Standardized Assessment | Six Components | Instability Classification
SINS INTERPRETATION
Critical Must-Knows
- Six components: Location, Pain, Bone lesion, Alignment, VB collapse, Posterolateral elements
- Score 13+ = unstable, requires surgical stabilization
- Junctional location (C0-C2, C7-T2, T11-L1, L5-S1) scores highest (3 points)
- Mechanical pain (worse with movement/loading) scores 3 points vs 1 for non-mechanical
- Bilateral posterolateral involvement scores 3 points (maximum instability)
Clinical Pearls
- "SINS was developed by Spinal Oncology Study Group (SOSG) in 2010
- "Calculate SINS for every metastatic spine viva case
- "Lytic lesions score higher than blastic (worse mechanical properties)
- "SINS assesses MECHANICAL instability, not neurological status
Critical SINS Exam Points
Score Thresholds
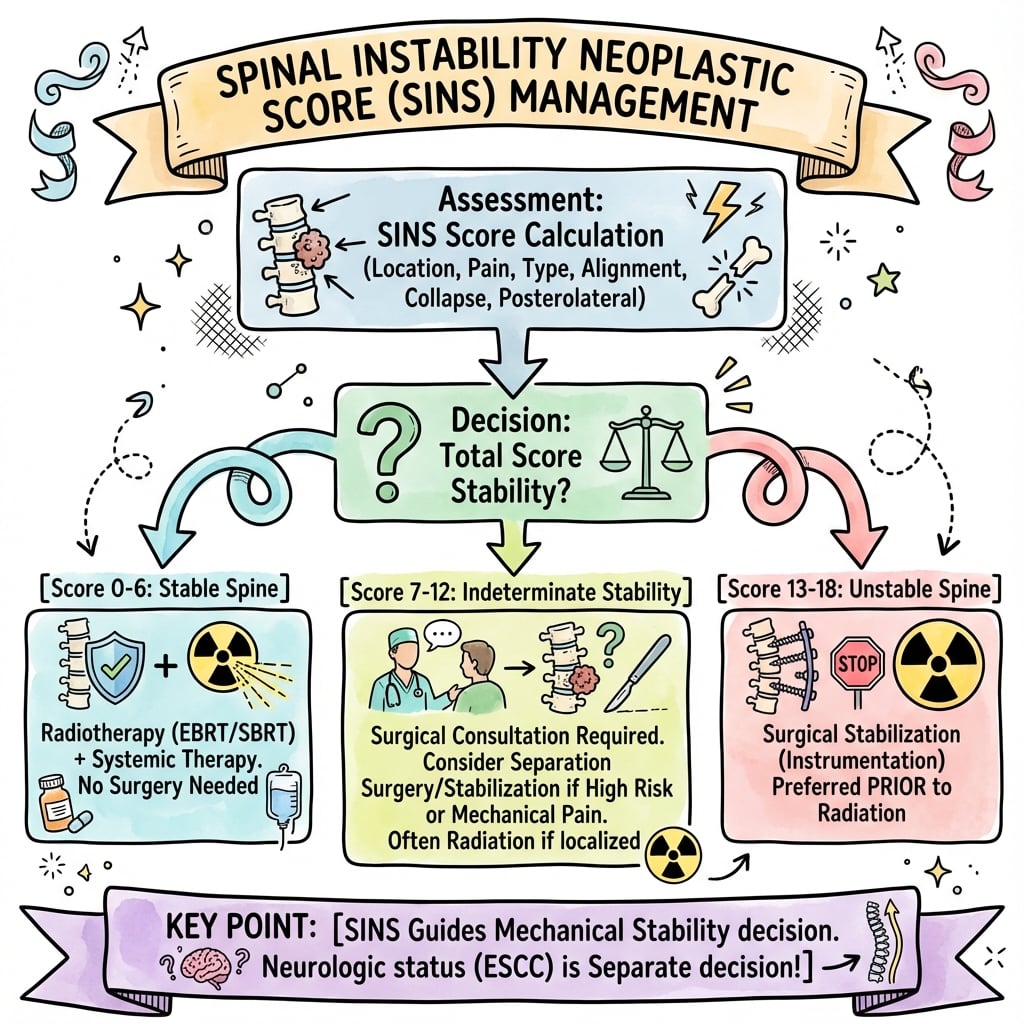
Memorize the cutoffs: 0-6 = stable (no consult), 7-12 = indeterminate (consult), 13-18 = unstable (surgery). A score of 13 or higher mandates surgical stabilization regardless of neurological status.
Location Scoring
Junctional zones are critical: Occipitocervical (C0-C2), cervicothoracic (C7-T2), thoracolumbar (T11-L1), and lumbosacral (L5-S1) score 3 points. Mobile spine scores 2, semi-rigid (T3-T10) scores 1, rigid (S2-S5) scores 0.
Pain Assessment
Mechanical vs non-mechanical: Mechanical pain (worse with movement, loading, upright position, relieved lying down) scores 3. Non-mechanical (constant, not movement-related) scores 1. Pain-free scores 0.
Imaging Assessment
Use CT for bone detail: Bone lesion quality (lytic=2, mixed=1, blastic=0), alignment, collapse, and posterolateral involvement are best assessed on CT. MRI for soft tissue and cord assessment.
SINS Component Scoring
| Component | Finding | Score |
|---|---|---|
| Location | Junctional (C0-C2, C7-T2, T11-L1, L5-S1) | 3 |
| Location | Mobile spine (C3-C6, L2-L4) | 2 |
| Location | Semi-rigid (T3-T10) | 1 |
| Location | Rigid (S2-S5) | 0 |
| Pain | Mechanical (movement-related) | 3 |
| Pain | Non-mechanical (constant/occasional) | 1 |
| Pain | None | 0 |
| Bone Lesion | Lytic | 2 |
| Bone Lesion | Mixed | 1 |
| Bone Lesion | Blastic | 0 |
| Alignment | Subluxation/translation | 4 |
| Alignment | De novo deformity (kyphosis/scoliosis) | 2 |
| Alignment | Normal | 0 |
| VB Collapse | Greater than 50% collapse | 3 |
| VB Collapse | Less than 50% collapse | 2 |
| VB Collapse | No collapse, over 50% body involved | 1 |
| VB Collapse | None of the above | 0 |
| Posterolateral | Bilateral involvement | 3 |
| Posterolateral | Unilateral involvement | 1 |
| Posterolateral | None | 0 |
At a Glance
The Spinal Instability Neoplastic Score (SINS) is a validated classification (Spinal Oncology Study Group, 2010) for assessing mechanical instability in metastatic spine disease. Six components scored: Location (junctional=3, mobile=2, semi-rigid=1, rigid=0), Pain (mechanical=3, non-mechanical=1, none=0), Bone lesion quality (lytic=2, mixed=1, blastic=0), Alignment (subluxation=4, deformity=2, normal=0), Vertebral body collapse (over 50%=3, under 50%=2), and Posterolateral elements (bilateral=3, unilateral=1). Score interpretation: 0-6 = stable (no surgical consultation), 7-12 = indeterminate (consult recommended), 13-18 = unstable (surgical stabilization indicated regardless of neurology). SINS assesses mechanical instability only—neurological status requires separate evaluation. Calculate SINS for every metastatic spine viva case.
LPBAVPSINS Components - LPBAVP
| L | Location Junctional=3, Mobile=2, Semi-rigid=1, Rigid=0 |
| P | Pain Mechanical=3, Non-mechanical=1, None=0 |
| B | Bone lesion quality Lytic=2, Mixed=1, Blastic=0 |
| A | Alignment Sublux=4, Deformity=2, Normal=0 |
| V | Vertebral body collapse Over 50%=3, Under 50%=2, Over 50% involved=1, None=0 |
| P | Posterolateral elements Bilateral=3, Unilateral=1, None=0 |
| L | Location Junctional=3, Mobile=2, Semi-rigid=1, Rigid=0 | B | Bone lesion quality Lytic=2, Mixed=1, Blastic=0 | V | Vertebral body collapse Over 50%=3, Under 50%=2, Over 50% involved=1, None=0 |
| P | Pain Mechanical=3, Non-mechanical=1, None=0 | A | Alignment Sublux=4, Deformity=2, Normal=0 | P | Posterolateral elements Bilateral=3, Unilateral=1, None=0 |
Hook:LPBAVP - Location Pain Bone Alignment Vertebral Posterolateral. Max score 18.
SINS SSINS Score Interpretation
| S | Stable (0-6) No surgical consultation needed - treat oncologically |
| I | Indeterminate (7-12) Surgical consultation recommended - clinical judgment |
| N | Needs surgery (13-18) Unstable - surgical stabilization required |
| S | Stable (0-6) No surgical consultation needed - treat oncologically |
| I | Indeterminate (7-12) Surgical consultation recommended - clinical judgment |
| N | Needs surgery (13-18) Unstable - surgical stabilization required |
Hook:SIN threshold: 7 for consult, 13 for Needs surgery
OCTLJunctional Zones - High Score Locations
| O | Occipitocervical (C0-C2) 3 points - craniovertebral junction |
| C | Cervicothoracic (C7-T2) 3 points - mobile-rigid transition |
| T | Thoracolumbar (T11-L1) 3 points - rigid-mobile transition |
| L | Lumbosacral (L5-S1) 3 points - mobile-rigid transition |
| O | Occipitocervical (C0-C2) 3 points - craniovertebral junction | T | Thoracolumbar (T11-L1) 3 points - rigid-mobile transition |
| C | Cervicothoracic (C7-T2) 3 points - mobile-rigid transition | L | Lumbosacral (L5-S1) 3 points - mobile-rigid transition |
Hook:OCTL junctions score 3 - transitions between mobile and rigid spine
Overview and Background
The Spinal Instability Neoplastic Score (SINS) was developed by the Spinal Oncology Study Group (SOSG) in 2010 to standardize the assessment of spinal instability in patients with neoplastic disease.
Rationale for Development:
Prior to SINS, there was no standardized method to assess mechanical instability in metastatic spine disease. This led to inconsistent management and communication between specialties.
Clinical Significance:
| SINS Score | Category | Clinical Implication |
|---|---|---|
| 0-6 | Stable | No surgical consult needed |
| 7-12 | Indeterminate | Surgical consultation recommended |
| 13-18 | Unstable | Surgical stabilization required |
Validation:
SINS has been validated in multiple studies with near-perfect reliability (interobserver ICC 0.846, intraobserver ICC 0.886 in the Fourney et al. validation). It is now widely adopted in clinical practice and incorporated into major treatment frameworks including NOMS.
SINS vs Neurology
SINS assesses MECHANICAL instability only. It does NOT assess neurological status or epidural cord compression. Use Bilsky grading for neurological assessment. A spine can be mechanically stable (low SINS) but have severe cord compression (high Bilsky), and vice versa.
SINS Components in Detail
Spinal Location (0-3 points)
Based on biomechanical stability of different spinal regions.
| Location | Points | Rationale |
|---|---|---|
| Junctional (C0-C2, C7-T2, T11-L1, L5-S1) | 3 | Transitions between mobile/rigid segments |
| Mobile spine (C3-C6, L2-L4) | 2 | High mobility increases instability risk |
| Semi-rigid (T3-T10) | 1 | Ribcage provides some stability |
| Rigid (S2-S5) | 0 | Fused segments, inherently stable |
Junctional zones are where mobile and rigid segments meet. These areas experience high mechanical stress and are prone to failure when involved by tumor.
Pathophysiology of Spinal Metastatic Instability
Biomechanical Principles
Three-Column Concept:
The Denis three-column model provides the foundation for understanding spinal stability:
| Column | Structures | Role in Stability |
|---|---|---|
| Anterior | Anterior longitudinal ligament, anterior 2/3 vertebral body | Resists extension |
| Middle | Posterior 1/3 vertebral body, posterior longitudinal ligament | Key load-bearing column |
| Posterior | Pedicles, facets, laminae, spinous processes, ligaments | Resists flexion, provides tension band |
Metastatic Destruction Pattern:
Spinal metastases typically begin in the vertebral body (anterior and middle columns) due to the rich vascular supply of cancellous bone via the Batson venous plexus. As tumor expands, it progressively destroys load-bearing trabecular bone.
Load Transfer Mechanism
Normal Spine:
In the upright position, approximately 80% of axial load passes through the anterior and middle columns (vertebral bodies and discs), while 20% passes through the posterior column (facet joints).
Metastatic Involvement:
When tumor destroys vertebral body bone, load-bearing capacity decreases proportionally to bone loss. Stress concentration occurs at tumor margins, microfractures propagate through weakened bone, and progressive collapse ensues.
Threshold for Failure:
Biomechanical studies suggest that loss of approximately 30-50% of vertebral body involvement significantly increases fracture risk. This correlates with the SINS scoring where greater than 50% body involvement scores 1 point even without collapse.
Lytic vs Blastic Lesions
Lytic Lesions (2 points in SINS):
Osteoclast-mediated bone destruction results in loss of trabecular architecture. Common in lung, renal cell, thyroid, and breast carcinoma. Mechanical strength decreases dramatically as bone is replaced by tumor tissue with minimal structural integrity.
Blastic Lesions (0 points in SINS):
Osteoblast-mediated new bone formation creates sclerotic bone. Common in prostate carcinoma. Although this bone may be abnormal in quality, it retains load-bearing capacity and is less prone to collapse.
Mixed Lesions (1 point in SINS):
Combination of lytic and blastic components. The net effect on stability depends on the proportion of each component. Breast cancer commonly produces mixed lesions.
Junctional Zone Biomechanics
Why Junctions Score Higher:
Junctional zones (cervicothoracic, thoracolumbar, lumbosacral) represent transitions between mobile and rigid spinal segments. These areas experience higher mechanical stress due to concentration of forces at the transition point.
The thoracolumbar junction (T11-L1) is the most common site of pathological fracture because it marks the transition from the rigid, ribcage-supported thoracic spine to the mobile lumbar spine.
Posterior Element Contribution
Tension Band Mechanism:
The posterior elements function as a tension band during flexion. When intact, they limit kyphotic collapse by resisting distraction forces on the posterior spine.
Bilateral Involvement (3 points):
Destruction of bilateral pedicles, facets, or costovertebral joints eliminates the tension band effect completely. This allows unchecked progressive kyphotic collapse and significantly increases instability.
Biomechanical Basis of SINS
Each SINS component reflects a specific biomechanical principle: location (stress concentration at junctions), pain (symptom of structural failure), bone quality (material properties), alignment (evidence of failure), collapse (quantified failure), and posterolateral elements (tension band integrity). Understanding these principles helps explain the scoring system and predict clinical behavior.
Classification and Interpretation
Stable Spine
Score: 0-6 points
Clinical Implication:
- No surgical consultation needed
- Treat oncologically (radiation, chemotherapy)
- Activity as tolerated
- No bracing required
Example Scenario:
- T5 (semi-rigid=1)
- Non-mechanical pain=1
- Lytic lesion=2
- Normal alignment=0
- No collapse=0
- No posterolateral involvement=0
- Total: 4/18 = Stable
Management focuses on tumor control with radiation. Monitor for progression.
Clinical Presentation and Assessment
Presenting Symptoms Suggesting Instability
Mechanical Back Pain:
- Worse with axial loading (standing, sitting)
- Relieved by recumbency
- Provoked by movement
- May have positional radicular symptoms
Progressive Deformity:
- Loss of height
- Increasing kyphosis
- Change in posture
Neurological Symptoms:
- May or may not be present
- Instability can exist without cord compression
- Cord compression can exist without instability
Clinical Assessment
History:
- Cancer diagnosis and treatment history
- Pain characteristics (mechanical vs oncological)
- Functional status (ECOG)
- Neurological symptoms
Examination:
- Spinal tenderness
- Deformity assessment
- Full neurological examination
- ASIA score if myelopathy
Differential Diagnosis of a Vertebral Lesion / Collapse
Before applying SINS, confirm the lesion is neoplastic and characterise the cause of any collapse, since SINS is only validated for tumour-related instability.
Differential Diagnosis of Vertebral Body Collapse
| Diagnosis | Key discriminating features | Pedicle involvement | Best test |
|---|---|---|---|
| Metastatic / myeloma collapse | Convex posterior border, epidural or paraspinal soft-tissue mass, multiple non-contiguous levels | Common (highly suggestive) | MRI with contrast; CT for bone |
| Osteoporotic insufficiency fracture | Intravertebral fluid/vacuum cleft, retropulsed fragment, band-like marrow oedema, T11-L2 site | Typically spared | MRI (STIR); DWI/ADC |
| Pyogenic / TB spondylodiscitis | Endplate erosion with disc involvement, paravertebral abscess, raised inflammatory markers | Variable | MRI with contrast; biopsy/cultures |
| Traumatic burst fracture | History of trauma, retropulsion, normal marrow signal away from fracture | May be fractured, not infiltrated | CT; MRI for PLC |
| Primary bone tumour (e.g. chordoma, plasmacytoma) | Solitary aggressive lesion, characteristic location, expansile | Often involved | MRI plus image-guided biopsy |
Imaging Requirements
CT Scan:
- Best for bone detail
- Lytic vs blastic assessment
- Vertebral body collapse measurement
- Posterior element involvement
MRI:
- Soft tissue assessment
- Epidural compression (Bilsky grade)
- Cord signal changes
- Whole spine for skip lesions
Do Not Rely on Single Modality
Both CT and MRI are needed for complete assessment. CT provides bone detail for SINS scoring. MRI provides soft tissue and neurological assessment. Do not calculate SINS from MRI alone if CT is available.
Imaging for SINS Assessment
CT for SINS Components
CT is the gold standard for bone assessment in SINS.
Location:
- Identify vertebral level
- Assess junctional proximity
Bone Lesion Quality:
- Lytic: Dark, lucent areas, bone destruction
- Blastic: Bright, sclerotic areas
- Mixed: Combination
Alignment:
- Sagittal reconstruction essential
- Compare to adjacent levels
- Measure subluxation in mm
VB Collapse:
- Measure anterior and middle column height
- Compare to adjacent levels
- Estimate percentage loss
Posterolateral Elements: Axial images are best for pedicle and facet involvement assessment. Document whether involvement is bilateral or unilateral.
Management Algorithm
Treatment Algorithm by SINS Category
Management of Stable Spine
Primary Treatment:
- Oncological (radiation therapy, systemic therapy)
- Activity as tolerated
- No bracing required
- No surgical consultation needed
Radiation Options:
- Conventional external beam (cEBRT)
- Stereotactic body radiation (SBRT)
- Based on tumor histology and extent
Monitoring:
- Clinical follow-up for symptoms
- Imaging if symptoms change
- Repeat SINS if progression suspected
Transition to Surgery: Consider surgery if SINS increases to 7 or higher on follow-up, if neurological deficits develop, or if radiation fails in radioresistant tumors.
Surgical Techniques
Percutaneous Stabilization:
- Cement augmentation (kyphoplasty/vertebroplasty)
- Percutaneous pedicle screws
- Minimal morbidity
- For selected indeterminate cases
Open Posterior Fusion:
- Standard for unstable spine
- Long segment instrumentation
- Cement-augmented screws in poor bone
- May include decompression
Combined Approach:
- Anterior corpectomy + posterior fusion
- For circumferential disease
- Vertebral body reconstruction
Cement Augmentation of Screws
In metastatic disease with poor bone quality, cement augmentation of pedicle screws significantly improves pullout strength. Consider PMMA augmentation for all screws in vertebrae adjacent to tumor involvement or in osteoporotic bone.
Surgical Technique
Stabilization for Unstable Spine (SINS 13+)
Posterior Instrumented Fusion:
- Standard approach for unstable metastatic spine
- Pedicle screw fixation minimum 2 levels above and below
- Consider 3 levels in junctional regions (T11-L1, L5-S1)
- Cement augmentation of screws in osteoporotic or tumor-involved bone
Construct Principles:
- Span the unstable segment completely
- Avoid ending at junctional zones
- Consider cross-links for rotational stability
- Assess adjacent level integrity
Surgical Options by SINS Category
| Procedure | SINS 7-12 | SINS 13-18 | Key Considerations |
|---|---|---|---|
| Cement augmentation only (VP/KP) | May be appropriate | Usually insufficient alone | For pain, not primary stabilization |
| Percutaneous pedicle screws | Good option | Acceptable if no decompression needed | Minimal morbidity, faster recovery |
| Open posterior fusion | Selected cases | Standard treatment | Allows decompression if needed |
| Combined anterior-posterior | Rarely needed | Circumferential disease | High morbidity, reserved for selected cases |
Complications and Pitfalls
SINS Scoring Pitfalls
Under-scoring:
- Missing posterolateral involvement
- Not recognizing junctional location
- Pain misclassified as non-mechanical
- Using MRI alone (less sensitive for bone)
Over-scoring:
- Attributing all pain to instability
- Pre-existing deformity counted as de novo
- Facet arthropathy mistaken for tumor
Clinical Pitfalls
Delayed Diagnosis:
- New back pain in cancer patient attributed to other causes
- Progressive deformity not recognized
- Imaging delayed
Delayed Treatment:
- Waiting for further progression
- Attempting conservative management for unstable spine
- Inadequate surgical stabilization
Surgical Complications
Intraoperative:
- Cord injury during positioning (unstable spine)
- Vascular injury
- Dural tear
Post-operative:
- Hardware failure
- Adjacent level fracture
- Wound complications
- Progression at other levels
Prevention Strategies
Early Recognition:
- Calculate SINS for all spine metastases
- Reassess with any symptom change
- Low threshold for surgical consultation
Adequate Treatment:
- Instrumentation of appropriate length
- Cement augmentation when indicated
- Address all unstable segments
Postoperative Care
Immediate Post-Operative Management
Day 0-1:
- ICU or HDU monitoring if high-risk patient
- Neurological checks every 2-4 hours
- DVT prophylaxis (mechanical and chemical)
- Pain management (multimodal approach)
- Drain management (if placed)
Day 1-3:
- Early mobilization with physiotherapy
- Sitting and standing as tolerated
- Wound inspection
- Bowel/bladder function assessment
Bracing
| Spine Level | Brace Type | Duration |
|---|---|---|
| Cervical | Rigid cervical collar or CTO | 6-12 weeks |
| Thoracic | TLSO | 6-12 weeks |
| Lumbar | LSO or TLSO | 6-12 weeks |
| Thoracolumbar | TLSO | 6-12 weeks |
Note: Bracing requirements depend on construct stability and bone quality. May be reduced with solid instrumentation and cement augmentation.
Outcomes
Surgical Outcomes for Spinal Metastases
Pain Relief:
- 70-90% achieve significant pain improvement
- Mechanical pain responds better than oncological pain
- Improvement often seen within days of stabilization
Neurological Outcomes:
- 60-80% with preoperative deficits show improvement
- Best results with incomplete deficits (ASIA B-D)
- Complete deficits (ASIA A) rarely improve
Ambulatory Status:
- 80-90% who are ambulatory pre-op maintain ambulation
- 50-70% of non-ambulatory patients regain ambulation
Outcomes by Intervention Type
| Outcome Measure | Stabilization Alone | Decompression + Stabilization | SBRT Alone (Stable SINS) |
|---|---|---|---|
| Pain improvement | 70-80% | 80-90% | 60-70% |
| Neurological improvement | Variable | 60-80% | 30-50% |
| Local tumor control | Requires adjuvant RT | Requires adjuvant RT | 80-90% at 1 year |
| Surgical morbidity | 10-15% | 15-25% | N/A |
Evidence Base
SINS Development (SOSG Consensus)
- Systematic review plus modified Delphi consensus of the Spine Oncology Study Group
- Six components defined: location, pain, bone lesion quality, alignment, vertebral body collapse, posterolateral involvement
- Three-tier classification: stable (0-6), potentially unstable (7-12), unstable (13-18)
- Demonstrated content validity to guide when surgical consultation is warranted
SINS Reliability and Validity
- 30 patient cases scored by SOSG members on two occasions at least 6 weeks apart
- Interobserver ICC 0.846 and intraobserver ICC 0.886 for total SINS score
- Sensitivity 95.7% and specificity 79.5% for potentially unstable or unstable lesions
- Kappa for predictive validity 0.712 against consensus gold standard
SINS Predicts Vertebral Fracture After SBRT
- Multi-institutional analysis of 252 patients and 410 spinal segments treated with SBRT
- Vertebral compression fracture in 14% (57/410); 65% occurred within the first 4 months
- Dose per fraction (highest risk with 24 Gy or more) was the strongest predictor
- Three SINS criteria - baseline fracture, lytic tumour and spinal deformity - independently predicted fracture
SINS 7-12 Outcomes: Surgery vs Radiotherapy
- International prospective cohort of 220 patients with potentially unstable (SINS 7-12) spinal metastases
- Surgery cohort (n=136) had a 3.0-point fall in pain score and 12.7-point rise in SOSGOQ2.0 by 12 weeks
- Radiotherapy-alone cohort (n=84) had smaller pain improvement that was not sustained beyond 3 months
- Surgical benefit in pain and quality of life was maintained to 52 weeks
NOMS Decision Framework
- Defines the Neurologic, Oncologic, Mechanical and Systemic (NOMS) decision framework
- SINS provides the Mechanical (M) sentinel decision point within NOMS
- Integrates Bilsky epidural grade, tumour radiosensitivity, stability and systemic status
- Directs choice between cEBRT, spine SBRT, separation surgery and instrumented stabilisation
Burden and Surgical Risk of Spinal Metastases
- Systematic review confirming the spinal column is the most common osseous site of metastatic spread
- Surgical site infection was the leading complication at 6.5% (135/2088)
- Neurological deterioration 3.3% and instrumentation failure 2.0%
- Overall re-operation rate 8.3%, most often for infection
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Calculate SINS for Metastatic Breast Cancer
"A 58-year-old woman with metastatic breast cancer presents with mechanical back pain at T12. CT shows a lytic lesion involving over 50% of the vertebral body with less than 50% collapse. There is no subluxation but new kyphosis is present. The left pedicle is involved."
Radioresistant Tumor with Indeterminate SINS
"A 65-year-old man with renal cell carcinoma presents with back pain at L3. MRI shows a metastasis with Bilsky 1c epidural compression. CT reveals a lytic lesion with no collapse, no alignment change, but bilateral pedicle involvement. Pain is mainly constant, not positional. SINS is calculated as 9."
Post-Radiation Fracture Risk
"A 52-year-old woman with metastatic lung cancer has an L1 lytic metastasis. SINS is 8 (indeterminate). The radiation oncologist asks your opinion about fracture risk if they proceed with SBRT."
Complete SINS Calculation from Imaging
"You are shown CT and MRI images of a 70-year-old man with prostate cancer. The images show a T7 vertebral body with mixed lytic and blastic metastasis. There is 60% collapse with retropulsion. Both pedicles are involved. The patient reports constant back pain not affected by position."
SPINAL INSTABILITY NEOPLASTIC SCORE (SINS)
Clinical summary
SINS Components (LPBAVP)
- •L = Location: Junctional=3, Mobile=2, Semi-rigid=1, Rigid=0
- •P = Pain: Mechanical=3, Non-mechanical=1, None=0
- •B = Bone lesion: Lytic=2, Mixed=1, Blastic=0
- •A = Alignment: Subluxation=4, Deformity=2, Normal=0
- •V = VB collapse: Over 50%=3, Under 50%=2, Over 50% involved=1, None=0
- •P = Posterolateral: Bilateral=3, Unilateral=1, None=0
Score Interpretation
- •0-6 = STABLE (no surgical consult)
- •7-12 = INDETERMINATE (surgical consult recommended)
- •13-18 = UNSTABLE (surgical stabilization required)
- •Score 13+ mandates surgery regardless of neurology
Junctional Zones (3 points)
- •Occipitocervical (C0-C2)
- •Cervicothoracic (C7-T2)
- •Thoracolumbar (T11-L1)
- •Lumbosacral (L5-S1)
Maximum Scoring Components
- •Alignment (subluxation) = 4 points (highest single component)
- •VB collapse over 50% = 3 points
- •Bilateral posterolateral = 3 points
- •Junctional location = 3 points
- •Mechanical pain = 3 points
SINS vs Bilsky
- •SINS = MECHANICAL instability assessment
- •Bilsky = NEUROLOGICAL (epidural) assessment
- •Both are independent and complementary
- •Can have high SINS + low Bilsky or vice versa
Clinical Pearls
- •Calculate SINS for ALL spine metastasis cases
- •Use CT for optimal SINS scoring (bone detail)
- •Indeterminate = clinical judgment + MDT
- •Lytic lesions have higher post-radiation fracture risk
MCQ Practice Points
Clinical Pearl
Q: What are the SINS score thresholds for stability classification? A: 0-6 = Stable (non-surgical), 7-12 = Indeterminate (requires surgical consultation), 13-18 = Unstable (surgical stabilization likely needed). The indeterminate range reflects cases where clinical judgment and imaging assessment are crucial.
Clinical Pearl
Q: What are the six components of the SINS score? A: Location (junctional zones score higher), Pain (mechanical worse than non-mechanical), Lesion type (lytic worse than blastic), Spinal alignment (subluxation/deformity), Vertebral body collapse (greater than 50% worse), and Posterolateral element involvement (bilateral worst).
Clinical Pearl
Q: Which spinal location scores highest on SINS and why? A: Junctional zones (occipital-C2, C7-T2, T11-L1, L5-S1) score 3 points compared to mobile spine (1 point) or rigid spine (0 points). Junctional zones experience the highest mechanical stress due to transition between mobile and rigid segments.
Clinical Pearl
Q: How does lesion type affect SINS scoring? A: Lytic lesions score 2 points (worst), blastic 0 points (best), and mixed 1 point. Lytic lesions weaken bone structure more than blastic lesions because they destroy load-bearing cortical and trabecular bone rather than adding (albeit abnormal) bone density.
Guidelines, Registries & Global Practice
Global Epidemiology
The vertebral column is the most common osseous site of metastatic spread, and spinal metastases are the dominant indication for SINS assessment worldwide. According to PubMed, a systematic review by Tarawneh et al. confirmed the spine as the leading bony metastatic site and quantified the morbidity of surgery for spinal metastases - surgical site infection 6.5%, neurological deterioration 3.3%, instrumentation failure 2.0% and an overall re-operation rate of 8.3% (Eur Spine J 2021). These figures frame the threshold for offering stabilisation in an unstable SINS.
Guideline and Society Positions
SINS is endorsed across major international guidance as the standard descriptor of neoplastic mechanical instability. There is broad convergence, with differences chiefly in emphasis.
International Guidance Incorporating SINS
| Body / Framework | Region | Position on SINS | Evidence basis |
|---|---|---|---|
| Spine Oncology Study Group (SOSG) | International | Originated and validated SINS; the reference standard for mechanical instability | Consensus plus validation (Fisher 2010, Fourney 2011) |
| NOMS framework (MSKCC) | International / USA | SINS is the Mechanical (M) sentinel decision point | Expert framework (Laufer 2013) |
| NICE (NG234, metastatic spinal cord compression) | UK | Recommends structured stability assessment and urgent spinal surgical referral for suspected instability | Guideline (GRADE-based) |
| BASS / British Orthopaedic Association (BOAST) | UK | SINS used within MDT pathways for metastatic spine disease | Standards / consensus |
| EANO / ESMO (CNS and bone metastasis guidance) | Europe | Endorse multidisciplinary stability assessment incorporating SINS | Guideline (expert consensus) |
| AO Spine Knowledge Forum Tumour | International | Develops and refines SINS and SOSGOQ outcome tools | Prospective cohort programmes |
Registry and Prospective Cohort Evidence
There is no dedicated implant registry for metastatic spine instrumentation comparable to arthroplasty registries. The strongest reproducible evidence comes from international prospective cohorts coordinated by AO Spine and the SOSG, including the prospective SINS 7-12 outcomes study (Versteeg et al.) and the multi-institutional SBRT fracture analysis (Sahgal et al.), both cited above.
Practice Variation
- Indeterminate band (7-12) drives most variation: thresholds for stabilisation, prophylactic cement augmentation and the choice between open and percutaneous fixation differ between units and between high- and lower-resource settings.
- Access to spine SBRT varies markedly worldwide; where SBRT is available, separation surgery for radioresistant tumours is favoured, whereas conventional external beam radiotherapy with broader surgical decompression predominates elsewhere.
- Australian context: SINS and the NOMS framework are standard within Australian tertiary spine-oncology multidisciplinary meetings, with increasing use of minimally invasive percutaneous pedicle screw fixation and cement augmentation. Smoking cessation support (Quitline 13 7848) is offered to optimise wound healing before instrumented fusion.
References
- Fisher CG, DiPaola CP, Ryken TC, et al. A novel classification system for spinal instability in neoplastic disease: an evidence-based approach and expert consensus from the Spine Oncology Study Group. Spine (Phila Pa 1976). 2010;35(22):E1221-9. PMID 20562730. DOI
- Fourney DR, Frangou EM, Ryken TC, et al. Spinal instability neoplastic score: an analysis of reliability and validity from the spine oncology study group. J Clin Oncol. 2011;29(22):3072-7. PMID 21709187. DOI
- Versteeg AL, Sahgal A, Rhines LD, et al. Health related quality of life outcomes following surgery and/or radiation for patients with potentially unstable spinal metastases. Spine J. 2021;21(3):492-499. PMID 33098985. DOI
- Sahgal A, Atenafu EG, Chao S, et al. Vertebral compression fracture after spine stereotactic body radiotherapy: a multi-institutional analysis with a focus on radiation dose and the spinal instability neoplastic score. J Clin Oncol. 2013;31(27):3426-31. PMID 23960179. DOI
- Laufer I, Rubin DG, Lis E, et al. The NOMS framework: approach to the treatment of spinal metastatic tumors. Oncologist. 2013;18(6):744-51. PMID 23709750. DOI
- Tarawneh AM, Pasku D, Quraishi NA. Surgical complications and re-operation rates in spinal metastases surgery: a systematic review. Eur Spine J. 2021;30(10):2791-2799. PMID 33184702. DOI
Evidence verified against PubMed. All cited DOIs link to the original peer-reviewed articles.