Suprascapular Nerve | Suprascapular & Spinoglenoid Notch | Overhead Athletes
- Two notches, two patterns: suprascapular notch lesion weakens supraspinatus AND infraspinatus; spinoglenoid notch lesion weakens infraspinatus ONLY
- Paralabral cyst: arises from a posterosuperior labral tear acting as a one-way valve; the classic spinoglenoid notch compressor
- Isolated infraspinatus wasting in an overhead athlete is suprascapular neuropathy at the spinoglenoid notch until proven otherwise
- EMG/NCS is the diagnostic standard; MRI finds the compressive lesion and shows muscle atrophy/fatty change
- Most cases are non-operative; decompress a discrete compressive lesion or refractory symptoms
- “Supraspinatus spared = lesion is at the spinoglenoid notch (distal)
- “Cyst means look for the labral tear that feeds it
- “Painless isolated infraspinatus wasting is common and often asymptomatic in athletes
- “Routine nerve release adds nothing to rotator cuff repair (Level I evidence)
Suprascapular notch = supraspinatus + infraspinatus weak. Spinoglenoid notch = infraspinatus only (supraspinatus spared because its motor branches leave proximally).
A spinoglenoid paralabral cyst is fed by a posterosuperior labral tear acting as a one-way valve. Treat the tear, not just the cyst, to prevent recurrence.
In overhead athletes, isolated infraspinatus wasting is often painless and well tolerated. High prevalence does not equal a surgical indication.
EMG/NCS confirms neuropathy and grades severity; MRI finds the compressive lesion and the labral tear. Both are usually needed.
- Likely Site
- Suprascapular notch
- Key Test
- EMG/NCS + MRI
- First Step
- Non-operative; image for cyst/ligament
- Likely Site
- Spinoglenoid notch
- Key Test
- MRI for paralabral cyst
- First Step
- Activity modification; aspirate/decompress cyst if symptomatic
- Likely Site
- Traction neuropathy
- Key Test
- MRI cuff + EMG
- First Step
- Treat the cuff tear; routine nerve release not required
Overview and Epidemiology
It is an easily missed cause of posterior shoulder pain and weakness that mimics a rotator cuff tear with normal tendons. According to PubMed, it is thought to cause roughly 2% of chronic shoulder pain (Clavert and Thomazeau, DOI). Recognising the notch-specific weakness pattern is high-yield.
Suprascapular neuropathy is compression or traction of the suprascapular nerve along its course over the scapula, producing posterior shoulder pain and weakness of external rotation and/or abduction.
- Overhead athletes: volleyball, baseball, tennis, swimming
- Isolated infraspinatus wasting: common in elite volleyball players (often the dominant/hitting shoulder)
- Older patients: traction from large/retracted rotator cuff tears
- Historically considered a diagnosis of exclusion; now recognised more often
Ask specifically about overhead sport and dominant arm.
- Paralabral (ganglion) cyst: from a posterosuperior labral tear
- Traction: repetitive overhead activity; retracted cuff tear
- Compression: ossified transverse scapular ligament, tumour, scapular fracture
- Distended notch veins: a recognised mimic of a cyst on MRI
Always look for an underlying labral tear when a cyst is present.
Pathophysiology and Anatomy of Suprascapular Neuropathy
The suprascapular nerve (C5-C6, from the upper trunk) passes UNDER the transverse scapular ligament at the suprascapular notch (the suprascapular artery passes OVER the ligament - "Army over Navy / artery over, nerve under"). It supplies supraspinatus, then curves around the base of the scapular spine through the spinoglenoid notch to reach infraspinatus.
- The motor branches to supraspinatus leave the nerve at or proximal to the suprascapular notch.
- The branches to infraspinatus are given off after the nerve rounds the spinoglenoid notch.
- Therefore a suprascapular notch lesion weakens both muscles, while a spinoglenoid notch lesion weakens infraspinatus only (supraspinatus is spared).
- Compression - a paralabral cyst, ossified/hypertrophied transverse scapular ligament, tumour, or distended veins narrow the notch.
- Traction - repetitive overhead motion stretches the nerve over a fixed point; the "sling effect" of the spinoglenoid ligament tethers the nerve during cross-body adduction and internal rotation. A large retracted cuff tear can also pull on the nerve medially.
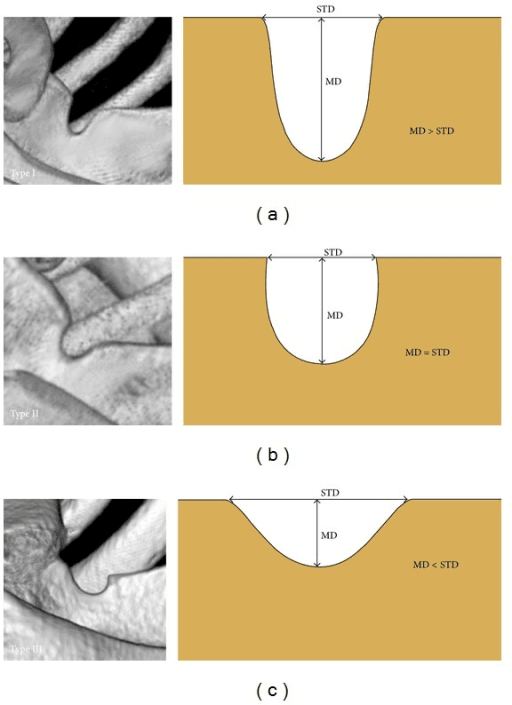
- A deep, narrow (U-shaped) suprascapular notch crowds the nerve and is associated with a higher entrapment risk.
UPPERSuprascapular Nerve Roots and Course
Hook:UPPER trunk nerve takes an UPPER route - C5-C6, over the top of the scapula, then around the spine to the infraspinatus.
CTOCauses of Suprascapular Neuropathy
Hook:CTO - Cyst, Traction, Other - the three mechanisms that injure the suprascapular nerve.
SINSpinoglenoid vs Suprascapular Notch
Hook:SIN = Spinoglenoid means Infraspinatus-only weakness, and it is the Notch where cysts sit.
Why It Hurts: The Nerve's Articular Sensory Territory
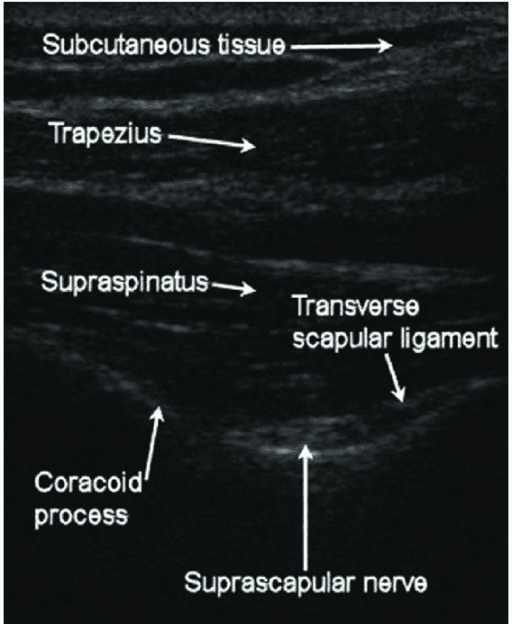
The topic repeatedly describes "deep, poorly-localised posterior shoulder pain" and uses a diagnostic/therapeutic nerve block (the imaging atlas even shows a block ultrasound) — both are explained by the suprascapular nerve's unusual sensory anatomy.
- Predominantly motor, but a major joint-sensory nerve. Beyond supplying supraspinatus and infraspinatus, the suprascapular nerve provides articular (sensory) branches to roughly two-thirds to 70% of the shoulder joint — the posterosuperior glenohumeral capsule, the acromioclavicular joint, the subacromial bursa and the coracoclavicular/coracoacromial ligaments. It has no cutaneous territory.
- Why the pain is deep and poorly localised. Because its sensory supply is deep, capsular and non-dermatomal, entrapment produces a diffuse, aching, hard-to-point-to posterolateral shoulder pain rather than a sharp, mappable pain — a useful contrast with C5-C6 radiculopathy (which follows a dermatome) in the differential.
- Why the nerve block works. A suprascapular nerve block anaesthetises that large articular territory, which is why it is both diagnostic here (temporary relief supports the diagnosis) and a recognised analgesic tool for shoulder pain more broadly (adhesive capsulitis, post-operative and chronic degenerative or hemiplegic shoulder pain). Ultrasound- or landmark-guided blocks target the nerve in the floor of the suprascapular fossa.
- Corollary: pain can persist after a technically successful decompression if the articular pain generator (the labral tear, capsule) is not also addressed — which is why several series report residual pain.
Q: Why does suprascapular neuropathy cause deep, poorly-localised pain, and why does a suprascapular nerve block relieve shoulder pain so broadly? A: The suprascapular nerve supplies about 70% of the shoulder joint's sensory (articular) innervation — posterosuperior capsule, AC joint, subacromial bursa and nearby ligaments — with no cutaneous territory. So its pain is deep and non-dermatomal (unlike C5-C6 radiculopathy), and blocking it anaesthetises much of the joint, giving both a diagnostic test and analgesia for many shoulder conditions.
Classification Systems
Classification by Site of Compression
- Supraspinatus
- Weak
- Infraspinatus
- Weak
- Typical Cause
- Ligament ossification, cyst, traction
- Supraspinatus
- Spared
- Infraspinatus
- Weak
- Typical Cause
- Paralabral cyst, spinoglenoid ligament
- Supraspinatus
- Variable
- Infraspinatus
- Variable
- Typical Cause
- Traction injury, neuralgic amyotrophy mimic
The clinical pattern of weakness localises the lesion before imaging.
Clinical Assessment
- Pain: deep, poorly localised posterolateral shoulder pain
- Weakness: external rotation (and abduction if proximal)
- Sport: repetitive overhead activity, dominant arm
- Often painless: isolated infraspinatus wasting may be an incidental finding
- Red flags: rapid progression, suspected mass
A cyst can present with pain even before weakness develops.
- Inspection: infraspinatus (and/or supraspinatus) wasting in the fossa
- External rotation weakness: with the arm at the side
- Abduction weakness: if supraspinatus involved (notch lesion)
- Tenderness: over the suprascapular/spinoglenoid notch
- Compensation: deltoid/trapezius overactivity, altered scapular rhythm
Always compare both shoulders from behind.
Consider rotator cuff tear, C5-C6 cervical radiculopathy, Parsonage-Turner syndrome (neuralgic amyotrophy), quadrilateral space syndrome (axillary nerve), and a posterosuperior labral tear without neuropathy. Distended spinoglenoid notch veins can mimic a paralabral cyst on MRI.
Investigations
Investigation Protocol
Localise by weakness pattern. Isolated infraspinatus weakness suggests a spinoglenoid notch lesion; combined weakness suggests a suprascapular notch lesion.
Diagnostic gold standard. Prolonged motor latency to supraspinatus and/or infraspinatus and denervation potentials confirm and localise the neuropathy. Note that pain can occur with a normal study.
Best for the compressive lesion. Shows a paralabral cyst, the feeding labral tear, muscle oedema (acute denervation) or fatty atrophy (chronic), and excludes a mass.
Ultrasound can show a cyst and guide aspiration. A diagnostic suprascapular nerve block giving temporary relief supports the diagnosis.
Management Algorithm
Non-operative Management
Conservative Steps
Reduce provocative overhead load. Especially for athletes with painless wasting who are functioning well.
Scapular stabilisation and cuff/periscapular strengthening. Restore scapulohumeral rhythm; recruit compensators where infraspinatus is weak.
Analgesia and a diagnostic/therapeutic suprascapular nerve block. Can confirm the diagnosis and relieve pain.
Consider aspiration of a symptomatic paralabral cyst. Often a temporising measure; cysts commonly recur if the labral tear is untreated.
Most isolated neuropathies, particularly painless wasting in athletes, are managed non-operatively.
Surgical Technique
Arthroscopic Suprascapular Notch Decompression
Surgical Steps
Beach-chair or lateral decubitus. Standard diagnostic glenohumeral and subacromial arthroscopy first.
Work medial to the coracoid, anterior to the supraspinatus. Develop the interval to expose the transverse scapular ligament.
Protect the suprascapular artery (above the ligament) and the nerve (below). Confirm the nerve before any release.
Divide the transverse scapular ligament to decompress the nerve. Address any bony narrowing if present.
Verify free nerve excursion. Standard portal closure; early ROM.
Preliminary series show normalisation of nerve latency and good pain/function outcomes after arthroscopic release.
Complications
- Comment
- Chronic fatty atrophy may not reverse
- Mitigation
- Treat early before irreversible atrophy
- Comment
- If labral tear left untreated
- Mitigation
- Repair labrum, not aspiration alone
- Comment
- Notch dissection is demanding
- Mitigation
- Identify and protect structures
- Comment
- Pain can persist despite decompression
- Mitigation
- Counsel on realistic expectations
Early diagnosis matters: once the infraspinatus undergoes chronic fatty infiltration, strength may not fully recover even after successful decompression.
Grading Fatty Atrophy and the Window for Recovery
The topic states repeatedly that chronic fatty atrophy "may not reverse" and that early treatment matters — here is how that atrophy is graded and why it sets the timing of intervention.
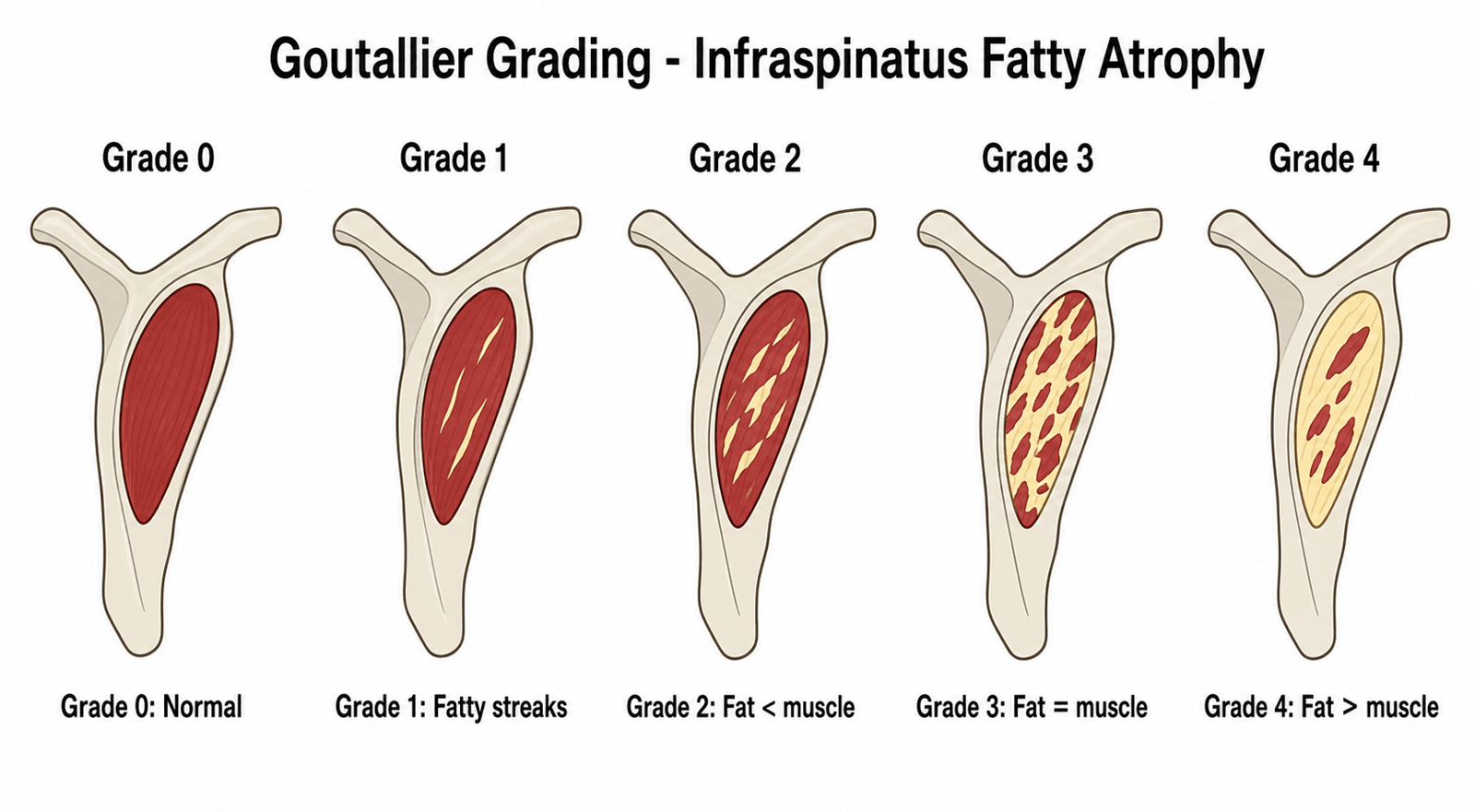
- Goutallier grading (originally CT, now applied on the sagittal-oblique "Y" MRI): Grade 0 normal muscle; Grade 1 a few fatty streaks; Grade 2 fat present but less than muscle; Grade 3 fat equal to muscle; Grade 4 fat exceeding muscle. Higher grades reflect irreversible replacement of the denervated infraspinatus (and/or supraspinatus) by fat.
- Supporting measures: the tangent sign (the muscle belly failing to cross a line drawn across the top of the fossa on the Y-view indicates significant atrophy) and the muscle occupation ratio quantify the same process.
- Why it governs timing. Denervated muscle first shows reversible oedema (acute denervation on MRI), then progresses to fatty infiltration and finally fixed atrophy. Once advanced fatty change (Goutallier grade 2-3 or higher) is established, decompression may relieve pain but strength often does not fully recover — the muscle is no longer contractile tissue. This is the mechanistic basis for the "treat early" refrain and for confirming/localising with EMG before atrophy sets in.
- Practical rule: muscle oedema without fatty infiltration on MRI is a favourable, potentially reversible picture; established fatty atrophy predicts incomplete strength recovery and should temper the surgical promise made to the patient.
Q: How does the degree of muscle change on MRI affect the prognosis of decompression in suprascapular neuropathy? A: Acute denervation oedema is potentially reversible, but once the muscle shows advanced fatty infiltration (Goutallier 2-3 or higher) — supported by a positive tangent sign / low occupation ratio — decompression may relieve pain yet strength recovery is limited. This is why the topic stresses early diagnosis and treatment before fixed fatty atrophy develops.
Clinical Relevance and Controversies
A double-blinded RCT (Sachinis, PMID 34156877) and a meta-analysis (Yang, PMID 35833960) show that adding suprascapular nerve release to rotator cuff repair does not improve pain, function, or nerve recovery. Routine release is not recommended.
Compressive neuropathy is common in overhead athletes, yet many have no clinically relevant deficit (Strauss, PMID 32732653). Prevalence does not equal a surgical indication.
Image-guided aspiration can relieve a spinoglenoid cyst (Wee, PMID 30283206) but recurrence is common unless the feeding labral tear is repaired.
Distended spinoglenoid notch veins can mimic a paralabral cyst on MRI and must be distinguished before percutaneous aspiration (Carroll, PMID 12589484).
Other open questions: whether traction neuropathy from a retracted cuff tear needs any direct nerve treatment; the threshold for operating on painless wasting in a high-level athlete; and the lack of a unified outcome metric across small surgical series.
Guidelines, Registries & Global Practice
Global Epidemiology
- An uncommon but under-recognised cause of shoulder pain, estimated at roughly 2% of chronic shoulder pain (PMID 25454727).
- Compressive neuropathy is highly prevalent among overhead athletes, but most have no clinically relevant deficit (PMID 32732653).
- Isolated infraspinatus wasting is well described in elite volleyball and other overhead sports, frequently in the dominant arm (PMID 16035699, PMID 29364045).
Side-by-Side Guidance
- Diagnosis
- Pattern of weakness, EMG/NCS, MRI for lesion
- First-line
- Non-operative: activity modification, physiotherapy, nerve block
- Surgical default
- Arthroscopic decompression for a compressive lesion or refractory symptoms
- Diagnosis
- Electrophysiology plus MRI; ultrasound for cyst
- First-line
- Conservative; image-guided cyst aspiration
- Surgical default
- Endoscopic release has superseded open surgery (PMID 25454727)
- Diagnosis
- Confirm neuropathy; assess functional need
- First-line
- Rehabilitation; treat the athlete, not just the scan
- Surgical default
- Decompress only symptomatic, well-indicated athletes (PMID 32732653)
Across regions the convergent position is that diagnosis rests on EMG/NCS plus MRI, that most cases are managed non-operatively, and that surgery - now predominantly arthroscopic - is reserved for a discrete compressive lesion or refractory symptoms.
Registry & Outcome Notes
- No dedicated international registry exists; evidence rests on RCTs (PMID 34156877), meta-analysis (PMID 35833960), and surgical case series (PMID 33091550, PMID 17210425).
- Arthroscopic decompression series report significant functional improvement and, in the absence of major concomitant pathology, no complications or revisions at medium-term follow-up (PMID 33091550).
High- vs Limited-Resource Practice
- High-resource: routine EMG/NCS, MRI for cyst and labral tear, ultrasound-guided block/aspiration, arthroscopic decompression.
- Limited-resource: clinical pattern recognition and a diagnostic suprascapular nerve block guide management; open decompression under regional anaesthesia remains effective where arthroscopy is unavailable.
Documentation & Consent (universal)
- Record the weakness pattern (supraspinatus vs infraspinatus) and visible wasting at each visit.
- When a cyst is present, document the feeding labral tear and the plan to address it.
- Consent for decompression should include incomplete strength recovery if chronic atrophy exists, cyst recurrence if the labrum is untreated, and risk to the suprascapular nerve and artery.
MCQ Practice Points
Q: A patient has weak external rotation with preserved abduction and isolated infraspinatus wasting. Where is the lesion? A: Spinoglenoid notch - distal to the supraspinatus motor branches, so only infraspinatus is affected.
Q: What is the relationship of the suprascapular artery and nerve at the suprascapular notch? A: Nerve passes UNDER the transverse scapular ligament; artery passes OVER it ("Army over, Navy under" / artery over, nerve under).
Q: What is the usual source of a spinoglenoid paralabral cyst? A: A posterosuperior labral tear acting as a one-way valve. Repair the labrum to prevent recurrence.
Q: What is the gold-standard diagnostic test for suprascapular neuropathy? A: EMG / nerve conduction studies. MRI identifies the compressive lesion and muscle atrophy.
Q: Does routine suprascapular nerve release improve outcomes during rotator cuff repair? A: No. A Level I RCT (Sachinis) and meta-analysis (Yang) show no added benefit.
Q: What can mimic a spinoglenoid paralabral cyst on MRI? A: Distended spinoglenoid notch veins (venous varix) - distinguish before any aspiration.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 24-year-old elite volleyball player has visible wasting of the infraspinatus fossa of the dominant shoulder, noted at a routine screen. He has mild posterior ache but performs at a high level. Abduction strength is normal; external rotation is mildly weak.”
“A 40-year-old presents with deep posterior shoulder pain and weakness of both abduction and external rotation. MRI shows no rotator cuff tear but an ossified-looking transverse scapular ligament. EMG shows prolonged latency to both supraspinatus and infraspinatus.”
“A 64-year-old has a large, retracted, reparable rotator cuff tear and EMG-confirmed suprascapular neuropathy. The patient asks whether the nerve also needs to be released at the time of repair.”
Key Anatomy
- Suprascapular nerve = C5-C6 from upper trunk
- Nerve UNDER transverse scapular ligament; artery OVER
- Suprascapular notch supplies supraspinatus first
- Spinoglenoid notch then supplies infraspinatus
Localising the Lesion
- Suprascapular notch = supraspinatus + infraspinatus weak
- Spinoglenoid notch = infraspinatus only
- Isolated infraspinatus wasting in athlete = spinoglenoid
- Confirm and localise with EMG/NCS
Causes
- Paralabral cyst from posterosuperior labral tear
- Traction: overhead sport or retracted cuff tear
- Ossified ligament, tumour, scapular fracture
- Distended notch veins (MRI mimic of cyst)
Management
- Non-operative first for most cases
- Aspirate symptomatic cyst (recurs without labral repair)
- Decompress for compressive lesion / refractory symptoms
- Arthroscopic release now dominant; treat early
Key Evidence
- Routine nerve release adds nothing to cuff repair (PMID 34156877, 35833960)
- Arthroscopic decompression: good durable outcomes (PMID 33091550)
- EMG normalises after release (PMID 17210425)
- Most athlete wasting is well tolerated (PMID 32732653)
Evidence Base
- Suprascapular neuropathy is under-recognised and increasingly diagnosed
- Aetiologies: repetitive overhead activity, traction from a rotator cuff tear, and compression at the suprascapular or spinoglenoid notch
- EMG/nerve conduction studies remain the diagnostic standard; MRI shows space-occupying lesions and fatty infiltration
- Initial treatment is non-operative; decompression for extrinsic compression or progressive pain/weakness
- Diagnosis combines history, examination, imaging, and electrodiagnostic studies
- Compressive neuropathy is highly prevalent in overhead athletes but most have no clinically relevant deficit
- Surgical release can improve return to play in well-indicated patients
- Surgery is not routinely recommended unless pain or strength deficits fail non-surgical care