Unicameral Bone Cyst | Pediatric Metaphyseal Lesion | Pathological Fracture Risk
Neer Classification (Activity)
Critical Must-Knows
- Simple bone cyst is a solitary fluid-filled cavity with thin wall containing clear or blood-tinged fluid
- Peak incidence 5-15 years, proximal humerus (50%) and proximal femur (25%) most common sites
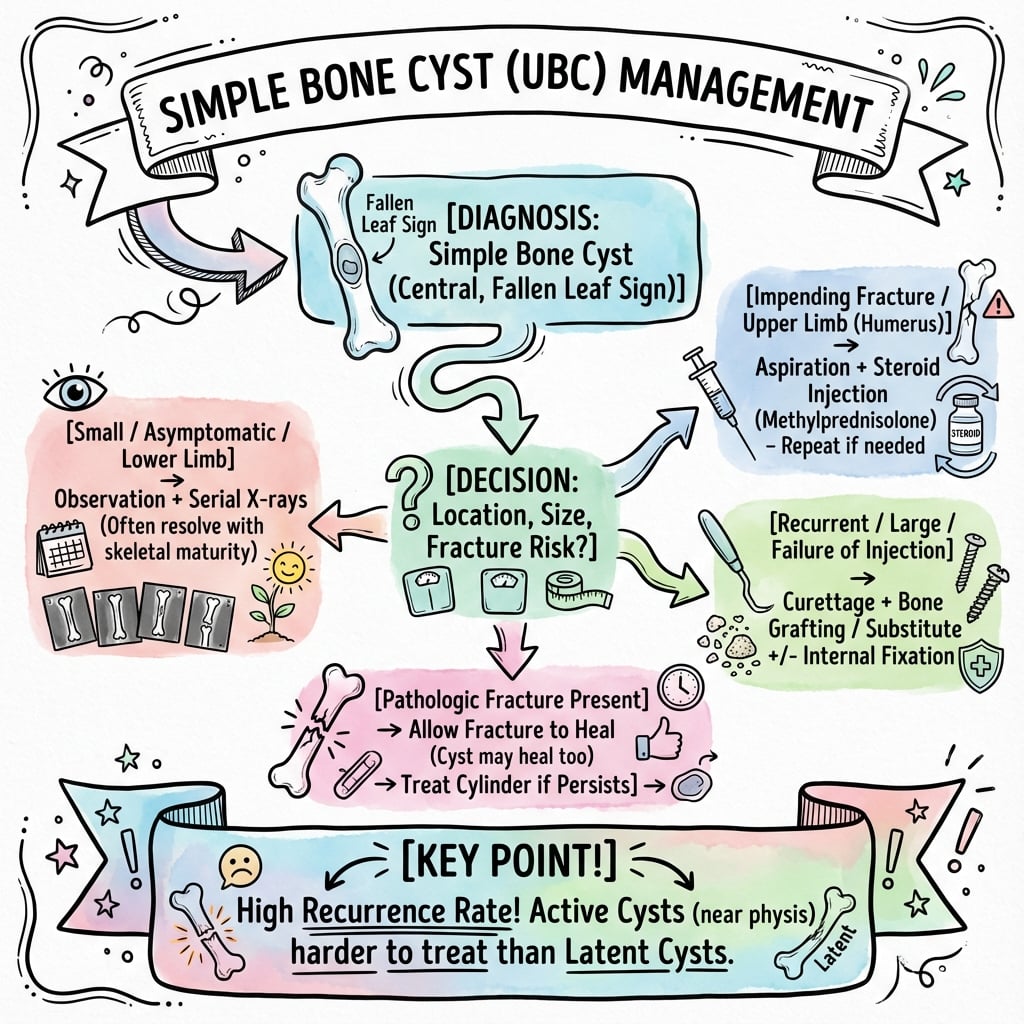
- 66% present with pathological fracture after minor trauma - fallen leaf sign pathognomonic
- Active cysts (adjacent to physis) have higher recurrence rates than latent cysts (separated from physis)
- Treatment options include observation, steroid injection, bone marrow aspiration, or curettage with grafting
Clinical Pearls
- "Fallen leaf sign: cortical fragment fallen to dependent portion of cyst after fracture
- "Rising bubble sign: contrast bubbles to top of fluid-filled cavity when injected
- "Active vs latent distinction critical for treatment decisions and prognosis
- "Multiple treatment modalities available - choice depends on age, location, fracture risk
Clinical Imaging
Imaging Gallery




Critical Simple Bone Cyst Exam Points
Pathognomonic Sign
Fallen leaf sign: Cortical fragment lying in dependent portion of cyst after pathological fracture. Confirms fluid-filled nature and distinguishes from solid lesions.
Active vs Latent
Neer Classification: Active cysts (adjacent to physis) are expanding and have higher recurrence (30-50%). Latent cysts (separated from physis) are more stable with lower recurrence (10-20%).
Differential Diagnosis
Key differentials: Aneurysmal bone cyst (fluid-fluid levels, eccentric, expansile), fibrous dysplasia (ground glass), enchondroma (rings and arcs calcification), eosinophilic granuloma (punched out).
Treatment Controversy
Multiple options exist: Observation (latent, small), steroid injection (gold standard, 60-90% success), bone marrow injection (newer, less invasive), curettage with grafting (definitive, surgical risk).
At a Glance
Simple bone cyst (unicameral bone cyst) is a solitary fluid-filled cavity with thin wall containing clear/serosanguinous fluid, occurring in children aged 5-15 years. Most common locations: proximal humerus (50%) and proximal femur (25%). 66% present with pathological fracture after minor trauma. Pathognomonic sign: "Fallen leaf sign" (cortical fragment lying in dependent portion of cyst). The Neer classification distinguishes Active cysts (adjacent to physis, higher recurrence 30-50%) from Latent cysts (separated from physis, 10-20% recurrence). Treatment options: steroid injection (gold standard, 60-90% success), bone marrow aspiration, curettage with grafting, or observation for latent cysts.
SIMPLESimple Bone Cyst Key Features
| S | Solitary fluid-filled cavity Single lesion with thin wall containing clear or serosanguinous fluid |
| I | Immature skeleton Peak incidence 5-15 years, rare after physeal closure |
| M | Metaphyseal location Adjacent to physis, migrates with growth (active to latent) |
| P | Proximal humerus/femur 75% in these locations, 50% humerus, 25% femur |
| L | Lytic centrally located Well-defined radiolucent lesion in medullary canal |
| E | Easy fracture risk 66% present with pathological fracture after minor trauma |
| S | Solitary fluid-filled cavity Single lesion with thin wall containing clear or serosanguinous fluid | M | Metaphyseal location Adjacent to physis, migrates with growth (active to latent) | L | Lytic centrally located Well-defined radiolucent lesion in medullary canal |
| I | Immature skeleton Peak incidence 5-15 years, rare after physeal closure | P | Proximal humerus/femur 75% in these locations, 50% humerus, 25% femur | E | Easy fracture risk 66% present with pathological fracture after minor trauma |
Hook:SIMPLE cyst = Solitary fluid in Immature Metaphysis, Proximal sites, Lytic, Easy to fracture!
FLATImaging Features
| F | Fallen leaf sign Cortical fragment in dependent portion after fracture (pathognomonic) |
| L | Lytic well-defined Radiolucent with thin sclerotic rim, central medullary location |
| A | Active or latent Active = adjacent to physis, Latent = separated by normal bone |
| T | Thin cortex expanded Cortical thinning with mild expansion, no periosteal reaction |
| F | Fallen leaf sign Cortical fragment in dependent portion after fracture (pathognomonic) | A | Active or latent Active = adjacent to physis, Latent = separated by normal bone |
| L | Lytic well-defined Radiolucent with thin sclerotic rim, central medullary location | T | Thin cortex expanded Cortical thinning with mild expansion, no periosteal reaction |
Hook:FLAT cyst on imaging: Fallen leaf, Lytic, Active/latent, Thin cortex!
SCAMTreatment Options
| S | Steroid injection Methylprednisolone 80-200mg, 60-90% success rate, gold standard |
| C | Curettage and grafting Definitive treatment, 90-95% success, surgical morbidity |
| A | Aspiration bone marrow Percutaneous BMA injection, 50-70% success, newer technique |
| M | Monitor (observation) For latent cysts, low fracture risk, asymptomatic patients |
| S | Steroid injection Methylprednisolone 80-200mg, 60-90% success rate, gold standard | A | Aspiration bone marrow Percutaneous BMA injection, 50-70% success, newer technique |
| C | Curettage and grafting Definitive treatment, 90-95% success, surgical morbidity | M | Monitor (observation) For latent cysts, low fracture risk, asymptomatic patients |
Hook:Treatment options: Steroid, Curettage, Aspiration, Monitor!
Overview and Epidemiology
Simple bone cyst (also called unicameral bone cyst or solitary bone cyst) is a benign fluid-filled cavity occurring in the metaphysis of long bones in children and adolescents. The cyst contains clear or blood-tinged serous fluid and is lined by a thin membrane of fibrous tissue. It represents approximately 3% of primary bone tumors and is one of the most common benign bone lesions in the pediatric population.
Clinical Significance
Simple bone cyst is clinically important because: (1) it typically presents with pathological fracture (66% of cases), causing pain and concern for malignancy; (2) the lesion weakens bone and creates ongoing fracture risk until healed; (3) active cysts adjacent to the physis have significant recurrence rates (30-50%) after treatment; and (4) multiple treatment modalities exist with varying success rates and morbidity, making management decisions complex.
Demographics
- Age: Peak 5-15 years (80% under 20 years)
- Sex: Male greater than female 2:1 to 3:1
- Location: 50% proximal humerus, 25% proximal femur
- Bilateral: Rare (less than 2% of cases)
Anatomical Distribution
- Proximal humerus: 50% of all cases
- Proximal femur: 25% of cases (higher fracture risk)
- Proximal tibia: 10% of cases
- Other sites: Calcaneus (5%), ilium, radius, fibula (rare)
Proximal Femur High-Risk Location
Proximal femur cysts have significantly higher fracture risk and complications due to weight-bearing stresses. Femoral neck cysts may cause coxa vara deformity and require more aggressive prophylactic treatment. Pathological fractures may lead to growth arrest or avascular necrosis in rare cases.
Pathophysiology and Etiology
Etiology Theories
The exact cause of simple bone cyst formation remains unclear, but several theories have been proposed based on histological and biochemical studies:
Etiological Theories of Simple Bone Cyst
| Theory | Mechanism | Supporting Evidence |
|---|---|---|
| Venous obstruction | Blockage of intraosseous venous drainage causes increased pressure and cystic cavity formation | Elevated venous pressure measured in active cysts, proximity to physis |
| Trauma theory | Intraosseous hematoma after trauma fails to resorb and forms cystic cavity | High incidence of initial presentation with fracture |
| Synovial rest theory | Ectopic synovial tissue produces fluid accumulation | Fluid composition similar to serum, presence of prostaglandins |
| Lysosomal enzyme theory | Increased lysosomal enzymes cause bone resorption and cyst formation | Elevated acid phosphatase and collagenase in cyst fluid |
Cyst Fluid Composition
Simple bone cyst fluid is typically clear or serosanguinous (yellow-brown) with biochemical composition similar to blood serum. The fluid contains elevated levels of prostaglandins (particularly PGE2), interleukin-1, and lysosomal enzymes. The rising bubble sign on cystography (contrast bubbles to top of cavity when injected) confirms the fluid-filled nature and distinguishes it from solid lesions.
Classification
Neer Classification (Activity-Based)
The Neer classification is the most widely used system, based on the relationship of the cyst to the physis:
Active Cyst:
- Adjacent to physis (less than 5mm separation)
- Expanding, symptomatic
- High fracture risk (50-66%)
- Higher recurrence rate after treatment (30-50%)
Latent Cyst:
- Separated from physis by normal bone (greater than 5mm)
- More stable, less likely to expand
- Lower fracture risk (20-30%)
- Lower recurrence rate (10-20%)
Neer Classification Summary
| Feature | Active Cyst | Latent Cyst |
|---|---|---|
| Distance from physis | Less than 5mm | Greater than 5mm |
| Behavior | Expanding, symptomatic | Stable, often asymptomatic |
| Fracture risk | 50-66% | 20-30% |
| Recurrence after treatment | 30-50% | 10-20% |
Clinical Presentation
Presentation Patterns
Presentation Modes of Simple Bone Cyst
| Presentation | Frequency | Clinical Features | Management Priority |
|---|---|---|---|
| Pathological fracture | 66% | Sudden pain after minor trauma, unable to use limb, swelling, deformity | Immobilize, rule out other pathology, plan definitive treatment |
| Incidental finding | 25% | Asymptomatic, discovered on X-ray for other reason, no pain or dysfunction | Assess fracture risk, consider prophylactic treatment if high risk |
| Pain without fracture | 9% | Vague aching pain, worse with activity, may indicate impending fracture | Protected weight-bearing, evaluate for microfractures, consider treatment |
History
Typical presentation in school-age child (5-15 years) with acute onset pain after minor trauma (falling during sports, reaching overhead, or stumbling). Parents often report the trauma seemed trivial compared to the severity of pain and inability to use the limb. In proximal femur lesions, child refuses to bear weight and has antalgic gait.
Pain Characteristics
- Onset: Sudden with fracture, gradual if no fracture
- Location: Well-localized to affected bone
- Severity: Severe with fracture, mild to moderate without
- Exacerbating: Weight-bearing (femur), overhead activity (humerus)
- Night pain: Absent (distinguishes from osteoid osteoma)
Functional Impact
- Upper limb: Difficulty lifting, throwing, overhead activities
- Lower limb: Antalgic gait, refusal to bear weight
- Fracture: Unable to use limb, protective guarding
- Activities: Usually unrestricted until fracture occurs
Physical Examination
Systematic Examination of Simple Bone Cyst
Swelling may be visible if superficial (proximal humerus). Deformity present if displaced fracture. Ecchymosis at fracture site. Arm held in protective position (humerus), leg externally rotated and shortened (femur fracture). Antalgic or non-weight-bearing gait if lower limb affected.
Localized tenderness to cyst location, worse at fracture site. Soft tissue swelling over fracture. May feel crepitus if fracture present. Temperature normal (not warm, distinguishes from infection). Lymph nodes not enlarged (no systemic features).
Active ROM limited by pain and protective muscle spasm. Passive ROM full if no fracture, limited and painful if fracture. Strength reduced due to pain and guarding. Assess fracture stability.
Pulses: radial/ulnar (humerus), dorsalis pedis/posterior tibial (femur). Sensation intact in all dermatomes. Motor: no neurological deficit (fractures usually minimally displaced). Compartments soft, no signs of compartment syndrome.
Proximal Femur Fracture Assessment
Displaced proximal femur fracture through bone cyst requires urgent assessment. Risk of further displacement causing neurovascular injury. Potential for growth plate involvement or avascular necrosis. Coxa vara deformity may develop if fracture heals with angulation. Early stabilization may be indicated for displaced fractures.
Investigations and Imaging
Plain Radiography
Plain X-rays are usually diagnostic and demonstrate characteristic features of simple bone cyst. Two orthogonal views (AP and lateral) are mandatory.
Classic Radiographic Features
- Location: Central medullary, metaphyseal
- Margins: Well-defined with thin sclerotic rim
- Pattern: Radiolucent (lytic) without matrix
- Cortex: Thinned but intact, mild expansion
- Periosteal reaction: None (unless fractured)
- Fallen leaf sign: Pathognomonic when present
Neer Classification (Activity)
- Active: Cyst margin contacts physis (less than 5mm separation)
- Latent: Normal bone between cyst and physis (greater than 5mm)
- Assessment: Measure closest distance from cyst to physis
- Prognosis: Active cysts have higher recurrence rates
Fallen Leaf Sign
The fallen leaf sign (also called falling fragment sign) is pathognomonic for simple bone cyst. After pathological fracture, a fragment of cortical bone breaks off and falls to the dependent (gravity-dependent) portion of the fluid-filled cavity. This proves the cystic nature and distinguishes from solid lesions. The fragment may be small or large, and position changes with patient positioning.


Neer Classification
The Neer classification categorizes cysts based on relationship to the growth plate and guides treatment decisions:
Neer Classification of Simple Bone Cyst
| Classification | Definition | Behavior | Recurrence Risk | Treatment Approach |
|---|---|---|---|---|
| Active | Adjacent to physis (less than 5mm) | Expanding, symptomatic, high fracture risk | 30-50% after treatment | Intralesional treatment, consider prophylactic fixation |
| Latent | Separated from physis (greater than 5mm) | Stable, lower fracture risk | 10-20% after treatment | Observation vs treatment based on location and size |
| Healing | After fracture or treatment | Sclerotic changes, cyst filling | May recur if incomplete healing | Observation, serial X-rays every 3-6 months |
Management Algorithm
Treatment Decision Framework
Management of simple bone cyst depends on multiple factors including patient age, cyst activity (active vs latent), anatomical location, fracture risk, and whether presenting with acute fracture.
Treatment Algorithm for Simple Bone Cyst
Confirm diagnosis with X-ray, rarely need MRI. Classify activity: Active (adjacent to physis) vs Latent (separated). Assess location: Proximal femur (high risk) vs humerus (lower risk). Fracture status: Acute fracture vs intact bone.
Immobilization with cast or splint (most fractures minimally displaced). Protected weight-bearing: Non-weight-bearing if femur. Pain control with NSAIDs and analgesia. Serial X-rays to monitor fracture healing and cyst response. Observation period 12-16 weeks to assess healing. Decision point: If cyst heals (20-30%), observe. If persists, plan treatment.
Observation: Latent cyst, small (less than 50% diameter), asymptomatic, low fracture risk. Steroid injection: Active or latent, moderate size, first-line minimally invasive treatment. Bone marrow injection: Alternative to steroids, newer technique, lower morbidity. Curettage and grafting: Large cysts, failed injections, high-risk locations (femoral neck).
Serial X-rays every 3-6 months first year, then 6-12 months. Assess healing: Cyst filling, cortical thickening, sclerosis. Monitor recurrence (20-30% overall recurrence rate). Repeat treatment if recurs, consider alternative modality. Discharge when cyst healed and physes closed (usually 2-3 years follow-up).
Surgical and Interventional Treatment
Corticosteroid Injection (Gold Standard Minimally Invasive)
Intralesional steroid injection is considered the gold standard first-line treatment for simple bone cyst. The technique was popularized by Scaglietti in 1982 and has success rates of 60-90% depending on technique and cyst characteristics.
Mechanism of Action
Corticosteroids are thought to work by reducing prostaglandin production (especially PGE2) which promotes bone resorption, decreasing inflammatory mediators and lysosomal enzyme activity, altering cyst fluid osmolality and reducing fluid accumulation, and stimulating bone formation by cyst wall membrane.
Technique
Steroid Injection Procedure
Informed consent: Discuss success rates (60-90%), need for multiple injections, risks. Anesthesia: General anesthesia (children) or sedation with local. Positioning: Supine for femur, beach chair for humerus. Image guidance: Fluoroscopy or ultrasound guidance mandatory. Sterile field: Full surgical scrub and draping.
Needle placement: Large bore needle (11-14 gauge) into cyst cavity under image guidance. Confirmation: Aspiration of clear or serosanguinous fluid confirms diagnosis. Fluid volume: Record volume aspirated (typically 10-100mL). Contrast injection: Optional - rising bubble sign confirms fluid cavity. Fluid analysis: Send for culture and cytology if diagnosis uncertain.
Agent: Methylprednisolone acetate (Depo-Medrol) most common. Dose: 80-200mg total dose (1-3 mL of 40mg/mL or 80mg/mL formulation). Multiple sites: Inject through 2-3 separate portals if large cyst. Distribution: Ensure even distribution throughout cavity. Needle removal: Remove needles, apply compression dressing.
Immobilization: Sling (humerus) or protected weight-bearing (femur) for 4-6 weeks. X-rays: At 6 weeks, 3 months, 6 months, 12 months. Healing criteria: Cortical thickening, cyst filling, sclerosis. Repeat injections: If no improvement by 6 months, repeat (up to 3 injections). Success: Complete healing or sufficient filling to prevent fracture.
Success Rates and Prognostic Factors
Factors Affecting Steroid Injection Success
| Factor | Higher Success Rate | Lower Success Rate |
|---|---|---|
| Cyst activity | Latent cysts (70-90%) | Active cysts (50-70%) |
| Location | Proximal humerus (75-90%) | Proximal femur (50-70%) |
| Age | Older children near skeletal maturity (80%) | Young children (60%) |
| Number of injections | Multiple injections (2-3) improves success to 80-90% | Single injection (60-70%) |
Multiple Injection Strategy
Serial injections improve success rates. Studies show that repeating steroid injection 2-3 times at 2-3 month intervals significantly improves healing rates from 60% (single injection) to 85-90% (multiple injections). The mechanism is cumulative effect on reducing fluid production and stimulating bone formation. Current practice is to inject, wait 6 months, and if no healing response, repeat up to total of 3 injections before considering surgical curettage.
This completes the steroid injection section.
Complications and Outcomes
Treatment-Related Complications
Complications by Treatment Modality
| Treatment | Common Complications | Rate | Management |
|---|---|---|---|
| Observation | Pathological fracture | 30-50% over 2 years | Immobilize, consider treatment after healing |
| Steroid injection | Failure to heal requiring repeat injection | 30-40% | Repeat injection up to 3 times total |
| Curettage and grafting | Recurrence of cyst | 5-15% | Repeat curettage or consider alternative treatment |


Prognosis Counseling
Overall prognosis is excellent: Over 95% of simple bone cysts eventually heal, either spontaneously, after fracture, or with treatment. The main morbidity is from pathological fractures (pain, time off school/sports, immobilization). Once healed, there are no long-term functional consequences. Malignant transformation does not occur. Most cysts resolve by skeletal maturity.
Postoperative Care
After Steroid/Bone Marrow Injection
Immediate Care:
- Outpatient procedure, discharge same day
- Sling (humerus) or crutches (femur) for comfort
- Oral analgesics as needed
Activity Modification:
- Protected weight-bearing for femur cysts (4-6 weeks)
- No contact sports for 6-8 weeks
- Avoid high-impact activities until healing confirmed
Follow-up Schedule:
- 6 weeks: First X-ray to assess initial response
- 3 months: Assess cyst filling, cortical thickening
- 6 months: Decision on repeat injection if needed
- 12 months: Confirm healing or plan further treatment
Outcomes
Treatment Success Rates
Steroid Injection:
- Single injection: 60-70% success
- Multiple injections (2-3): 85-90% success
- Active cysts: Lower success (50-70%)
- Latent cysts: Higher success (70-90%)
Curettage and Grafting:
- Overall success: 90-95%
- Recurrence rate: 5-15%
- Higher success in latent cysts
Natural History (Observation):
- 20-30% heal spontaneously after fracture
- Most cysts resolve by skeletal maturity
- Pathological fracture rate 30-50% if untreated
Evidence Base
Natural History and the Active vs Latent Classification
- Followed 175 cases and described cyst behaviour relative to the physis
- Introduced the active (abutting physis) vs latent (separated by normal bone) concept
- Showed a proportion of cysts heal after pathological fracture, but most persist without treatment
- Documented migration of the cyst away from the physis with continued skeletal growth
Intralesional Methylprednisolone Acetate - Original Series
- Reported favourable healing of bone cysts with repeated intralesional methylprednisolone acetate injection
- Authors abandoned routine open surgery for bone cysts from 1974 on the basis of these results
- Cited an approximately 25-30% recurrence rate after the surgical treatment they replaced
- Proposed corticosteroid acts on the pathological cyst lining to favour a reparative ossification process
Bone Marrow vs Steroid Injection - Landmark RCT
- 90 children randomised to bone marrow or methylprednisolone acetate injection; 77 followed for 2 years
- Healing in 16/38 (42%) of steroid-treated versus 9/39 (23%) of bone marrow-treated cysts (p = 0.01)
- No difference between groups in function, pain, number of injections, refracture or complications
- Radiographic healing assessed by a blinded radiologist (the only randomised trial in this field)
Steroid vs Autologous Bone Marrow - Recurrence and Number of Procedures
- 30 patients treated by steroid injection and 28 by autologous bone marrow grafting
- Overall success was similar: 86.7% (steroid) versus 92.0% (bone marrow), p greater than 0.05
- Success after a single procedure was lower for steroid (23.3%) than bone marrow (52.0%), p less than 0.05
- Recurrence after the first procedure was higher with steroid (41.7%) than bone marrow (13.3%), p less than 0.05
Comparative Effectiveness of Treatment Modalities - Meta-analysis
- 62 studies, 3,211 patients pooled; male-to-female ratio 2.2:1
- Methylprednisolone acetate injection healing 77.4% versus bone marrow injection 77.9% (comparable)
- Curettage with autograft or allograft both ~90%; flexible intramedullary nailing approached 100%
- Conservative (observation) healing 64.2%; active treatment outperformed observation
UBC vs ABC - Contemporary Review and Treatment Principles
- UBC is a fluid-filled, usually unicameral metaphyseal lesion; ABC is expansile, haemorrhagic and multicameral
- MRI fluid-fluid levels are evocative of ABC; distinguishing UBC from ABC is mandatory as treatment differs
- UBCs tend to resolve between adolescence and adulthood; principal concern is pathological fracture
- Femoral neck lesions at fracture risk may warrant curettage, bone substitute/graft and osteosynthesis
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Acute Presentation with Pathological Fracture
"A 9-year-old boy presents to ED with sudden onset left shoulder pain after falling while playing football. X-ray shows a minimally displaced pathological fracture through a proximal humerus lesion. The lesion is radiolucent, centrally located in the metaphysis, with a thin sclerotic rim and a small cortical fragment lying in the dependent portion of the cavity. How would you manage this patient?"
Scenario 2: Incidental Finding Requiring Treatment Decision
"A 12-year-old girl has an X-ray for wrist pain after gymnastics injury. The wrist X-ray is normal, but there is an incidental finding of a 3cm radiolucent lesion in the proximal humerus metaphysis, centrally located, with thin cortex and sclerotic rim. The lesion is immediately adjacent to the proximal humeral physis (less than 5mm). She has no shoulder pain and full function. How would you manage this?"
Scenario 3: Failed Treatment Requiring Next Steps
"A 10-year-old boy with a proximal femur simple bone cyst has undergone two steroid injections over the past 12 months without significant improvement. The cyst remains large (4cm, occupying 60% of femoral neck diameter) with very thin cortex. He has had one pathological fracture that healed, but the cyst persists. Family is frustrated and requesting definitive treatment. How would you counsel and manage?"
MCQ Practice Points
Clinical Pearl
Q: What is a unicameral (simple) bone cyst and what is its typical location?
A: Unicameral bone cyst (UBC) is a benign, fluid-filled lesion occurring in children and adolescents (peak age 5-15 years). Typical locations: Proximal humerus (50%), proximal femur (25%), proximal tibia, calcaneus. Classified as active (adjacent to physis, higher recurrence) or latent/inactive (separated from physis by normal bone). Contains straw-colored fluid with elevated prostaglandins. Often discovered incidentally or after pathological fracture (presenting symptom in 65-85%). Males affected more than females.
Clinical Pearl
Q: What is the "fallen leaf sign" and its diagnostic significance?
A: The fallen leaf sign (fallen fragment sign) is pathognomonic for UBC. On radiograph, after pathological fracture, a cortical fragment "falls" to the dependent portion of the cyst cavity, lying at the bottom like a leaf settling in water. Demonstrates the cyst contains fluid, not solid tissue. Confirms diagnosis without need for biopsy. Other imaging features: Central, metaphyseal, well-defined lytic lesion with sclerotic margins, mild expansion, no periosteal reaction (unless fractured). MRI shows homogeneous fluid signal.
Clinical Pearl
Q: What are the treatment options for unicameral bone cyst?
A: Observation: Small, asymptomatic cysts may resolve spontaneously, especially after skeletal maturity. Corticosteroid injection: Methylprednisolone acetate (40-80mg per injection) - aspirate fluid, inject steroid; repeat every 2-3 months × 3; 70-90% success rate. Bone marrow injection: Autologous bone marrow aspirate - similar success to steroids. Curettage and bone grafting: For persistent/recurrent cysts; higher recurrence rate (15-30%). Flexible nails: For humeral cysts - stabilize and decompress simultaneously. Pathological fracture: Usually heals with immobilization; may lead to cyst resolution.
Clinical Pearl
Q: How do you differentiate unicameral bone cyst from aneurysmal bone cyst?
A: UBC: Unilocular, fluid-filled, central medullary location, minimal expansion, contains straw-colored fluid, usually proximal humerus/femur, less aggressive appearance, fallen leaf sign possible. ABC: Multilocular ("soap bubble" appearance), blood-filled, more eccentric, marked expansion (may break cortex), "fluid-fluid levels" on MRI (blood products settling), more common spine and flat bones, can be primary or secondary to other lesions. Both occur in children/adolescents. ABC is more locally aggressive and requires more extensive treatment.
Clinical Pearl
Q: What factors predict higher recurrence rate after treatment of unicameral bone cyst?
A: Higher recurrence risk: Active cyst (adjacent to physis) - 50% recurrence vs 10% for latent; Younger age at diagnosis; Large cyst size; Proximal femur location (higher than humerus); Incomplete healing after first treatment. The cyst becomes "latent" as it migrates away from the physis with growth. Recurrence decreases after skeletal maturity. Many cysts resolve spontaneously after epiphyseal closure. Multiple injection sessions often needed - plan for 2-3 treatments before considering surgical intervention.
Guidelines, Registries & Global Practice
Global Epidemiology and Consensus
Simple bone cyst accounts for roughly 3% of primary bone lesions, with a consistent worldwide age peak of 5-15 years and a male predominance of about 2:1. The proximal humerus and proximal femur dominate every published series irrespective of region. There is no formal national-society clinical guideline dedicated to simple bone cyst; practice is driven by the evidence base (one randomised trial, several cohorts and a large meta-analysis) and by paediatric oncology referral pathways.
Areas of broad international agreement:
- Plain radiographs are usually diagnostic; MRI/biopsy reserved for atypical or treatment-refractory lesions to exclude aneurysmal bone cyst or other pathology
- Many lesions resolve toward skeletal maturity, so observation is acceptable for low-risk latent cysts
- Intralesional injection (steroid first-line) is the standard minimally invasive treatment
- Surgery with stabilisation is reserved for high-risk locations (notably femoral neck) and failed injection
Practice Framing Across Major Training Systems and Societies
| Body / System | Diagnostic emphasis | First-line treatment | Surgery threshold |
|---|---|---|---|
| AAOS / North America (ABOS) | Radiograph-led; MRI if atypical | Steroid or marrow injection; multimodal (decompression + substitute) increasingly used | Failed injection, femoral neck, recurrent fracture |
| BOA / UK (FRCS Tr&Orth) | Refer suspicious lesions to a bone tumour unit before intervention | Injection or observation per activity/risk | High-risk site or diagnostic uncertainty |
| EFORT / European (Mascard) | MRI fluid-fluid levels to separate UBC from ABC | Methylprednisolone injection for non-threatening lesions | Femoral neck at fracture risk: curettage, graft/substitute, fixation |
| FRACS / EBOT / DNB-MS / SICOT | Same radiograph-first principles; tumour-unit referral if doubt | Steroid injection; marrow where steroid less available | High-risk site, failed injection, impending fracture |
Registry and Evidence Note
Unlike arthroplasty, simple bone cyst is not tracked by joint or implant registries; the evidence base is the registry surrogate here. The single highest-level evidence is the Wright et al. multicentre RCT (steroid superior to bone marrow for healing), supported by the Kadhim et al. meta-analysis (62 studies, over 3,200 patients) showing comparable healing for steroid and bone marrow injection and high healing with curettage or flexible nailing.
SIMPLE BONE CYST (Unicameral Bone Cyst)
Clinical summary
Definition and Epidemiology
- •Benign fluid-filled cavity in metaphysis of long bones in children
- •3% of primary bone tumors, peak age 5-15 years, male greater than female 2-3:1
- •50% proximal humerus, 25% proximal femur, 75% in these two locations
- •66% present with pathological fracture after minor trauma
- •Thin-walled cavity containing clear or serosanguinous fluid (10-100mL)
Classification (Neer)
- •Active: adjacent to physis (less than 5mm), expanding, high fracture risk, recurrence 30-50%
- •Latent: separated from physis (greater than 5mm), stable, lower fracture risk, recurrence 10-20%
- •Healing: after fracture or treatment, sclerotic changes, cyst filling with bone
- •Classification guides treatment decisions and prognosis
Pathognomonic Signs
- •Fallen leaf sign: cortical fragment in dependent portion after fracture (pathognomonic)
- •Rising bubble sign: contrast bubbles to top when injected into fluid cavity
- •Central medullary location, thin sclerotic rim, no periosteal reaction unless fractured
- •No fluid-fluid levels (distinguishes from ABC), no matrix (distinguishes from enchondroma)
Differential Diagnosis
- •ABC: eccentric, expansile, fluid-fluid levels on MRI, blow-out appearance
- •Fibrous dysplasia: ground-glass matrix, expansile, no fluid content
- •Enchondroma: rings and arcs calcification, hands/feet, chondroid matrix
- •Eosinophilic granuloma: punched-out, periosteal reaction, elevated ESR, button sequestrum
Treatment Algorithm
- •Acute fracture: immobilize, observe 12-16 weeks (20-30% heal spontaneously)
- •Observation: latent, small (less than 50% diameter), low fracture risk, asymptomatic
- •Steroid injection: first-line treatment, 60-90% success, 80-200mg methylprednisolone, may repeat 2-3 times
- •Bone marrow injection: alternative to steroids, 50-70% success, requires iliac crest aspiration
- •Curettage and grafting: definitive treatment, 90-95% success, for failed injections or high-risk lesions
High-Yield Exam Points
- •Active vs latent distinction is critical for prognosis and treatment decisions
- •Proximal femur is high-risk location (weight-bearing, higher recurrence, coxa vara risk)
- •Multiple steroid injections (2-3) better than single injection (85-90% vs 60%)
- •Overall prognosis excellent: over 95% heal, no malignant transformation, no long-term disability
- •Most cysts resolve spontaneously after skeletal maturity
Complications to Know
- •Pathological fracture: 66% at presentation, 30-50% during observation
- •Recurrence: 30-50% active cysts, 10-20% latent cysts, 5-15% after curettage
- •Coxa vara: proximal femur fractures healing in varus (rare)
- •Growth arrest: very rare, reported with aggressive treatment near physis
- •Treatment failure: 30-40% after single steroid injection, 10% after curettage
Viva Pearls
- •Steroid injection is gold standard minimally invasive treatment (better evidence than bone marrow)
- •Observation after first fracture is appropriate (avoid overtreatment, 20-30% heal)
- •Prophylactic fixation may be needed for large proximal femur cysts (greater than 50% diameter)
- •Adjuvants (phenol, burr) may reduce recurrence but avoid within 1-2cm of physis
- •MRI indicated if atypical presentation or failed treatment to exclude ABC component
References
-
Neer CS, Francis KC, Marcove RC, et al. Treatment of unicameral bone cyst: a follow-up study of one hundred seventy-five cases. J Bone Joint Surg Am. 1966;48(4):731-745.
-
Scaglietti O, Marchetti PG, Bartolozzi P. Final results obtained in the treatment of bone cysts with methylprednisolone acetate (depo-medrol) and a discussion of results achieved in other bone lesions. Clin Orthop Relat Res. 1982;(165):33-42.
-
Kadhim M, Thacker M, Kadhim A, Holmes L Jr. Treatment of unicameral bone cyst: systematic review and meta-analysis. J Child Orthop. 2014;8(2):171-191. doi:10.1007/s11832-014-0566-3
-
Cho HS, Oh JH, Kim HS, Kang HG, Lee SH. Unicameral bone cysts: a comparison of injection of steroid and grafting with autologous bone marrow. J Bone Joint Surg Br. 2007;89(2):222-226. doi:10.1302/0301-620X.89B2.18116
-
Wright JG, Yandow S, Donaldson S, Marley L. A randomized clinical trial comparing intralesional bone marrow and steroid injections for simple bone cysts. J Bone Joint Surg Am. 2008;90(4):722-730. doi:10.2106/JBJS.G.00620
-
Mascard E, Gomez-Brouchet A, Lambot K. Bone cysts: unicameral and aneurysmal bone cyst. Orthop Traumatol Surg Res. 2015;101(1 Suppl):S119-S127. doi:10.1016/j.otsr.2014.06.031
-
Campanacci M, Capanna R, Picci P. Unicameral and aneurysmal bone cysts. Clin Orthop Relat Res. 1986;(204):25-36.
-
Chang CH, Stanton RP, Glutting J. Unicameral bone cysts treated by injection of bone marrow or methylprednisolone. J Bone Joint Surg Br. 2002;84(3):407-412. doi:10.1302/0301-620x.84b3.12115
-
Dormans JP, Sankar WN, Moroz LA, Erol B. Percutaneous intramedullary decompression, curettage, and grafting with medical-grade calcium sulfate pellets for unicameral bone cysts in children: a new minimally invasive technique. J Pediatr Orthop. 2005;25(6):804-811. doi:10.1097/01.bpo.0000173244.64427.38
-
Rapp TB, Ward JP, Alaia MJ. Aneurysmal bone cyst. J Am Acad Orthop Surg. 2012;20(4):233-241. doi:10.5435/JAAOS-20-04-233