Posterior = Emergency | Airway Compromise | Mediastinal Structures at Risk
- Posterior dislocation is an EMERGENCY - can compress trachea, esophagus, great vessels
- SC joint is strongest joint in body - ligaments stronger than bone (physeal injury more common in under 25)
- Serendipity view (40 degree cephalic tilt) best plain film for diagnosis
- CT with contrast is gold standard - assess vascular compression
- Most dislocations are treated conservatively - recurrence well tolerated
- “Posterior dislocation: Dysphagia, dyspnea, venous congestion in arm/neck
- “Under 25 years - likely physeal injury (SH I/II), not true dislocation
- “Do NOT reduce posterior dislocation without thoracic surgery backup
- “Figure-of-8 reconstruction with hamstring/fascia lata for chronic instability
Posterior dislocation compresses mediastinum. Signs: dysphagia, dyspnea, venous engorgement, diminished pulses. Requires EMERGENT reduction. Have thoracic surgery on standby.
SC joint physis closes at age 25 - the last physis to close in the body. In patients under 25, most "dislocations" are actually Salter-Harris fractures through the medial clavicular physis.
40 degree cephalic tilt X-ray. Anterior dislocation: affected clavicle projects ABOVE opposite side. Posterior: projects BELOW. CT is definitive but serendipity view is exam favorite.
Most SC dislocations managed conservatively. Anterior: sling 6 weeks. Even with residual subluxation, function is usually excellent. Surgery reserved for persistent symptomatic instability.
- Findings
- Joint tender, stable
- Urgency
- Non-urgent
- Treatment
- Sling, ice, NSAIDs
- Findings
- Clavicle prominent anteriorly
- Urgency
- Non-urgent
- Treatment
- Closed reduction (optional), sling 6 weeks
- Findings
- Clavicle depressed, venous distension
- Urgency
- Urgent
- Treatment
- CT angiogram, closed reduction in OR, thoracic standby
- Findings
- Stridor, hypoxia, arm ischemia
- Urgency
- EMERGENCY
- Treatment
- Immediate reduction, airway management, thoracic surgery
- Findings
- Recurrent subluxation, pain with activity
- Urgency
- Elective
- Treatment
- Figure-of-8 reconstruction with graft
ABCDSC Joint Dislocation Direction
Hook:Anterior is common and cosmetic. Posterior is Perilous - watch for Problems!
CICASC Joint Ligaments
Hook:CICA stabilizes the SC joint - Costoclavicular is king!
Overview and Epidemiology
Incidence and Demographics:
- 3% of all shoulder girdle injuries
- Peak incidence: young adults (15-25 years) - sports, MVA
- Second peak: elderly (falls)
- Male predominance (2:1)
- Anterior dislocations 25 times more common than posterior
Mechanism of Injury:
- Direct blow to anteromedial clavicle (rare)
- Indirect force with lateral shoulder compression and arm forward
- Medial clavicle displaces anteriorly (lifts up and forward)
- Direct blow to anterolateral clavicle
- Lateral shoulder compression with arm back and down
- Medial clavicle displaces posteriorly into mediastinum
- High-energy mechanism (MVA, rugby tackle)
Age determines pathology: In patients under 25, the medial clavicular physis (last to close at age 22-25) is weaker than ligaments - expect physeal fracture (Salter-Harris I or II) rather than true dislocation.
Anatomy and Biomechanics
Bony Anatomy:
- SC joint is the only true articulation between upper limb and axial skeleton
- Saddle-type synovial joint (incongruous surfaces)
- Medial clavicular epiphysis is the LAST physis to close (age 22-25)
- Intra-articular disc (fibrocartilage) divides joint and acts as shock absorber
Key Stabilizers:
- Function
- PRIMARY stabilizer - limits elevation, anterior/posterior translation
- Clinical Significance
- Short and very strong - origin of physis injury concept
- Function
- Strongest capsular component - resists posterior displacement
- Clinical Significance
- Must be disrupted for posterior dislocation
- Function
- Weaker - resists anterior displacement
- Clinical Significance
- Disrupted in anterior dislocation
- Function
- Connects medial clavicles across sternum
- Clinical Significance
- Limits excessive clavicular depression
- Function
- Intra-articular shock absorber
- Clinical Significance
- Can tear with subluxation
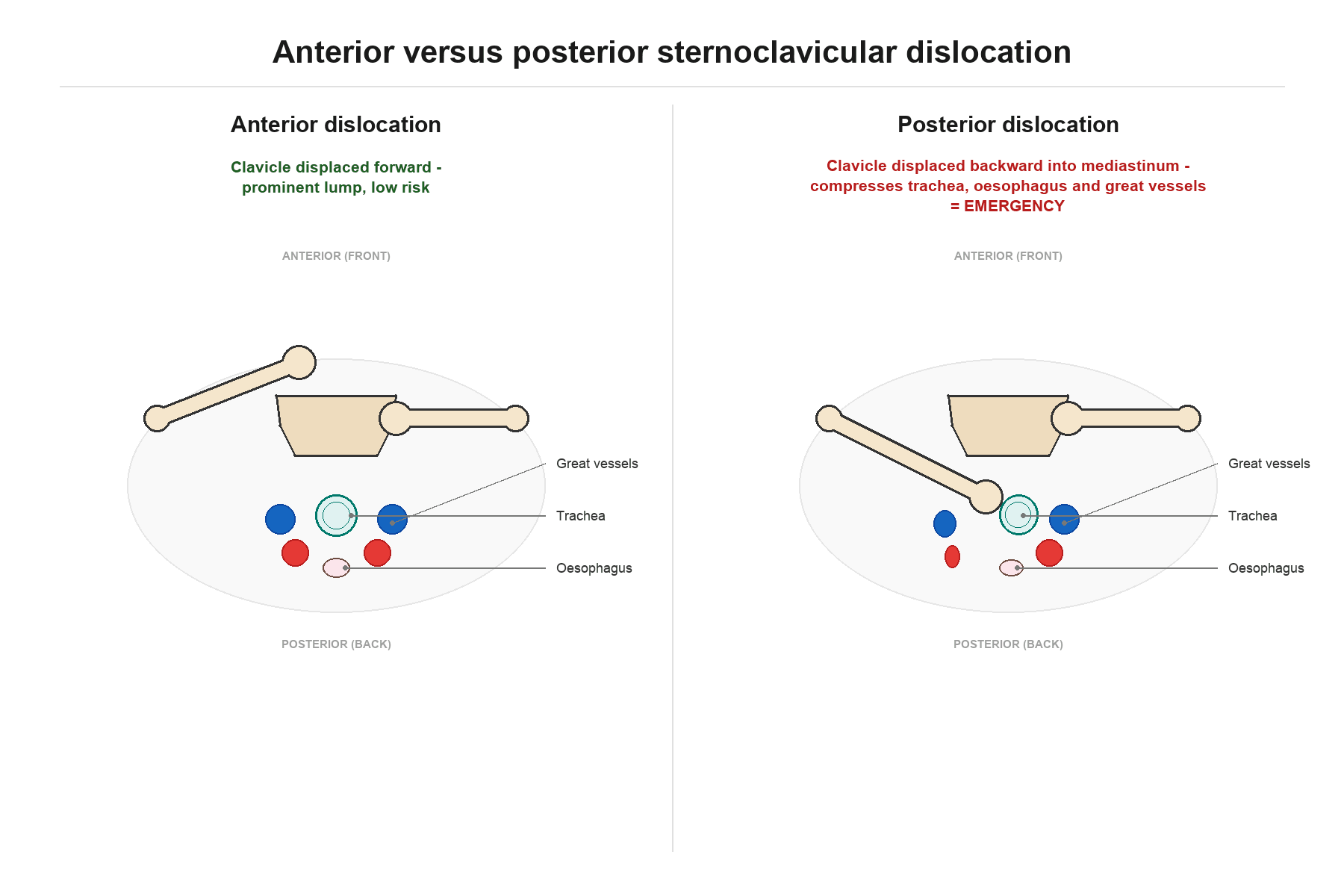
Posterior Mediastinal Relations:
The following critical structures lie only 1-2cm behind the SC joint:
- Trachea (directly posterior)
- Esophagus
- Subclavian artery and vein
- Carotid artery
- Internal jugular vein
- Innominate (brachiocephalic) artery and vein
- Brachial plexus
- Lung apex
Posterior dislocation can compress, lacerate, or thrombose any of these structures, making this a surgical emergency.
Biomechanics:
- The clavicle acts as a strut - transmits forces from upper limb to axial skeleton
- SC joint permits 35 degrees elevation, 35 degrees anterior/posterior movement, 50 degrees rotation
- True dislocation requires high energy to overcome very strong ligaments
Classification Systems
Most commonly used - based on direction and severity:
- Description
- Sprain
- Pathology
- Ligaments intact, microscopic tears
- Treatment
- Sling, ice, conservative
- Description
- Subluxation
- Pathology
- Capsule torn, costoclavicular intact
- Treatment
- Sling 4-6 weeks
- Description
- Anterior dislocation
- Pathology
- Complete ligament rupture, anterior displacement
- Treatment
- Usually conservative
- Description
- Posterior dislocation
- Pathology
- Complete ligament rupture, posterior displacement
- Treatment
- Urgent reduction required
Types I-III are generally managed conservatively with good outcomes. Type IV (posterior) is the only true emergency requiring urgent intervention.
Because the medial physis is the last to fuse (around age 22-25), the under-25 patient who looks "dislocated" usually has a Salter-Harris I or II separation: the epiphysis stays reduced against the manubrium (held by the intact sternoclavicular ligaments) while the metaphysis/clavicular shaft displaces anteriorly or posteriorly. This has two management implications. First, a posteriorly displaced physeal injury is just as dangerous as a true posterior dislocation — the displaced metaphysis can still compress the mediastinum, so it is reduced urgently with the same precautions (closed reduction, cardiothoracic cover, CT angiography). Second, because this is a fracture through bone in a patient with enormous remodelling potential, it heals reliably and rarely needs internal fixation — an anteriorly displaced or successfully reduced physeal injury is generally managed non-operatively, with (soft-tissue, never metal) fixation reserved for the irreducible posterior injury. This superior prognosis over a true ligamentous dislocation is why distinguishing the two on CT matters.
Clinical Assessment
History:
- High-energy mechanism (MVA, sports collision, fall onto shoulder)
- Direct blow vs indirect (lateral shoulder compression)
- Arm position at time of injury
- Symptoms suggesting vascular/airway compromise (dyspnea, dysphagia, arm swelling)
Physical Examination:
- Medial clavicle prominence (palpable anteriorly)
- Pain with arm movement, especially cross-body
- Swelling at SC joint
- Full shoulder ROM typically preserved
- Cosmetic deformity is main concern
- Medial clavicle less prominent or hollow (depressed posteriorly)
- Venous congestion in neck or ipsilateral arm
- Dysphagia (esophageal compression)
- Dyspnea, stridor (tracheal compression)
- Hoarseness (recurrent laryngeal nerve)
- Diminished upper limb pulses (subclavian compression)
- Brachial plexus symptoms (rare)
Examine every SC joint injury for:
- Stridor or respiratory distress
- Dysphagia or odynophagia
- Venous engorgement (neck, face, ipsilateral arm)
- Diminished or absent radial pulse
- Neurological deficit (brachial plexus)
- Supraclavicular hematoma
If any present - treat as posterior dislocation until proven otherwise!
Special Tests:
- Adson test: May assess subclavian artery compression
- Pulse comparison: Compare radial pulses bilaterally
- Venous distension: Look at jugular veins and arm veins
Differential Diagnosis:
- Distinguishing Features
- Skeletally immature patient, mechanism as for dislocation
- Key Discriminator
- CT/MRI shows physeal separation with metaphysis displaced; epiphysis stays reduced to manubrium
- Distinguishing Features
- Bony tenderness lateral to joint line, crepitus
- Key Discriminator
- Fracture line on CT distinct from joint; far more common than SCJD
- Distinguishing Features
- Older patient, gradual onset, no acute trauma
- Key Discriminator
- Osteophytes and joint-space loss on CT; symmetrical, activity-related ache
- Distinguishing Features
- Fever, warmth, raised inflammatory markers, IV drug use or immunocompromise
- Key Discriminator
- Joint aspirate and MRI; may extend to mediastinal abscess
- Distinguishing Features
- Painful bony swelling, palmoplantar pustulosis, bilateral
- Key Discriminator
- Sclerosis and hyperostosis on CT; bone scan 'bullhead' sign
- Distinguishing Features
- Young patient, atraumatic localised swelling
- Key Discriminator
- Fragmentation/sclerosis of sternal epiphysis, self-limiting
- Distinguishing Features
- Non-mechanical swelling, systemic symptoms
- Key Discriminator
- Cross-sectional imaging; not related to joint or trauma
Not all SC instability is traumatic. Atraumatic spontaneous subluxation is a distinct entity, typically in young patients (often women) with generalised ligamentous laxity (occasionally a connective-tissue disorder such as Ehlers-Danlos). The medial clavicle subluxes anteriorly on arm elevation and reduces when the arm is lowered, is frequently bilateral, and is usually painless or only mildly symptomatic. The cardinal rule mirrors atraumatic/voluntary shoulder instability: management is non-operative (reassurance, activity modification, and physiotherapy for scapular and periscapular control), and surgical stabilisation should be avoided — it has poor results and high recurrence, and the SC joint's mediastinal-hardware hazards make a failed reconstruction especially undesirable. Distinguish it from a fixed traumatic dislocation, which does not spontaneously reduce.
Investigations
- Findings
- Often inconclusive - structures overlap
- Indication
- Initial screening only
- Findings
- Anterior: clavicle UP; Posterior: clavicle DOWN
- Indication
- Classic exam view - good for direction
- Findings
- Gold standard for fracture/dislocation assessment
- Indication
- All suspected dislocations
- Findings
- Vascular injury assessment
- Indication
- All posterior dislocations
- Findings
- Soft tissue, physeal injury in young patients
- Indication
- Subacute/chronic cases, physeal injury
Serendipity view technique: Patient supine, X-ray beam angled 40 degrees cephalad centered on sternum. Compare both SC joints on same film. Anterior dislocation: affected clavicle projects ABOVE the normal side. Posterior: projects BELOW. This is a classic exam question!
CT Findings:
- Definitive for direction of displacement
- Identifies associated fractures
- With contrast - assesses vascular compression/injury
All posterior SC dislocations require CT angiography to assess for vascular compression or injury. Even after successful reduction, delayed vascular complications can occur.
Management Algorithm
Conservative Management:
Treatment Protocol
- Ice, sling for comfort
- NSAIDs for pain and inflammation
- Avoid aggravating activities
- Protected range of motion
- Wean from sling as pain allows
- Progressive ROM exercises
- Gentle strengthening
- Avoid contact sports/heavy lifting
- Full ROM should be achieved
- Sport-specific rehabilitation
- Gradual return to full activity
Prognosis: Excellent - near 100% return to full function
Surgical Technique
- Chronic symptomatic anterior or posterior instability
- Failed conservative management
- Recurrent dislocation affecting function
- Active infection
- SC joint arthritis (consider resection instead)
- Positioning and Approach - Supine with bump under shoulders, transverse skin incision over SC joint, protect supraclavicular nerves, expose SC joint and medial clavicle
- Tunnel Preparation - Create 5-6mm tunnel through medial clavicle (anterior to posterior), create 5-6mm tunnel through manubrium or 1st rib, protect mediastinal structures with retraction and finger guard
- Graft Passage - Pass doubled graft through clavicular tunnel, cross graft in figure-of-8 pattern, pass through sternal/rib tunnel, return to clavicular tunnel
- Tensioning and Fixation - Reduce SC joint anatomically, tension graft with arm in neutral position, secure graft with interference screw or suture over bone bridge, confirm stability with stress
This technique provides stable reconstruction without metal hardware.
BUMPReduction Technique
Hook:BUMP the shoulders back and pull the clavicle forward!
Complications
- Anterior Dislocation
- Rare
- Posterior Dislocation
- Common - subclavian/innominate compression or laceration
- Anterior Dislocation
- No
- Posterior Dislocation
- Yes - tracheal compression can be fatal
- Anterior Dislocation
- No
- Posterior Dislocation
- Yes - esophageal compression
- Anterior Dislocation
- No
- Posterior Dislocation
- Risk with open reduction
- Anterior Dislocation
- Common (usually cosmetic)
- Posterior Dislocation
- Rare if adequately reduced
- Anterior Dislocation
- 5-10%
- Posterior Dislocation
- 5-10%
- Anterior Dislocation
- If metal used - can be fatal
- Posterior Dislocation
- If metal used - can be fatal
Multiple case reports document fatal migration of pins, screws, and plates from the SC joint into:
- Heart (cardiac tamponade)
- Aorta (hemorrhage)
- Pulmonary vessels
- Subclavian vessels
Migration can occur months to years after surgery. Metal hardware is absolutely contraindicated at the SC joint.
- Use only soft tissue reconstruction
- CT angiogram for all posterior dislocations
- Thoracic surgery standby for reduction
- Careful tunnel placement during reconstruction
- Vascular injury: Immediate thoracic/vascular surgery
- Chronic instability: Figure-of-8 reconstruction
- Arthritis: Medial clavicle resection (rare)
STAVEPosterior SC Complications
Hook:Posterior dislocation can STAVE in the mediastinum - structures are compressed!
Postoperative Care
After Closed Reduction:
- Figure-of-8 brace or sling for 6 weeks
- NSAIDs for pain
- Ice to reduce swelling
- Serial X-rays to confirm maintained reduction
- Progressive ROM after immobilization
After Figure-of-8 Reconstruction:
Rehabilitation Protocol
- Sling immobilization
- Elbow, wrist, hand ROM maintained
- Pendulum exercises at 2 weeks
- No lifting, pushing, or pulling
- Wean from sling
- Active-assisted shoulder ROM
- Gentle isometric strengthening
- No resistance exercises
- Progressive resistance exercises
- Full ROM should be achieved
- Return to light activities
- Sport-specific training
- Gradual return to contact (if applicable)
- Functional testing before clearance
Outcomes and Prognosis
Natural History:
- Most SC injuries have excellent outcomes with conservative treatment
- Even with residual deformity, function is typically normal
- Posterior dislocations require intervention but outcomes good if promptly treated
- Treatment
- Conservative
- Good/Excellent Outcome
- 95-100%
- Return to Full Activity
- 4-6 weeks
- Treatment
- Conservative
- Good/Excellent Outcome
- 85-95%
- Return to Full Activity
- 6-12 weeks
- Treatment
- Closed reduction
- Good/Excellent Outcome
- 80-90%
- Return to Full Activity
- 6-12 weeks
- Treatment
- Figure-of-8 reconstruction
- Good/Excellent Outcome
- 75-85%
- Return to Full Activity
- 4-6 months
Prognostic Factors:
- Time to treatment (especially posterior)
- Age (younger patients do better)
- Associated injuries
- Compliance with rehabilitation
Guidelines, Registries & Global Practice
Global Epidemiology:
- Figure
- Less than 3%
- Source
- Groh & Wirth, JAAOS 2011 (PMID 21205762)
- Figure
- 0.6%
- Source
- Bakir et al, Eur J Trauma Emerg Surg 2020 (PMID 31960070)
- Figure
- Posterior far less common than anterior
- Source
- Groh & Wirth, JAAOS 2011
- Figure
- Bimodal peaks at approximately 20 and 50 years, male predominance
- Source
- Bakir et al 2020
- Figure
- Most 'dislocations' are medial physeal injuries
- Source
- Webb & Suchey 1985; Groh & Wirth 2011
Guidance Across Major Bodies:
There is no dedicated AAOS, NICE or BOAST guideline specific to SC joint dislocation; this is a rare injury where practice is driven by case series, systematic reviews and trauma-system principles rather than formal society guidelines. The consensus positions below are drawn from the indexed evidence base.
- Prevailing Position
- Treat as an emergency; attempt prompt closed reduction, ideally within 10 days
- Evidence Level / Source
- Level IV - Groh et al, JSES 2011 (PMID 20579908)
- Prevailing Position
- Strongly recommended to be available; evidence does not mandate physical presence
- Evidence Level / Source
- Level IV meta-analysis - Sernandez & Riehl 2019 (PMID 30844956)
- Prevailing Position
- Largely non-operative; accept residual prominence
- Evidence Level / Source
- Level IV - Sernandez & Riehl 2019
- Prevailing Position
- Soft-tissue (tendon-graft) reconstruction over metal fixation
- Evidence Level / Source
- Level IV/V - Spencer & Kuhn 2004 (PMID 14711951); Kendal et al 2018 (PMID 30399119)
- Prevailing Position
- Contraindicated - risk of fatal migration
- Evidence Level / Source
- Level V - Janssens de Varebeke 1993 (PMID 8140842)
Registry and Practice Variation:
- No national joint registry (NJR, AJRR, AOANJRR, SHAR) captures SC joint dislocation as a tracked procedure, reflecting its rarity and the absence of an implanted prosthesis; the best population-level data come from national administrative datasets such as the German big-data analysis above.
- Practice variation is driven chiefly by access to cross-sectional imaging and cardiothoracic surgery rather than by regional guideline differences: in well-resourced settings CT angiography and on-site thoracic cover are standard before reducing a posterior dislocation, whereas in limited-resource settings prompt closed reduction may proceed with whatever surgical backup is available, accepting higher risk.
- The single global constant across all settings is the absolute avoidance of trans-articular metalwork.
- Complete neurovascular examination before and after any intervention (document pulses, sensation, motor function)
- Imaging confirming direction of dislocation before reduction
- Documented thoracic surgery consultation for posterior dislocations
- Informed consent discussing hardware migration risk if any fixation planned
- CT post-reduction to confirm anatomic position
- Delayed diagnosis of posterior dislocation leading to vascular injury
- Vascular injury during reduction without surgical backup
- Hardware migration causing cardiac/vascular injury
- Inadequate documentation of neurovascular status
Viva Scenarios
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old male presents to the emergency department after a motorcycle accident. He complains of difficulty swallowing and shortness of breath. You note venous engorgement in his right neck and arm. The right medial clavicle appears less prominent than the left.”
“A 22-year-old rugby player presents with a prominent lump over his right sternoclavicular joint following a tackle. He has full range of motion of the shoulder but pain with overhead activities. Plain X-rays are inconclusive. What is your assessment and management?”
“A 35-year-old female office worker presents with chronic pain at her right SC joint. She had an anterior dislocation 2 years ago treated conservatively. Now she has a prominent medial clavicle that subluxes with arm elevation and causes pain affecting her work. She requests surgical treatment.”
MCQ Practice Points
Q: What is the last epiphyseal plate to close in the human body?
A: The medial clavicular physis closes at age 22-25 years. This is clinically important because in patients under 25, SC joint injuries often represent Salter-Harris physeal fractures rather than true ligamentous dislocations, with better healing potential.
Q: On a serendipity view, how does an anterior SC dislocation appear compared to the contralateral normal side?
A: The affected medial clavicle projects ABOVE the normal side in anterior dislocation. In posterior dislocation, it projects BELOW. The serendipity view is obtained with a 40-degree cephalic tilt X-ray beam centered on the sternum.
Q: A patient with a posterior SC dislocation presents with stridor and dysphagia. What mediastinal structures are being compressed?
A: Trachea (causing stridor) and esophagus (causing dysphagia). Other structures at risk include the subclavian vessels, innominate artery/vein, carotid artery, internal jugular vein, and brachial plexus. This constitutes a surgical emergency.
Q: What is the primary concern if metal hardware (plates/screws) is used for SC joint fixation?
A: Migration into the mediastinum. Hardware can migrate into the heart, great vessels, or lungs, causing fatal complications including cardiac tamponade and hemorrhage. Only soft tissue reconstruction (figure-of-8 with tendon graft) should be used for SC joint stabilization.
Q: Which ligament is the primary stabilizer of the SC joint?
A: The costoclavicular ligament is the primary stabilizer. It runs from the first rib/costal cartilage to the inferior medial clavicle and limits elevation, anterior translation, and posterior translation of the clavicle.
Q: In the Rockwood classification of SC joint injuries, which type requires emergent treatment?
A: Type IV (posterior dislocation) requires urgent/emergent reduction due to risk of mediastinal structure compression. Types I-III (sprains and anterior dislocation) are generally managed conservatively.
Key Statistics
- 3% of all shoulder girdle injuries
- Anterior : Posterior ratio = 25:1
- Medial clavicular physis closes at 22-25 years (LAST physis)
- Under 25 = likely physeal injury, not true dislocation
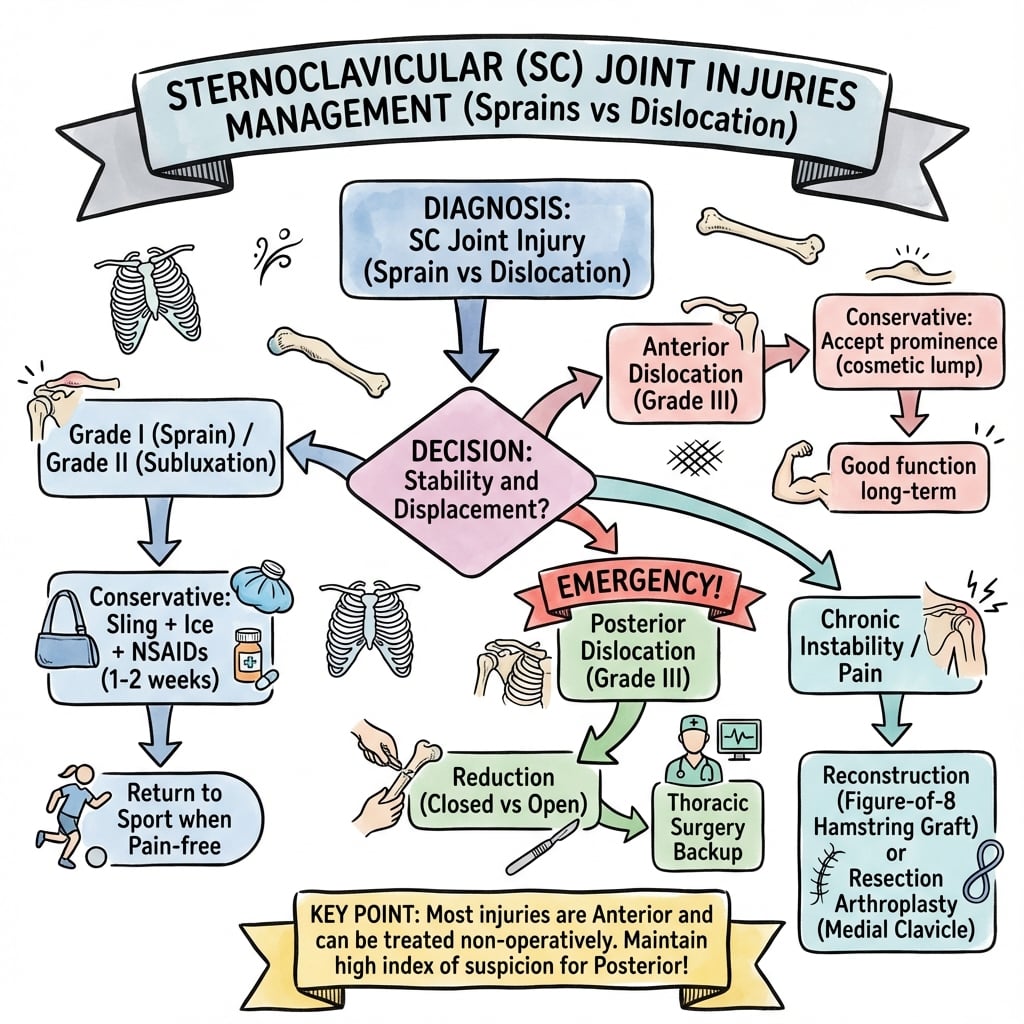
Rockwood Classification
- Type I: Sprain - ligaments intact - conservative
- Type II: Subluxation - capsule torn - conservative
- Type III: Anterior dislocation - usually conservative
- Type IV: Posterior dislocation = EMERGENCY
Posterior Dislocation Signs (STAVE)
- Subclavian vessel compression
- Trachea compression (stridor/dyspnea)
- Artery (carotid) compression
- Vein (jugular) engorgement
- Esophagus compression (dysphagia)
Management Principles
- Anterior: Conservative - sling 6 weeks, accept prominence
- Posterior: URGENT reduction - thoracic surgery standby
- Chronic: Figure-of-8 reconstruction with tendon graft
- NEVER use metal hardware - migration into mediastinum
Key Imaging
- Serendipity view: 40 degree cephalic tilt
- Anterior = clavicle projects ABOVE normal
- Posterior = clavicle projects BELOW normal
- CT/CTA mandatory for posterior (assess vascular)
Must Know for Exam
- Posterior SC dislocation is a surgical emergency
- Thoracic surgery backup mandatory for reduction
- No metal hardware at SC joint (fatal migration)
- Costoclavicular ligament is primary stabilizer
- Last physis to close = medial clavicle (22-25y)
Evidence Base
Medial Clavicular Physeal Closure Age (defining anatomical reference)
- Known-age skeletal study of 605 males and 254 females aged 11-40 years; staged epiphyseal union of the medial clavicle (and anterior iliac crest)
- The medial clavicular epiphysis is among the last to unite, with partial-to-complete union spanning the late teens into the mid-twenties
- Broader age ranges for each union stage than earlier studies; male and female ranges similar or differing by only 1-2 years
- Underpins the clinical teaching that the medial clavicular physis is the last in the body to fuse
Closed Reduction of Traumatic Posterior SC Dislocation (largest single-centre series)
- Twenty-one patients with traumatic posterior SC injury; all underwent a trial of closed reduction, definitive in 8 (38%)
- Closed reduction was significantly more likely to succeed when performed within 10 days of injury
- The remaining 13 patients had open reduction and SC reconstruction; 18 of 21 overall rated good or excellent on the UCLA scale
- Successful early closed reduction obviated the risks of surgery; failed reductions did well with costoclavicular ligament reconstruction
Epidemiology of Medial Clavicle and SC Joint Injuries (nationwide data)
- Nationwide German registry analysis (ICD-10) identified 14,264 medial clavicle injuries between 2012 and 2014
- SC joint dislocation accounted for only 0.6% of clavicle-related shoulder-girdle injuries (medial clavicle fracture 11.6%) - confirming these are genuinely rare
- Bimodal age distribution with peaks around 20 and 50 years, with overall male predominance
- Females showed proportionally more injuries beyond 70 years; no significant sex difference under 16 years
Natural History and Indications - Systematic Review and Meta-analysis
- Meta-analysis of 92 acute (under 3 weeks) SC dislocations in patients 16 years and older addressing untreated outcome and reduction indications
- Anterior dislocations frequently do well managed non-operatively even when reduction is not maintained
- For posterior dislocations the evidence supports attempting closed reduction acutely, with open treatment when closed reduction fails
- The literature did not demonstrate that a cardiothoracic surgeon must be physically present, although availability remains widely recommended given catastrophic potential complications
Biomechanics of SC Joint Reconstruction (defining graft-construct study)
- Cadaveric biomechanical comparison (36 specimens) of intramedullary ligament, subclavius tendon, and figure-of-eight semitendinosus reconstructions
- Figure-of-eight semitendinosus graft through clavicular and manubrial tunnels was significantly stiffer than the other two constructs in both directions
- Peak load to failure for the semitendinosus figure-of-eight was approximately 230 N anteriorly and 241 N posteriorly, roughly three times the alternatives
- Provided the biomechanical rationale for figure-of-eight tendon-graft reconstruction now used clinically
Fatal Hardware Migration from the SC Joint (sentinel case + literature review)
- Spontaneous migration of a broken Kirschner pin from the right SC joint into the anterior mediastinum, perforating the pericardium and main pulmonary artery and causing cardiac tamponade
- Literature review emphasised the high risk of migration when pins or wires are used about the shoulder girdle, sometimes life-threatening
- Recommends mandatory removal of all metal once united, especially if broken or with local bone resorption
- Highlights the medicolegal consequences of neglected follow-up of such implants
Surgical Management of Posterior Dislocation - Systematic Review
- PRISMA systematic review of 40 studies (108 cases) of traumatic posterior SC dislocation managed surgically
- Favourable outcomes across all five stabilisation categories; overall complication rate 16% including 4 cases of recurrent instability
- Tendon-graft ligament reconstruction had the lowest recurrent instability and complication rates
- Open reduction and internal fixation required a second operation for implant removal in 80% of cases