Familial avascular necrosis of the phalangeal epiphyses | Typically affects adolescents | Presents with painless or mildly painful PIP joint swelling
- Pathology: Idiopathic avascular necrosis (osteochondrosis) affecting the epiphyses of the phalanges, most frequently the proximal interphalangeal (PIP) joints of the hands.
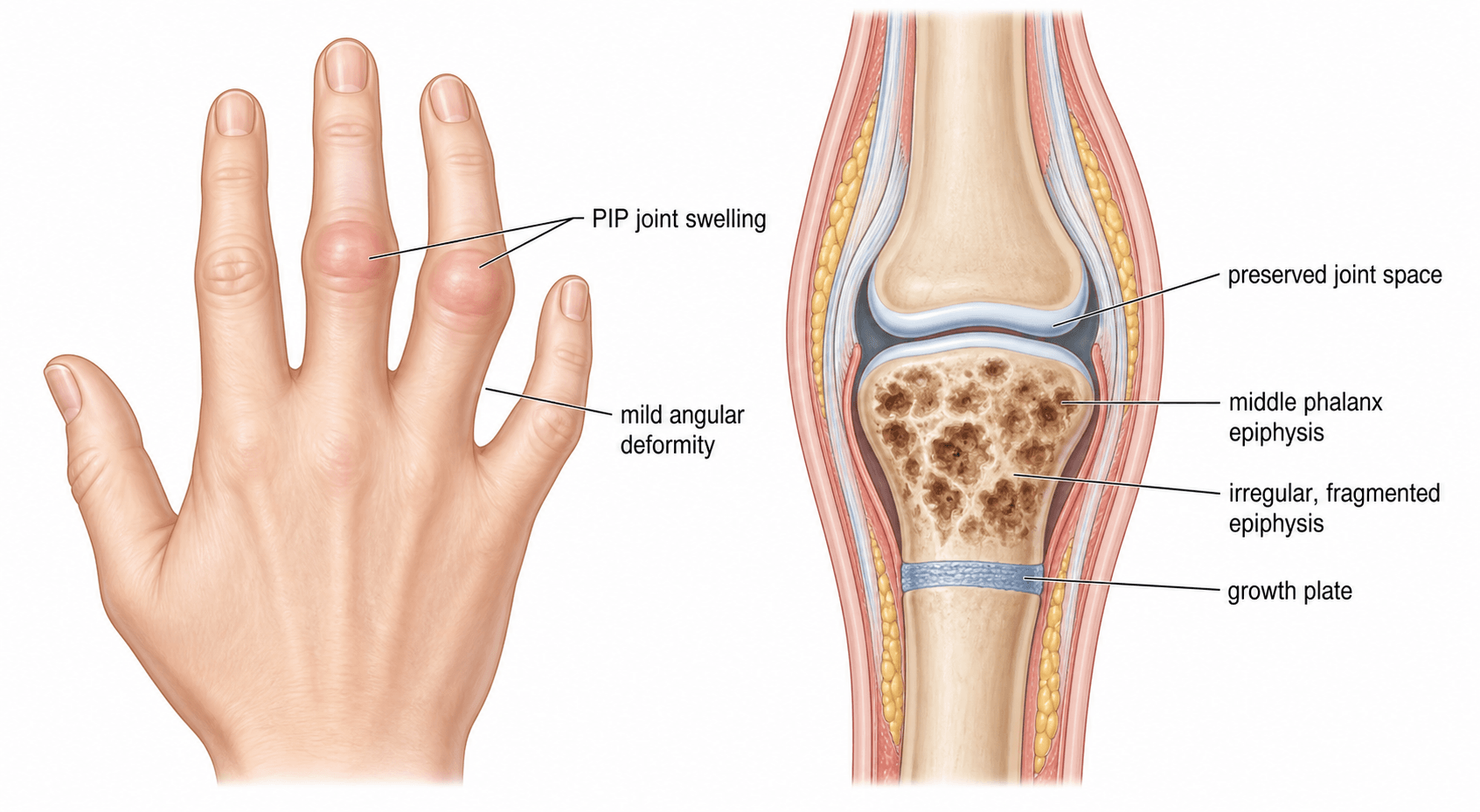
- Presentation: Typically presents in adolescence with broad, swollen digits that are often painless or only mildly painful, with preserved range of motion initially.
- Imaging: Radiographs show sclerosis, flattening, and fragmentation of the affected phalangeal epiphyses, which later fuse prematurely leading to brachydactyly.
- Genetics: Often familial with an autosomal dominant inheritance pattern, though sporadic cases occur. It may be linked to mutations affecting skeletal development.
- Management: Primarily conservative. Observation, activity modification, and NSAIDs for pain. Surgery is rarely indicated unless severe deformity or osteoarthritis develops later in life.
- “Unlike inflammatory arthritis, Thiemann disease often presents with painless or mildly painful joint swelling without systemic inflammatory markers.
- “The hallmark radiological finding is the 'fragmented epiphysis' of the phalanx.
- “Premature physeal closure is a common sequela, resulting in shortened digits (brachydactyly).
- “Always differentiate from juvenile idiopathic arthritis to avoid unnecessary immunosuppressive therapy.
The classic patient is a healthy adolescent presenting with swollen PIP joints that are remarkably painless or only mildly aching. Do not jump straight to JIA without considering osteochondroses.
Look for sclerosis, flattening, and fragmentation of the phalangeal epiphyses. The joint space is typically preserved early on, which helps distinguish it from inflammatory arthritis.
The avascular necrosis damages the growth plate, leading to premature fusion. This results in brachydactyly (short digits), a classic late finding in adults who had Thiemann disease in adolescence.
The condition is usually self-limiting. Reassure the patient and family. Do not prescribe aggressive systemic treatments or plan early surgical intervention unless significant deformity dictates it.
Overview
Thiemann disease is a rare osteochondrosis characterised by avascular necrosis of the epiphyses of the phalanges. It most commonly affects the proximal interphalangeal (PIP) joints of the hands, though the distal interphalangeal (DIP) joints and the toes can also be involved.
It typically presents in adolescence (between 11 and 19 years of age) with broad, swollen digits. Unlike many other arthropathies, the swelling in Thiemann disease is often painless or accompanied by only mild discomfort, and range of motion is initially preserved.
The condition can occur sporadically, but it frequently shows a strong familial tendency with an autosomal dominant pattern of inheritance with high penetrance. For the exam, the key is distinguishing this benign, self-limiting osteochondrosis from more destructive inflammatory conditions like Juvenile Idiopathic Arthritis (JIA).
Genetics: TRPV4 & the Thiemann-FDAB Spectrum
The topic states familial cases are "autosomal dominant" and "may be linked to mutations affecting skeletal development" without naming the gene or the related condition its own cited evidence (Damseh et al) identifies.
- The gene. Familial Thiemann disease has been associated with a heterozygous missense variant in TRPV4 (Transient Receptor Potential Vanilloid 4), a calcium-permeable cation channel - the same variant that causes familial digital arthropathy-brachydactyly (FDAB).
- One spectrum, not two diseases. Because an identical TRPV4 variant produced both labels in the same family, Thiemann disease and FDAB are now thought to represent phenotypic variability of the same non-inflammatory digital arthropathy rather than distinct entities.
- How they differ within the spectrum. Thiemann initially affects the PIP joints, primarily the bases of the middle phalanges; FDAB tends to affect the distal (DIP) joints first, with the heads of the middle phalanges as the primary site, plus more extensive involvement, radial deviation and more pronounced brachydactyly.
- Counselling. Inheritance is autosomal dominant with high penetrance, so a clear family history and genetic testing (TRPV4) guide reproductive counselling - while reassuring that the arthropathy is non-inflammatory and largely self-limiting. (TRPV4 is pleiotropic - other variants cause skeletal dysplasias and neuropathies - but the digital-arthropathy phenotype is the relevant one here.)
Familial Thiemann disease is linked to a TRPV4 variant - the same gene/variant as familial digital arthropathy-brachydactyly (FDAB) - so they are likely one spectrum. Thiemann hits the PIP / middle- phalanx bases first, whereas FDAB hits the DIP / middle-phalanx heads with radial deviation and more brachydactyly. Inheritance is autosomal dominant, high penetrance.
Pathophysiology
The core pathology is idiopathic avascular necrosis (osteonecrosis) of the secondary ossification centres (epiphyses) of the phalanges.
- Vascular Insufficiency: During the adolescent growth spurt, the expanding epiphyses have high metabolic demands. A mismatch between blood supply and demand, possibly exacerbated by microtrauma or genetic predisposition, leads to ischaemia and necrosis of the epiphyseal bone.
- Bone Response: The necrotic bone is reabsorbed and replaced by new bone (creeping substitution). During this vulnerable phase, normal mechanical stresses across the joint can cause the weakened epiphysis to flatten, fragment, and deform.
- Physeal Involvement: The adjacent physis (growth plate) is often damaged by the ischaemic process. This leads to premature physeal closure, arresting longitudinal growth of the affected phalanx and resulting in brachydactyly (short digits).
- Joint Mechanics: While the articular cartilage is initially spared, the altered shape of the subchondral bone eventually leads to joint incongruity. This predisposes the joint to secondary osteoarthritis in early adulthood.
Where Thiemann Sits Among the Osteochondroses
The topic repeatedly calls Thiemann an "osteochondrosis" and compares it to other osteochondroses (Perthes, Kienböck, etc.) without ever giving the framework that classifies them - a high-yield exam structure.
The osteochondroses are a heterogeneous group of disorders of the growing skeleton caused by disturbed endochondral ossification, many representing avascular necrosis of an ossification centre. They are conventionally divided by the site involved:
- Articular (epiphyseal) - involve the joint surface/epiphysis: Legg-Calvé-Perthes (femoral head), Freiberg (2nd metatarsal head), Kienböck (lunate), Köhler (tarsal navicular), Panner (capitellum), and THIEMANN (phalangeal epiphyses).
- Non-articular (apophyseal) - at a traction apophysis/tendon insertion: Osgood-Schlatter (tibial tubercle), Sever (calcaneal apophysis), Sinding-Larsen-Johansson (inferior pole of patella).
- Physeal - at the growth plate: Scheuermann (vertebral) and Blount (proximal tibial physis).
Thiemann is an articular (epiphyseal) "crushing" osteochondrosis of the phalangeal epiphyses - which is why the weakened epiphysis flattens and fragments and the physis may close prematurely (brachydactyly), exactly the behaviour of the articular group. (Each named disease has its own dedicated OrthoVellum topic.)
Osteochondroses split into articular/epiphyseal (Perthes, Freiberg, Kienböck, Köhler, Panner, Thiemann), non-articular/apophyseal (Osgood-Schlatter, Sever, Sinding-Larsen-Johansson) and physeal (Scheuermann, Blount). Thiemann is an articular epiphyseal osteochondrosis of the phalanges - hence epiphyseal fragmentation/flattening and premature physeal closure.
Classification
While there is no universally adopted staging system exclusively for Thiemann disease, its progression follows the typical radiological stages of osteochondroses (similar to Legg-Calvé-Perthes disease):
Radiographic Findings: Normal or slight increase in radiodensity (sclerosis) of the epiphysis.
Clinical Correlation: Mild swelling, often painless.
Clinical Presentation
The diagnosis of Thiemann disease relies heavily on recognising the classic clinical phenotype.
- Demographics: Adolescents, typically between 11 and 19 years old.
- Symptoms: Gradual onset of swelling in the PIP joints. The swelling is remarkably painless or causes only mild, aching pain after exertion. There are no systemic symptoms (no fever, rash, or malaise).
- Signs:
- Broadened, knobbly appearance of the PIP joints.
- Symmetrical or asymmetrical involvement (often bilateral but not necessarily perfectly symmetrical).
- Normal overlying skin (no erythema or warmth).
- Range of motion is often fully preserved early on, though mild restriction may develop as the bony deformity progresses.
- Late Presentation (Adults): Adults who had the disease in adolescence present with shortened digits (brachydactyly), enlarged joints, and symptoms of secondary osteoarthritis (pain, stiffness, loss of motion).
Investigations
Diagnosis is primarily clinical and radiological.
- Plain Radiographs (Hands/Feet): The gold standard for diagnosis.
- Early: Sclerosis and flattening of the phalangeal epiphyses.
- Progressive: Fragmentation of the epiphyses. The joint space is typically preserved (differentiating it from inflammatory arthritis).
- Late: Premature fusion of the growth plate, broad and flattened articular surfaces, shortened phalanges (brachydactyly), and secondary osteoarthritic changes (osteophytes, joint space narrowing).
- Blood Tests: Typically completely normal. ESR, CRP, rheumatoid factor (RF), and anti-CCP antibodies are negative. This is crucial for excluding juvenile idiopathic arthritis.
- MRI: Rarely required, but would show bone marrow oedema and typical changes of avascular necrosis (loss of normal marrow signal on T1-weighted images) early in the disease process before plain film changes are obvious.
Management
The management of Thiemann disease is overwhelmingly conservative. The goal is to manage symptoms while the epiphysis revascularises and heals, preventing unnecessary intervention.
- Reassurance and Education: The cornerstone of treatment. Explain the self-limiting nature of the acute phase, but warn about the potential for short digits and early arthritis.
- Activity Modification: Avoid heavy lifting, contact sports, or activities that place excessive axial load on the fingers during the active fragmentation phase.
- Analgesia: Simple analgesics or NSAIDs for pain relief during flares.
- Splinting: Temporary splinting may be used for symptomatic relief if pain is significant, but prolonged immobilisation should be avoided to prevent stiffness.
Complications
The complications of Thiemann disease are related to the mechanical damage inflicted on the growing bone and joint surface.
- Brachydactyly: Premature closure of the physis leads to noticeably shortened fingers or toes. This is mostly a cosmetic issue but can occasionally affect grip mechanics.
- Secondary Osteoarthritis: The deformed, flattened articular surface creates joint incongruity, leading to early wear and tear. This is the most significant long-term clinical problem, causing pain and stiffness in early to mid-adulthood.
- Joint Deformity and Stiffness: Broadened, knobbly joints that may develop flexion contractures or lose terminal flexion.
Guidelines, Registries and Global Practice
- Diagnostic Approach: Global practice emphasises the clinical differentiation of Thiemann disease from Juvenile Idiopathic Arthritis (JIA). The presence of painless epiphyseal fragmentation with negative inflammatory markers is universally accepted as diagnostic, avoiding unnecessary rheumatological workups.
- Genetic Counseling: In cases with a strong family history, genetic counseling may be offered to discuss the autosomal dominant inheritance pattern and the potential link to broader skeletal dysplasias (such as familial digital arthropathy-brachydactyly).
- Surgical Indications: There are no formal guidelines advocating for early surgical intervention in Thiemann disease. International consensus supports conservative management during adolescence.
- Nomenclature: While eponyms are becoming less favored in some medical communities, "Thiemann disease" remains the standard term used in orthopaedic literature and examinations worldwide to describe this specific epiphyseal avascular necrosis.
Memory aids
THIEFThiemann Features
Hook:Thiemann disease is a THIEF that steals the blood supply to the epiphyses in teenagers.
JIFTDifferential Diagnosis
Hook:Consider the JIFT list when an adolescent presents with swollen joints.
RESTTreatment Strategy
Hook:The best approach to Thiemann disease is to let it REST.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 14-year-old boy presents with a 6-month history of swelling in the PIP joints of his middle and ring fingers bilaterally. He denies any significant pain, morning stiffness, or systemic symptoms. Blood tests (ESR, CRP, RF) are normal. Radiographs show fragmentation of the PIP epiphyses. What is the diagnosis and how do you manage it?”
“The examiner shows you a radiograph of a 15-year-old's hand with flattening and sclerosis of the PIP epiphyses. They ask you to outline your differential diagnosis for avascular necrosis in the hand and wrist, and how you differentiate them clinically.”
“A 45-year-old man presents with chronic pain and stiffness in his PIP joints. Examination shows broad, shortened fingers (brachydactyly). He mentions his fingers have looked 'knobbly' since he was a teenager. Radiographs show severe PIP joint osteoarthritis with flattened articular surfaces. What is the likely underlying etiology and what are your management options?”
Core Concepts
- Avascular necrosis (osteochondrosis) of phalangeal epiphyses
- Peak incidence in adolescence (11-19 years)
- Familial cases show autosomal dominant inheritance
- Most commonly affects PIP joints of the hands
Clinical Presentation
- Broad, swollen, 'knobbly' PIP joints
- Painless or only mildly aching
- No systemic symptoms; normal inflammatory blood markers
- Late presentation: short digits (brachydactyly) and early OA
Radiographic Findings
- Early: Epiphyseal sclerosis and flattening
- Active: Epiphyseal fragmentation
- Late: Premature physeal closure, broad joint surface, OA changes
- Joint space is initially preserved
Management Strategy
- Conservative: Reassurance, activity modification, NSAIDs
- Self-limiting acute phase
- Avoid aggressive interventions
- Surgery only for end-stage secondary osteoarthritis in adults
Evidence: Key Papers in Thiemann Disease
Because Thiemann disease is rare, the literature consists primarily of case series and case reports. These papers highlight the genetic links and the diagnostic challenges.
Thiemann disease and familial digital arthropathy - brachydactyly: two sides of the same coin?
- Reviewed clinical and genetic features of Thiemann disease and familial digital arthropathy-brachydactyly (FDAB).
- Noted significant phenotypic overlap between the two conditions, including adolescent onset of PIP joint swelling and eventual brachydactyly.
- Suggested that these conditions might represent a spectrum of the same underlying genetic skeletal dysplasia rather than distinct entities.
- Highlighted the importance of genetic testing and detailed family history in familial cases.
Thiemann's disease: a very rare bone disorder.
- Case report detailing the presentation of a patient with Thiemann disease.
- Emphasised the diagnostic challenge, as patients often present to rheumatology clinics with suspected inflammatory arthritis.
- Confirmed the classic radiographic findings of epiphyseal fragmentation and subsequent early fusion without erosions typical of inflammatory disease.
Thiemann disease.
- Reported on the clinical and radiographic progression of Thiemann disease.
- Reiterated the hallmark features of painless or mildly painful swelling in the PIP joints during adolescence.
- Documented the typical conservative management strategy and the natural history leading to brachydactyly.