SC Joint Injury | Anterior vs Posterior | Mediastinal Emergency | Reconstruction Risk
- Sternoclavicular joint is a saddle-type synovial joint with the least bony stability of any major joint
- Posterior dislocation is a surgical emergency - mediastinal compromise of vessels, trachea, oesophagus
- CT scan (with vascular contrast) is the investigation of choice - plain films miss up to 50 percent
- Anterior dislocations: most managed non-operatively with sling and analgesia
- Reconstruction risks: instability, recurrent dislocation, implant-related complications, medial clavicle resection concerns
- “Posterior SC dislocation = trauma call, not clinic referral
- “CT with IV contrast to define both bony anatomy and mediastinal structure involvement
- “Anterior SC dislocations are common and stable - do not reduce operatively unless chronic instability
- “Atraumatic SC subluxation in young women is usually multidirectional laxity, not trauma
Posterior dislocation can compress mediastinal structures including brachiocephalic vessels, internal jugular vein, common carotid, subclavian vessels, trachea, oesophagus, vagus and phrenic nerves. Dyspnoea, dysphagia, stridor, hoarseness, or arm ischaemia mandates urgent reduction.
Plain radiographs miss up to 50 percent of SC dislocations. CT (ideally with IV contrast) demonstrates direction, displacement, and relationship to mediastinal structures. Serendipity view is obsolete.
SC joint reconstruction is high-risk: recurrent instability, implant migration, neurovascular injury, prominent hardware, medial clavicle resection complications, and infection. Reserve for symptomatic chronic instability.
Anterior dislocations are common and generally stable after closed reduction. Operative stabilisation has high failure and complication rates - non-operative management is the default.
- Anterior SC Dislocation
- Anterior 3:1 more common
- Posterior SC Dislocation
- Posterior 1:3 ratio, much less common
- Anterior SC Dislocation
- Rare, not an emergency
- Posterior SC Dislocation
- Common - vessels, trachea, oesophagus at risk
- Anterior SC Dislocation
- Sling, analgesia, early mobilisation
- Posterior SC Dislocation
- Urgent closed reduction under GA with thoracic backup
- Anterior SC Dislocation
- Stable after reduction, even if re-subluxes cosmetically
- Posterior SC Dislocation
- Treat as trauma emergency, do not delay CT
MEDIASTINUMPosterior SC Dislocation Warning Signs
Hook:MEDIASTINUM signs warn of posterior SC dislocation compressing vital structures.
FORCEFULAnterior SC Dislocation Mechanism
Hook:FORCEFUL injury with a forward vector gives an anterior SC dislocation.
STERNALSC Joint Anatomy and Stability
Hook:STERNAL anatomy: ligamentous stability is the only thing keeping the SC joint reduced.
Overview and Epidemiology
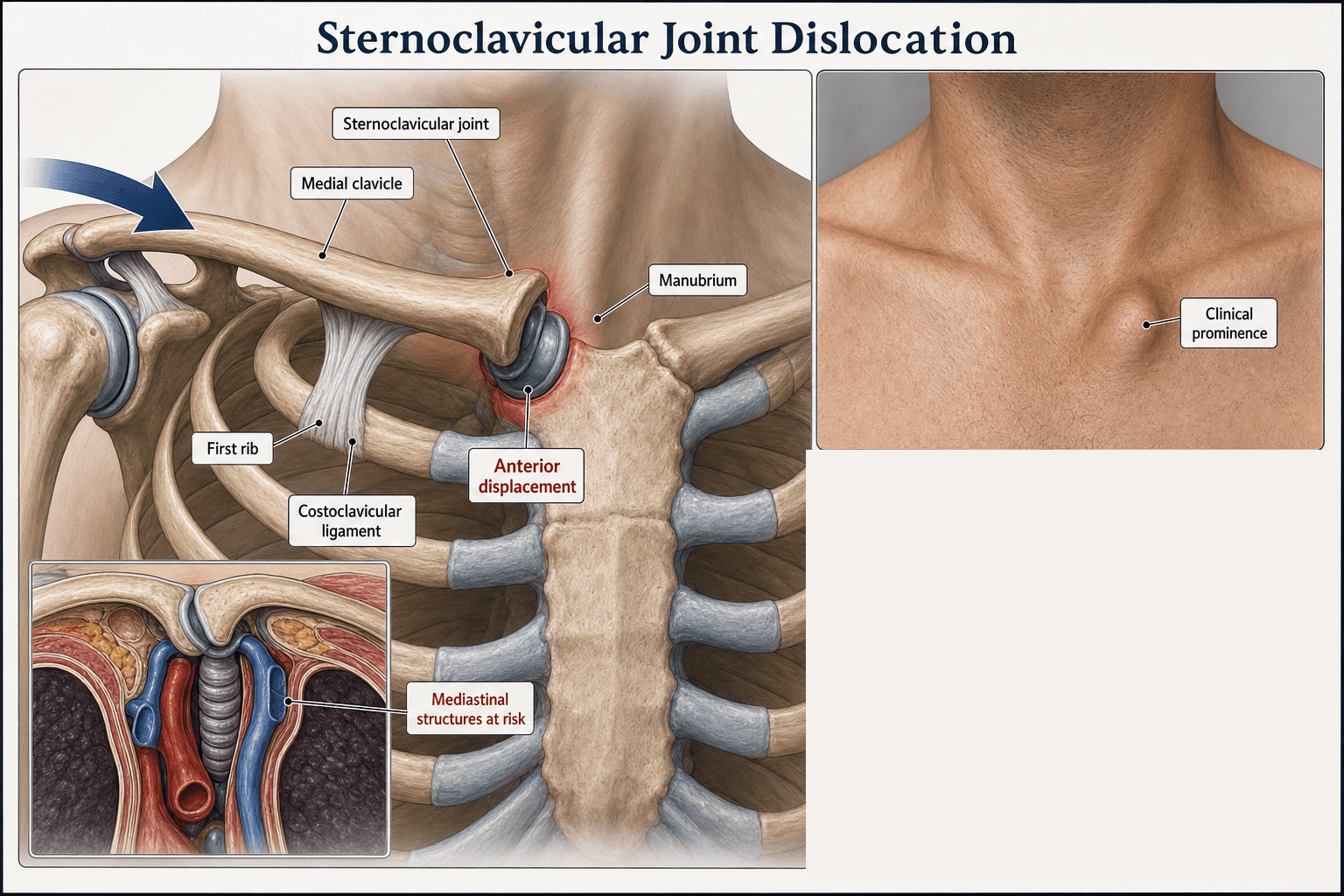
The sternoclavicular joint is the only true articulation between the upper limb and the axial skeleton. It is the least stable major joint in the body because more than 50 percent of the medial clavicle articular surface sits outside the manubrial socket, leaving stability entirely ligamentous. Posterior dislocations are rare but life-threatening because the medial clavicle can directly compress the brachiocephalic vein, common carotid, subclavian vessels, trachea, oesophagus, and vagus/phrenic nerves.
- Indirect high-energy trauma: Force applied to the lateral shoulder (most common)
- Road traffic collisions: Restrained driver/passenger, lateral compression
- Contact and collision sport: Direct blow to medial clavicle or shoulder
- Fall onto outstretched hand: Force transmitted medially through clavicle
- Atraumatic subluxation: Multidirectional laxity in young patients
- Anterior: Cosmetic prominence, mild pain, often well-tolerated
- Posterior: Mediastinal emergency - dyspnoea, dysphagia, vascular compromise
- Chronic instability: Functional limitation in overhead athletes
- Physeal injury: In adolescents, medial clavicle physeal separation mimics dislocation
Pathophysiology
The SC joint is a saddle-type (sellar) synovial joint with a complete intra-articular disc of fibrocartilage. The medial clavicle is larger than the manubrial fossa, with only a small portion articulating. Stability depends on the anterior and posterior capsular ligaments (the posterior capsule is the strongest single restraint), the interclavicular ligament (between both clavicles across the suprasternal notch), the costoclavicular (rhomboid) ligament (between clavicle and first rib), and the intra-articular disc. The costoclavicular ligament is the primary restraint to medial-lateral displacement and is the key structure to reconstruct in chronic instability.
- Origin-Insertion
- Anterior manubrium to anterior clavicle
- Primary Function
- Resists posterior displacement
- When Injured
- First torn in anterior dislocation
- Origin-Insertion
- Posterior manubrium to posterior clavicle
- Primary Function
- Strongest restraint to anterior displacement
- When Injured
- Failed in posterior dislocation
- Origin-Insertion
- First rib to clavicle (medial)
- Primary Function
- Resists medial-lateral and superior-inferior
- When Injured
- Key to reconstruction in chronic instability
- Origin-Insertion
- Clavicle to clavicle across suprasternal notch
- Primary Function
- Resists superior displacement
- When Injured
- Torn in complete dislocations
- Origin-Insertion
- First rib to clavicle through joint
- Primary Function
- Shock absorber, force transmission
- When Injured
- Often torn in dislocation, may block reduction
Indirect force to lateral shoulder drives medial clavicle
Clavicle pivots at costoclavicular ligament
Anterior force vector (most common) = anterior dislocation, posterior capsule intact
Posterior force vector (less common, high-energy) = posterior dislocation, posterior capsule torn
Direct blow to medial clavicle can drive it posteriorly
Posterior to medial clavicle: brachiocephalic vein, common carotid, subclavian artery and vein
Deeper plane: trachea, oesophagus, vagus nerve, phrenic nerve, thoracic duct (left)
Physeal injury in adolescents often mimics posterior dislocation on imaging - real structure is medial clavicular physis (last to fuse at 23-25 years)
Classification and Types
Classification by Direction of Displacement
- Frequency
- Most common (3:1 vs posterior)
- Mechanism
- Indirect force, anterior vector
- Urgency
- Usually non-operative
- Frequency
- Less common
- Mechanism
- Indirect high-energy or direct posterior blow
- Urgency
- Emergency - mediastinal risk
- Frequency
- Common in young hypermobile patients
- Mechanism
- Spontaneous or with minor movement
- Urgency
- Reassurance, physiotherapy
Posterior dislocations are surgical emergencies. Always image with CT to confirm direction and exclude mediastinal compromise.
Direction and timing are only two axes; examiners also expect the severity grade of the ligamentous injury, because it dictates whether the joint is stable:
- Grade I - sprain: the capsular ligaments are stretched but intact; the joint is stable and minimally displaced. Tenderness and mild swelling only; treated with a sling and analgesia.
- Grade II - subluxation: partial capsular/ligament disruption with the costoclavicular ligament still intact; the joint subluxes but is not frankly dislocated and is partially stable; sling, analgesia, and avoidance of provocative positions.
- Grade III - dislocation: complete disruption of the capsular ligaments (and usually the costoclavicular ligament); the joint is frankly anteriorly or posteriorly dislocated and unstable - this is where the anterior-vs-posterior distinction and the mediastinal emergency apply.
Key point: a Grade I-II injury does NOT need reduction, only symptomatic care; the dramatic management decisions (urgent CT, theatre reduction, reconstruction) belong to the Grade III dislocation. Do not over-treat a sprain or subluxation.
Clinical Assessment
- Mechanism: High-energy trauma, contact sport, MVC, fall
- Posterior red flags: Dyspnoea, stridor, dysphagia, voice change, arm paraesthesia or ischaemia
- Prior episodes: Recurrent subluxation suggests multidirectional laxity
- Age: Under 25 years - consider physeal injury rather than true dislocation
- Inspect: Visible asymmetry, swelling, ecchymosis, skin tethering
- Palpate: Medial clavicle position relative to suprasternal notch and contralateral side
- Posterior signs: Neck vein engorgement, tracheal deviation, pulses, neuro exam
- Provocative test: Arm elevation in extension stresses the joint
Always assess and document in any SC joint injury:
- Respiratory distress, stridor, voice change
- Neck vein distension (SVC or brachiocephalic vein compression)
- Subclavian and axillary pulses, capillary refill
- Brachial plexus sensation and motor (C5-T1)
- Swallowing difficulty (oesophageal impingement)
- Phrenic nerve (diaphragm screening with ultrasound or fluoroscopy if intubated)
- Vagus (recurrent laryngeal - voice change)
A posterior SC dislocation with any of these signs mandates urgent reduction with cardiothoracic or vascular surgery on standby.
- Anterior SC Dislocation
- Prominent medial clavicle, often visible lump
- Posterior SC Dislocation
- Depression or sulcus at SC joint
- Anterior SC Dislocation
- Rare
- Posterior SC Dislocation
- Common - dyspnoea, stridor, dysphagia, venous congestion
- Anterior SC Dislocation
- Erythema, swelling, possible skin tenting
- Posterior SC Dislocation
- May have skin dimple, cyanosis, surgical emphysema
- Anterior SC Dislocation
- Painful but usually full
- Posterior SC Dislocation
- Markedly limited by pain and mediastinal symptoms
- Direction of Deformity
- Anterior prominence
- Discriminating Finding
- Lateral compression reproduces pain, palpable step
- Key Test / Imaging
- CT confirms anterior position
- Direction of Deformity
- Loss of medial clavicle contour
- Discriminating Finding
- Mediastinal signs, asymmetric pulses
- Key Test / Imaging
- CT with IV contrast to define mediastinal relationship
- Direction of Deformity
- Anterior or posterior
- Discriminating Finding
- Adolescent (under 25), mechanism matches trauma
- Key Test / Imaging
- CT shows physeal line; MRI can confirm physis
- Direction of Deformity
- Variable, often bilateral
- Discriminating Finding
- Multidirectional laxity, no high-energy event
- Key Test / Imaging
- Clinical; imaging normal or minor asymmetry
- Direction of Deformity
- No acute deformity
- Discriminating Finding
- Insidious pain, crepitus, older patient
- Key Test / Imaging
- X-ray and CT show joint space narrowing, osteophytes
- Direction of Deformity
- No acute deformity
- Discriminating Finding
- Middle-aged women, pain without laxity
- Key Test / Imaging
- X-ray: sclerosis of medial clavicle
- Direction of Deformity
- No acute deformity
- Discriminating Finding
- Insidious medial clavicle pain
- Key Test / Imaging
- MRI shows AVN changes
- Direction of Deformity
- Swelling, warmth, fluctuance
- Discriminating Finding
- Fever, IVDU, immunocompromise, recent infection
- Key Test / Imaging
- Bloods, joint aspiration, MRI
A swollen, warm, tender SC joint is not always traumatic - septic arthritis of the SC joint is a distinct, examinable entity that is easily missed:
- Host risk factors: intravenous drug use (classic), diabetes, immunosuppression, chronic kidney disease, an indwelling central line/catheter, and a distant source of bacteraemia. It can also occur with no obvious risk factor.
- Organisms: Staphylococcus aureus is commonest overall; Pseudomonas aeruginosa is classically associated with intravenous drug use.
- Why it is dangerous: the SC joint sits over the mediastinum, so untreated infection can spread to a chest-wall abscess, sternoclavicular osteomyelitis, and mediastinitis - a potentially life-threatening complication.
- Diagnosis: raised inflammatory markers, blood cultures, CT or MRI (to define abscess/osteomyelitis/retrosternal extension) and joint aspiration for Gram stain and culture.
- Management: targeted IV antibiotics for early disease, but established septic arthritis with abscess or osteomyelitis usually needs surgical debridement or en bloc resection of the SC joint (medial clavicle and manubrial portion), which is generally well tolerated functionally.
Exam point: in an IV drug user or immunocompromised patient with a hot, painful medial clavicle and fever, think SC septic arthritis with possible mediastinal extension - image and aspirate, do not treat as a sprain.
Atraumatic SC joint subluxation is common in young, hypermobile women and is not a dislocation. The medial clavicle subluxes spontaneously or with minor movements and reduces. It does not require reduction, immobilisation, or surgery. Education, reassurance, and avoidance of provocative positions are the appropriate management. Operating on this condition has high failure and complication rates.
Investigations
Imaging Protocol
Views: AP chest, serendipity view (40-degree cephalic tilt) - now largely superseded
Sensitivity: Plain films miss up to 50 percent of SC dislocations
Role: Initial screen, exclude associated rib or lung injury
Limitations: Cannot define direction accurately; cannot assess mediastinal relationship
Indication: All suspected SC dislocations
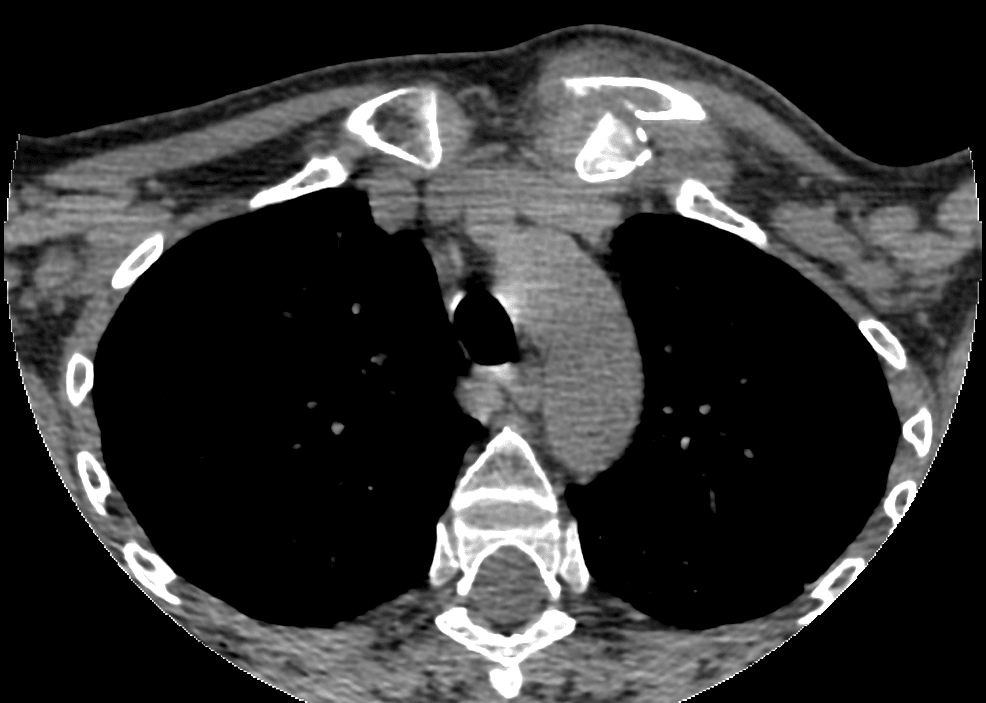
Acquisition: Thin-slice (1 mm) CT from chin to diaphragm, with IV contrast
Findings: Direction of dislocation, distance displaced, relationship to mediastinal vessels, trachea, oesophagus
Reconstructions: 3D and multiplanar reformats for surgical planning
Advantage: Definitive diagnosis, vessel mapping, surgical planning
Indication: Posterior dislocation with pulse deficit, expanding haematoma, or asymmetry
Findings: Vessel compression, intimal injury, pseudoaneurysm, occlusion
Outcome: Joint surgical planning with vascular surgery
Pre-op: Image sharing and on-table angiography as needed
Indication: Adolescents to distinguish physeal injury from true dislocation
Findings: Physeal oedema, intact ligaments, no true joint disruption
Role: Conservative treatment justification, avoids operation on physis
Plain films cannot reliably diagnose or exclude SC dislocation. Any patient with clinical suspicion (mechanism, deformity, mediastinal symptoms) requires CT with IV contrast. Do not delay CT to obtain multiple plain views - the serendipity view is a historical curiosity.
Management Algorithm
Anterior SC Joint Dislocation
Goal: Symptom relief and return to function. Most are stable and well-tolerated even if the medial clavicle remains prominent.
Treatment Protocol
Analgesia: Oral paracetamol, NSAID, short opioid course if needed
Sling: Broad-arm sling for 1-3 weeks for comfort
Ice and rest: First 48-72 hours
Counselling: Explain that the lump may persist cosmetically; this is acceptable
Progressive ROM: Pendulum, then active-assisted, then active
Strengthening: Rotator cuff and scapular stabilisers at 3-4 weeks
Avoid: Heavy lifting, contact sport for 6-12 weeks
Sport-specific rehab: Overhead athletes, throwers, contact sports
Surgery reserved for: Persistent instability, functional limitation, failure of rehab
Realistic outcome: Most return to full function with acceptable cosmesis
Do not operate on a first-time anterior SC dislocation. Operative reduction and stabilisation has high failure and complication rates (recurrent instability, hardware failure, neurovascular injury). Even if the medial clavicle remains prominent, function is generally excellent with conservative care. Surgery is reserved for chronic, symptomatic instability that has failed structured rehabilitation.
Complications
- Incidence
- Up to 30 percent of posterior dislocations
- Risk Factors
- High-energy mechanism, sharp displaced fragment
- Management
- Vascular surgery, repair or bypass
- Incidence
- Reported in case series
- Risk Factors
- Posterior displacement, delayed reduction
- Management
- Urgent reduction, possible tracheostomy
- Incidence
- Rare
- Risk Factors
- Penetrating component, sharp posterior fragment
- Management
- Contrast study, surgical repair
- Incidence
- 20-30 percent after reconstruction
- Risk Factors
- Ligamentous laxity, hypermobility, inadequate rehab
- Management
- Revision reconstruction or resection
- Incidence
- Catastrophic when it occurs
- Risk Factors
- Use of K-wires across SC joint
- Management
- Avoid K-wires; use plates or tendon graft
- Incidence
- Up to 50 percent with plates
- Risk Factors
- Thin soft tissue cover, repetitive motion
- Management
- Removal of hardware once ligaments healed
- Incidence
- Rare
- Risk Factors
- Posterior compression, intimal injury
- Management
- Anticoagulation, vascular intervention
K-wires and Kirschner wires across the sternoclavicular joint have migrated into the heart, aorta, pulmonary artery, lung, oesophagus, trachea, and spinal cord, with multiple reported deaths. Use plate fixation, suture anchors, or tendon graft reconstruction. If a wire is used (rare salvage scenarios), it must have a secure bend at the lateral end, and the patient must be followed with serial imaging until removal.
Outcomes and Prognosis
- Indication
- First-time anterior dislocation
- Expected Outcome
- 90 percent good function, acceptable cosmesis
- Long-term Function
- Excellent return to sport and work
- Indication
- Acute posterior dislocation, stable after reduction
- Expected Outcome
- Good function, low recurrence if costoclavicular intact
- Long-term Function
- Excellent if reduced within 24-48 hours
- Indication
- Failed closed, mediastinal compromise
- Expected Outcome
- Good but with surgical morbidity
- Long-term Function
- Good if vascular or visceral injury addressed
- Indication
- Failed non-operative, symptomatic instability
- Expected Outcome
- 70-80 percent good-to-excellent
- Long-term Function
- Variable; re-operation common
Best prognosis: Acute anterior dislocation treated conservatively, acute posterior dislocation reduced within 24 hours with intact costoclavicular ligament, low-demand patient
Poor prognosis: Delayed posterior dislocation, failed closed reduction, multiple reconstruction attempts, hypermobility syndromes, contact athletes returning to high-impact sport
Key threshold: 24-48 hours for posterior dislocation - outcomes decline significantly with delay due to mediastinal compression and soft tissue contracture
Guidelines, Registries & Global Practice
- SC dislocations are rare, representing under 1 percent of all joint dislocations and 3 percent of shoulder-girdle injuries
- Anterior dislocations are 3 to 1 more common than posterior
- Posterior dislocations are predominantly high-energy - road traffic collisions, contact sport, falls from height
- Mediastinal compromise is reported in a quarter to a third of posterior dislocations in published series
- High-resource: 24-hour access to CT, vascular and cardiothoracic surgery, and image intensifier for closed reduction
- Limited-resource: Closed reduction under sedation in the emergency department may be necessary if theatre and vascular backup are unavailable - transfer to a tertiary centre is preferred if any mediastinal signs
- Universal principle: Posterior SC dislocation requires urgent reduction; do not delay transfer for a CT that is not available locally
- Reconstruction: Concentrated in specialist shoulder units; soft tissue techniques preferred over hardware
- Diagnosis emphasis
- CT with contrast in any suspected SC dislocation
- Acute treatment
- Posterior: closed reduction in theatre with thoracic backup; anterior: conservative
- Surgery / reconstruction
- Soft tissue reconstruction (figure-of-8 tendon graft) for failed non-operative
- Diagnosis emphasis
- CT for direction and mediastinal assessment
- Acute treatment
- Posterior: urgent closed or open reduction; anterior: sling and rehab
- Surgery / reconstruction
- Tendon graft preferred; plates reserved for failed soft tissue; avoid K-wires
- Diagnosis emphasis
- CT or MRI in suspected dislocation, MRI for physeal assessment
- Acute treatment
- Posterior: closed reduction under GA, thoracic surgery standby
- Surgery / reconstruction
- Tendon reconstruction (sternocleidomastoid, palmaris longus, hamstring)
- Diagnosis emphasis
- CT with contrast; vascular surgery consult for posterior
- Acute treatment
- Posterior: closed reduction in theatre; anterior: non-operative
- Surgery / reconstruction
- Soft tissue reconstruction with suture anchors preferred
There is no dedicated registry for sternoclavicular joint dislocation. Evidence is dominated by small retrospective case series and technique papers. The major arthroplasty registries (NJR, AJRR, AOANJRR) do not capture SC joint reconstruction, as it is uncommon. Practice is principle-based: CT with contrast for diagnosis, urgent closed reduction of posterior dislocations with cardiothoracic backup, and soft tissue reconstruction for chronic instability using tendon graft rather than hardware.
Record in every SC joint injury:
- Direction of dislocation (anterior or posterior) on CT
- Mediastinal structure assessment (vessels, trachea, oesophagus)
- Pulses, capillary refill, and neurological exam in the affected arm
- Voice, breathing, and swallowing symptoms at presentation
- Plan for closed versus open reduction and surgical team involved
- Counselling about recurrence, hardware, and re-operation risks if reconstruction is performed
Posterior SC dislocation with missed mediastinal injury is a recurring source of severe morbidity and litigation worldwide. Document the CT findings, the surgical team involved, and the reduction technique in every case.
Controversies & Areas of Uncertainty
Soft tissue reconstruction (figure-of-8 tendon graft, suture anchors) is biomechanically and biologically appealing but has higher reported re-dislocation rates in some series. Plate fixation provides initial stability at the cost of frequent hardware-related re-operation. There are no head-to-head trials.
Some surgeons advocate operative stabilisation of first-time anterior dislocations in young, high-demand athletes, but complication rates are high and re-dislocation is common. Most guidance reserves surgery for chronic, symptomatic instability that has failed structured non-operative care.
Sternocleidomastoid (in situ), hamstring (semitendinosus, gracilis), and palmaris longus have all been described. There is no clear winner. Sternocleidomastoid is convenient but limited in length; hamstring is robust but adds donor morbidity; palmaris longus is thin and may be absent.
Excessive resection destabilises the medial clavicle and worsens instability. The safe upper limit is generally cited as 1 to 1.5 cm in adults, with preservation of the costoclavicular ligament. Beyond this, reconstruction or arthrodesis may be required.
MCQ Practice Points
Q: What is the primary ligamentous restraint to anterior and posterior translation at the sternoclavicular joint? A: The posterior capsule is the strongest restraint to anterior displacement, and the anterior capsule and costoclavicular (rhomboid) ligament together resist posterior displacement. The costoclavicular ligament is the primary restraint to medial-lateral displacement and is the key structure to reconstruct in chronic instability.
Q: What is the investigation of choice for suspected sternoclavicular joint dislocation? A: CT scan with IV contrast. Plain radiographs miss up to 50 percent of dislocations, and the serendipity view is largely obsolete. CT demonstrates direction, displacement, and relationship to mediastinal structures. CT angiography is added if vascular injury is suspected.
Q: A patient has a posterior SC dislocation with dyspnoea, dysphagia, and diminished radial pulse. What is your immediate management? A: This is a mediastinal emergency. Follow ATLS, establish IV access, send bloods, obtain urgent CT with IV contrast, and contact cardiothoracic and vascular surgery. The dislocation requires reduction under general anaesthesia in theatre with surgical backup, ideally within 24 hours.
Q: What is the first-line management of an acute anterior SC dislocation? A: Non-operative management with sling, analgesia, and physiotherapy. Operative reduction and stabilisation has high failure and complication rates and is reserved for chronic symptomatic instability. Even if the medial clavicle remains prominent, function is generally excellent.
Q: Why are K-wires contraindicated in sternoclavicular joint reconstruction? A: K-wires have migrated into the heart, aorta, pulmonary artery, lung, oesophagus, trachea, and spinal cord, with multiple reported deaths. Use plate fixation, suture anchors, or autologous tendon graft reconstruction (figure-of-8 sternocleidomastoid or hamstring graft).
Q: A 17-year-old presents after a fall with apparent anterior SC dislocation. What is the most likely true diagnosis? A: Medial clavicle physeal separation. The medial clavicular physis is the last in the body to fuse (around 23-25 years) and is the weakest link in the SC region in adolescents. True joint dislocation requires disruption of the strong posterior capsule and costoclavicular ligament, which is uncommon before skeletal maturity. The injury is usually stable after closed reduction and remodels over time.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 22-year-old rugby player presents to the emergency department after a direct tackle to his left shoulder. He has pain over the medial clavicle, difficulty breathing, and a change in his voice. On examination, there is a palpable depression at the left SC joint, the left arm is cooler than the right, and the left radial pulse is diminished. What is your immediate assessment and management?”
“A 19-year-old competitive cyclist falls over his handlebars during a race and presents to the emergency department with a visible lump over the medial end of his right clavicle. He has no dyspnoea, dysphagia, voice change, or vascular symptoms. CT confirms anterior SC dislocation with the medial clavicle displaced anterior to the manubrium and no mediastinal compromise. He is keen to return to competitive cycling. How do you manage this?”
Key Anatomy
- Saddle-type synovial joint with intra-articular disc
- Medial clavicle larger than manubrial fossa - stability is entirely ligamentous
- Posterior capsule = strongest restraint to anterior displacement
- Costoclavicular ligament = primary restraint to medial-lateral and reconstruction target
- Medial clavicle physis is the last to fuse (23-25 years) - weakest link in adolescents
Diagnosis
- Posterior = mediastinal emergency: dyspnoea, dysphagia, voice change, vascular signs
- Anterior = cosmetic lump, often stable, rarely an emergency
- CT with IV contrast is the investigation of choice - plain films miss up to 50 percent
- Always assess pulses, voice, breathing, and swallowing in any SC injury
- Serendipity view is largely obsolete - do not delay CT to obtain multiple plain views
Treatment Algorithm
- Anterior (first time) = non-operative: sling, analgesia, physiotherapy, return to sport 8-12 weeks
- Posterior (acute) = urgent closed reduction under GA with thoracic/vascular backup
- Posterior (failed closed) = open reduction via supraclavicular approach with vascular control
- Chronic instability = figure-of-8 tendon graft reconstruction; K-wires contraindicated
Reconstruction Risks
- K-wire migration into heart, aorta, lung, oesophagus, spinal cord - never use
- Plate fixation has high rate of hardware-related re-operation
- Tendon graft reconstruction - 20-30 percent re-dislocation rate
- Medial clavicle resection greater than 1.5 cm destabilises further
- Reserve surgery for chronic, symptomatic instability after failed non-operative care
Complications and Pitfalls
- Missed posterior SC dislocation with mediastinal injury is catastrophic
- Attempting closed reduction without imaging or surgical backup risks vascular injury
- Operating on atraumatic SC subluxation in hypermobile patients fails
- Anterior SC dislocation in adolescent = medial clavicle physeal separation, not true dislocation
- Document direction, mediastinal assessment, and reduction technique in every case
Evidence Base and Key Trials
Acute traumatic retrosternal dislocation of the clavicle
- Classic retrospective series of acute traumatic posterior (retrosternal) SC dislocations - early recognition and closed reduction produced good outcomes
- Delayed diagnosis beyond 24-48 hours significantly increased the need for open reduction and the rate of complications
- Mediastinal vascular compression was a recurring feature in unreduced posterior dislocations
Sternoclavicular joint dislocation: a systematic review and meta-analysis
- Systematic review and meta-analysis of sternoclavicular joint dislocations - synthesises treatment outcomes across the published series
- Posterior dislocations are uncommon but carry substantially higher morbidity than anterior dislocations, with mediastinal compromise the key concern
- Operative reconstruction is reserved for chronic symptomatic instability; most anterior dislocations are managed non-operatively with good functional outcomes
Treatment of traumatic posterior sternoclavicular dislocations
- Consecutive series of traumatic posterior SC dislocations treated with closed or open reduction - CT was the diagnostic test of choice
- Majority of cases reduced closed within 24-48 hours; open reduction reserved for those failing closed methods
- Vascular and oesophageal injuries were uncommon but required pre-operative CT angiography to identify
Sternoclavicular epiphyseal separation with adjacent clavicular fracture
- Classic first description of medial clavicular epiphyseal (physeal) separation - adolescents presenting with apparent SC dislocation more often have a physeal injury than a true joint dislocation
- True SC dislocation requires disruption of the strong posterior capsule and costoclavicular ligament, which is uncommon in skeletally immature patients
- Physeal injury is more often stable after closed reduction and rarely requires operative fixation
Posterior sternoclavicular joint injuries in the adolescent population: a meta-analysis
- Meta-analysis of posterior SC joint injuries in adolescents - most are actually medial clavicular physeal separations rather than true joint dislocations
- CT is the imaging modality of choice; physeal separations are usually managed with closed reduction and rarely require operative fixation
- Vascular and mediastinal complications are rare but require prompt recognition; overall outcomes after appropriate treatment are excellent