Clostridium tetani | Tetanospasmin | Wound Classification | Vaccination + Immunoglobulin
- Tetanus is PREVENTABLE - proper prophylaxis is 95% effective
- Check vaccination history - ask about childhood vaccines AND adult boosters
- Tetanus-prone wounds: more than 6 hours old, puncture, crush, devitalized, contaminated, burns, frostbite
- TIG provides immediate passive immunity (250-500 IU IM) - give at different site from vaccine
- Clean wound, fully vaccinated, less than 5 years = no prophylaxis needed
- “Shorter incubation period = more severe disease (less than 7 days = poor prognosis)
- “TIG does NOT cross blood-brain barrier once toxin is fixed to neurons
- “Vaccination history takes priority over wound type in decision-making
- “Compound fractures and farm injuries are HIGH RISK - give TIG if any doubt
The classic exam (and clinical) failures are: (1) assuming an adult is immune because they "had injections as a child" - childhood doses without adult boosters do not guarantee protection, especially in the elderly and migrants; and (2) forgetting TIG in a tetanus-prone or high-risk wound (open fracture, farm/soil injury, burn) when vaccination is incomplete or unknown. Tetanus is almost entirely preventable, so a missed prophylaxis decision is indefensible.
Overview & Epidemiology
Tetanus is an acute, often fatal neuromuscular disease caused by the exotoxin tetanospasmin, produced by Clostridium tetani - a Gram-positive, spore-forming, obligate anaerobe ubiquitous in soil, dust and animal/human faeces. It is not transmissible person-to-person; spores enter through wounds and germinate in low-oxygen, devitalised tissue. Because it is entirely vaccine-preventable, every wound encounter is an opportunity for prophylaxis.
- Open fractures, crush injuries, farm/soil trauma and burns are classic tetanus-prone wounds
- Prophylaxis is a routine, examinable part of open-fracture management
- Violent spasms can cause vertebral compression fractures, bringing tetanus to the orthopaedic surgeon
- Rare in high-coverage countries; clusters in elderly, under-vaccinated, migrants, people who inject drugs
- Major burden in limited-resource settings (neonatal/maternal tetanus)
- Seroprotection falls sharply after age 60 - the highest-risk group
Pathophysiology
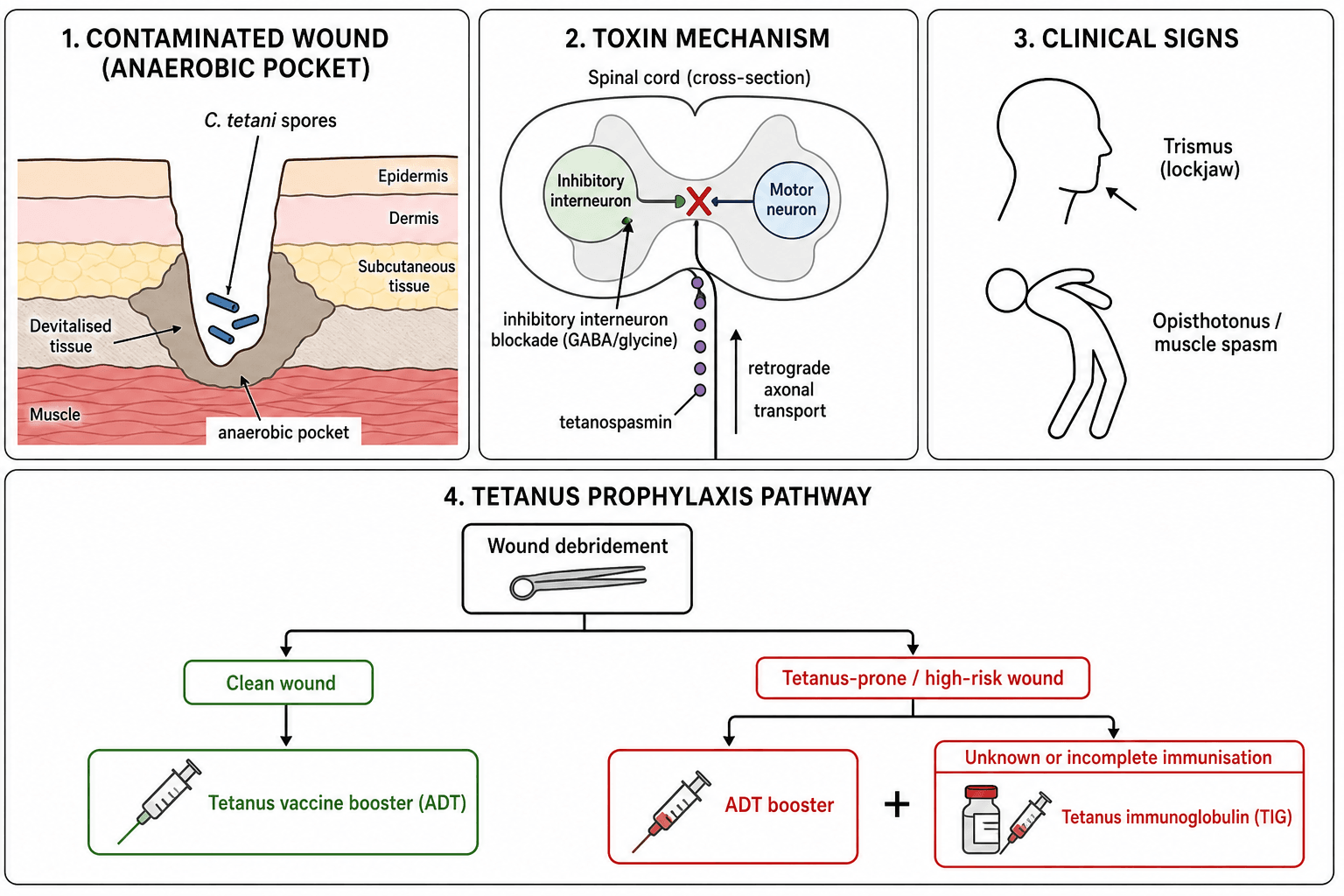
After spores germinate in anaerobic tissue, C. tetani releases tetanospasmin, which enters peripheral motor nerve terminals and undergoes retrograde axonal transport to the spinal cord and brainstem. There it cleaves synaptobrevin (VAMP), blocking release of the inhibitory neurotransmitters GABA and glycine from Renshaw and other inhibitory interneurons.
- Loss of inhibition causes unopposed motor neuron firing leading to rigidity and spasm
- Affects autonomic neurons causing sympathetic overactivity and instability
- Incubation 3-21 days; shorter incubation and onset = more severe disease
- TIG neutralises only circulating, unbound toxin
- Once toxin is internalised and fixed to neurons, it cannot be reversed
- Toxin binding is effectively irreversible - recovery requires growth of new nerve terminals
Both are clostridial toxins that cleave SNARE proteins, but botulinum blocks acetylcholine release at the neuromuscular junction (flaccid paralysis), whereas tetanospasmin blocks inhibitory interneurons centrally (spastic paralysis/rigidity).
Classification of Wounds & Disease
Clean vs Tetanus-Prone vs High-Risk
- Features
- Under 6 hours, linear, superficial, minimal contamination
- Implication
- Booster threshold 10 years; TIG never needed
- Features
- Over 6 hours, puncture, crush, devitalised tissue, soil/faecal contamination, burns, frostbite
- Implication
- Booster threshold 5 years; TIG if incomplete/unknown
- Features
- Heavy contamination, extensive devitalised tissue, delayed surgery, compound fracture
- Implication
- TIG strongly indicated if any doubt; consider 500 IU
Clinical Presentation
Most prophylaxis decisions are made in an asymptomatic patient with a fresh wound - clinical features matter for recognising established disease and the rare patient who presents late.
- Trismus (lockjaw) - earliest sign in most cases
- Risus sardonicus, neck/abdominal rigidity, opisthotonus
- Reflex spasms triggered by light, sound or touch
- Autonomic instability: labile BP, tachycardia, sweating
- Consciousness preserved throughout
- Localised: rigidity confined to the injured region; may precede generalised disease
- Cephalic: cranial nerve involvement after head/neck wounds or otitis; poor prognosis
- Neonatal: floppy then rigid neonate, poor feeding, days after unhygienic cord care
Investigations & Diagnosis
Tetanus is a clinical diagnosis - there is no single confirmatory test, and treatment must not await investigations.
- Role
- Touching posterior pharynx provokes reflex masseter bite (positive) rather than gag
- Caveat
- Supportive bedside test; high specificity reported but not definitive
- Role
- May grow C. tetani
- Caveat
- Negative culture does NOT exclude tetanus; positive does not confirm disease
- Role
- Protective level makes tetanus very unlikely
- Caveat
- Not rapidly available; do not delay treatment
- Role
- Assess rhabdomyolysis, renal function, ventilation
- Caveat
- For severity and complications, not diagnosis
Prophylaxis Products
Available Tetanus Vaccines
- Components
- Diphtheria, tetanus, acellular pertussis
- Indication
- Primary course in infants (2, 4, 6 months)
- Components
- Reduced diphtheria, tetanus, acellular pertussis
- Indication
- Boosters in adolescents and adults
- Components
- Reduced diphtheria + tetanus
- Indication
- Adult booster, wound prophylaxis
- Components
- Tetanus toxoid only
- Indication
- Rarely used alone - combination preferred
ADT (dT) is the standard vaccine for wound prophylaxis in adults - it contains tetanus and reduced diphtheria toxoid. dTpa (Boostrix) adds pertussis and is preferred for booster doses where pertussis protection is also needed, but ADT is equally effective for tetanus prophylaxis.
Vaccination Schedule
- Primary course: 3 doses at 2, 4, 6 months (gives immunity at 6 months)
- Boosters: 18 months, 4 years, 10-15 years (school program)
- Adult boosters: Every 10 years recommended, or at 50 years of age
- Wound booster: Given if more than 5 years (tetanus-prone) or more than 10 years (clean) since last dose
Adverse Effects and the Hazard of Over-Vaccination
The emergency-department audit by Brand and colleagues found that overtreatment (17 percent) was far more common than undertreatment (6 percent), and that a structured protocol reduces both. Understanding why unnecessary tetanus toxoid is harmful - not merely wasteful - is a favourite examiner probe.
- Seen in hyperimmunised patients with already-high antitoxin who receive a booster too soon
- Immune-complex deposition causes a large, painful, sometimes whole-limb local swelling
- Onset a few hours to about a day after the dose; can be severe and mistaken for cellulitis
- A patient given a tetanus-containing dose within the last 5 years does not need a wound booster - repeating one adds reactogenicity without benefit
- Routine over-boosting drives local reactions, fever and injection-site pain
- This is the safety rationale behind the 5-year (tetanus-prone) and 10-year (clean) thresholds
Common, expected and self-limiting reactions to tetanus toxoid are local injection-site pain, redness and swelling, low-grade fever and malaise; genuine anaphylaxis to the toxoid itself is very rare. The practical message mirrors the algorithm: give a booster when the interval justifies it, and resist reflexively boosting a recently vaccinated patient.
When asked why you would withhold a booster from a patient vaccinated three years ago who has a tetanus-prone wound, answer with the Arthus reaction: repeated toxoid in a hyperimmunised person deposits immune complexes and produces an exaggerated, painful local reaction. Adequate immunity plus a within-interval dose means the booster carries risk without benefit.
Differential Diagnosis of Clinical Tetanus
When trismus, rigidity or generalised spasms follow a wound, tetanus must be distinguished from its mimics. The diagnosis is clinical (there is no confirmatory test); the spatula test (touching the posterior pharynx provokes reflex masseter spasm rather than gag) supports it.
- Distinguishing Features
- Trismus, risus sardonicus, opisthotonus, preserved consciousness, autonomic instability; recent wound
- Key Discriminator
- Generalised rigidity WITH retained awareness and normal sensorium
- Distinguishing Features
- Oculogyric crisis, torticollis, after antiemetics/antipsychotics; responds to anticholinergics/benztropine
- Key Discriminator
- Rapid resolution with IV anticholinergic
- Distinguishing Features
- Generalised spasms with full muscle relaxation between episodes; rapid onset
- Key Discriminator
- Complete relaxation between spasms (tetanus retains baseline rigidity)
- Distinguishing Features
- Localised trismus, fever, focal oropharyngeal signs, no generalised rigidity
- Key Discriminator
- Trismus only, with local infective source
- Distinguishing Features
- Carpopedal spasm, Chvostek/Trousseau signs, perioral paraesthesia
- Key Discriminator
- Low ionised calcium; corrects with calcium
- Distinguishing Features
- Hyperthermia, rigidity, altered mental state, drug exposure
- Key Discriminator
- Altered consciousness plus offending drug
- Distinguishing Features
- Insidious axial rigidity, anti-GAD antibodies, no wound or autonomic storm
- Key Discriminator
- Chronic course, autoantibody positive
A crucial discriminator: in tetanus the patient is fully conscious and aware despite agonising spasms, because tetanospasmin acts on motor and autonomic pathways, not cortex. Altered consciousness should redirect you to encephalitis, NMS, serotonin syndrome or metabolic causes.
Management - Prophylaxis Algorithm
1. What type of wound? Clean vs tetanus-prone 2. What is the vaccination history? Fully vaccinated (3+ doses) vs incomplete/unknown
Clean/Minor Wound Algorithm
- ADT Required?
- NO
- TIG Required?
- NO
- ADT Required?
- YES
- TIG Required?
- NO
- ADT Required?
- YES (complete series)
- TIG Required?
- NO
- ADT Required?
- YES (start series)
- TIG Required?
- NO
TIG is NEVER required for clean wounds regardless of vaccination status. The low bacterial inoculum and non-tetanus-prone environment mean the vaccine alone (starting or completing the series) provides adequate protection.
Treatment of Clinical Tetanus
- ICU admission - anticipate respiratory compromise
- TIG 3000-6000 IU IM (or 500 IU intrathecally in some protocols)
- Wound debridement - remove source of toxin
- Metronidazole 500mg IV q8h - kills C. tetani vegetative cells
- Benzodiazepines - diazepam for spasm control
- Airway management - early intubation/tracheostomy
- Quiet, dark environment - reduces spasm triggers
- Nutritional support - NG/PEG feeding
- DVT prophylaxis - prolonged immobility
- Magnesium sulfate - adjunct for spasm/autonomic control
Metronidazole is preferred over penicillin for C. tetani because penicillin is a GABA antagonist and may theoretically worsen tetanus symptoms. Metronidazole has no such effect and is effective against anaerobes.
Complications
- Mechanism
- Laryngospasm, diaphragm/intercostal spasm
- Prevention/Management
- Early intubation, mechanical ventilation
- Mechanism
- Dysphagia, impaired airway protection
- Prevention/Management
- Airway protection, NG feeding, antibiotics
- Mechanism
- Violent muscle spasms - especially thoracic vertebrae
- Prevention/Management
- Muscle relaxants, sedation, supportive care
- Mechanism
- Sympathetic overactivity - hypertension, tachycardia, arrhythmias
- Prevention/Management
- Magnesium, beta-blockers, ICU monitoring
- Mechanism
- Sustained muscle contraction
- Prevention/Management
- IV fluids, monitor CK and renal function
- Mechanism
- Prolonged immobility, ICU admission
- Prevention/Management
- Pharmacological prophylaxis, compression devices
- Mechanism
- Respiratory failure, cardiac complications
- Prevention/Management
- ICU care, early aggressive treatment
Thoracic vertebral compression fractures can occur from violent opisthotonus spasms. This is a well-documented complication and may be the presentation that brings the orthopaedic surgeon into the case. Always consider tetanus in unexplained vertebral fractures with history of recent wound.
Guidelines, Registries & Global Practice
Global Epidemiology
- Vaccine-preventable, still endemic: tetanus persists worldwide, concentrated in low- and middle-income settings with low immunisation coverage and unhygienic wound/birth practices.
- Neonatal/maternal burden: an estimated ~58,000 neonatal deaths per year despite the WHO Maternal and Neonatal Tetanus Elimination Initiative; 24 countries had not eliminated maternal/neonatal tetanus as of 2014.
- High-income pattern: cases are now rare and cluster in older adults, the under-vaccinated, migrants and people who inject drugs - groups with waning or absent immunity.
- Age-related immunity gap: seroprevalence falls sharply after age 60, so the elderly are both more likely to lack protection and to suffer severe disease.
Side-by-Side Guideline Comparison
- Wound risk framing
- Clean-minor vs all other wounds
- Booster / TIG emphasis
- Td/Tdap if greater than 10 yr (clean) or greater than 5 yr (other); TIG if fewer than 3 doses and wound not clean-minor
- Wound risk framing
- De-emphasises strict 6-hour rule; weights contamination, devitalised tissue, mechanism
- Booster / TIG emphasis
- Reinforcing dose by immunisation status; TIG (or IVIG) for tetanus-prone / high-risk if not fully immunised
- Wound risk framing
- Focus on coverage, clean delivery and surveillance for elimination
- Booster / TIG emphasis
- Toxoid-containing vaccine across the life course; TIG/antitoxin where available
- Wound risk framing
- All open fractures and crush injuries treated as tetanus-prone
- Booster / TIG emphasis
- Prophylaxis bundled with debridement and early antibiotics
Despite different wording, all major guidelines converge on two principles: (1) decision = wound type + immunisation history, and (2) TIG is reserved for tetanus-prone / high-risk wounds in the incompletely or unknown-vaccinated. The main divergence is how rigidly the 6-hour cut-off is applied.
High- vs Limited-Resource Practice Variation
- Reduced-antigen combined vaccines (Td/Tdap or dT/dTpa) and human TIG readily stocked
- Routine documentation and electronic immunisation records
- Point-of-care antibody tests increasingly used to avoid unnecessary boosters/TIG
- Human TIG often scarce; equine antitoxin (with hypersensitivity risk) may be the only option
- Plain tetanus toxoid may be used where combination vaccines are unavailable
- Prevention via maternal vaccination and clean delivery is the dominant strategy
Surveillance Rather Than Registries
Unlike arthroplasty, tetanus has no implant registry; surveillance relies on national notifiable-disease systems (e.g. CDC NNDSS, UK UKHSA) and WHO global reporting, which track incidence, vaccination coverage and elimination status to guide programme priorities.
Controversies & Areas of Uncertainty
The classic "more than 6 hours = tetanus-prone" cut-off is convention rather than robust trial data. Several authorities (including UK guidance) now de-emphasise a strict time limit and weight contamination, devitalised tissue and mechanism more heavily. Treat age as one factor, not an absolute rule.
Rapid bedside tetanus immunoassays can reduce unnecessary boosters and TIG in patients with uncertain history. Sensitivity at the protective threshold is imperfect, so a negative quick test should prompt prophylaxis but a positive result is not yet universally trusted to withhold it.
Magnesium reduces sedative and spasm-control drug needs but, in the largest RCT, did NOT reduce ventilation or mortality. Intrathecal/intramuscular human TIG and the optimal therapeutic antitoxin dose remain debated, with limited high-quality evidence.
Some modelling suggests that after a complete childhood primary series plus adolescent and adult boosters, decennial boosters may be unnecessary in low-incidence settings, favouring fewer lifetime doses. Wound-driven boosting remains standard regardless of this debate.
State the conventional teaching first (6-hour rule, decennial boosters), then acknowledge the nuance. Examiners reward candidates who apply the algorithm safely while showing awareness that thresholds are pragmatic conventions, not hard biological constants.
At a Glance - Quick Decision Table
- ADT?
- No
- TIG?
- No
- ADT?
- Yes
- TIG?
- No
- ADT?
- No
- TIG?
- No
- ADT?
- Yes
- TIG?
- No
- ADT?
- Yes (start/complete)
- TIG?
- No
- ADT?
- Yes (start/complete)
- TIG?
- Yes
DIRTYTetanus-Prone Wound - DIRTY
Hook:A wound with any DIRTY feature is tetanus-prone and lowers the booster threshold to 5 years, with TIG added if vaccination is incomplete or unknown.
4 DsTetanus Management - 4 Ds
Hook:The 4 Ds summarise treatment of established tetanus, layered on ICU support, airway control and active immunisation (the disease does not confer immunity).
TRISMUSClinical Tetanus Signs - TRISMUS
Hook:Preserved consciousness with generalised rigidity and stimulus-triggered spasms after a wound is the hallmark of tetanus.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old farmer presents with an open tibial fracture (Gustilo IIIA) after being kicked by a cow. The wound is heavily contaminated with soil and manure. He thinks he had 'some injections as a child' but has not had any boosters. How would you manage tetanus prophylaxis?”
“A 45-year-old woman is having an elective total hip replacement. During pre-assessment, she mentions she received her last tetanus booster 12 years ago after cutting her hand. Should she receive tetanus prophylaxis?”
“An 82-year-old man presents with a closed distal radius fracture after a fall at home. The fracture requires manipulation and K-wire fixation. He has no idea about his vaccination history and has no GP records available. How would you approach tetanus prophylaxis?”
Key Definitions
- Tetanus = disease from tetanospasmin toxin produced by C. tetani
- Clean wound = less than 6 hours, linear, superficial, minimal contamination
- Tetanus-prone = more than 6 hours, puncture, crush, devitalized, contaminated, burns
- Fully vaccinated = 3 or more doses of tetanus toxoid
Wound Assessment (6 DIRTY Ps)
- More than 6 hours old
- Devitalized tissue
- Infected/contaminated (soil, feces, saliva)
- Ragged/stellate configuration
- Tissue loss (burns, frostbite)
- Yielding to depth (puncture), Penetrating foreign body
Clean Wound Prophylaxis
- Fully vaccinated + less than 10 years = NO prophylaxis
- Fully vaccinated + more than 10 years = ADT only
- Incomplete/unknown = ADT (start/complete series)
- TIG is NEVER required for clean wounds
Tetanus-Prone Wound Prophylaxis
- Fully vaccinated + less than 5 years = NO prophylaxis
- Fully vaccinated + more than 5 years = ADT only
- Incomplete (1-2 doses) = ADT + TIG (250-500 IU)
- Unknown vaccination = ADT + TIG (250-500 IU)
TIG Administration
- Dose: 250 IU IM (500 IU for heavy contamination)
- Give at DIFFERENT site from vaccine
- Provides immediate passive immunity
- Cannot neutralize toxin already fixed to neurons
High-Risk Wounds (Always Tetanus-Prone)
- Compound fractures - all Gustilo grades
- Farm/agricultural injuries - soil contamination
- Burns and frostbite - devitalized tissue
- Bite wounds - human, dog, cat
- Gunshot wounds - deep contaminated tracts
Clinical Tetanus Features
- Incubation 3-21 days (shorter = more severe)
- Trismus (lockjaw) - earliest sign
- Risus sardonicus - sardonic smile
- Opisthotonus - arched back
- Spasms triggered by noise, touch, light
Tetanus Treatment
- ICU admission - anticipate respiratory failure
- TIG 3000-6000 IU IM (treatment dose, not prophylaxis)
- Metronidazole 500mg IV q8h (NOT penicillin)
- Wound debridement
- Benzodiazepines for spasms
- Early intubation/tracheostomy
Evidence Base
Population Seroprevalence of Tetanus Immunity
- NHANES III seroprevalence study, n=10,618 persons aged 6 years and older
- Only 69.7% overall had protective antitoxin (greater than 0.15 IU/mL)
- Protection fell from 87.7% (age 6-11) to 27.8% (age 70 and over)
- Excellent vaccination-immunity correlation in 6-year-olds (96% vs 96%)
- Most 1989-90 tetanus cases occurred in adults aged 60 and over
Serotherapy and Antitoxin Dose in Tetanus
- Analysis of 545 US tetanus cases reported 1965-1971
- Antitoxin-treated patients had significantly lower case-fatality than untreated
- Equine antitoxin and human TIG were equally effective
- 500 IU TIG appeared as effective as the then-recommended 3,000-10,000 IU therapeutic dose
- Effect was independent of patient age or race
Metronidazole vs Penicillin in Tetanus Treatment
- Prospective open (non-randomised) trial in 173 patients with moderate tetanus
- Metronidazole group had significantly lower mortality than procaine penicillin
- Metronidazole also gave shorter hospital stay and better treatment response
- Penicillin is a GABA antagonist and may theoretically worsen spasms
- Established metronidazole as the antibiotic of choice for C. tetani
Quality of Wound Tetanus Prophylaxis in Practice
- 620 patients with open soft-tissue injuries across six emergency rooms
- 23% were treated incorrectly (6% undertreated, 17% overtreated)
- Highest-risk patients (tetanus-prone wound, never fully immunised) only 27% correctly treated
- A structured protocol (time, mechanism, contamination, devitalised tissue, depth, immunisation history) improves accuracy
- Protocol-based care reduces both under- and over-treatment without raising cost
References
-
Gergen PJ, McQuillan GM, Kiely M, et al. A population-based serologic survey of immunity to tetanus in the United States. N Engl J Med. 1995;332(12):761-766. doi:10.1056/NEJM199503233321201. PMID: 7862178
-
Ahmadsyah I, Salim A. Treatment of tetanus: an open study to compare the efficacy of procaine penicillin and metronidazole. Br Med J (Clin Res Ed). 1985;291(6496):648-650. doi:10.1136/bmj.291.6496.648. PMID: 3928066
-
Blake PA, Feldman RA, Buchanan TM, et al. Serologic therapy of tetanus in the United States, 1965-1971. JAMA. 1976;235(1):42-44. doi:10.1001/jama.1976.03260270024017. PMID: 946000
-
Brand DA, Acampora D, Gottlieb LD, et al. Adequacy of antitetanus prophylaxis in six hospital emergency rooms. N Engl J Med. 1983;309(11):636-639. doi:10.1056/NEJM198309153091104. PMID: 6888430
-
Thwaites CL, Yen LM, Loan HT, et al. Magnesium sulphate for treatment of severe tetanus: a randomised controlled trial. Lancet. 2006;368(9545):1436-1443. doi:10.1016/S0140-6736(06)69444-0. PMID: 17055945
-
Cook TM, Protheroe RT, Handel JM. Tetanus: a review of the literature. Br J Anaesth. 2001;87(3):477-487. doi:10.1093/bja/87.3.477. PMID: 11517134
-
Thwaites CL, Beeching NJ, Newton CR. Maternal and neonatal tetanus. Lancet. 2015;385(9965):362-370. doi:10.1016/S0140-6736(14)60236-1. PMID: 25149223
-
Rodrigo C, Fernando D, Rajapakse S. Pharmacological management of tetanus: an evidence-based review. Crit Care. 2014;18(2):217. doi:10.1186/cc13797. PMID: 25029486
-
Centers for Disease Control and Prevention. Tetanus: For Clinicians. CDC. 2024. Available at: cdc.gov/tetanus/clinicians.html
-
UK Health Security Agency. Tetanus: The Green Book, Chapter 30. 2024. Available at: gov.uk/government/publications/tetanus-the-green-book-chapter-30
-
World Health Organization. Tetanus vaccines: WHO position paper. Wkly Epidemiol Rec. 2017;92(6):53-76.