Split vs Full Thickness, and What a Graft Will (and Won't) Take On
- A skin graft is a FREE transfer of skin with NO intrinsic blood supply, so it depends entirely on the RECIPIENT BED for survival - it takes in three phases: PLASMATIC IMBIBITION (0-48h, nutrients diffuse from the bed), INOSCULATION (48-72h, graft and bed capillaries link up) and REVASCULARISATION (~day 4-7, new vessels grow in).
- Because of this, a graft will only take on a WELL-VASCULARISED bed; it will NOT reliably take on BARE CORTICAL BONE (without periosteum), BARE TENDON (without paratenon), BARE CARTILAGE (without perichondrium), heavily contaminated/infected wounds, or irradiated tissue - such defects need a FLAP. With intact periosteum/paratenon a graft can still take.
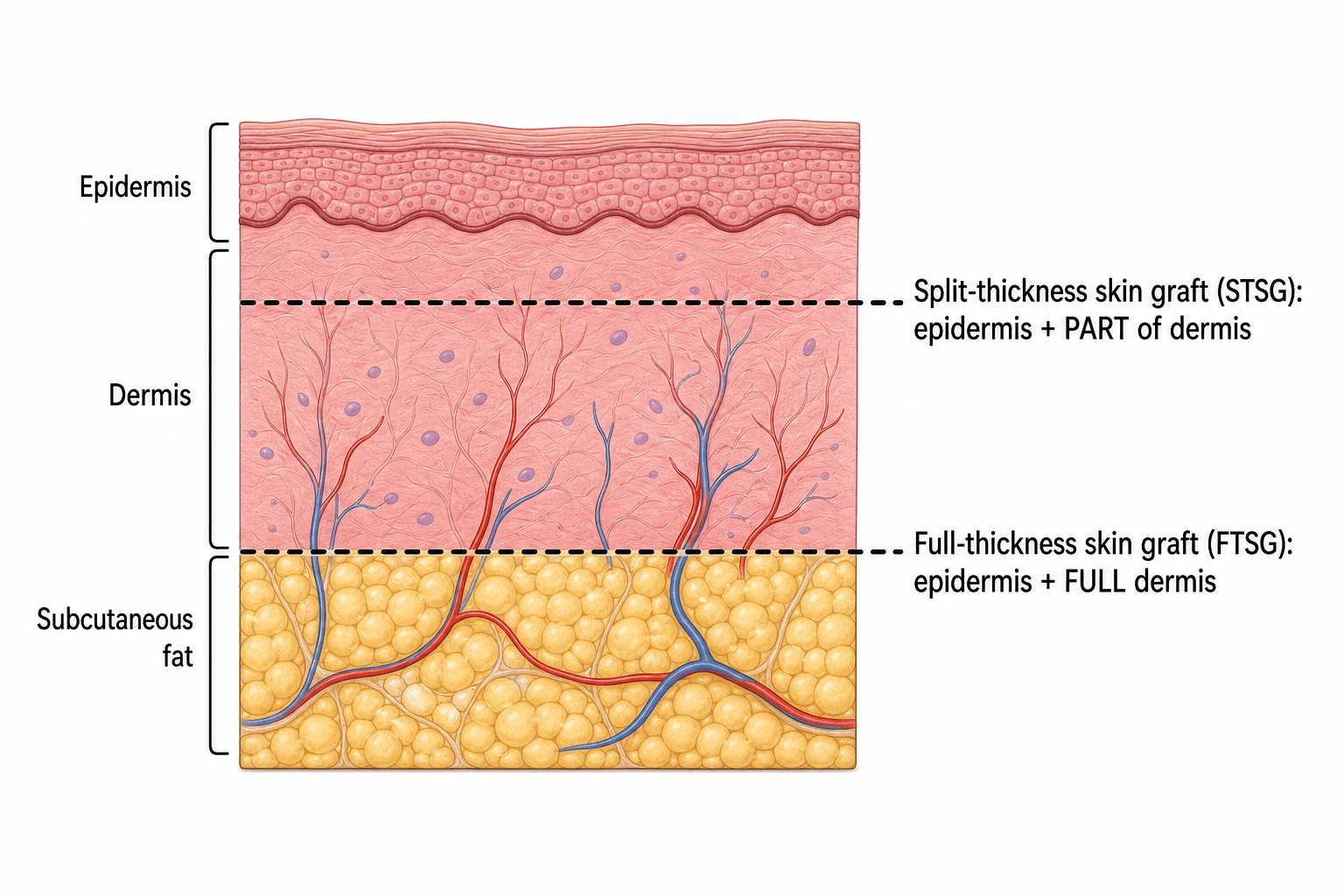
- SPLIT-THICKNESS grafts (epidermis + part of dermis) take more reliably and cover large areas, the donor site heals by re-epithelialisation, but they undergo MORE secondary CONTRACTION and give poorer durability, sensation and colour - so in the hand they are used for large or dorsal defects, granulating wounds and temporary cover.
- FULL-THICKNESS grafts (epidermis + the full dermis) undergo LESS secondary contraction and give better durability, sensation and colour match, so they are preferred on the PALM, the FINGERTIPS and ACROSS FLEXION CREASES (where contracture would be disastrous); the trade-off is that they need a cleaner, better-vascularised bed and the donor site must be closed primarily, limiting size.
- DONOR-SITE choice matters: common hand FTSG donors are the wrist/hypothenar crease, antecubital fossa, medial arm and groin; GLABROUS skin (hypothenar eminence, instep) is chosen for PALMAR/fingertip defects to match the special palmar skin; STSG is usually harvested from the thigh.
- GRAFT FAILURE is most often due to HAEMATOMA or SEROMA lifting the graft off the bed, INFECTION, or SHEAR/movement - so meticulous haemostasis, a bolster/tie-over dressing, and IMMOBILISATION are essential; the graft fits on the RECONSTRUCTIVE LADDER above primary closure/secondary intention and below local/regional and free flaps.
- “Graft take = imbibition (0-48h) -> inosculation (48-72h) -> revascularisation (~day 4-7); needs a vascular bed.
- “Won't take on bare bone/tendon/cartilage (no periosteum/paratenon/perichondrium), infected or irradiated beds -> use a FLAP.
- “FTSG (less contracture, durable, sensate) for palm/fingertips/flexion creases; STSG (reliable, large) for dorsum/large wounds. Failure = haematoma/infection/shear.
A well-vascularised bed: muscle, fascia, granulation, paratenon-covered tendon, periosteum-covered bone, perichondrium-covered cartilage.
Bare cortical bone, bare tendon, bare cartilage, infected/heavily contaminated or irradiated beds, or exposed hardware/joint - cover with a flap.
Graft Types & Take Physiology
A skin graft carries no blood supply of its own, so it survives only if the recipient bed can nourish and revascularise it. Take occurs in three phases: plasmatic imbibition in the first ~48 hours, when the graft absorbs nutrients by diffusion from the bed; inosculation at ~48-72 hours, when graft and bed capillaries align and connect; and revascularisation from about day 4-7, when new vessels grow into the graft. A split-thickness graft (epidermis + part of dermis) is thinner, so it imbibes and revascularises more readily and takes more reliably, but it contracts more and is less durable; a full-thickness graft (epidermis + full dermis) needs a better bed but contracts less and is more durable and sensate.
| Feature | Split-thickness (STSG) | Full-thickness (FTSG) |
|---|
Hand-Specific Principles & Donor Sites
- Palm and fingertips: use a FTSG, ideally from GLABROUS (non-hairy) skin - the hypothenar eminence or the instep - to match the thick, hairless, durable palmar skin and provide better sensation; an FTSG/glabrous graft is reliable for fingertip and donor-site defects.
- Across flexion creases: prefer FTSG (or a flap) because STSG secondary contraction can cause a flexion contracture - a major functional problem in the hand.
- Dorsum and large defects: STSG (e.g. from the thigh) gives reliable cover; meshing expands area and lets exudate escape but worsens cosmesis/contraction.
- Donor sites for FTSG: wrist/hypothenar crease, antecubital fossa, medial arm, groin (hairless areas preferred for the hand).
- Exposed bone/tendon/cartilage without periosteum/paratenon/perichondrium, or infected/irradiated beds: a graft will fail - choose a flap (local, regional or free).
The commonest reasons a graft fails are a HAEMATOMA or SEROMA lifting it off the bed, INFECTION, and SHEAR/movement. Prevent these with meticulous haemostasis, a bolster (tie-over) dressing or negative-pressure dressing to maintain contact, and immobilisation/splinting of the hand for the first ~5 days; treat any infection and avoid grafting onto a clearly contaminated wound (delayed grafting after the bed is clean - 'delayed primary' grafting - is an option). Counsel about graft hyperpigmentation and reduced bulk.
Evidence & Key Studies
Comparison of reading man flap and skin grafting for donor defects in homodigital reverse-flow flaps
- For donor-site defects of homodigital fingertip flaps, full-thickness skin grafting and the reading-man flap gave SIMILAR flap survival, complications, range of motion, two-point discrimination and aesthetic outcomes.
- No patients developed cold intolerance or hypersensitivity, supporting FTSG as a reliable option for finger donor-site resurfacing.
- Demonstrates the role of skin grafting within the reconstructive options for fingertip/donor defects.
Delayed primary full-thickness skin graft for a distal interphalangeal fingertip injury: a case report
- A fingertip injury with bone exposed distal to the DIP but with INTACT PERIOSTEUM (and no tendon over the bone) was reconstructed with a full-thickness skin graft after wound preparation.
- The literature review emphasises that FTSGs are unreliable over poorly vascularised beds and only work without serious blood-supply issues - i.e. an adequate vascular bed is essential.
- Outcomes were good function and aesthetics with normal touch/vibration; disadvantages were limited soft-tissue volume and graft hyperpigmentation.
According to PubMed, the reliability of FTSG for fingertip/donor-site resurfacing comes from the cited Qin comparison, and the requirement for an adequately vascularised bed (FTSG over periosteum-covered bone, not bare bone) and the FTSG advantages/disadvantages from the cited Soraya case report. The graft-take phases, STSG/FTSG properties and the reconstructive ladder are standard, well-established plastic/hand-surgery teaching. (See also our Fingertip Injuries, Wound Closure Techniques and Soft-Tissue Coverage topics.)
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“What is the difference between a split- and full-thickness skin graft, how does a graft take, and how would you choose between them in the hand?”
“A graft you placed on the hand has failed. What are the likely reasons and how do you prevent them?”
Mnemonics & Memory Aids
III (take)
Hook:Graft take = the three I's: Imbibition, Inosculation, Ingrowth.
HIS (failure)
Hook:Grafts fail for HIS reasons: Haematoma, Infection, Shear.
Types
- STSG: epidermis + part dermis - reliable, large, donor re-epithelialises, but MORE contraction
- FTSG: epidermis + full dermis - less contraction, durable, sensate; donor closed primarily
- Glabrous FTSG (hypothenar/instep) for palmar/fingertip match
Take physiology
- Imbibition (0-48h) -> inosculation (48-72h) -> revascularisation (~day 4-7)
- Needs a WELL-VASCULARISED bed (no own blood supply)
- Won't take: bare bone/tendon/cartilage, infected/irradiated -> FLAP
Hand choices
- Palm/fingertips/flexion creases: FTSG (avoid STSG contracture)
- Dorsum/large/temporary: STSG (+/- mesh)
- FTSG donors: wrist/hypothenar, antecubital, medial arm, groin
Failure & prevention
- Causes: haematoma/seroma, infection, shear, poor bed
- Prevent: haemostasis, mesh/fenestrate, bolster/tie-over or NPWT, immobilise
- Reconstructive ladder: graft sits below flaps, above primary/secondary closure