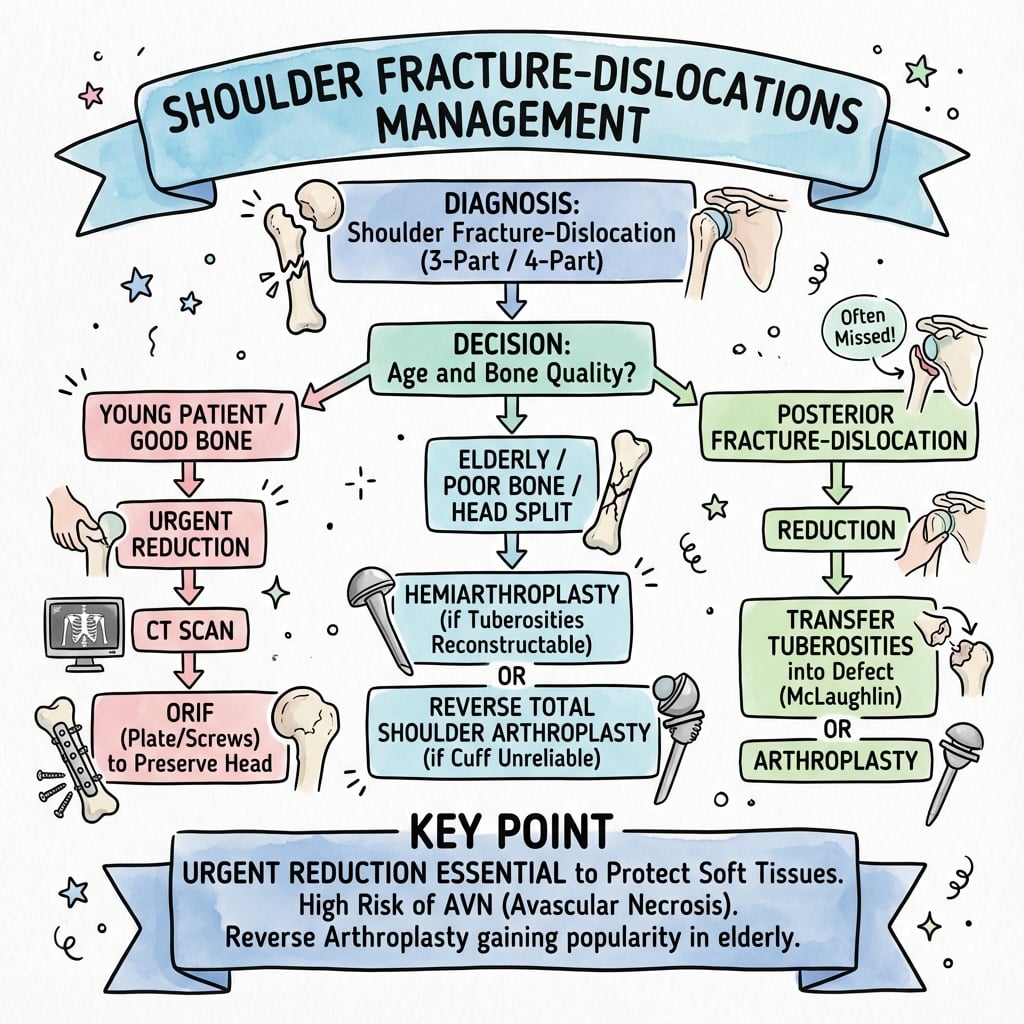
Decision Flowchart
Reduction:
- Conscious sedation or GA.
- Gentle traction-countertraction.
- Avoid Kocher (leverage) maneuver (Risks spiral fracture).
Post-Reduction:
- Check stability.
- GT Fracture: If reduces to less than 5mm displacement then Conservative (Sling).
- GT Displaced: Greater than 5mm then ORIF (Screw/Suture).
- Unstable: Surgical stabilization.
Always re-Xray (and often CT) post-reduction to confirm concentric reduction and tuberosity position.
Surgical Technique
Operative Strategies
Indication: Posterior dislocation with medium defect (20-45%).
- Concept: Fill the defect with the Lesser Tuberosity (and Subscapularis).
- Approach: Deltopectoral Approach.
- Steps:
- Identify the Lesser Tuberosity (LT) which is often intact.
- Perform an osteotomy of the LT with the Subscapularis tendon attached.
- Reduce the humeral head (disimpact from glenoid).
- Internally rotate slightly to expose the defect.
- Transfer the LT graft into the anteromedial defect.
- Fix with 2x cannulated screws or suture anchors.
This converts a bone loss problem into a tendon transfer solution and prevents the posterior rim from engaging the defect.
Complications
Potential Pitfalls
Missed Diagnosis
Chronic Locked Posterior: Common. Average delay to diagnosis is 3-6 months. Requires major reconstruction (Allograft/Arthroplasty) vs simple reduction.
AVN
Late Collapse: 4-part fracture dislocations have high AVN rate. Warn patient pre-op. May need later conversion to arthroplasty.
Recurrent Instability
Recurrent Instability: Failure to address defect: If Reverse Hill-Sachs greater than 25% is ignored, it WILL dislocate again.
Stiffness
Fibrosis: Both surgery and immobilization cause stiffness. Early range of motion is key once stable. Frozen Shoulder: Secondary adhesive capsulitis is common. Hydrodilatation may be needed later.
Heterotopic Ossification
Associations: Associated with head injury or prolonged coma. Prophylaxis (Indomethacin/Radiation) may be considered in high-risk groups.
Nerve Injury
Axillary Nerve:
- Traction injury (Neuropraxia) common.
- 90% recover spontaneously in 3-6 months.
- EMG/NCS at 6 weeks if no recovery (deltoid firing).
Postoperative Care
Rehabilitation
- Anterior: Sling in Internal Rotation.
- Posterior: Braced in Neutral or External Rotation (Gunslinger) to relax posterior capsule and keep defect away from rim.
- Gentle passive ROM.
- Limit IR for Posterior repairs.
- Limit ER for Anterior repairs (Bankart/Subscap).
- AAROM then AROM.
- Hydrotherapy.
- Wean brace.
- Cuff strengthening.
- Scapular stabilization.
- Return to sport 6-9 months.
Outcomes
Prognosis
- Simple dislocation with GT fx: Excellent outcome if GT heals anatomically.
- Missed Posterior: Poor outcome without surgery. Arthroplasty usually successful for pain but ROM limited.
- McLaughlin Procedure: Good outcomes for medium defects, low recurrence rate.
- RTSA: Predictable elevation to 130 degrees, good pain relief. Functional rotation often limited.
| Treatment | Relief | ROM | Re-operation Risk |
|---|---|---|---|
| ORIF (Young) | High | Excellent (if no AVN) | Moderate (Screw cutout/AVN) |
| McLaughlin | High | Good (Limit IR) | Low |
| RTSA (Elderly) | High | Functional (Limit Rot) | Low (if stable) |
| Hemiarthroplasty | Moderate | Unpredictable | High (Tuberosity failure) |
Evidence Base
Key Studies
Hawkins - Locked Posterior Dislocation
- 41 locked posterior dislocations in 40 patients; diagnosis missed by the initial physician in the majority
- Mean interval from injury to diagnosis was 1 year; causes were MVA, seizure, alcohol, electroshock
- An axillary radiograph confirmed the diagnosis in every shoulder and showed the impression-defect size
- Treatment included accepted deformity, closed reduction, subscapularis or lesser-tuberosity transfer, hemi- and total arthroplasty
Neer - Displaced Proximal Humeral Fractures (Classification)
- Part I paper establishing the 4-segment classification (head, greater tuberosity, lesser tuberosity, shaft)
- Defines a part as displacement over 1 cm or angulation over 45 degrees
- Describes fracture-dislocation as a distinct, high-risk subgroup
- Forms the anatomical basis for fracture-dislocation pattern description
Robinson - Anterior Fracture-Dislocation ORIF
- 58 acute anterior fracture-dislocations; mean age 66 years
- Type-I head retains capsular attachment with arterial back-bleeding; type-II head devascularised
- Osteonecrosis in 2/23 type-I vs 4/7 type-II injuries after ORIF
- ORIF justified for type-I; elderly type-II best treated by hemiarthroplasty
Robinson - Complex Posterior Fracture-Dislocation
- Incidence of posterior fracture-dislocation 0.6 per 100,000 per year; peak in middle-aged men
- Most injuries occurred during a seizure or a fall from height
- All cases had an anatomical-neck fracture propagating from a reverse Hill-Sachs lesion; three subtypes described
- ORIF gave a median 2-year Constant score of 83.5 with low complication rate
Cicak - Posterior Dislocation of the Shoulder
- Review of diagnosis and management of posterior shoulder dislocation
- Emphasises clinical sign of fixed internal rotation with loss of external rotation
- CT recommended to quantify the reverse Hill-Sachs defect and guide treatment
- Defect size and chronicity direct the choice between transfer, graft and arthroplasty
Hertel - Predictors of Humeral Head Ischemia
- Prospective study of 100 intracapsular proximal humeral fractures
- Best ischemia predictors: short calcar (under 8 mm), disrupted medial hinge, anatomical-neck pattern
- Combined criteria gave a positive predictive value of up to 97% for ischemia
- Ischemia does not always progress to collapse (creeping substitution)
PROFHER - Surgery vs Nonsurgery for Proximal Humeral Fracture
- Multicentre RCT of 250 adults with displaced surgical-neck fractures (mean age 66)
- No significant difference in Oxford Shoulder Score over 2 years (39.07 surgical vs 38.32 nonsurgical)
- No difference in complications, secondary surgery or mortality
- Results do not support the trend of increasing surgery for these fractures
Sebastia-Forcada - RSA vs Hemiarthroplasty in Fracture
- Blinded RCT of 62 patients over 70 years with acute proximal humeral fracture
- Reverse shoulder arthroplasty gave higher Constant (56.1 vs 40.0) and UCLA scores than hemiarthroplasty
- Forward elevation 120 vs 80 degrees favouring RSA; outcome independent of tuberosity healing in the RSA group
- Lower revision rate with RSA (6 hemiarthroplasties required revision for proximal migration)
Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
"A 45-year-old man presents 4 weeks after an 'epileptic fit' with a stiff painful shoulder. X-rays are reported as normal. Diagnosis?"
"You are treating a 75-year-old female with an anterior fracture-dislocation (3-part). What factors influence your decision between ORIF and Arthroplasty?"
"Describe the 'Lightbulb Sign'."
MCQ Practice
Self-Assessment Questions
Q1: Posterior Dislocation Signs
Q: Which physical examination finding is pathognomonic for a locked posterior shoulder dislocation?
- A) Loss of abduction
- B) Fixed Internal Rotation (loss of External Rotation)
- C) Fixed External Rotation (loss of Internal Rotation)
- D) Palpable anterior mass
- E) Wrist drop
A: B - The hallmark of a locked posterior dislocation is the inability to externally rotate the arm (often blocked at neutral or in internal rotation) due to the head being engaged on the posterior glenoid rim.
Q2: Reverse Hill-Sachs
Q: A Reverse Hill-Sachs lesion is a defect of the:
- A) Posterolateral humeral head
- B) Anteromedial humeral head
- C) Anterior Glenoid rim
- D) Posterior Glenoid rim
- E) Greater Tuberosity
A: B - A Reverse Hill-Sachs lesion (impression fracture) occurs on the Anteromedial aspect of the humeral head due to impaction against the posterior glenoid rim during posterior dislocation. (Standard Hill-Sachs is Posterolateral).
Q3: Management Algorithm
Q: The Modified McLaughlin procedure involves transfer of which structure into a reverse Hill-Sachs defect?
- A) Greater Tuberosity / Supraspinatus
- B) Lesser Tuberosity / Subscapularis
- C) Conjoined Tendon
- D) Latissimus Dorsi
- E) Pectoralis Major
A: B - The Modified McLaughlin procedure involves osteotomy of the Lesser Tuberosity (with Subscapularis attachment) and transferring it into the anteromedial defect to fill the void and prevent internal rotation instability.
Q4: Nerve Injury
Q: Which nerve is most commonly injured in anterior fracture-dislocations of the shoulder?
- A) Radial Nerve
- B) Musculocutaneous Nerve
- C) Axillary Nerve
- D) Suprascapular Nerve
- E) Median Nerve
A: C - The Axillary nerve (wrapping around the surgical neck) is at highest risk during anterior fracture-dislocations, especially in elderly patients. Incidence ranges from 5-30%.
Q5: Reduction Risk
Q: You attempt closed reduction of a chronic (4 week) fracture-dislocation in the ED. What is the major risk?
- A) Recurrent dislocation
- B) Iatrogenic fracture of the surgical neck
- C) Brachial artery injury
- D) Rotator cuff tear
- E) Infection
A: B - Forceful manipulation of a chronic dislocation or fracture-dislocation risks completing the fracture pattern (e.g., propagating a crack into a complete surgical neck fracture), creating a free-floating head that requires complex surgery.
Guidelines, Registries & Global Practice
Global epidemiology
- Posterior fracture-dislocation incidence is approximately 0.6 per 100,000 per year, with a peak in middle-aged men (Robinson 2007).
- Posterior dislocations make up only 2-4% of shoulder dislocations but are missed initially in up to half of cases.
- Bimodal injury pattern: high-energy trauma in the young versus low-energy osteoporotic injury in the elderly.
Society guidance, side by side
| Body | Position relevant to fracture-dislocation |
|---|---|
| AAOS (US) | Evidence on proximal humeral fractures is largely inconclusive; shared decision-making and individualised treatment recommended |
| BOA / BOAST (UK) | Orthogonal imaging mandatory before reduction; urgent senior review for locked and neurovascularly compromised dislocations |
| AO Foundation | Classification-led planning; preserve medial calcar and head vascularity; ORIF for reconstructable patterns |
| EFORT / European consensus | Reverse arthroplasty favoured over hemiarthroplasty in elderly unreconstructable heads |
Registry signals
- Arthroplasty registries (AOANJRR, NJR, AJRR, Swedish/Norwegian) show a sustained shift from hemiarthroplasty toward reverse total shoulder arthroplasty for acute fracture in older patients, mirroring RCT evidence (Sebastia-Forcada 2014).
- RCT-level evidence (PROFHER) shows no benefit of surgery over nonoperative care for isolated displaced surgical-neck fractures, so registry surgery trends should be read as selective, not blanket.
High- versus limited-resource practice
- High-resource: routine CT for defect quantification, axillary/Velpeau views, arthroplasty backup, sub-specialist upper-limb referral for chronic locked dislocations.
- Limited-resource: reliance on plain orthogonal radiographs, greater use of closed reduction and transfer procedures, and earlier acceptance of deformity when implants are unavailable.
Shoulder Fx-Dislocation - Exam Quick Reference
Clinical summary
Key Facts
- •Posterior = Seizure/Shock/Blocked ER
- •Anterior = Trauma/Abducted
- •Signs: Lightbulb (Post), Axillary view (Gold std)
- •Defect: Reverse Hill-Sachs (Check size)
- •Risk: Axillary nerve palsy
Surgical Steps
- •Acute Anterior: Reduce then Fix Tuberosities
- •Acute Posterior: Reduce then Gunn slinger brace
- •Unstable Posterior: Modified McLaughlin (Subscap transfer)
- •Chronic/Elderly: RTSA (Reverse)
- •Approach: Deltopectoral (Workhorse)
- •Fixation: Locking plates + Sutures for cuff
Common Pitfalls
- •Missing the posterior dislocation on AP X-ray
- •Breaking the surgical neck during reduction
- •Ignoring the engaging defect (will redislocate)
- •Not checking Axillary nerve
- •Accepting a varus reduction (high failure rate)
Examiner Favorites
- •Lightbulb sign description
- •McLaughlin procedure details
- •Hertel criteria for Ischemia
- •Management of the missed posterior dislocation
- •Blood supply to the humeral head (Arcuate artery)
Radiology Signs
- •Lightbulb Sign (Posterior)
- •Rim Sign (Glenoid)
- •Trough Line (Reverse Hill-Sachs)
- •Mercedes Benz Sign (3-part GT fracture)