Surgical Approaches to the Forearm, Wrist and Hand
Use the interval, protect the nerve, preserve tendon glide
Approach Families
Critical Must-Knows
- In the upper limb, a small cutaneous nerve or tendon pulley can determine the result.
- The Henry approach is safe only when the radial artery, superficial radial nerve, FCR plane and pronator handling are deliberate.
- The Thompson approach risks the posterior interosseous nerve; pronation moves the nerve away during proximal radius exposure.
- Hand incisions should respect creases, skin flaps, neurovascular bundles and tendon glide.
- Closure and rehabilitation are part of the approach because stiffness, adhesions and scar sensitivity can dominate outcome.
Clinical Pearls
- "For forearm fractures, approach choice follows the bone surface that needs reduction and plate placement.
- "For flexor tendon surgery, exposure must allow repair while preserving pulleys and digital neurovascular bundles.
- "For dorsal wrist work, protect extensor compartments and repair the retinaculum when needed to prevent bowstringing or tendon irritation.
- "A carpal tunnel incision should avoid the palmar cutaneous branch and recurrent motor branch territory.
Small structures, large consequences
Upper-limb approaches fail when the surgeon treats the exposure as a skin incision. Nerve branches, vessels, pulleys, extensor compartments and tendon sheaths must be protected from the start.
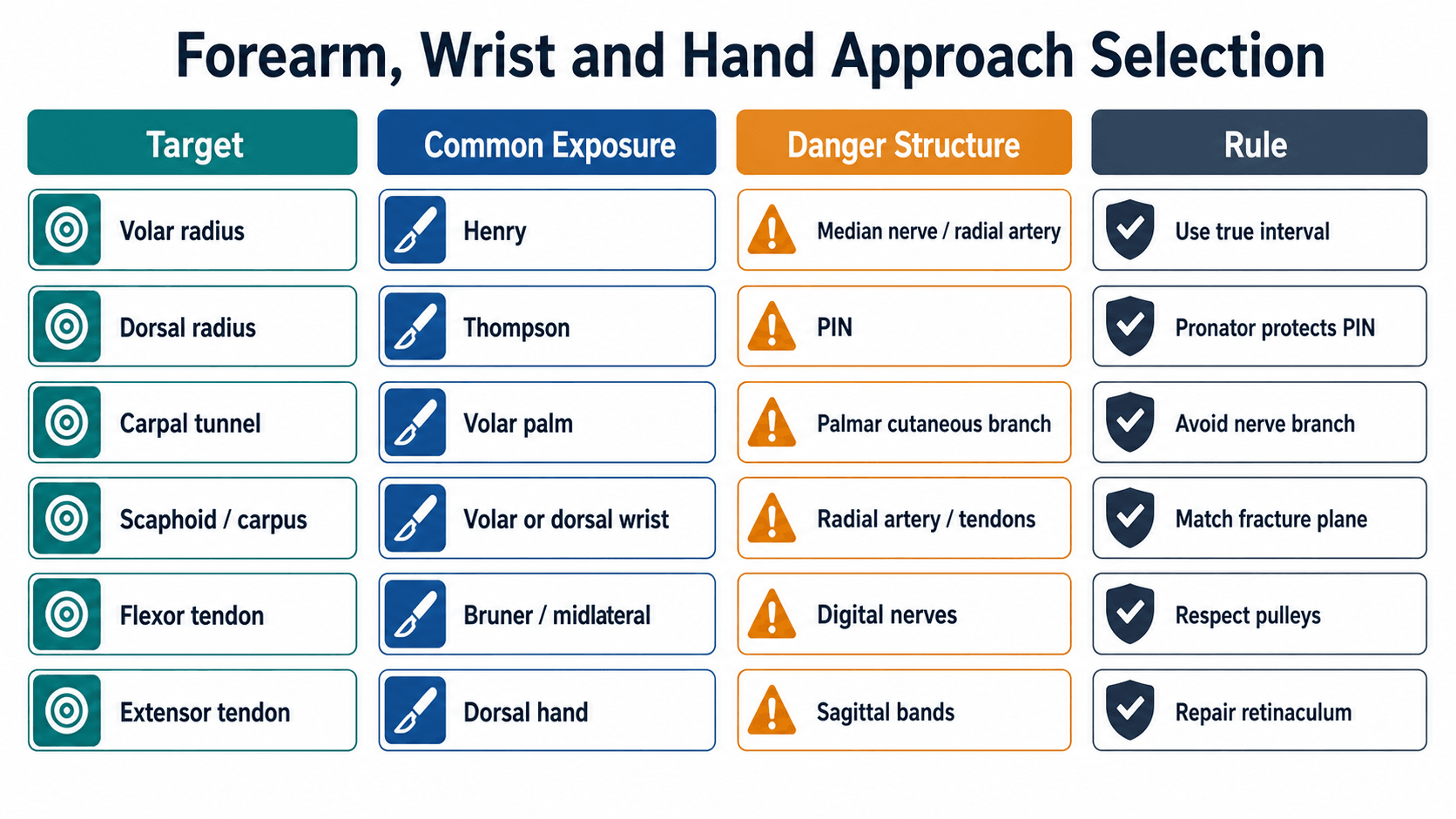
At a Glance: Upper-Limb Approach Choice
| Target | Common Exposure | Main Danger | Rule |
|---|---|---|---|
| Volar radius | Henry approach | Radial artery, median nerve, superficial radial nerve | Use FCR interval and protect pronator quadratus. |
| Dorsal/proximal radius | Thompson approach | Posterior interosseous nerve | Pronating the forearm helps move PIN away. |
| Ulna shaft | Subcutaneous border | Dorsal sensory ulnar nerve distally | Stay on safe border and preserve soft tissue. |
| Carpal tunnel | Volar palm | Palmar cutaneous branch and recurrent motor branch | Incision ulnar to thenar crease and controlled release. |
| Flexor tendon | Bruner or midlateral | Digital nerves and pulleys | Expose enough to repair but preserve pulley system. |
| Extensor tendon | Dorsal hand/wrist | Sagittal bands and extensor retinaculum | Repair stabilising structures and preserve tendon glide. |
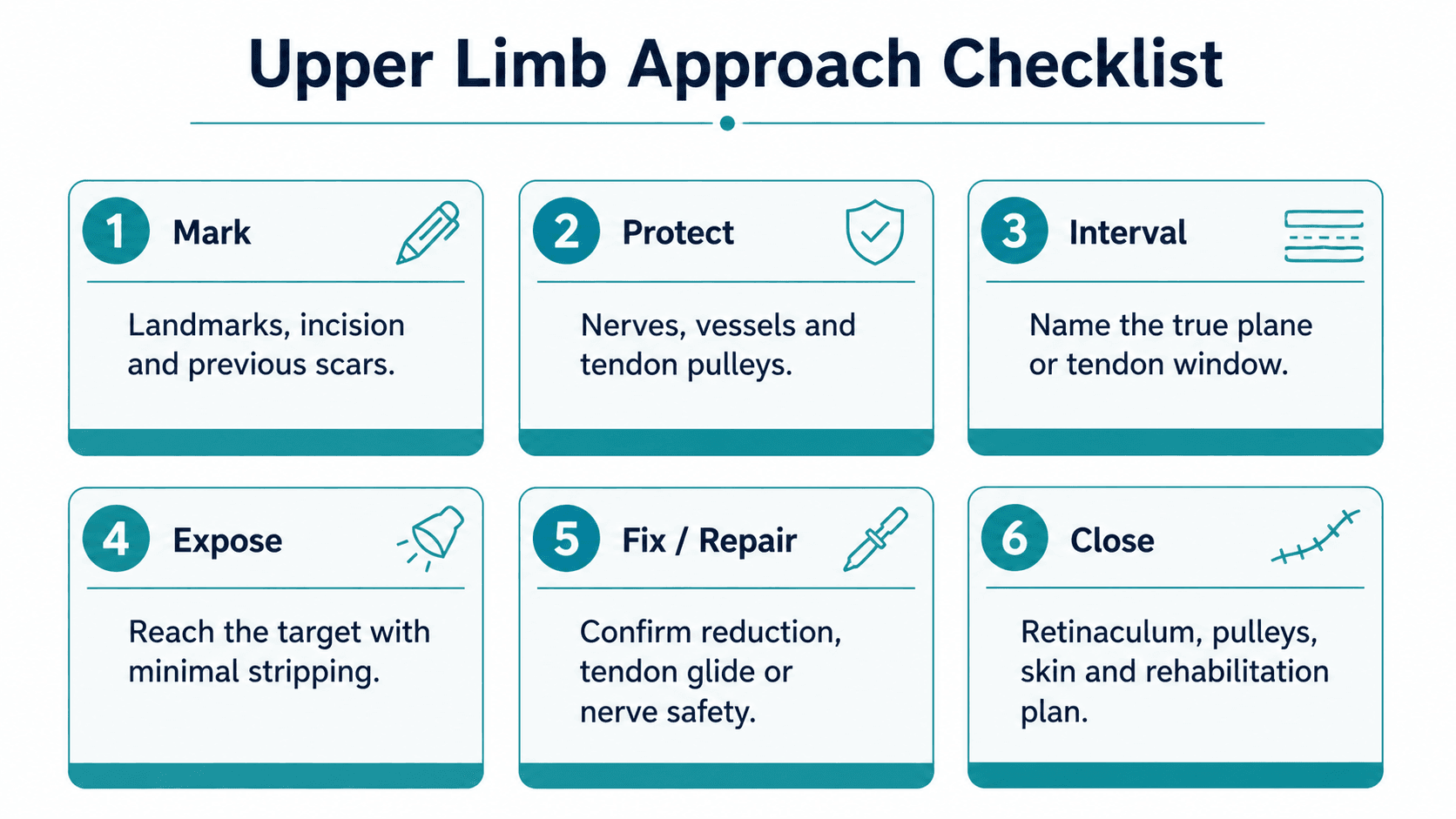
MAPUpper-Limb Approach
| M | Mark Landmarks, incision, previous scars and planned extension. |
| A | Avoid Named nerves, vessels, skin flaps and tendon pulleys. |
| P | Plane True interval, tendon window or subcutaneous border. |
| M | Mark Landmarks, incision, previous scars and planned extension. |
| A | Avoid Named nerves, vessels, skin flaps and tendon pulleys. |
| P | Plane True interval, tendon window or subcutaneous border. |
Hook:Map the limb before opening it.
GLIDEHand Exposure
| G | Gentle tissue handling Protect skin and subcutaneous flaps. |
| L | Locate nerves Digital, palmar cutaneous, dorsal sensory and superficial radial branches. |
| I | Incision planning Use Bruner, midlateral or dorsal lines according to target. |
| D | Do not sacrifice pulleys Preserve A2 and A4 when possible. |
| E | Early rehabilitation plan Closure must support tendon glide and therapy. |
| G | Gentle tissue handling Protect skin and subcutaneous flaps. | D | Do not sacrifice pulleys Preserve A2 and A4 when possible. |
| L | Locate nerves Digital, palmar cutaneous, dorsal sensory and superficial radial branches. | E | Early rehabilitation plan Closure must support tendon glide and therapy. |
| I | Incision planning Use Bruner, midlateral or dorsal lines according to target. |
Hook:The hand outcome depends on glide.
Overview and Indications
Forearm, wrist and hand approaches are selected by the target structure and by the functional tissue that must survive the exposure. In the forearm, the question is usually which bone surface needs reduction and fixation. In the wrist, the question is whether the target is volar, dorsal, radial, ulnar, intra-articular or ligamentous. In the hand, the question is how to reach tendon, nerve, bone or joint without creating stiffness, scar sensitivity or tendon adhesion.
Forearm
Prioritise safe intervals, plate position, radial artery and PIN safety. The radius has different safe windows depending on level.
Wrist
Prioritise carpal target, extensor compartments, palmar cutaneous branch, radial artery and DRUJ exposure.
Hand
Prioritise neurovascular bundles, pulleys, tendon glide, skin creases and rehabilitation-friendly closure.
Approach choice follows plate position
For forearm fixation, the approach should match the reduction surface and intended plate position. A technically easy incision that places the plate poorly is the wrong approach.
Relevant Anatomy
Upper-limb approach anatomy is dominated by named nerves, vessels, tendon compartments and gliding surfaces.
Anatomy That Changes the Approach
| Region | Key Structures | Why It Matters |
|---|---|---|
| Volar forearm | Radial artery, FCR, FPL, median nerve, pronator quadratus | Henry approach uses the FCR region and pronator quadratus for distal radius protection. |
| Dorsal proximal radius | PIN, supinator, EDC/ECRB interval | PIN injury is the feared complication; forearm rotation changes nerve position. |
| Ulnar border | Subcutaneous ulna, ECU/FCU interval, dorsal sensory ulnar nerve distally | Ulna is accessible but soft-tissue stripping still compromises healing. |
| Volar wrist | Median nerve, palmar cutaneous branch, recurrent motor branch, superficial palmar arch | Carpal tunnel release requires controlled distal and proximal release. |
| Dorsal wrist | Extensor compartments, EPL, dorsal sensory branches | Retinacular handling affects tendon irritation and bowstringing. |
| Digits | Digital nerves and arteries, flexor sheath, A2/A4 pulleys | Poor exposure can cause neuroma, tendon adhesion or bowstringing. |
Do not use generated anatomy as proof
For this region, exact nerve and vessel anatomy is too important to infer from a decorative diagram. Use verified anatomy sources and identify structures directly in theatre.
Internervous Plane and Intervals
Common Intervals
| Approach | Interval or Window | Target | Main Risk |
|---|---|---|---|
| Henry | Between brachioradialis and FCR region; develop volar radial interval | Volar radius and distal radius | Radial artery, superficial radial nerve, median nerve if too ulnar. |
| Thompson | Between EDC and ECRB proximally; dorsal radial exposure | Proximal/middle radius | PIN in supinator. |
| Subcutaneous ulna | Between ECU and FCU along ulnar border | Ulna shaft | Dorsal sensory ulnar branch distally, soft-tissue stripping. |
| Carpal tunnel | Volar palm incision ulnar to thenar crease | Transverse carpal ligament | Palmar cutaneous branch, recurrent motor branch, superficial arch. |
| Dorsal wrist | Between extensor compartments depending target | Carpus, distal radius, DRUJ, scaphoid | EPL, extensor retinaculum, dorsal sensory branches. |
| Bruner / midlateral | Zig-zag volar or midlateral finger incision | Flexor tendon, phalanx, digital nerve | Digital neurovascular bundle and pulleys. |
PIN protection
In dorsal proximal radius exposure, pronating the forearm helps move the posterior interosseous nerve away from the operative field. Still, do not rely on rotation alone if the dissection is unsafe.
Patient Positioning
Positioning and Setup
| Setup | Best Use | Practical Checks |
|---|---|---|
| Supine, arm table | Most forearm, wrist and hand surgery | Tourniquet, hand table, image intensifier, shoulder abduction comfortable. |
| Hand table with traction | Wrist arthroscopy, carpal work | Finger traps, traction tower, portals, nerve protection. |
| Arm across chest or pronated/supinated | Dorsal radius, Thompson, ulna access | Confirm C-arm views before prepping. |
| Wide prep to elbow or arm | Tendon, nerve, revision, infection or trauma | Allows proximal/distal extension and graft harvest if needed. |
Surgical Technique
Use: volar radius, distal radius fixation, radial shaft exposure.
- Supine position with arm on hand table.
- Mark radial styloid, FCR tendon, radial artery course and planned plate position.
- Incise along FCR for distal radius or extend proximally as needed.
- Develop the interval carefully; protect radial artery and superficial radial nerve.
- Mobilise FPL and expose pronator quadratus distally.
- Elevate pronator quadratus in a controlled manner and repair if possible.
- Confirm reduction, plate position and screw length.
Pitfalls: radial artery injury, median nerve traction, superficial radial nerve irritation, excessive pronator stripping and flexor tendon irritation from prominent plate.
Structures at Risk and Complications
Complications to Prevent
| Risk | Where | Prevention |
|---|---|---|
| PIN palsy | Thompson/proximal radius | Pronate forearm, respect supinator, avoid blind proximal dissection. |
| Radial artery injury | Henry and radial wrist | Identify and mobilise deliberately; avoid blind retraction. |
| Median nerve or branch injury | Carpal tunnel and volar wrist | Know palmar cutaneous and recurrent motor branch anatomy. |
| Digital nerve injury | Finger exposures | Use full-thickness flaps and identify bundles early. |
| Tendon adhesions | Hand tendon surgery | Gentle handling, pulley preservation, repair quality and early therapy. |
| Scar sensitivity | Palm and digits | Plan incisions away from high-pressure zones when possible. |
When to extend
Extend when reduction, tendon retrieval, nerve identification or implant safety cannot be achieved through the current window.
When to stop
Stop when the nerve is not found, tendon glide is compromised, skin viability is doubtful or image intensifier views are inadequate.
Differential of Approach Choice
When the target is decided, the remaining decision is which window minimises the structure at greatest risk. The table below compares the competing approaches surgeons actually weigh against each other in the exam and in theatre.
Choosing Between Competing Exposures
| Clinical Problem | Option A | Option B | Deciding Factor |
|---|---|---|---|
| Distal radius fracture | Volar (Henry-type, FCR) plate | Dorsal plate | Volar fixation lowers tendon-irritation risk but carries higher median-nerve/CTS risk; dorsal lowers neuropathy but irritates extensors (Wei 2013). |
| Proximal third radius fracture | Thompson (dorsal) | Henry extended proximally | Both expose the PIN in supinator; Thompson splits supinator over the nerve, Henry's distal volar exposure is safer but proximal radius access is limited. |
| Carpal tunnel syndrome | Open release | Endoscopic release | Endoscopic gives faster return to work and less scar pain but higher transient nerve injury; equivalent permanent injury and symptom relief (Li 2020, Koong 2022). |
| Both-bone forearm fracture | Single incision per bone | Reduce/plate to restore radial bow | Outcome tracks restoration of radial bow magnitude and location, not the skin incision (Schemitsch 1992). |
| Zone II flexor laceration | Bruner zig-zag | Mid-lateral | Bruner gives wide central exposure; mid-lateral keeps the scar off the volar pad and crease but limits dorsal-to-bundle access. Both must vent A2/A4 judiciously (Douwes 2025). |
Evidence Base
Radial bow restoration drives forearm function
- Restoration of the normal magnitude AND location of the radial bow correlated with a good functional result (over 80 percent of normal rotation, p less than 0.05).
- Recovery of grip strength was associated with restoring the location of the radial bow toward normal (p less than 0.005).
- 84 percent achieved excellent, good or acceptable function by Grace and Eversmann criteria.
PIN landmark in the proximal radius
- On a ventral approach the PIN runs about 10 mm proximal to the radial tuberosity in supination and about 5 mm distal to it in pronation.
- Laterally, pronation increases the PIN-to-tuberosity distance to roughly 3 cm.
- The radial tuberosity is a reliable intraoperative landmark for orientation to the nerve.
PIN position shifts with rotation and trauma
- In neutral the PIN crossed the radius a mean of 4.2 cm distal to the radiocapitellar joint; pronation increased this to 5.6 cm and supination decreased it to 3.2 cm.
- After a simulated diaphyseal fracture the protective effect of pronation was largely lost (shift fell from 2.13 cm to 0.24 cm).
- Following a simulated Essex-Lopresti injury the nerve migrated proximally toward the capitellum in all positions.
Endoscopic versus open carpal tunnel release
- Endoscopic release gave higher satisfaction, greater key pinch strength and earlier return to work (mean 7.25 days sooner) with fewer scar-related complications.
- Endoscopic release carried a higher transient nerve injury rate (OR 4.87, 95 percent CI 1.37-17.25).
- Permanent nerve injury did not differ significantly between techniques (OR 1.93, 95 percent CI 0.58-6.40).
Open versus single- or dual-portal endoscopic release
- Endoscopic release showed a higher incidence of transient postoperative nerve injury regardless of portal number, but equivalent overall complication and re-operation rates.
- Dual-portal release reduced scar tenderness compared with single-portal and open methods.
- Pillar pain, symptom relief and patient-reported satisfaction did not differ significantly between groups.
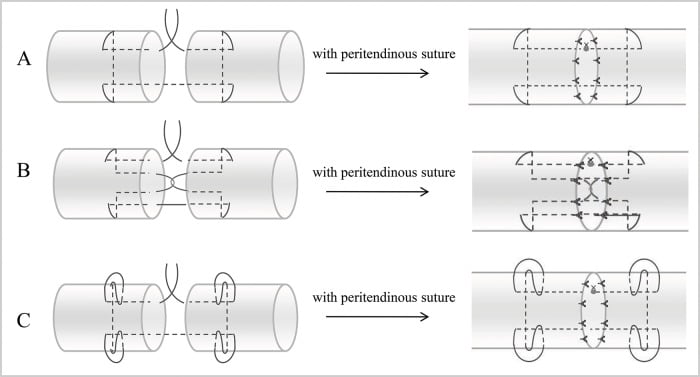
Zone II flexor tendon repair: evidence-based principles
- Repair should use a four-strand or multi-strand core suture, with or without an epitendinous suture.
- Judicious pulley venting (including parts of A2/A4) is safe and effective when needed for glide.
- Early controlled mobilisation, passive or active, is the cornerstone of management and reduces adhesion formation.
Dorsal versus volar plating complication profile
- Overall complication rates did not differ between volar and dorsal fixation.
- Volar fixation increased neuropathy (RR 2.19) and carpal tunnel syndrome (RR 4.56) but reduced tendon irritation (RR 0.38).
- Dorsal fixation lowered neuropathy at the cost of higher tendon-irritation risk.
AO Foundation / AO Surgery Reference — forearm and wrist exposures
- Anterior (Henry) approach is the workhorse for the radial shaft and distal radius; the dorsal (Thompson) approach is reserved for proximal/dorsal radius with deliberate PIN identification.
- Restore length, axial and rotational alignment and the radial bow for diaphyseal forearm fractures.
- The subcutaneous border of the ulna is exposed with minimal periosteal stripping to protect blood supply.
Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Approach for radial shaft fixation
"An adult has a displaced radial shaft fracture requiring plate fixation."
Flexor tendon exposure
"A patient has a zone II flexor tendon laceration requiring repair."
Open versus endoscopic carpal tunnel release
"A patient with electrodiagnostically confirmed carpal tunnel syndrome asks whether you will use an open or endoscopic release."
Controversies and Areas of Uncertainty
Open vs endoscopic carpal tunnel
Endoscopic release returns patients to work sooner with less scar pain, but randomised evidence shows a higher transient nerve-injury rate and no advantage in permanent injury or symptom relief. The debate is about morbidity and cost, not cure.
Volar vs dorsal distal radius plating
Volar locked plating dominates practice, yet meta-analysis shows it trades lower tendon-irritation risk for higher median-nerve and carpal-tunnel risk versus dorsal plating. Overall outcomes are similar, so fragment pattern and surgeon experience decide.
Pulley venting in zone II
Historic teaching protected A2 and A4 absolutely. Contemporary evidence supports judicious venting of part of A2 or A4 to allow a bulky repair to glide, provided enough pulley is preserved to prevent bowstringing.
WALANT vs tourniquet
Wide-awake local anaesthesia no tourniquet allows intraoperative testing of tendon glide and gapping, but the zone II review found it is not superior in outcome. Its role is pragmatic rather than evidence-mandated.
Answer controversy with the trade-off
Examiners reward candidates who frame a controversy as a balanced trade-off backed by evidence (for example, endoscopic carpal tunnel release: faster recovery versus higher transient nerve injury) rather than dogmatically declaring one option correct.
Guidelines, Registries and Global Practice
These approaches are performed worldwide and the underlying principles are universal, but emphasis and resource access differ by setting.
Society and Reference Guidance, Side by Side
| Source | Region | Position on Approach Selection |
|---|---|---|
| AO Foundation / AO Surgery Reference | International (Davos) | Henry (anterior) for radial shaft and distal radius; Thompson (dorsal) for proximal/dorsal radius with PIN identification; minimal-stripping ulnar exposure; restore radial bow. |
| AAOS | United States | Evidence-based clinical practice guidance on carpal tunnel syndrome and distal radius fractures; supports both open and endoscopic carpal tunnel release as effective options. |
| BOA / BSSH (UK) | United Kingdom | Standards for trauma and hand surgery emphasise complete carpal tunnel release, early protected motion after flexor tendon repair and specialist hand-therapy input. |
| EFORT / FESSH (Europe) | Europe | Consensus and instructional content supporting interval-based exposure, multi-strand flexor repair and structured rehabilitation. |
Global epidemiology
Distal radius fractures are among the most common fractures worldwide, with a bimodal distribution (young high-energy and elderly fragility). Carpal tunnel syndrome is the most common compressive neuropathy, affecting roughly 1 to 5 percent of the general adult population. Flexor tendon and digital injuries cluster in working-age men through occupational and machinery trauma.
Registry and outcome data
Hand and wrist procedures are less consistently captured in national arthroplasty registries than hip and knee, but distal radius fracture management is tracked in trauma audits (for example UK trauma audit datasets), which consistently show wide variation in operative versus non-operative management of the elderly distal radius fracture.
High-resource settings
Routine access to mini C-arm imaging, locking-plate systems, hand-therapy services, wrist arthroscopy and endoscopic carpal tunnel equipment. Wide-awake (WALANT) surgery is increasingly used to allow intraoperative tendon-glide testing.
Limited-resource settings
Reliance on open release, conventional plating or non-operative management, with fewer dedicated hand-therapy services. The core principles, interval-based exposure, nerve protection and pulley preservation, remain unchanged and matter even more when revision and therapy are scarce.
Forearm, Wrist and Hand Approaches: Decision Sheet
Clinical summary
Forearm
- •Henry: volar radius, radial artery and superficial radial nerve awareness.
- •Thompson: dorsal/proximal radius, PIN risk.
- •Ulna: subcutaneous border, preserve soft tissue.
Wrist
- •Carpal tunnel: avoid palmar cutaneous and recurrent motor branches.
- •Dorsal wrist: respect extensor compartments and retinaculum.
- •Scaphoid/carpus: approach follows fracture plane and fixation goal.
Hand
- •Use Bruner or midlateral incisions for digital exposure.
- •Identify digital neurovascular bundles.
- •Preserve pulleys and tendon glide.
Must not miss
- •PIN palsy in dorsal proximal radius exposure.
- •Radial artery injury in volar radial exposure.
- •Incomplete carpal tunnel release.
- •Digital nerve injury and tendon adhesions.