Spinal Cord Cavity | Dissociated Cape Sensory Loss | Charcot Joint | Scoliosis
- Cape-like suspended dissociated sensory loss is the classic presentation (C2-T1)
- Spinothalamic fibers cross in anterior white commissure (where central syrinx strikes first)
- Dorsal columns spared early - proprioception, vibration, light touch preserved
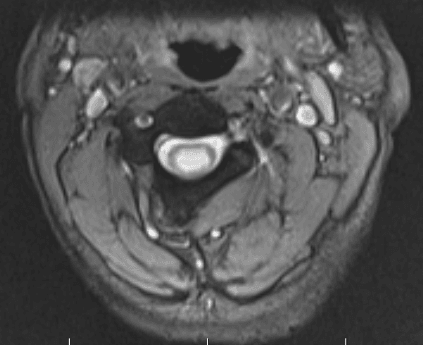
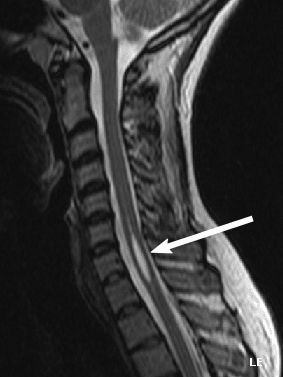
- MRI is the diagnostic gold standard (sagittal T2, axial T2, post-gad T1)
- Treat the cause: Chiari decompression, tumour resection, arachnoidolysis
- Charcot shoulder is painless destruction of the glenohumeral joint - classic exam sign
- “Syringomyelia + painless swollen shoulder = Charcot joint until proven otherwise
- “Every new left-thoracic scoliosis in a child needs MRI to exclude syrinx
- “Cape distribution reflects the longest crossing spinothalamic fibers (C2-T1)
- “Syringomyelia is a cause of scoliosis, NOT a complication - correct workup matters
- “Syrinx growth over 2-3 mm per year on serial MRI suggests active disease
- “Never correct scoliosis in syringomyelia without addressing the syrinx first
Central cord cavitation (syrinx) damages crossing spinothalamic fibers in the anterior white commissure first. Pain and temperature are lost in a suspended, cape-like distribution (typically C2-T1) while dorsal columns are spared - hence the term dissociated sensory loss.
Suspended segmental sensory loss over the shoulders, upper arms, and upper chest (cape). Reflects damage to crossing fibers at the level of the syrinx, NOT a peripheral nerve territory. Dorsal column modalities (proprioception, vibration) preserved.
Neuropathic (Charcot) arthropathy of the shoulder is the classic orthopaedic presentation - painless swelling, instability, and joint destruction from loss of proprioception and protective sensation. The 6 D's: Destruction, Density, Dislocation, Disorganization, Distension, Debris.
Syrinx is found in 25-50% of children with idiopathic scoliosis and up to 90% of painful, atypical, or left-thoracic curves. MRI of the neuraxis is mandatory before scoliosis surgery, posterior correction with sublaminar wires is dangerous, and any worsening neurology on follow-up mandates urgent re-imaging.
- Key Finding
- Lost pain/temp, preserved light touch
- Imaging
- MRI whole spine + brain
- Action
- Refer to spinal neurosurgery urgently
- Key Finding
- Charcot arthropathy, no pain
- Imaging
- X-ray shoulder + MRI cervical spine
- Action
- Charcot = spinal MRI to look for syrinx
- Key Finding
- Asymmetric reflexes, abdominal reflex loss
- Imaging
- MRI whole neuraxis before any fusion
- Action
- Correct syrinx first; brace/observe scoliosis
- Key Finding
- Worsening pain, sensory level rising
- Imaging
- MRI confirms post-traumatic syrinx
- Action
- Arachnoidolysis, shunt, or detethering
CAPECape Distribution of Dissociated Sensory Loss
Hook:CAPE of dissociated sensory loss = the orthopaedic classic - if you see it, image the whole neuraxis!
6DsThe 6 D's of Charcot (Neuropathic) Joint
Hook:The 6 D's - Destruction, Density, Dislocation, Disorganization, Distension, Debris - on a painless swollen joint should always trigger syrinx workup!
Overview and Epidemiology
Syringomyelia is the classic exam cause of dissociated sensory loss over a cape distribution. It is also a silent driver of two orthopaedic problems - Charcot shoulder and progressive scoliosis - and a known cause of catastrophic neurological injury during scoliosis correction if not recognised pre-operatively. The orthopaedic surgeon may be the first to suspect it when faced with a painless destroyed shoulder or an atypical curve.
- Prevalence: estimated 8-9 per 100,000 in the general population
- Peak age: 20-50 years for Chiari-associated, bimodal for post-traumatic
- Sex: slight male predominance overall; female predominance for Chiari I
- Onset: insidious in Chiari-associated, delayed (years) after trauma
- Charcot shoulder: present in approximately 50% of symptomatic syrinx patients
- Charcot elbow: second most common upper limb neuropathic joint
- Scoliosis: 25-50% of paediatric idiopathic scoliosis; up to 90% of atypical curves harbour a syrinx
- Myelopathy risk: undiagnosed syrinx during spinal deformity correction risks paraplegia
Pathophysiology
The crossing spinothalamic fibers ascend 1-2 segments before decussating through the anterior white commissure, immediately anterior to the central canal. A central cord syrinx expands from the central canal outward, hitting these crossing fibers first. Because crossing fibers from C2-T1 travel through the longest vertical segment of the cord and have the most extensive central representation, the cape distribution (C2-T1) is the classic zone of dissociated loss. Dorsal columns (posterior) are spared until late disease.
- Proposer
- Gardner (1965)
- Mechanism
- CSF pushed from 4th ventricle into central canal via obex
- Clinical Implication
- Explains Chiari II / Dandy-Walker; less applicable to Chiari I
- Proposer
- Oldfield (1994)
- Mechanism
- Tonsils act as piston, forcing CSF into cord via Virchow-Robin spaces
- Clinical Implication
- Best supported by cine-MRI; basis for foramen magnum decompression
- Proposer
- Ball & Dayan (1972)
- Mechanism
- Spinal CSF pressure transiently exceeds cranial; CSF tracks along dorsal roots into cord
- Clinical Implication
- Explains non-Chiari syrinx; supports restoration of normal CSF dynamics
- Proposer
- Levine (1995)
- Mechanism
- Chronic epidural venous hypertension drives fluid transudation into cord
- Clinical Implication
- Particularly relevant to post-traumatic and arachnoiditic syrinx
Anterior commissure crossing at each cord level
C2-T1 segments have the longest crossing fibers
Cape shape = bilateral suspended loss over shoulders, arms, and upper chest
Spinothalamic modalities (pain, temperature) lost first
Dorsal columns (proprioception, vibration) escape early
Loss of proprioception → microtrauma goes unperceived
Loss of pain → repeated injury without protective guarding
Loss of sympathetic tone → vasodilation, hyperaemia, osteoclastic activation
Result: hypertrophic joint destruction, often with massive effusion
Shoulder most common (50%) because the cord level matches
STAMPCauses of Syringomyelia
Hook:STAMP the cause onto the cord - Chiari is the most common STAMP in the exam!
Classification and Types
Classification by Aetiology
- Frequency
- 60-80 percent
- Imaging Clue
- Tonsils greater than 5 mm below foramen magnum
- Surgical Implication
- Posterior fossa decompression, duraplasty
- Frequency
- 5-15 percent of SCI
- Imaging Clue
- Cord injury site, focal syrinx, often rostral
- Surgical Implication
- Arachnoidolysis, syringopleural shunt
- Frequency
- Up to 30 percent with tumour
- Imaging Clue
- Enhancing nodule, expansile cord
- Surgical Implication
- Tumour resection; syrinx usually resolves
- Frequency
- Variable
- Imaging Clue
- Clumped nerve roots, CSF flow void loss
- Surgical Implication
- Subarachnoid space decompression, shunt
- Frequency
- Variable
- Imaging Clue
- Low-lying conus, lipoma, diastematomyelia
- Surgical Implication
- Detethering, dysraphism repair
Chiari I is by far the most common cause in exam questions. Always look for tonsillar descent on sagittal brain and cervical MRI.
Clinical Assessment
- Sensory: painless burns or injuries to hands, inability to feel hot water
- Motor: progressive upper limb weakness, gait disturbance, falls
- Pain: deep, poorly localized, often in the cape distribution
- Autonomic: hyperhidrosis or anhydrosis, bladder symptoms, Horner
- Trigger: antecedent trauma (often years earlier) or new shoulder swelling
- Sensory: dissociated suspended loss (pain/temp lost, light touch/proprioception preserved)
- Motor: LMN wasting at syrinx level (small muscles of hand), UMN signs below (brisk reflexes, Babinski)
- Reflexes: lost at the level (biceps, triceps); brisk below (knee, ankle)
- Shoulder: painless swelling, instability, crepitus - Charcot sign
- Spine: scoliosis, abdominal reflex asymmetry, stiff gait
Test pin-prick (pain) and cold (temperature) in the upper limbs, trunk, and lower limbs. Then test vibration (128 Hz tuning fork) and joint position sense (toe up or down). In early syringomyelia, pin-prick is lost over a cape while vibration is preserved. A sensory level on the trunk implies thoracic extension. Always compare both sides and document the upper limit of sensory loss - this corresponds to the rostral end of the syrinx.
- What It Tests
- Pin-prick vs vibration
- Finding
- Lost pain, preserved vibration over cape
- Significance
- Anterior commissure involvement
- What It Tests
- Small muscles (T1)
- Finding
- Thenar/hypothenar atrophy
- Significance
- Lower motor neuron at syrinx level
- What It Tests
- Lower limb corticospinal
- Finding
- Brisk knee/ankle, Babinski
- Significance
- Upper motor neuron below syrinx
- What It Tests
- Thoracic segments
- Finding
- Asymmetric or absent
- Significance
- Suggests intraspinal pathology (Chiari, syrinx)
- What It Tests
- Charcot arthropathy
- Finding
- Massive effusion, no tenderness
- Significance
- Urgently image the cervical spine
The syringomyelic hand shows a characteristic combination: wasted small muscles (LMN at T1) with preserved large muscle bulk of the forearm (because the syrinx is sparing the anterior horn cells at C5-C7). This produces the "main en griffe" or intrinsic minus pattern plus trophic skin changes, recurrent burns, and Charcot joints. Recognising this combination on inspection is a viva-favourite.
Syringomyelia is the classic cause of dissociated sensory loss, but the examiner who asks "what else does this?" expects a structured differential, because the lesion can be central-cord, vascular, or peripheral:
- Other central-cord lesions: an intramedullary tumour (ependymoma, astrocytoma, haemangioblastoma) can give the identical suspended dissociated pattern with or without a syrinx; acute central cord syndrome (hyperextension injury in a spondylotic neck) gives a cape-like upper-limb-predominant deficit.
- Vascular: anterior spinal artery (ventral two-thirds cord) infarction spares the dorsal columns and so produces dissociated loss (lost pain/temperature, preserved vibration/proprioception) - but with a sudden onset and a clear sensory level rather than a suspended cape.
- Peripheral / infective: leprosy is the commonest cause of dissociated sensory loss worldwide (it preferentially destroys the small pain/temperature fibres in cool acral skin), and hereditary sensory and autonomic neuropathies (HSAN) and amyloid/diabetic small-fibre neuropathy give a distal, length-dependent dissociated loss - distinguished from a syrinx by the peripheral (glove) rather than suspended (cape) distribution.
- Brainstem: a lateral medullary (Wallenberg) syndrome gives crossed dissociated loss (ipsilateral face, contralateral body).
The discriminator is the shape: a suspended, bilateral, cape pattern with LMN-at-level plus UMN-below points to a central cord process (syrinx or tumour), which mandates MRI of the whole neuraxis; a glove/length-dependent pattern points peripheral; a sudden level with preserved dorsal columns points to anterior spinal artery infarct.
Investigations
Imaging Protocol
Sequences: sagittal T2 entire spine, axial T2 at the syrinx level, T1 pre- and post-gadolinium
Look for: cord cavity position, length, wall nodularity (suggests tumour), Chiari I (greater than 5 mm tonsillar descent), craniocervical CSF flow void loss
Cine phase-contrast MRI: confirms obstruction at foramen magnum in Chiari-associated cases
Indication: focal cord expansion, mural nodule, syrinx centred on enhancing mass
Findings: ependymoma (cap sign, hemosiderin), astrocytoma (eccentric, long segment), hemangioblastoma (cyst with mural nodule)
Spinal angiography reserved for hemangioblastoma preoperative planning
Indication: confirmed syrinx under surveillance or post-treatment
Frequency: 6 months, then annually for stable syrinx; sooner if neurology changes
Threshold for intervention: increase in length greater than one level or diameter greater than 2-3 mm per year with symptoms
MRI is the only definitive investigation in syringomyelia. Plain films are normal. CT is unhelpful except to define associated bone abnormalities. Always request brain plus whole spine because associated Chiari I, hydrocephalus, or dysraphism will change management.
Management Algorithm
Chiari I Malformation with Syrinx
Goal: Restore normal CSF dynamics at the foramen magnum, decompress the syrinx, and halt neurological decline
Surgical Protocol
Imaging: confirm tonsillar descent greater than 5 mm and cine-MRI flow obstruction
Counsel: symptom stabilisation is the goal; pain responds best, sensory loss less reliably
Consent: CSF leak, pseudomeningocele, wound infection, failure to improve
Position: prone, head neutral, neuro-monitoring (SSEP, MEP)
Bone work: suboccipital craniectomy 3 x 3 cm, C1 (and sometimes C2) laminectomy
Dura: opening for duraplasty is the standard; bone-only decompression is debated for paediatric cases
Patch: pericranial or synthetic graft, water-tight closure
Tonsillar coagulation: shrinks obstructing tonsils
Fourth ventricle stenting: for persistent obstruction
Syrinx shunting: reserved for persistent or expanding syrinx after decompression
Imaging: MRI at 3 months, then 12 months
Syrinx behaviour: 50-80% decrease in size; persistent or growing syrinx suggests failed decompression
Symptoms: pain typically improves first; sensory and motor recovery less predictable
The single most important predictor of success is adequate bone removal and a water-tight duraplasty. Intraoperative ultrasound demonstrating restoration of CSF pulsation across the foramen magnum is a useful end-point. Tonsillar coagulation and syrinx shunting are reserved for the unusual case that does not respond.
Orthopaedic Manifestations
- Mechanism
- Loss of proprioception and pain sensation
- Clinical Picture
- Painless swelling, instability, joint destruction
- Management
- Brace, arthrodesis; arthroplasty controversial
- Mechanism
- Same - upper limb neuropathic joint
- Clinical Picture
- Painless instability, crepitus, effusion
- Management
- Brace, arthrodesis for end-stage
- Mechanism
- Cord dysfunction, asymmetric paraspinal input
- Clinical Picture
- Atypical curve (left thoracic), rapid progression
- Management
- MRI first, brace, treat syrinx, then fuse
- Mechanism
- T1 anterior horn cell loss plus sympathetic loss
- Clinical Picture
- Wasted intrinsics, trophic skin, recurrent burns
- Management
- Skin care, hand therapy, protect from injury
- Mechanism
- Vertebral body denervation
- Clinical Picture
- Painless vertebral collapse, kyphosis
- Management
- Brace, address syrinx, instrumented fusion
Posterior scoliosis correction in a patient with an unrecognised or untreated syrinx has a substantially increased risk of intra-operative neurological deterioration - paraplegia, hemiplegia, or new sensory level. MRI of the whole neuraxis is mandatory before any scoliosis fusion. If a syrinx is found, treat it first (cause-directed surgery), then proceed to deformity correction with full neuro-monitoring. Sublaminar wires (Luque-Galveston) are particularly hazardous - prefer pedicle screws and incremental correction.
- Left thoracic curve (right thoracic is the usual idiopathic pattern)
- Painful scoliosis in a child or adolescent
- Rapid progression of curve despite bracing
- Neurological signs: asymmetric reflexes, abdominal reflex loss, gait change
- Skin stigmata of dysraphism: dimple, hair patch, lipoma, sinus
- Foot deformities: cavus, claw toes, leg length discrepancy
- First: MRI whole neuraxis to confirm syrinx and identify cause
- Then: refer to spinal neurosurgery to address the cause
- Brace: for curves under 25-30 degrees, while syrinx is treated
- Fusion: only after syrinx stabilised or resolved, with full neuro-monitoring
- Follow-up: monitor for neurological change and curve progression
- Caution: pedicle screws preferred over sublaminar wires
Treatment of the syrinx does not reverse established Charcot changes, but it may halt progression. Surgical options for end-stage Charcot shoulder include arthrodesis (fusion is the most reliable procedure despite the destruction) and reverse total shoulder arthroplasty (controversial - high failure from persistent denervation, used selectively in stable neurology). Bracing and activity modification are first line. Always address the syrinx before reconstructive surgery.
The 6 D's above describe the hypertrophic (productive) neuropathic joint - the exuberant sclerosis, osteophyte and debris pattern typical of the diabetic foot and tabetic knee. But the upper-limb Charcot of syringomyelia is classically the ATROPHIC (resorptive) form, and recognising it is a distinct radiographic exam point:
- Atrophic / resorptive pattern: gross osteolysis and resorption of bone ends with little or no new bone - the humeral head can simply melt away, giving the "licked candy stick" / "sucked candy" tapered appearance, a surgical-looking "resorptive amputation" of the proximal humerus, scant debris and gross instability/pseudarthrosis. It is more common in non-weight-bearing, proximal upper-limb joints.
- Hypertrophic / productive pattern: the 6 D's (Destruction, Density/sclerosis, Dislocation, Disorganisation, Distension, Debris) with abundant osteophyte and fragmentation - more common in weight-bearing lower-limb joints.
- Why it matters: the resorptive shoulder is easily mistaken for an aggressive tumour or infection (massive osteolysis), so the painless presentation + dissociated sensory loss + a cervical syrinx on MRI is what makes the diagnosis. It also explains why reconstruction is so hard - there is little bone stock left to fuse or implant into.
Exam point: a painless shoulder with massive bony resorption ("licked candy stick" humeral head) rather than the florid productive 6 D's is the atrophic neuropathic joint of syringomyelia - image the cervical cord.
Complications
- Incidence
- Untreated or progressive syrinx
- Risk Factors
- Syrinx growth greater than 2-3 mm per year
- Management
- Cause-directed surgery, shunting as salvage
- Incidence
- Up to 50 percent of symptomatic cases
- Risk Factors
- Long-standing syrinx, delayed diagnosis
- Management
- Brace, arthrodesis, address syrinx
- Incidence
- Up to 50 percent in paediatric series
- Risk Factors
- Atypical curve, untreated syrinx
- Management
- Brace, fuse after syrinx treated
- Incidence
- 5-10 percent
- Risk Factors
- Inadequate duraplasty, poor wound healing
- Management
- Re-explore, resuture, lumbar drain
- Incidence
- Up to 10 percent
- Risk Factors
- Inadequate dural closure, raised ICP
- Management
- Compression, re-suture, lumbar drain
- Incidence
- 20-50 percent at 5 years
- Risk Factors
- Proteinaceous fluid, scarring
- Management
- Revision, alternative shunt, cause retreatment
- Incidence
- Rare but catastrophic
- Risk Factors
- Unrecognised syrinx, sublaminar wires
- Management
- Wake-up test, neuro-monitoring, abort and stage
The most common medicolegal claims involving syringomyelia centre on (1) failure to image the cervical spine in a patient with a painless Charcot shoulder, (2) failure to perform a pre-operative MRI in atypical scoliosis, and (3) failure to recognise an ascending sensory level years after spinal cord injury. Document the dissociated sensory exam, image the neuraxis when the cape pattern is present, and ensure scoliosis workup includes MRI of the entire spine and brain.
Outcomes and Prognosis
- Treatment
- Foramen magnum decompression + duraplasty
- Pain Relief
- 70-80 percent improved
- Sensory / Motor Recovery
- 30-50 percent improved; 80 percent stabilised
- Long-term
- Good, durable if syrinx collapses on MRI
- Treatment
- Arachnoidolysis, shunt, detethering
- Pain Relief
- 70 percent improved
- Sensory / Motor Recovery
- Stabilised rather than recovered
- Long-term
- Shunt failure common; revision often required
- Treatment
- Tumour resection
- Pain Relief
- Syrinx usually resolves
- Sensory / Motor Recovery
- Depends on tumour biology and resection extent
- Long-term
- Syrinx recurrence implies tumour recurrence
- Treatment
- Subarachnoid decompression, shunt
- Pain Relief
- Variable
- Sensory / Motor Recovery
- Stabilised in most
- Long-term
- Shunting often needed, prone to obstruction
Best prognosis: Chiari I-associated syrinx, short duration of symptoms, no fixed neurological deficit, intact gait, normal hand function.
Poor prognosis: long-standing dense motor deficit, established Charcot joints, post-traumatic aetiology, post-arachnoiditic scarring, recurrent syrinx after multiple shunts.
Key threshold: pain is the most responsive symptom; fixed sensory and motor deficits are stabilised more often than reversed.
Guidelines, Registries & Global Practice
- Prevalence: estimated 8-9 per 100,000 population, with higher rates in tertiary referral centres
- Chiari I: 0.5-1% of MRI series, with smaller numbers progressing to symptomatic syringomyelia
- Post-traumatic: 5-15% of spinal cord injury patients, often delayed years after index injury
- Scoliosis link: 25-50% of paediatric idiopathic scoliosis; up to 90% of atypical curves in some series
- High-resource: cine phase-contrast MRI, intraoperative ultrasound, full neuro-monitoring, and dedicated CSF flow clinics
- Limited-resource: structural MRI plus clinical follow-up; bone-only decompression may be used where duraplasty grafts are limited
- Universal principle: treat the cause first; never fuse a curve through an unrecognised syrinx
- Surgery: foramen magnum decompression is concentrated in tertiary spinal units globally
- Diagnostic emphasis
- Whole-spine MRI plus cine flow study; tonsillar descent greater than 5 mm
- Treatment emphasis
- Foramen magnum decompression plus duraplasty for Chiari I; syrinx shunting reserved for salvage
- Key caution
- Bone-only decompression debated; lower response in adults
- Diagnostic emphasis
- MRI whole neuraxis; brain included to identify hydrocephalus or Chiari
- Treatment emphasis
- Multidisciplinary spina bifida and Chiari clinics; syringo-pleural shunt for non-Chiari syrinx
- Key caution
- Shunt failure rates 20-50% at 5 years - counsel patients carefully
- Diagnostic emphasis
- Standardised MRI protocols; cine flow study where available
- Treatment emphasis
- Cause-directed surgery with selective shunting
- Key caution
- Scoliosis correction requires pre-operative MRI; pedicle screws over sublaminar wires
- Diagnostic emphasis
- MRI mandatory for atypical, painful, or left-thoracic curves
- Treatment emphasis
- Brace while syrinx is treated; staged fusion only after syrinx resolved
- Key caution
- Intra-operative neuro-monitoring; abort and stage if signals change
There is no dedicated international registry for syringomyelia comparable to NJR or AJRR for arthroplasty. The evidence base is dominated by single-centre surgical series and a few landmark imaging-pathogenesis studies (Oldfield, Heiss, Milhorat, Samii). Registry data is therefore drawn from condition-specific databases (Chiari and Syringomyelia Foundation, the Park-Reeves Syringomyelia Research Consortium) rather than from arthroplasty platforms. For orthopaedic outcomes, the Scoliosis Research Society database remains the most useful source for complication rates after scoliosis surgery in syrinx-positive patients.
Record in every patient with suspected or confirmed syringomyelia:
- Dissociated sensory exam with sensory level clearly mapped on a body diagram
- Reflex chart including abdominal reflexes
- MRI whole neuraxis (brain and full spine) with and without contrast
- Cine phase-contrast CSF flow study if Chiari I is suspected
- Multidisciplinary referral to spinal neurosurgery
- Pre-operative MRI and neurology status before any scoliosis correction
A missed syrinx in a patient undergoing scoliosis correction is a recurring source of complaints and claims worldwide. Theatres that perform deformity correction should have a standing rule that any atypical, painful, or left-thoracic curve has a documented whole-neuraxis MRI.
Controversies & Areas of Uncertainty
Some paediatric centres advocate bone-only suboccipital decompression without duraplasty to reduce CSF-related complications, but adults and patients with established syrinx tend to have higher response rates with duraplasty. There is no large randomised trial; choice is surgeon-led and tailored to age, severity, and syrinx behaviour.
Direct syrinx shunting (syringo-subarachnoid, syringo-pleural, syringo-peritoneal) is a salvage option for persistent or expanding syrinx after adequate cause-directed surgery. Shunt failure rates of 20-50% at 5 years limit enthusiasm, and shunting should not be the primary procedure for Chiari I or tumour-associated cases.
Reverse total shoulder arthroplasty is increasingly used for end-stage Charcot shoulder in selected patients with stable neurology, but the failure rate remains higher than in primary osteoarthritis. Glenohumeral arthrodesis remains the most reliable option for the heavily destroyed joint in a young, high-demand patient.
There is no high-quality evidence on how long to wait after syrinx surgery before correcting scoliosis. Most centres perform serial MRI and clinical review, with fusion once the syrinx has stabilised or resolved (often 6-12 months) and the curve is no longer responding to bracing. Decisions remain patient-specific.
MCQ Practice Points
Q: Why does syringomyelia classically cause a cape-distribution sensory loss? A: The crossing spinothalamic fibers in the anterior white commissure are damaged by a central cord cavitation. The C2-T1 fibers travel through the longest vertical segment of the central cord and have the most extensive central representation, so the loss is suspended, bilateral, and cape-shaped. Dorsal column modalities (proprioception, vibration) are spared early.
Q: What is the gold-standard investigation for suspected syringomyelia, and what additional sequences would you request? A: MRI of the whole spine and brain with sagittal T2 of the whole spine, axial T2 at the level of the cavity, T1 pre- and post-gadolinium (to exclude tumour), and cine phase-contrast CSF flow imaging (to assess for Chiari I and foramen magnum obstruction).
Q: A 35-year-old presents with a painless, swollen, warm shoulder. Examination shows preserved range of motion despite gross instability. What is the most likely underlying diagnosis? A: Charcot (neuropathic) arthropathy of the shoulder secondary to syringomyelia. The combination of painless swelling, gross destruction, and preserved movement despite instability is the hallmark. Urgent cervical spine MRI is mandatory to confirm the syrinx.
Q: A 12-year-old presents with a rapidly progressive left-thoracic scoliosis. What imaging must you arrange before considering any surgical correction, and why? A: MRI of the whole neuraxis (brain and entire spine) with contrast. Atypical, painful, or rapidly progressive curves - and left-thoracic curves in particular - have a high prevalence of intraspinal pathology, most commonly syringomyelia with or without Chiari I malformation. Unrecognised syrinx during posterior fusion is a recognised cause of catastrophic intra-operative spinal cord injury.
Q: What is the surgical treatment of Chiari I malformation with associated syringomyelia? A: Foramen magnum decompression (suboccipital craniectomy approximately 3 x 3 cm, C1 laminectomy, sometimes C2) with water-tight duraplasty, often augmented by tonsillar coagulation. The goal is restoration of normal CSF dynamics at the foramen magnum, which leads to syrinx collapse in the majority of cases. Direct syrinx shunting is reserved for the persistent or expanding syrinx despite adequate decompression.
Q: Which symptom of syringomyelia is most likely to improve after surgical treatment? A: Pain is the most responsive symptom (70-80% improvement after foramen magnum decompression). Fixed motor and sensory deficits are stabilised rather than recovered. Established Charcot joint destruction is permanent and does not reverse with syrinx treatment.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 32-year-old teacher presents with 6 months of progressive difficulty using her right hand - she has dropped mugs of hot coffee twice without noticing the temperature. On examination, there is dissociated sensory loss over both shoulders and upper arms, with loss of pin-prick and temperature but preserved vibration and joint position sense. Reflexes are absent in the upper limbs and brisk in the lower limbs with bilateral Babinski signs. The right hand shows small muscle wasting. What is the most likely diagnosis, how do you confirm it, and what is the definitive treatment?”
“A 14-year-old boy is referred with a left-convex thoracic scoliosis. His mother says the curve has progressed rapidly over 6 months despite bracing. He denies pain but his school teacher has noticed that he occasionally drags his left foot. On examination there is a left thoracic rib hump, asymmetric abdominal reflexes (absent on the right), and a subtle broad-based gait. There are no skin stigmata of dysraphism. What is the most important next step, and why does it change the surgical plan?”
Definition and Pathology
- Syringomyelia = fluid cavity within the spinal cord (syrinx)
- Hydromyelia = true dilation of the central canal lined by ependyma
- Most cases are mixed; both are managed identically
- Causes: Chiari I (60-80%), post-traumatic, tumour, arachnoiditis, dysraphic, idiopathic
Clinical Pattern - The Cape
- Dissociated suspended sensory loss over C2-T1 (cape distribution)
- Pain and temperature lost; vibration and proprioception preserved
- Crossing spinothalamic fibers in anterior white commissure damaged first
- LMN signs at syrinx level (wasted hand, absent upper limb reflexes)
- UMN signs below (brisk lower limb reflexes, Babinski)
Imaging
- MRI whole neuraxis (brain plus entire spine) is the gold standard
- T2 sagittal and axial; T1 pre- and post-gadolinium to exclude tumour
- Cine phase-contrast flow study for Chiari I and foramen magnum obstruction
- Serial MRI to track growth (greater than 2-3 mm per year suggests progression)
Management Principles
- Treat the cause: Chiari decompression, tumour resection, arachnoidolysis
- Foramen magnum decompression plus water-tight duraplasty for Chiari I
- Syrinx shunting reserved for persistent or progressive syrinx despite cause treatment
- Surgery stabilises deficits and relieves pain; fixed deficits often do not recover
Orthopaedic Manifestations
- Charcot shoulder: painless swelling, instability, joint destruction - image cervical spine
- Charcot elbow: second most common upper limb neuropathic joint
- Syrinx scoliosis: 25-50% of paediatric idiopathic curves; up to 90% of atypical curves
- MRI whole neuraxis is mandatory before scoliosis surgery in atypical cases
- Sublaminar wires are hazardous in unrecognised syrinx; use pedicle screws
Complications and Red Flags
- Progressive myelopathy, ascending sensory level, neurogenic bladder
- Charcot joint destruction and recurrent burns from loss of protective sensation
- Syrinx scoliosis progression if underlying cause not addressed
- CSF leak and pseudomeningocele after posterior fossa decompression
- Shunt obstruction in 20-50% of syrinx shunts at 5 years
Exam Pearls
- Cape dissociated sensory loss = syringomyelia until proven otherwise
- Painless destroyed shoulder in a young adult = MRI cervical spine
- Left-thoracic curve in a child = MRI whole neuraxis before any fusion
- Pain is the most treatment-responsive symptom; fixed deficits stabilise
- Never correct scoliosis in a patient with an untreated syrinx
Evidence Base and Key Trials
Pathophysiology of syringomyelia associated with Chiari I malformation of the cerebellar tonsils: implications for diagnosis and treatment
- Cine phase-contrast MRI demonstrated obstructed CSF flow at foramen magnum in Chiari I with syrinx
- Cadaveric and clinical evidence supports a piston mechanism - cerebellar tonsils compress cord on each cardiac systole
- Restoration of normal flow after foramen magnum decompression correlates with syrinx collapse
Elucidating the pathophysiology of syringomyelia
- Intraoperative ultrasound and pre/post-operative cine MRI in Chiari I patients
- Successful foramen magnum decompression restored normal CSF dynamics and led to syrinx shrinkage
- Demonstrated that abnormal CSF flow, not congenital central canal dilation, drives syrinx propagation
Chiari I malformation redefined: clinical and radiographic findings for 364 symptomatic patients
- Largest single-centre series redefining Chiari I and classifying syringomyelia
- Tonsillar descent greater than 5 mm below foramen magnum used as diagnostic threshold
- Syrinx patterns stratified by communication with central canal - hydromyelia, non-communicating, extracanalicular
Surgical results of 100 intramedullary tumors in relation to accompanying syringomyelia
- One hundred intramedullary tumours resected; syrinx present in a substantial subset
- Syrinx resolution correlated with extent of tumour resection
- Persistent or recurrent syrinx was a marker of residual or recurrent tumour