Congenital Interphalangeal Joint Ankylosis
- Symphalangism is a CONGENITAL FAILURE OF DIFFERENTIATION (segmentation) of a digital joint: the interphalangeal joint fails to form, so the phalanges are ANKYLOSED and there is no true synovial joint - it belongs to the 'failure of differentiation' group of congenital hand anomalies, distinct from an acquired contracture.
- The PROXIMAL (true) form, affecting the PROXIMAL interphalangeal (PIP) joint, is the most common; a DISTAL form affecting the DIP joint also occurs - the affected digit is straight and STIFF at the involved joint, and the little and ring fingers are commonly involved.
- The hallmark clinical sign is an ABSENT FLEXION CREASE over the affected joint with NO active or passive interphalangeal motion (the joint is ankylosed); radiographs show LITTLE OR NO joint space, with progressive bony fusion across the joint as the child grows (it may begin as a cartilaginous bar and ossify with maturity).
- It may be ISOLATED - frequently AUTOSOMAL DOMINANT, often affecting several digits and both hands (and feet) - or part of a SYNDROME, so an assessment for other anomalies and a genetic/family history is appropriate. The best-defined associations are the NOG-related allelic conditions, in which the SAME mutation may present as proximal symphalangism (SYM1), MULTIPLE SYNOSTOSES SYNDROME (SYNS1), stapes ankylosis with broad thumbs and toes (SABTT), tarsal-carpal coalition syndrome or brachydactyly type B2; symphalangism also occurs in Apert syndrome.
- ASSESS THE HEARING - and describe its treatment accurately. Stapes footplate ankylosis causes a CONDUCTIVE hearing loss across much of the NOG-related spectrum, and it is easily missed, so formal audiology is warranted in any child with proximal symphalangism. But do not call it straightforwardly surgically curable: reported outcomes of OTOMICROSURGERY ARE NOT ENCOURAGING because the BONE REGROWS, and the measures recommended are regular assessment and HEARING AIDS.
- The key DIFFERENTIAL is from an acquired or other congenital cause of a stiff/flexed finger - especially CAMPTODACTYLY (a flexion contracture of the PIP with preserved joint architecture and a flexion crease) and post-traumatic/arthritic ankylosis - because symphalangism is a primary failure of joint formation, not a contracture that can be released.
- MANAGEMENT is largely SUPPORTIVE because there is NO true joint to mobilise or reconstruct: function is usually surprisingly good when the digit is fused in a near-straight, useful position; attempts to create motion are generally unrewarding, so treatment focuses on optimising function, and any surgery (e.g. correcting a poor position, or arthrodesis in a better position if a fused joint is in a poor attitude) is reserved for specific functional problems - even a fracture through a symphalangic joint can heal with simple splinting and restored baseline function.
- “Symphalangism = congenital FAILURE OF DIFFERENTIATION -> the IP joint never forms (ankylosis). Proximal (PIP) = most common. Hallmark = ABSENT flexion crease + no IP motion.
- “Isolated (often autosomal dominant, multiple digits/bilateral) or syndromic - NOG-related spectrum (SYM1, multiple synostoses syndrome, SABTT, tarsal-carpal coalition, brachydactyly B2) and Apert. Differentiate from CAMPTODACTYLY (contracture with preserved joint + crease).
- “DON'T MISS THE DEAFNESS: stapes ankylosis causes conductive hearing loss - assess it formally. But otomicrosurgery outcomes are poor because bone REGROWS; hearing aids and regular review are the mainstay. No genotype-phenotype correlation predicts severity.
- “Largely supportive - there is NO true joint to reconstruct; function is good if fused near-straight; surgery only for a poorly-positioned digit (reposition/arthrodesis).
A straight, stiff finger with an absent flexion crease and no IP motion, and little/no joint space on radiograph = symphalangism (failure of joint differentiation). Often bilateral/multiple digits; may be syndromic.
Camptodactyly is a flexion contracture with a preserved joint and a flexion crease - it can be stretched/released. Symphalangism has no joint to release.
What It Is & How It Presents
Symphalangism is a congenital failure of differentiation (segmentation) of a digital joint - the interphalangeal joint fails to form, leaving the phalanges ankylosed with no true synovial joint. The proximal (true) form at the PIP joint is the most common (a distal DIP form also occurs), and the little and ring fingers are commonly affected. The affected digit is straight and stiff at the involved joint. The hallmark sign is an absent flexion crease with no active or passive IP motion; radiographs show little or no joint space, often beginning as a cartilaginous bar that ossifies into bony fusion as the child matures. It may be isolated (frequently autosomal dominant, multiple digits, bilateral, and may involve the feet) or syndromic - most importantly the NOG-related conditions (multiple synostoses syndrome and its allelic relatives) and Apert syndrome - warranting assessment for other anomalies, a family/genetic history, and formal hearing assessment.

Differential & Management
- Symphalangism
- Failure of joint differentiation (no joint forms)
- Camptodactyly
- Flexion contracture (joint is present)
- Symphalangism
- Straight, stiff (ankylosed)
- Camptodactyly
- Flexed (PIP) deformity
- Symphalangism
- Absent over the joint
- Camptodactyly
- Present
- Symphalangism
- Little/none; bony fusion
- Camptodactyly
- Preserved joint
- Symphalangism
- Supportive; reposition/arthrodesis if poorly positioned
- Camptodactyly
- Stretch/splint; release if needed (joint can move)
- Largely supportive: there is no true joint to mobilise; function is usually good when the digit is fused in a near-straight, useful position, and attempts to create motion are generally unrewarding.
- Assess associations: look for syndromic features and other anomalies; consider genetics/family history.
- Surgery - selective: reserved for a digit fused in a poor position (reposition/osteotomy) or to provide a stable arthrodesis in a better functional position; not to manufacture motion across a joint that never formed.
The central clinical reality of symphalangism is that the interphalangeal joint never formed - there is no articular cartilage or synovial joint to release, mobilise or replace - so it is fundamentally different from a contracture such as camptodactyly. Operations aimed at creating motion across a symphalangic joint are generally unrewarding and can make function worse. The realistic goal is to optimise the position and stability of the fused digit: most patients function well with the digit ankylosed near-straight, and surgery (repositioning osteotomy or arthrodesis in a better position) should be reserved for a digit whose fixed position genuinely impairs function. Recognising the diagnosis correctly - by the absent flexion crease, the lack of IP motion and the radiographic absence of a joint - prevents inappropriate attempts at joint release.
The Genetics: NOG, GDF5, and the Cushing Eponym
- The genes. Proximal (true) symphalangism (SYM1) is caused by heterozygous loss-of-function mutations in NOG (noggin, on chromosome 17q22) or in GDF5 (growth/differentiation factor 5). Both act in the BMP signalling pathway that patterns the joint interzone - the strip of cells that normally cavitates to form a synovial joint. When interzone formation fails, the phalanges never separate and fuse, giving the ankylosis.
- Inheritance. It is typically autosomal dominant with variable expressivity and reduced penetrance, so several digits, both hands (and often the feet) may be involved and the family history is frequently positive.
- The eponym. Harvey Cushing described and named symphalangism in 1916 in a family with proximal interphalangeal ankylosis, so "Cushing's symphalangism" refers to the proximal (true) form - the distal (DIP) form (SYM2) is a separate, rarer entity.
Q: What is the genetic basis of proximal symphalangism?
A: Proximal (true) symphalangism (SYM1) results from heterozygous mutations in NOG (noggin, 17q22) or GDF5, which disrupt BMP signalling and the formation of the joint interzone, so the phalanges never separate. It is autosomal dominant with variable penetrance (hence multiple-digit/bilateral/feet involvement and a positive family history). Harvey Cushing described and named the (proximal) condition in 1916 - "Cushing's symphalangism" is the proximal form.
Multiple Synostoses Syndrome and Conductive Deafness
- Multiple synostoses syndrome (SYNS1). The same NOG/GDF5 mutations that cause isolated proximal symphalangism also cause the multiple synostoses syndrome, in which the symphalangism is accompanied by synostoses at other joints - carpal and tarsal fusions, and often elbow (humeroradial) and other joint synostoses - with a characteristic facies.
- Stapes ankylosis and conductive hearing loss. A cardinal, high-yield feature is fixation (ankylosis) of the stapes footplate in the middle ear, producing a conductive hearing loss. A child diagnosed with proximal symphalangism - especially with other synostoses - should have hearing formally assessed, because the deafness is easily missed and is manageable.
- But be careful how you say "treatable". The instinctive answer is stapes surgery, and it is the wrong emphasis here: reported outcomes of otomicrosurgery are not encouraging, because the bone REGROWS and refixes the stapes. The measures actually recommended are regular systematic examination and HEARING AIDS. Offer surgery, if at all, as an option with a real risk of recurrence rather than as the definitive fix.
- The wider NOG-related family. The same NOG mutations produce a spectrum of allelic conditions, and the same mutation can give different labels: SYM1 (proximal symphalangism), SYNS1 (multiple synostoses syndrome), SABTT (stapes ankylosis with broad thumbs and toes), TCC (tarsal-carpal coalition syndrome) and BDB2 (brachydactyly type B2). Several of these feature stapes ankylosis, which is why the hearing question arises across the whole group.
- You cannot predict the phenotype from the mutation. Although reported NOG mutations cluster at regional hot spots and affect residues highly conserved in mammals, no distinct genotype-phenotype correlation has been established, and expression varies widely even within a family. Genetic testing confirms the diagnosis and guides counselling; it does not tell you how severe the hand or the hearing will be.
- Why it matters. Recognising the syndrome directs a search for carpal/tarsal/elbow synostoses and, crucially, the hearing loss, and informs autosomal-dominant genetic counselling.
Q: Which syndromic association of symphalangism must not be missed, and why?
A: Proximal symphalangism is a cardinal feature of the multiple synostoses syndrome (NOG/GDF5), which also causes carpal/tarsal and elbow synostoses and, importantly, stapes ankylosis with a conductive hearing loss. So a child with proximal symphalangism should have hearing formally assessed and be examined for other joint synostoses, with autosomal-dominant genetic counselling. Be precise about treatment: otomicrosurgical outcomes are reported as unencouraging because the bone regrows, so regular assessment and hearing aids are the mainstay rather than stapes surgery. The same NOG mutations also cause SABTT (stapes ankylosis with broad thumbs and toes), tarsal-carpal coalition syndrome and brachydactyly type B2, and no genotype-phenotype correlation allows you to predict severity.
Mnemonics & Memory Aids
FUSED
Hook:FUSED: Failure of differentiation, Unable to move, Smooth (no crease), Examine for syndromes and Ears, Don't reconstruct a joint that isn't there.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A child has a straight, stiff little finger with no crease at the PIP joint. What is the likely diagnosis and how do you manage it?”
What it is
- Congenital failure of differentiation - IP joint fails to form (ankylosis)
- Proximal (true, PIP) most common; distal (DIP) variant
- Little/ring fingers commonly involved
Diagnosis
- Absent flexion crease over the joint; no active/passive IP motion
- Radiograph: little/no joint space; progressive bony fusion
- Differentiate from camptodactyly (contracture with a preserved joint + crease)
Associations & management
- Isolated (often autosomal dominant, bilateral/multiple) or syndromic
- NOG-related allelic spectrum: SYM1, multiple synostoses syndrome, SABTT, tarsal-carpal coalition, brachydactyly B2; also Apert
- ASSESS HEARING - stapes ankylosis gives conductive loss; hearing aids + regular review
- Otomicrosurgery outcomes unencouraging (bone regrows) - don't promise a surgical cure
- No genotype-phenotype correlation - the mutation does not predict severity
- Largely supportive - no true joint to reconstruct; function good if fused near-straight
- Surgery only for a poorly-positioned digit (reposition/arthrodesis)
Evidence & Key Studies
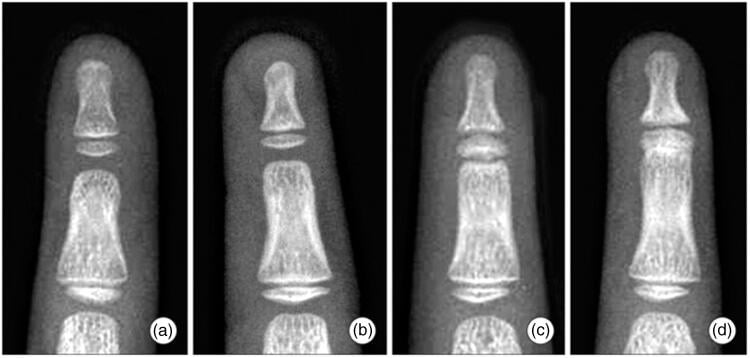
Proximal interphalangeal-level fracture in a patient with symphalangism
- A SINGLE CASE REPORT - it establishes that a fracture through a symphalangic segment can be managed non-operatively, and nothing about how often this happens or how reliably it works.
- The report presents a fracture at the level of a fused proximal interphalangeal joint in a patient with proximal symphalangism of the hand.
- Non-operative management with splinting resulted in osseous healing and restored baseline function - a useful reassurance, since the instinct on seeing a fracture line at a fused joint may be to fix it.
- No follow-up duration, functional score or comparison is reported, and publication bias in single-case reporting favours good outcomes.
Multiple synostoses syndrome: clinical report and retrospective analysis
- A single Chinese pedigree with proximal symphalangism, conductive hearing loss and distinctive facies, plus a review of the published literature - so a case report with a narrative synthesis, not a cohort.
- Whole-exome sequencing identified a novel NOG missense mutation (c.554C>G, p.Ser185Cys) cosegregating in the family, confirmed by Sanger sequencing across three generations.
- The literature review found the phenotype varies widely, but typical facies, conductive hearing loss and proximal symphalangism occur frequently. Mutations cluster at regional hot spots in residues highly conserved in mammals, yet NO DISTINCT GENOTYPE-PHENOTYPE CORRELATION has been identified across different populations - so the mutation does not predict severity.
- TREATMENT MESSAGE THAT MATTERS: regular systematic examination and HEARING AIDS are beneficial, whereas the outcomes of OTOMICROSURGERY ARE NOT ENCOURAGING owing to REGROWTH OF BONE. Stapes surgery should therefore not be presented as a definitive cure for the conductive deafness.
- Limitations: one family, and a narrative rather than systematic literature review with no pooled denominators, so the frequency statements are impressions from small published series.
Novel NOG mutation in Japanese patients with stapes ankylosis with broad thumbs and toes
- A CASE REPORT of one Japanese family, included because it defines the allelic spectrum rather than any outcome.
- NOG mutations cause a family of allelic bony disorders that can share the SAME mutation: stapes ankylosis with broad thumbs and toes (SABTT), proximal symphalangism (SYM1), multiple synostoses syndrome (SYNS1), tarsal-carpal coalition syndrome (TCC) and brachydactyly type B2 (BDB2) - collectively the NOG-related syndromes.
- Several of these phenotypes feature stapes ankylosis, which is why conductive hearing loss must be sought across the whole group and not only in classical multiple synostoses syndrome.
- The family reported had conductive hearing loss from congenital stapes ankylosis and a novel NOG mutation (c.682T>G, p.C228G); the authors propose altered BMP-antagonist activity or haploinsufficiency as the mechanism.
- Limitations: a single family, with the mechanism inferred from protein conformation modelling rather than demonstrated functionally.
The fracture through a fused PIP joint healing with splinting comes from Pan and colleagues (DOI), a single case report that is also the source of the radiographs. The finding that otomicrosurgical outcomes are unencouraging because of bone regrowth, that hearing aids and regular examination are the recommended measures, and that no genotype-phenotype correlation has been established for NOG come from Pan and co-workers' multiple-synostoses report and literature review (DOI). The NOG-related allelic spectrum - SYM1, SYNS1, SABTT, tarsal-carpal coalition syndrome and brachydactyly type B2 arising from the same mutations - comes from Ishino (DOI). The classification as a failure of differentiation, the proximal versus distal forms, the hallmark absent flexion crease, the interzone mechanism and the differential with camptodactyly are standard, well-established teaching.
What does not exist: no cohort of symphalangism has been published, so there is no incidence, no proportion that is syndromic rather than isolated, no figure for how many digits are typically involved, and no series reporting the results of repositioning osteotomy or arthrodesis. The radiographic grading of fibrous, cartilaginous and bony symphalangism is a descriptive scheme, not a validated classification with demonstrated reliability or prognostic value. All three papers cited here are single families or single patients.