Total Hip Arthroplasty: Dislocation
1-5% primary THA, posterior most common - Lewinnek safe zones, larger heads, dual mobility
- Lewinnek safe zones: inclination 40±10°, anteversion 15±10°, combined 25-45°
- Posterior dislocation most common (75-80%) - hip flexed, adducted, internally rotated
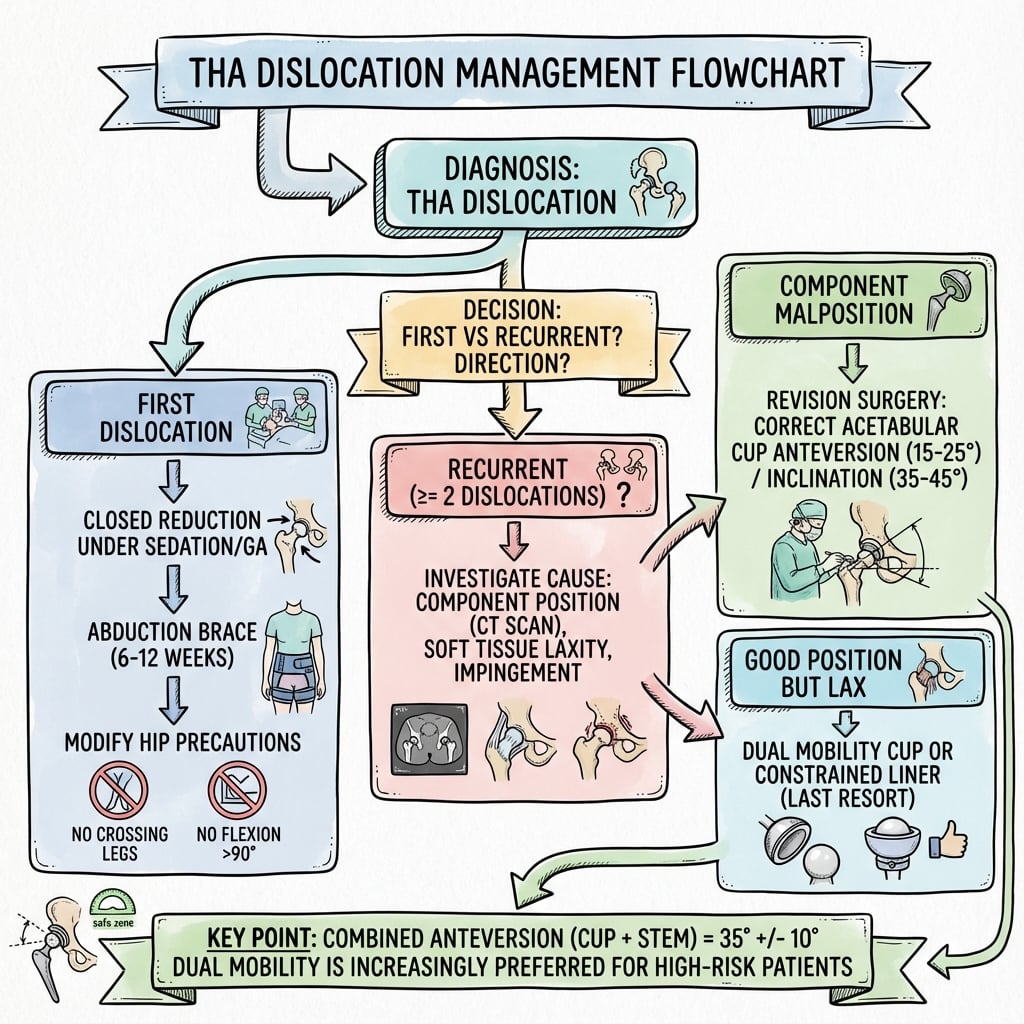
- First dislocation: closed reduction + hip brace, identify cause
- Recurrent: revision surgery - liner exchange, larger head, dual mobility, component revision
- Prevention: optimal positioning, head 36mm or larger, dual mobility in high risk
- “50% of dislocations occur within 3 months - early risk period
- “Posterior approach has 2-3x higher dislocation rate than anterior/anterolateral
- “CT scan best for assessing component version and impingement
- “Dual mobility cups indicated for revision, cognitive impairment, and neuromuscular disease
Images


At a Glance
THA dislocation occurs in 1-5% of primary cases, predominantly posterior direction (75-80%) with hip flexed, adducted, and internally rotated. Risk factors follow the 4 P's: Patient (age over 70, cognitive impairment, neuromuscular disease), Procedure (posterior approach 2-3× higher risk, revision), Position (component malposition), Power (inadequate soft tissue tension). Lewinnek safe zones: inclination 40±10°, anteversion 15±10°; combined anteversion 25-45° (cup + stem) is widely regarded as the most critical parameter. Prevention strategies: head size 36mm or larger (RCT-supported), meticulous posterior soft tissue repair (reduces risk substantially), and dual mobility cups for high-risk patients. First dislocation: closed reduction, identify cause with CT for component version, hip brace. Recurrent dislocation (25-50% recurrence after first event) usually requires revision — liner exchange, dual mobility, constrained liner, or component revision depending on cause. Registry data show dislocation/instability is among the leading indications for early revision.
DISLOCATEDISLOCATE - THA Dislocation Risk Factors
Hook:Think of what makes a hip DISLOCATE - covers surgical, patient, and component factors.
STABLE HIPSTABLE HIP - Dislocation Prevention Strategy
Hook:Remember what makes a HIP STABLE - covers component, soft tissue, and patient factors for comprehensive prevention.
REVISEREVISE - Management of Recurrent THA Dislocation
Hook:When dislocation recurs, you need to REVISE - both your assessment and potentially the components.
Overview
Definition and Significance
THA dislocation is complete loss of contact between the femoral head and the acetabular component — a devastating complication with significant impact on patient function, satisfaction, and healthcare costs.
Key Epidemiological Data:
- Primary THA dislocation rate: 1-5% (varies by approach and surgeon experience)
- Revision THA dislocation rate: 10-25%
- Recurrence after first dislocation: 25-50%
- Among the leading causes of early revision in joint replacement registries
- Peak incidence in first 3 months post-operatively (50% of all dislocations)
Clinical Impact: severe pain and disability, emergency presentations, need for closed reduction under sedation, high recurrence risk, psychological trauma and fear of movement, potential for revision surgery, and reduced patient satisfaction scores.
1-5% overall dislocation rate
Posterior approach: 2-5%
Anterior approach: 0.5-2%
Higher in first-time surgeons
10-25% dislocation rate
Previous instability: 25%+
Multiple revisions: Even higher
Major risk factor for further revision
50% in first 3 months
30% in 3-12 months
20% after 1 year
Late dislocations suggest component wear or loosening
Pathophysiology
Hip Joint Stability Mechanisms
Understanding normal hip stability is essential for preventing and managing THA dislocation.
Osseous Factors:
- Acetabular coverage: native acetabulum covers 170-180° of the femoral head
- THA cup coverage: typically 150-170° (trade-off with range of motion)
- Femoral head-neck ratio: larger heads provide greater jump distance
- Impingement-free arc: determined by component design and positioning
Soft Tissue Stabilizers:
Static Stabilizers:
- Joint capsule: primary restraint to dislocation
- Iliofemoral ligament (Y-ligament of Bigelow): strongest, prevents hyperextension
- Ischiofemoral ligament: prevents internal rotation in extension
- Pubofemoral ligament: prevents abduction and external rotation
- Acetabular labrum: deepens socket (not present in THA)
Dynamic Stabilizers:
- Gluteus medius and minimus: anterior fibers prevent anterior dislocation
- Short external rotators: posterior capsule reinforcement (piriformis, obturators, gemelli)
- Iliopsoas: anterior stabilizer
- Adequate muscle tension and activation
THA-Specific Stability Factors:
Component Factors: head size (larger heads increase jump distance and impingement-free arc), head-neck ratio (lower ratio increases range before impingement), neck-cup impingement (most common cause of mechanical dislocation), liner design (elevated/lipped liners increase coverage), and offset (restores abductor moment arm and soft tissue tension).
Positioning Factors: acetabular inclination (affects superior/medial coverage), acetabular anteversion (affects anterior/posterior coverage), femoral anteversion (works with cup version for combined stability), leg length (provides soft tissue tension), and lateral offset (tensions abductors).
Pathophysiology by Direction
Posterior Dislocation (75-80%): most common after posterior approach. Mechanism: hip flexion + internal rotation + adduction (sitting to standing, low chairs, tying shoes). Caused by posterior capsule disruption or inadequate repair, posterior wall deficiency, or external rotator insufficiency.
Anterior Dislocation (15-20%): more common after anterior/anterolateral approach. Mechanism: hip extension + external rotation (stepping backward, arising from bed). Caused by anterior capsule disruption, excessive acetabular anteversion, or psoas impingement on the anterior neck.
Superior Dislocation (rare): requires significant force or component failure; associated with severe abductor dysfunction, loosening, or catastrophic wear.
Component Malposition Leading to Dislocation:
- Acetabular cup: excessive inclination over 50° (reduced superior coverage, posterior instability); insufficient inclination under 30° (medial impingement); excessive anteversion over 25° (anterior instability); insufficient anteversion under 5° or retroversion (posterior instability).
- Femoral component: excessive anteversion (anterior instability), retroversion (posterior instability), varus positioning or undersized stem (reduced offset and soft tissue tension).
- Combined version: combined anteversion outside 25-45° increases risk; appropriate femoral version can compensate for borderline cup position, so both components must be considered together.
Lewinnek Safe Zones
EXAMINER FAVOURITE: "A patient dislocates despite cup position within Lewinnek safe zones - why?" Answer: safe zones are statistical concepts, not absolute. Other factors matter: combined anteversion, spinopelvic mobility / functional safe zone, impingement, soft tissue tension, patient factors (compliance, neuromuscular disease), and component design (head size, offset). A substantial proportion of dislocations occur in the "safe zone."
Classification
THA Dislocation Classification
By Direction:
- Posterior (75-80%) - most common, especially with posterior approach
- Anterior (15-20%) - more common with anterior approach
- Superior/inferior (rare)
By Timing:
- Early (less than 3 months) - 50% of dislocations; usually component malposition, soft tissue laxity, technique, or incomplete healing
- Intermediate (3-12 months) - borderline component position, emerging abductor dysfunction, variable compliance
- Late (greater than 1 year) - consider polyethylene wear, component loosening, soft tissue attenuation, new neurological issues
- Recurrent (2 or more dislocations)
| Type | Mechanism | Clinical Features |
|---|---|---|
| Posterior | Hip flexion, adduction, internal rotation | Leg shortened, internally rotated, adducted |
| Anterior | Hip extension, external rotation, abduction | Leg externally rotated, abducted |
| Early (less than 3 months) | Soft tissue healing, positioning, compliance | Usually single episode, often responds to conservative care |
| Late/Recurrent | Component malposition, wear, abductor dysfunction | Often requires surgical revision |
| Approach | Dislocation Rate | Peak Risk Period | Protective Strategies |
|---|---|---|---|
| 2-5% (historically higher) | First 6 weeks | Posterior soft tissue repair, larger heads ≥36mm, combined anteversion optimization | |
| 0.5-2% (lowest rate) | First 3 months | Preserve anterior capsule, avoid excessive ER, table positioning awareness | |
| 1-3% (intermediate) | First 3 months | Repair gluteus medius, avoid abductor damage, optimize tension | |
| 10-25% (any approach) | First 3 months | Consider dual mobility, constrained liners in high risk |
Risk Factors
Patient Risk Factors
Demographic: age over 70 years (2-3x risk), female sex (1.5-2x; lower muscle mass, anatomical factors), BMI at either extreme (under 20 or over 35), and frailty (significant independent risk factor).
Neuromuscular (highest risk): Parkinson's disease, prior stroke with residual deficit, cerebral palsy and other neuromuscular disorders, cognitive impairment or dementia (3-4x risk), alcohol/substance abuse and psychiatric disorders (non-compliance).
Medical/anatomical: previous ipsilateral hip surgery (2-3x risk), developmental dysplasia (DDH), prior femoral fracture (altered anatomy), inflammatory arthropathy (soft tissue quality), and abductor muscle damage or denervation (critical stability loss).
Surgical Risk Factors
Approach: posterior 2-5% (higher without soft tissue repair, 1-2% with enhanced repair); anterolateral 1-3%; direct anterior 0.5-2%; revision 10-25% regardless of approach.
Component-related:
- Acetabular cup: malposition outside Lewinnek zones (2-4x risk), excessive inclination over 50°, excessive anteversion over 25°, retroversion, or insufficient anteversion under 5°.
- Femoral: excessive anteversion or retroversion, undersized stem, varus positioning (reduced offset/tension).
- Bearing/head: head size under 32mm (2-3x risk vs 36mm); 28mm heads highest risk (largely abandoned); low head-neck ratio (impingement); modular necks (malposition if misassembled).
Technical: inadequate soft tissue repair (especially posterior capsule and external rotators), failure to restore offset, leg length discrepancy (over- or under-lengthening), unrecognized intraoperative instability, and abductor muscle damage (superior gluteal nerve injury, detachment).
Component Positioning:
- Cup inclination: 30-50° (outside this: risk increases 2-4x)
- Cup anteversion: 5-25° (outside this: risk increases 2-4x)
- Combined anteversion: 25-45° (most important parameter)
Head Size Impact:
- 28mm vs 36mm: ~3x higher dislocation risk (RCT: 5.4% vs 1.3%)
- 32mm vs 36mm: intermediate risk
- Dual mobility: markedly lower dislocation than standard bearings in high-risk groups
Recurrence Risk:
- After 1st dislocation: 25-50% recurrence rate
- After 2nd dislocation: 60-75% recurrence rate
- After 3rd dislocation: over 80% recurrence rate
Time Distribution:
- 0-3 months: 50% of all dislocations
- 3-12 months: 30% of all dislocations
- Over 12 months: 20% of all dislocations
Consider Dual Mobility or Constrained Liner:
- Prior THA dislocation (same hip)
- Neuromuscular disease (Parkinson's, stroke)
- Severe cognitive impairment
- Abductor deficiency or damage
- Revision for instability
- Tumor resection with soft tissue loss
These patients may need enhanced stability implants prophylactically.
Modify Surgical Technique:
- Age over 75 years
- Revision THA (non-instability)
- Previous hip surgery (fracture, prior arthroplasty)
- DDH with anatomical abnormalities
- Inflammatory arthropathy
- Posterior approach in high-risk patient
Consider larger heads, meticulous soft tissue repair, component position optimization.
Clinical Presentation
History and Examination
Acute Dislocation History: sudden severe hip pain after a precipitating movement or fall, sensation of "something went out," inability to move the leg or weight bear, and previous episodes if recurrent. Mechanism — posterior (sitting to standing, low chair, tying shoes, getting out of car); anterior (stepping backward, arising from bed, external rotation); traumatic (fall or impact).
Physical Examination:
- Posterior (most common): hip flexed, adducted, internally rotated; leg shortened 1-3cm; greater trochanter prominent; severe pain with movement; unable to straight leg raise.
- Anterior: hip extended, abducted, externally rotated; leg may appear lengthened or neutral; femoral head occasionally palpable in groin.
Neurovascular Examination (CRITICAL): assess and document the sciatic nerve — ankle dorsiflexion (common peroneal), plantarflexion (tibial), and sensation over the dorsal and plantar foot — before any reduction attempt. Sciatic nerve injury occurs in 10-20% of posterior dislocations (usually neuropraxia, occasionally permanent). Assess femoral nerve in anterior dislocations. Document pulses. Repeat the examination after reduction.
CRITICAL SAFETY: Always perform and document a complete neurovascular examination before attempted reduction. Sciatic nerve injury occurs in 10-20% of posterior THA dislocations. Document specific testing of ankle dorsiflexion (common peroneal) and plantarflexion (tibial), plus sensation in the dorsum and plantar foot. Repeat the examination after reduction.
Investigations
Plain Radiography
AP Pelvis (essential): both hips for comparison; confirm dislocation direction; measure cup inclination (angle between cup opening plane and inter-teardrop line; normal 40° ± 10°); compare with immediate post-op films; look for migration, loosening, polyethylene wear, periprosthetic or acetabular wall fracture, and heterotopic ossification.
Lateral Hip (cross-table or frog lateral): estimate cup anteversion (ellipse method; CT more accurate; normal 15° ± 10°); assess anterior/posterior wall integrity and femoral component profile.
Post-Reduction Films (mandatory): confirm concentric reduction (no subluxation, Shenton's line), assess for new iatrogenic fractures, and document the final component relationship as a baseline.
Computed Tomography
CT is often essential for recurrent dislocation or revision planning. Protocol: thin (1-2mm) cuts of pelvis and proximal femur to below the lesser trochanter, with 3D reconstruction.
- Acetabular measurements: inclination (coronal reconstructions), anteversion (axial cuts at the superior dome; angle between acetabular opening plane and the AP pelvic axis), bone stock assessment.
- Femoral measurements: femoral neck/stem version (angle between neck axis and posterior femoral condyles).
- Combined anteversion: acetabular AV + femoral AV; target 25-45°. McKibbin's combined index (traditional) is acetabular AV + femoral AV = 37° ± 10°.
- Impingement assessment: anterior (psoas tendon, anterior rim), posterior (ischium, posterior wall, component-component), with software-based detection where available.
- 3D reconstruction: useful in complex anatomy (DDH, revision), surgical planning, bone defect identification, and consent.
Additional Investigations
- Laboratory/aspiration: not routine; obtain ESR/CRP and aspirate (cell count, culture, alpha-defensin) if infection is suspected before revision.
- MARS MRI: rarely needed; useful to assess abductor integrity or soft tissue pathology.
- Neuromuscular: formal neurology consult and EMG/NCS (at 3-4 weeks) for persistent sciatic deficit; physiotherapy assessment of abductor function.
Lewinnek Safe Zones (Traditional):
- Cup Inclination: 40° ± 10° → 30-50°
- Cup Anteversion: 15° ± 10° → 5-25°
Combined Anteversion (More Important):
- Target: 25-45°
- Under 25°: Posterior instability risk
- Over 45°: Anterior instability risk
- Formula: Acetabular AV + Femoral AV
Danger Zones:
- Cup Inclination over 55°: High risk
- Cup Inclination under 25°: Impingement
- Cup Retroversion: Very high posterior risk
- Combined AV under 20° or over 50°: High risk
EXAMINER TRAP: "How do you measure acetabular anteversion on AP pelvis X-ray?" WRONG ANSWER: "You can't, need CT or lateral view." CORRECT ANSWER: "While CT is gold standard, you can estimate using a lateral radiograph with the ellipse method, but this has significant error. For recurrent instability, I would get a CT for precise 3D measurement of both acetabular and femoral version to calculate combined anteversion, which is the most important parameter."
Management
Immediate Management of Acute Dislocation
ED Assessment and Stabilization: analgesia (IV opioids, procedural sedation for reduction); neurovascular examination and documentation; AP pelvis and lateral hip radiographs; NPO in preparation for sedation; contact orthopaedic surgeon; review operative notes and post-op films.
Closed Reduction:
- Indications: all acute THA dislocations unless contraindicated; perform as soon as feasible (within 6 hours ideal).
- Contraindications: associated acetabular/femoral fracture requiring fixation, gross component loosening, suspected infection.
- Allis method (posterior): adequate sedation or GA; patient supine; assistant stabilizes pelvis with downward pressure on ASIS; surgeon flexes hip and knee to 90°; inline traction with gentle internal rotation and rocking; palpable clunk indicates reduction; test stability; post-reduction films.
- Stimson technique: patient prone, hip off bed edge flexed to 90°, gravity-assisted with gentle downward pressure on the calf.
- Anterior reduction: inline traction with hip extended and gentle internal rotation; direct pressure on the head may assist (more difficult than posterior).
Post-Reduction Protocol: repeat neurovascular exam and document changes; AP pelvis and lateral hip films; confirm concentric reduction; test the safe arc of motion; document the direction of instability.
Admission vs Discharge: first dislocation with stable reduction and good support may be discharged; admit for recurrent dislocation, persistent instability, new neurovascular deficit, or failed closed reduction.
Direction-Specific Hip Precautions:
- Posterior: avoid flexion beyond 90°, adduction past midline, and internal rotation; no low chairs/couches; elevated toilet seat; sleep supine or on the contralateral side; minimum 6 weeks, often 12.
- Anterior: avoid extension beyond neutral and external rotation; no reaching backward while standing; 6-12 weeks.
POST-REDUCTION MONITORING: After closed reduction, the patient MUST have a repeat neurovascular exam documented. New or worsening sciatic nerve deficit may indicate nerve entrapment and requires urgent repeat imaging and possible open reduction. Do not discharge until stability is confirmed and the patient can safely mobilize with precautions.
Surgical Technique
Principles of Revision for Instability
Pre-Operative Planning: CT with 3D reconstruction; precise cup inclination/version and femoral version; combined anteversion calculation; identify malpositioned component(s); assess bone stock; plan target positions. Have a full revision system available — dual mobility components, constrained liners (backup), larger heads, and augments for bone defects. Approach is usually the same as the index surgery (most commonly posterior), with extensile exposure if needed.
Indications: recurrent instability with a well-positioned, stable acetabular shell (inclination 30-50°, anteversion 5-25°), no wear/osteolysis, and combined anteversion correctable by head size or femoral change.
Pre-Operative Assessment: confirm shell stability and exact position on CT; verify liner type/modularity; document shell manufacturer and size.
Technique: use the previous approach; take down the capsular repair; expose and confirm shell stability; remove the liner with dedicated tools (protect threads/taper); inspect the shell. Select the largest head possible (36-40mm) and consider an elevated/lipped liner (oriented posteriorly for posterior instability) or a dual mobility liner if the shell is compatible and the patient is high-risk. Clean the taper/locking mechanism, ensure correct orientation, impact fully, and verify the locked position. Assess the femoral component and taper; exchange the head for a larger size if appropriate. Perform meticulous posterior soft tissue repair, then test stability through full range — if unstable, convert to dual mobility or constrained.
Outcomes/Complications: success 70-85% if the shell is well positioned (lower if borderline); dual mobility liners outperform standard liners. Recurrent instability 15-30%; risks include intraoperative shell loosening, liner-shell incompatibility, and inadequate available head size.
VIVA SCENARIO: "Patient with 3 dislocations, CT shows cup at 55° inclination, 25° anteversion. What do you do?" ANSWER FRAMEWORK: (1) Cup malpositioned (excessive inclination) → primary problem; (2) Revision surgery indicated — cannot treat non-operatively; (3) Cup revision to target 40° inclination with combined AV 25-45°; (4) Use dual mobility at the time of revision given recurrent instability; (5) Alternative: constrained liner if the cup cannot be revised, but higher failure rate. This demonstrates systematic problem identification and an evidence-based solution.
Complications
Recurrent Dislocation
Two or more episodes; occurs in 25-50% after a first dislocation, rising to 60-75% after a second. Drivers include non-compliance, neuromuscular/cognitive decline, unrecognized component malposition, failure to address the underlying cause, inadequate soft tissue repair, inappropriate head size, and uncorrected impingement. Management: systematic CT-based workup, revision surgery typically after the second dislocation, correction of the underlying cause, and an enhanced stability construct (dual mobility preferred). Non-operative treatment rarely succeeds.
Sciatic Nerve Injury
Occurs in 10-20% of acute dislocations (usually neuropraxia; permanent deficit 1-2%). The common peroneal division is most affected — foot drop, numbness over the dorsal foot and first web space, high-steppage gait; the tibial division causes plantarflexion weakness and plantar numbness. Document detailed motor/sensory exam before and after reduction; if a deficit worsens after reduction, consider nerve entrapment (urgent MRI/exploration). Manage with gentle reduction, AFO for foot drop, and physiotherapy. EMG/NCS at 3-4 weeks if persistent. Neuropraxia recovers in 80-90% over 6-12 months; consider tendon transfer (posterior tibial for foot drop) if no recovery by 12-18 months.
Periprosthetic Fracture
Posterior wall acetabular fracture is the most common fracture with posterior dislocation — may be occult on plain films, often needs CT. Small stable fragments are treated non-operatively; large fragments (over 25-30% of the wall) require ORIF and may need a larger head or dual mobility for stability. Femoral periprosthetic fractures (Vancouver classification) are rare and may occur during reduction — use gentle technique. Iatrogenic fractures during revision (greater trochanter, acetabulum, femur) require intraoperative recognition and fixation.
Component Wear and Loosening
Recurrent dislocation causes repetitive bearing trauma, accelerating polyethylene wear and potential osteolysis; constrained liners increase cup-bone interface forces and can accelerate loosening. Assess with serial radiographs (progressive radiolucent lines, migration, osteolysis, changing position). Late dislocation may reflect wear and laxity or component migration. Aseptic loosening requires revision; correct malposition and address wear (larger heads, dual mobility, highly cross-linked polyethylene) at the same time.
Psychological Impact
Fear of recurrence, anxiety about movement, depression, reduced quality of life, and self-imposed activity restriction are common. Manage with education, realistic expectations, psychological support where needed, supervised graded return to activity, and emphasis on what the patient can do safely.
Prevention Strategies
Surgical Technique Optimization
Component Positioning (most important):
- Acetabular: target 40° inclination, 15° anteversion (Lewinnek), but prioritise combined anteversion 25-45° individualised to femoral version; use navigation where available; avoid inclination over 50° and retroversion.
- Femoral: restore native version (typically 10-15° anteversion), combined with cup version for 25-45° total; restore offset and appropriate leg length for soft tissue tension.
Head Size: minimum 32mm in modern practice, 36mm for most patients, 40mm for high-risk if the acetabulum allows; never use 28mm. Larger heads increase jump distance and impingement-free arc, with diminishing returns and taper-corrosion concerns above 40mm.
Soft Tissue Management:
- Posterior approach: meticulous repair of the posterior capsule and short external rotators to the greater trochanter (transosseous or anchors) is mandatory and substantially reduces dislocation; consider capsular plication if lax; trochanteric slide in complex revisions.
- Anterolateral: anatomic gluteus medius repair, avoid superior gluteal nerve injury, restore abductor tension.
- Direct anterior: preserve the anterior capsule, avoid excessive external rotation, avoid anterior notching.
Offset and Leg Length: restore native offset (±5mm); lateral offset tensions the abductors for dynamic stability; avoid over-lengthening (dissatisfaction, nerve injury) and shortening (instability).
Intraoperative Stability Testing (essential): with trial components, confirm stability in flexion 90° + internal rotation + adduction (posterior) and extension + external rotation (anterior); assess the impingement-free arc; never accept instability at closure — modify position or increase head size immediately.
Pre-Operative Risk Stratification
- Very high risk (consider enhanced stability implants): prior THA dislocation, neuromuscular disease, severe cognitive impairment/dementia, abductor deficiency, revision for instability, tumor resection with soft tissue loss, multiple prior hip surgeries, age over 80 with frailty. Plan: dual mobility (primary or revision), consider direct anterior if experienced, larger head if standard bearing, extended rehabilitation.
- Moderately high risk (modify technique): age 70-80, non-instability revision, prior hip surgery, DDH, inflammatory arthropathy, morbid obesity, milder neuromuscular disease. Plan: head ≥36mm, meticulous soft tissue repair, extended precautions (12 weeks), abduction brace, enhanced education.
Patient Education and Enhanced Recovery
Pre-operative precautions teaching (video/demonstration, written materials), realistic expectations, and home-hazard planning. Post-operatively, deliver direction-specific precautions, early mobilization with an assistive device, abductor strengthening (critical for dynamic stability), and home safety assessment. High-risk patients use a hip abduction brace 6-12 weeks. Maintain lifelong awareness of high-risk positions and the need for urgent review if instability is suspected.
Component Positioning:
- Cup Inclination: 35-45° (narrower than Lewinnek for optimal stability)
- Cup Anteversion: 15-20° (middle of Lewinnek range)
- Combined Anteversion: 35-40° (middle of 25-45° range for safety margin)
Head Size:
- Standard risk: ≥36mm
- High risk: 36-40mm or dual mobility
- Never: Under 32mm in modern practice
Offset Restoration:
- Target: ±5mm of native offset
- Lateral offset critical for abductor tension
Soft Tissue Repair:
- Posterior approach: enhanced repair substantially reduces dislocation
- Capsular repair with heavy suture (No. 2 or 5)
- Short external rotators to bone (transosseous or anchors)
Postoperative Care
Immediate Period (0-6 weeks)
Hip precautions from day 0 with an abduction pillow/brace if high risk; neurovascular checks (especially after closed reduction); multimodal analgesia; VTE prophylaxis per protocol; early mobilization with a walker. Discharge once safe mobilization is achieved, with assistive devices (elevated toilet seat, reacher, sock aid, long shoe horn). First review at 1-2 weeks with wound check and radiographs to exclude early dislocation. Continue strict precautions and wean the assistive device as strength improves.
Intermediate Period (6-12 weeks)
Week 6: clinical and radiographic review, Trendelenburg assessment, begin weaning the abduction brace, and gradually liberalise activity. Weeks 6-12: progressive strengthening, low-impact activity (walking, swimming, cycling), and driving when safe. Week 12: final short-term review — discontinue formal precautions if low risk and stable, with lifelong awareness of extreme positions.
Long-Term Follow-Up
3-6 months: return to unrestricted activity if stable; maintenance abductor strengthening. 1 year and annually thereafter: clinical and radiographic surveillance for late dislocation, wear, and loosening; lifelong follow-up is recommended for all THA.
Red flags for urgent evaluation: sensation of instability or near-dislocation, acute dislocation, new severe pain, leg-length change, inability to weight bear, or new neurological symptoms.
After Closed Reduction for Dislocation:
- Repeat neurovascular exam (document)
- Post-reduction radiographs (confirm concentric reduction)
- Hip abduction brace fitting
- Strict hip precautions education
- Admit vs discharge (depends on stability, support)
- Follow-up 1-2 weeks for assessment
- CT scan if recurrent (identify cause)
- Plan revision surgery if malposition identified
Critical to identify the underlying cause and not just treat the symptom.
After Revision for Instability:
- Hip abduction brace 12 weeks (strict)
- Protected weight bearing 6 weeks if bone work
- Hip precautions minimum 12 weeks
- Serial radiographs: 6 weeks, 3 months, 6 months, 1 year
- Close monitoring for recurrence
- Enhanced rehabilitation
- Long-term annual follow-up
- Higher vigilance for complications
Revision patients have higher recurrence risk and need enhanced follow-up.
Outcomes
Outcomes by Treatment Strategy
- Non-operative (first dislocation): no-recurrence rate 50-75%; better with well-positioned components, traumatic mechanism, and good compliance; worse with malposition, atraumatic mechanism, neuromuscular disease, or cognitive impairment.
- Isolated liner exchange: 60-80% success if the cup is well positioned; better with larger heads and dual mobility liners; fails if underlying malposition is not addressed.
- Acetabular revision: 80-90% success with dual mobility, 70-85% with a standard large head; achieving combined anteversion 25-45° is critical.
- Dual mobility: dislocation 0.5-2% (primary use), 2-5% (revision); intraprosthetic dislocation 0.5-1%; best outcomes for recurrent instability in current evidence.
- Constrained liners: mechanical prevention 80-90% but reoperation 15-25% for locking ring failure/loosening — less favourable than dual mobility; salvage option.
| Intervention | Re-dislocation Rate | Satisfaction |
|---|---|---|
| Closed reduction + bracing | 30-40% | Variable, depends on recurrence |
| Component revision | 10-20% | Good if cause addressed |
| Constrained liner | 10-15% at 5 years | Good stability, some functional limitation |
| Dual mobility | 2-5% | Excellent stability |
Recurrent dislocations (3 or more), abductor deficiency, cognitive impairment, non-compliance with precautions, and neuromuscular disease all predict a poorer outcome and a higher chance of failure after intervention.
Evidence Base
- Series of 300 THAs; 9 (3%) dislocated
- Cup anteversion 15° ± 10° and lateral opening (inclination) 40° ± 10° defined the 'safe range'
- Dislocation rate 1.5% within the safe range vs 6.1% outside it
- Greatest risk in the first 30 days; higher risk in hips with prior surgery
- Multicentre RCT of 644 patients randomised to 36mm vs 28mm metal-on-highly-cross-linked-polyethylene
- Overall 1-year dislocation: 1.3% (36mm) vs 5.4% (28mm), p=0.012
- Primary THA: 0.8% (36mm) vs 4.4% (28mm), p=0.024
- Revision subgroup 4.9% vs 12.2% (not significant - small sample)
- Two surgeons adopted an identical enhanced posterior soft tissue repair via the posterior approach
- Surgeon 1: dislocation fell from 4% (395 hips) to 0% (395 hips) after enhanced closure
- Surgeon 2: dislocation fell from 6.2% to 0.8% after enhanced closure
- Differences highly statistically significant
- 320 navigated primary THAs; 92.5% were within the Lewinnek safe zone
- Of hips within Lewinnek, 14.2% fell outside the sagittal functional safe zone (combined sagittal index)
- These patients were considered at risk for dislocation despite 'normal' cup angles
- Best predictor of falling outside the functional safe zone was femoral/spinopelvic mobility, not cup position
- Systematic review and meta-analysis of comparative studies in revision THA
- Dual mobility had a significantly lower dislocation rate than fixed-bearing cups
- Dual mobility also showed better overall implant survivorship and lower aseptic loosening risk
- No significant difference in infection risk between groups
- 23 studies, 7,189 patients (mean age 77.8 years) treated with dual mobility THA for femoral neck fracture
- Dislocation significantly lower vs conventional THA (OR 0.26) and hemiarthroplasty (OR 0.27)
- Intraprosthetic dislocation rate only 0.04% (3 of 7,189)
- No increase in other complications
- Six arthroplasty registries (Australia, Denmark, Sweden, Netherlands, UK, USA): 15,024 dual mobility vs 97,200 conventional THAs for hip fracture
- No reduction in all-cause revision for dual mobility (HR 0.96, 95% CI 0.86-1.06) at 5 years
- Lower proportion revised for dislocation (0.9% vs 1.4%) but higher proportion revised for infection (1.2% vs 0.8%)
- Dual mobility use rose to 21% of fracture THAs by 2019, with wide between-country variation
Guidelines, Registries & Global Practice
Global Epidemiology and Registry Evidence
Instability/dislocation is consistently among the leading early indications for revision THA across major national registries (AOANJRR, NJR for England/Wales, AJRR, Swedish/Nordic registries). Registry data converge on several practice-changing signals:
- Approach: posterior approach carries a higher early dislocation/revision rate than direct anterior in most registries; the gap narrows substantially with enhanced posterior soft tissue repair.
- Head size: heads ≥36mm have lower dislocation than 28-32mm; 28mm is now rarely used in modern primary THA.
- Dual mobility: lowers revision for dislocation specifically, but international registry meta-analysis (Farey 2022, including AOANJRR, NJR, and four others) found no reduction in all-cause revision for hip-fracture THA and a possible infection trade-off — supporting selective rather than universal use.
- Re-revision burden: revision for instability carries a high re-revision rate, underlining that prevention at the index operation is paramount.
Side-by-Side Society Guidance
- Emphasis
- Patient-specific risk stratification; component positioning; larger heads and dual mobility for high-risk patients
- Emphasis
- Surgeon experience and approach selection; meticulous technique; registry surveillance via NJR
- Emphasis
- Restoration of offset, leg length, and soft tissue tension; intraoperative stability testing
- Emphasis
- Spinopelvic assessment (functional safe zone) in stiff-spine patients; dual mobility in defined high-risk groups
High- vs Limited-Resource Variation
- High-resource settings: CT and navigation/robotics for version planning; routine availability of dual mobility, constrained liners, augments, and modular revision systems; spinopelvic imaging for at-risk patients.
- Limited-resource settings: reliance on plain radiographs and mechanical alignment guides; emphasis on fundamentals — optimal positioning, ≥36mm heads where available, meticulous posterior soft tissue repair, and robust patient education/precautions, which deliver most of the achievable risk reduction at low cost.
Peri-operative Pharmacology (Global Principles)
- VTE prophylaxis: LMWH or oral anticoagulant (e.g. rivaroxaban, apixaban) with mechanical prophylaxis; duration commonly 10-14 days, extended up to ~35 days in higher-risk patients (follow local/society guidance).
- Antibiotic prophylaxis: a first-generation cephalosporin (e.g. cefazolin, weight-adjusted) within 60 minutes of incision, re-dosed for long cases or major blood loss; vancomycin/teicoplanin if MRSA risk or beta-lactam allergy; no proven benefit beyond 24 hours.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“”
- Confirm diagnosis: Posterior dislocation clinically and radiographically
- Document detailed neurovascular examination: Ankle dorsiflexion (common peroneal), plantarflexion (tibial), sensation dorsal and plantar foot - ALL NORMAL in this case
- Review post-operative radiographs and operative note (approach, component sizes)
- Analgesia: IV opioids for pain control
- NPO status in preparation for procedural sedation
- This is a first-time dislocation - closed reduction is indicated
- Arrange procedural sedation (propofol or ketamine) or general anesthesia
- Allis method: Patient supine, hip and knee flexed 90°, inline traction with gentle internal rotation
- Palpable clunk indicates reduction
- Repeat neurovascular examination immediately (document any changes)
- Post-reduction AP pelvis and lateral hip radiographs (confirm concentric reduction)
- Compare post-reduction films to immediate post-operative radiographs
- Measure cup inclination and estimate version
- First dislocation at 8 weeks with clear traumatic mechanism (getting out of low chair)
- If components appear well-positioned: Trial of non-operative management
- If clear malposition: Consider early revision surgery
- Hip abduction brace fitted (neutral to 15° abduction, 12 weeks)
- Strict posterior hip precautions: No flexion over 90°, no adduction, no internal rotation
- No low chairs or couches - provide elevated toilet seat
- Physical therapy for gait training and precautions education
- May discharge home if stable, good support, and patient can mobilize safely
- Follow-up 1-2 weeks for clinical and radiographic assessment
- Recurrence risk: 25-50% after first dislocation
- Strict precautions for 12 weeks minimum
- Lifelong awareness of high-risk positions (low chairs, bending to tie shoes, crossing legs)
- Immediate return if sensation of instability or dislocation
- If recurrence occurs, will need CT scan and likely revision surgery
- CT scan to measure precise cup and femoral version
- Calculate combined anteversion
- If significantly outside safe zones (inclination over 50°, retroversion, combined AV under 25° or over 45°): Early revision surgery recommended
- Revision options: Cup revision with dual mobility, or isolated liner exchange if shell salvageable
- Non-operative treatment likely to fail if malpositioned components
Systematic approach to acute THA dislocation, emphasis on neurovascular documentation, appropriate closed reduction technique, post-reduction assessment for underlying cause, individualized treatment plan based on component position and patient factors, clear counseling on recurrence risk and prevention strategies.
“”
- Recurrent instability (three dislocations) - this is a surgical problem
- Clear component malposition: Cup inclination 55° (outside Lewinnek safe zone of 30-50°)
- Combined anteversion calculation: 25° (cup) + 18° (femoral) = 43° (upper end of acceptable range 25-45°)
- Primary problem is excessive cup inclination leading to reduced posterior coverage
- Demonstrates instability on clinical examination (dislocates at 90° flexion + IR)
- Non-operative treatment has failed (three dislocations despite bracing)
- Review CT scan 3D reconstruction for surgical planning
- Assess bone stock for revision (any osteolysis or defects)
- Rule out infection: Check ESR, CRP (low threshold for aspiration if elevated)
- Review all previous operative notes (component types, sizes, fixation)
- Assess for polyethylene wear on radiographs
- Medical optimization and anesthetic assessment
- Indication: Recurrent instability with clear malpositioned acetabular component
- Goal: Revise cup to correct position AND provide enhanced stability construct
- Approach: Posterior approach (same as index surgery)
- Cup removal: greater than 360° exposure, curved osteotomes, explant device, preserve bone
- Target cup position: Inclination 40° (reduce from 55°), anteversion 20-25°
- Target combined anteversion: 38-43° (20-25° cup + 18° femoral = middle of safe range)
- Dual mobility prosthesis: Indicated given recurrent instability history
- Femoral component: Assess for loosening; if stable and version acceptable, retain
- Careful cup removal to preserve bone stock
- Ream to stable bleeding bone (may need larger cup than original)
- Decrease inclination to 40° - use mechanical alignment guides and intraoperative fluoroscopy
- Press-fit cementless cup with supplemental screw fixation (2-3 screws, avoid sciatic nerve zone)
- Insert dual mobility liner into shell (verify fully seated)
- Small head (28-32mm cobalt-chrome) into polyethylene liner
- Meticulous posterior soft tissue repair (capsule, short external rotators)
- Intraoperative stability testing - should be very stable with dual mobility
- If bone stock inadequate or medical comorbidities preclude major revision
- Consider dual mobility liner into existing shell (if compatible)
- Less ideal as doesn't correct malposition, but provides enhanced stability
- Constrained liner as salvage option (but higher failure rate than dual mobility)
- Hip abduction brace 12 weeks (strict)
- Protected weight bearing 6 weeks (for bone ingrowth)
- Strict posterior hip precautions 12 weeks
- Close follow-up: 2 weeks, 6 weeks, 3 months, 6 months, 1 year
- Serial radiographs to monitor cup fixation and position
- This is a complex revision with risk of recurrence (5-15% with dual mobility)
- Dual mobility significantly reduces dislocation risk compared to standard bearing
- Small risk of intraprosthetic dislocation (under 1%)
- Need for strict precautions and brace for 12 weeks
- Lifelong follow-up required
- Infection risk higher in revision (1-2%)
Systematic problem identification (component malposition as root cause), calculation of combined anteversion, recognition that three dislocations mandate surgery, appropriate selection of dual mobility for recurrent instability, technical plan to correct cup malposition, comprehensive patient counseling on risks and outcomes. This scenario tests ability to analyze CT data, understand combined version concept, and select appropriate revision strategy.
“”
- Parkinson's disease: markedly increased dislocation risk (neuromuscular disorder, rigidity, bradykinesia, falls)
- Cognitive impairment: increased risk (non-compliance with precautions, confusion)
- Age 78: increased risk (frailty, muscle weakness, falls)
- Previous acetabular fracture: increased risk (altered anatomy, potential bone defects, previous surgery)
- Overall assessment: This is a VERY HIGH RISK patient for dislocation
- CT scan of pelvis: Assess acetabular anatomy and bone stock post-fracture
- Look for bone defects or deformity from previous fracture
- Assess femoral version (may be altered from fracture)
- Plan component positioning based on native anatomy
- Detailed templating for offset and leg length restoration
- Neurology input for Parkinson's optimization
- Geriatrics/psychiatry input for cognitive assessment and perioperative management
- Primary recommendation: Dual mobility THA given multiple high-risk factors
- Evidence: Substantially reduces dislocation risk compared to standard bearings in high-risk groups
- Particularly effective in: Neuromuscular disease, cognitive impairment, elderly patients
- Trade-off: Accept potential increased wear for significant stability benefit
- Alternative: Standard bearing with 40mm head IF dual mobility not available, but significantly higher risk
- Direct anterior approach (if experienced): Lowest dislocation rate (0.5-2%), preserves posterior soft tissues
- Posterior approach (if anterior not feasible): Meticulous soft tissue repair mandatory
- Previous fracture may have scarring - approach through virgin tissue if possible
- Extensile approach if needed for acetabular exposure/reconstruction
- Target cup inclination: around 40° (middle of safe zone for margin of error)
- Target cup anteversion: around 20° (middle of safe zone)
- Assess femoral version intraoperatively
- Target combined anteversion: 35-40° (middle of 25-45° range)
- Use navigation if available: Improves accuracy, reduces outliers
- Restore offset and leg length: Adequate soft tissue tension critical
- Address any bone defects from previous fracture (augments, structural graft)
- If posterior approach: Meticulous capsular repair with heavy braided suture
- Short external rotator repair to greater trochanter (transosseous or suture anchors)
- Dual mobility construct assembly (practice on back table first)
- Extensive stability testing - should be very stable with dual mobility
- Assess for impingement through range of motion
- Hip abduction brace: 12 weeks minimum (may extend given cognitive impairment)
- Strict hip precautions: 12 weeks (simplified instructions for cognitive impairment)
- Caregiver education: Essential given cognitive status
- Home modifications: No low chairs/couches, elevated toilet, remove tripping hazards
- Physical therapy: Supervised only initially, gait training, fall prevention
- Parkinson's medication optimization: Work with neurologist to minimize dyskinesias and falls
- Dislocation risk remains elevated despite all precautions (realistic expectations)
- Dual mobility significantly reduces risk but doesn't eliminate it
- Lifelong supervision and precautions likely needed given Parkinson's and cognitive impairment
- Benefits of THA (pain relief, function) must outweigh risks
- Alternative: Continue non-operative management if risks too high
- Close follow-up required
Comprehensive risk stratification identifying multiple high-risk factors, appropriate selection of dual mobility prosthesis for high-risk patient, understanding of approach options and their dislocation risks, meticulous component positioning strategy with combined anteversion concept, enhanced post-operative protocol tailored to patient's limitations, realistic counseling on residual risk despite optimal technique. This scenario tests ability to synthesize multiple risk factors and formulate comprehensive prevention strategy.
MCQ Practice Points
Q: What is the most common direction of THA dislocation and why? A: Posterior dislocation (75-80% of cases). This is associated with the posterior approach, which disrupts the short external rotators and posterior capsule. Risk activities include flexion greater than 90°, adduction, and internal rotation.
Q: What are the Lewinnek "safe zones" for acetabular cup positioning? A: Inclination 40° (±10°) and anteversion 15° (±10°). Cups outside these ranges have significantly higher dislocation rates. Combined anteversion (cup + stem) of 25-45° is the modern target to account for stem version.
Q: What is the mechanism of dual mobility cups in reducing dislocation? A: Dual articulation provides a larger effective head size (increased jump distance). The small inner bearing articulates within a larger polyethylene liner, which itself articulates with the metal shell, providing greater range of motion before impingement.
Q: When is a constrained liner indicated in revision for instability? A: Recurrent dislocation with adequate component positioning and soft tissue deficiency (abductor insufficiency, neurological deficit), as a salvage option. Constrained liners mechanically lock the head into the socket but increase stress at the bone-implant interface, risking loosening.
Exam Day Cheat Sheet
Incidence & Direction
- Primary THA: 1-5%, Revision: 10-25%
- Posterior dislocation: 75-80% (posterior approach)
- Anterior dislocation: 15-20%
- 50% occur in first 3 months post-op
Lewinnek Safe Zones
- Cup inclination: 40° ± 10° (range 30-50°)
- Cup anteversion: 15° ± 10° (range 5-25°)
- Combined anteversion: 25-45° (MORE IMPORTANT)
- Many dislocations occur within safe zones - not absolute
Risk Factors (4 P's)
- Patient: Age over 70, cognitive impairment, neuromuscular disease
- Procedure: Posterior approach, revision surgery
- Position: Component malposition, impingement
- Power: Soft tissue laxity, abductor dysfunction
Acute Management
- 1) Document neurovascular exam thoroughly
- 2) Closed reduction (Allis: flexion 90°, traction + IR)
- 3) Post-reduction films + repeat neuro exam
- 4) Hip brace + precautions 12 weeks
First Dislocation
- Well-positioned components: Non-op (brace, precautions)
- Malpositioned: CT scan → early revision
- Recurrence risk: 25-50%
- NO low chairs/toilets, NO flexion over 90°
Recurrent Dislocation (2+ Events)
- CT scan MANDATORY - measure combined anteversion
- This is a SURGICAL problem - non-op fails
- Options: 1) Liner exchange + larger head (if cup OK)
- 2) Cup revision + dual mobility (GOLD STANDARD)
- 3) Constrained liner (salvage only)
Dual Mobility
- Two articulations: 28-32mm head in poly, poly in shell
- Effective head diameter ~50mm
- Dislocation rate: 0.5-2% vs 2-5% standard
- Best for: Recurrent instability, high-risk patients, revisions
- Risk: Intraprosthetic dislocation under 1%, wear
Head Size Effect
- 36mm vs 28mm: 1.3% vs 5.4% dislocation (Howie RCT)
- 28mm → 32mm → 36mm progressively more stable
- Minimum 32mm, prefer 36mm
- Larger = increased jump distance + impingement-free arc
Prevention (STABLE HIP Mnemonic)
- Soft tissue repair (meticulous posterior capsule)
- Thirty-six mm head minimum
- Anteversion combined 25-45°
- Brace for high-risk patients
- Leg length and offset restoration
- Education on precautions
- High-risk patients get dual mobility
- Inclination 35-45° (middle of safe zone)
- Patient selection and approach choice
Complications of Dislocation
- Recurrence: 25-50% after 1st, 60-75% after 2nd
- Sciatic nerve injury: 10-20% (neuropraxia, 80-90% recover)
- Posterior wall fracture: ORIF if over 25-30%
- Accelerated wear and loosening from recurrent events
Registry & Global Data
- Instability is a leading early revision cause (AOANJRR, NJR, AJRR)
- Anterior approach: lower dislocation revision than posterior
- Dual mobility: lower dislocation, but no all-cause revision benefit in fracture THA (Farey 2022)
- Re-revision after instability revision is high
Viva Scenario Approach
- First dislocation → Closed reduction + assess position
- Recurrent → CT + calculate combined AV → revise
- High-risk patient → Primary dual mobility + optimal positioning
- Cup 55° inclination → PRIMARY PROBLEM → revise cup
Combined Anteversion Calculation
- Formula: Cup AV + Femoral AV = Target 25-45°
- Ideal: 35-40° (middle of range for margin)
- Can compensate one component for the other
- Example SAFE: Cup 25° + Femoral 15° = 40°
- Example UNSAFE: Cup 10° + Femoral 20° = 30° (but cup retroverted)
Posterior Soft Tissue Repair
- Enhanced repair dramatically lowers dislocation (Pellicci 4% → 0%)
- Repair posterior capsule + short external rotators to GT
- Use heavy braided non-absorbable suture
- MANDATORY with posterior approach - not optional
High-Yield Exam Traps
- Safe zones not absolute - functional safe zone matters (spinopelvic)
- Combined AV more important than individual components
- Dual mobility preferred over constrained (better outcomes)
- Recurrent = surgical problem (non-op fails)
- CT mandatory for recurrent instability assessment
ULTIMATE EXAM PEARL: If an examiner shows recurrent dislocation, your immediate thought process should be: (1) "This is a SURGICAL problem - non-operative management has failed"; (2) "I need a CT scan to measure combined anteversion and identify the malpositioned component"; (3) "Treatment is revision surgery to correct malposition PLUS dual mobility for enhanced stability." Demonstrating this systematic approach shows senior-level decision making. Never say "try another closed reduction and longer bracing" for recurrent dislocation - this shows poor understanding and will fail the viva.